


Abstract
Scintigraphic imaging with 123I-metaiodobenzylguanidine (123I-MIBG) has demonstrated extensive losses of cardiac sympathetic neurons in idiopathic Parkinson's disease (IPD). In contrast, normal cardiac innervation has been observed in 123I-MIBG studies of multiple-system atrophy (MSA) and progressive supranuclear palsy (PSP). Consequently, it has been hypothesized that cardiac denervation can be used to differentiate IPD from MSA and PSP. We sought to test this hypothesis by mapping the distribution of cardiac sympathetic neurons in patients with IPD, MSA, and PSP by using PET and 11C-meta-hydroxyephedrine (11C-HED). Also, the relationship between cardiac denervation and nigrostriatal denervation was investigated by measuring striatal presynaptic monoaminergic nerve density with PET and 11C-dihydrotetrabenazine (11C-DTBZ). Methods: 11C-HED and 11C-DTBZ scans were obtained for patients with IPD (n = 9), MSA (n = 10), and PSP (n = 8) and for age-matched control subjects (n = 10). Global and regional measurements of 11C-HED retention were obtained to assess the extent of cardiac sympathetic denervation. 11C-DTBZ binding was measured in the caudate nucleus, anterior putamen, and posterior putamen. Results: As expected, extensive cardiac denervation was observed in several of the patients with IPD. However, substantial cardiac denervation was also seen in some patients with MSA and PSP. 11C-DTBZ studies demonstrated striatal denervation in all patients with IPD and in most patients with MSA and PSP. No correlation was found between cardiac 11C-HED retention and striatal 11C-DTBZ binding. Conclusion: Cardiac sympathetic denervation was found to occur not only in IPD but also in other movement disorders, such as MSA and PSP. This finding implies that scintigraphic detection of cardiac sympathetic denervation cannot be used independently to discriminate IPD from other movement disorders, such as MSA and PSP. Cardiac sympathetic denervation was not correlated with striatal denervation, suggesting that the pathophysiologic processes underlying cardiac denervation and striatal denervation occur independently in patients with parkinsonian syndromes. These findings provide novel information about central and peripheral denervation in patients with neurodegenerative disorders.
- Parkinson's disease
- multiple-system atrophy
- progressive supranuclear palsy
- PET
- meta-hydroxyephedrine
- dihydrotetrabenazine
Idiopathic Parkinson's disease (IPD) is associated with several autonomic manifestations, including gastrointestinal and genitourinary dysfunction and orthostatic hypotension. Patients with IPD who have orthostatic hypotension show decreased levels of norepinephrine in plasma and supersensitivity to norepinephrine infusion, indicating postganglionic sympathetic denervation (1). Multiple studies of IPD with planar scintigraphy or SPECT with 123I-metaiodobenzylguanidine (123I-MIBG), a false neurotransmitter taken up presynaptically by postganglionic sympathetic neurons innervating cardiac muscle, have shown striking reductions in myocardial 123I-MIBG uptake, indicating cardiac sympathetic denervation (2–18). Cardiac sympathetic denervation has been found in patients with IPD but without orthostatic hypotension, although to a lesser degree than in those with orthostatic hypotension (17,19). Although some investigators found cardiac sympathetic denervation in the early stages of IPD (7,10,11,13), others reported it only in cases at later stages (3,8). The neuropathologic basis of the denervation appears to be neurodegenerative, with Lewy body deposition in the cardiac plexus (20).
Several investigations of IPD with 123I-MIBG have included comparisons with 2 other parkinsonian syndromes, multiple-system atrophy (MSA) and progressive supranuclear palsy (PSP). Most have shown no abnormality in either MSA or PSP (6,8–10,12,13,15). Indeed, some investigators consider cardiac imaging with 123I-MIBG to be a means of differentiating IPD from other parkinsonian syndromes and to be particularly helpful in separating patients with IPD and with prominent autonomic symptoms from those with MSA (6,9,10,13,15,21). Although these investigations suggested that cardiac imaging can differentiate IPD from MSA and PSP, a few studies reported reduced uptake in both of these disorders, although the reductions reported were smaller than those in IPD (2,4,22).
PET offers higher sensitivity and more accurate measurements of tissue radioactivity concentrations than single-photon scintigraphy. PET with the sympathetic nerve tracer 11C-meta-hydroxyephedrine (11C-HED) not only provides quantitative measurements of cardiac tracer retention, reflecting sympathetic nerve density, but also allows for the detailed assessment of regional variations in left ventricular innervation (23,24). In this study, we used PET with 11C-HED to investigate the hypothesis that cardiac denervation is exclusive to IPD and as such can be used as a clinical measure to differentiate IPD from other movement disorders, such as MSA and PSP. We also measured striatal presynaptic monoaminergic nerve density with 11C-dihydrotetrabenazine (11C-DTBZ), a radioligand for the vesicular monoamine transporter (VMAT2), to determine whether the central and peripheral nervous system degenerative processes occur in parallel. Previous studies with 123I-MIBG demonstrated that essentially all subjects with more advanced stages of IPD (Hoehn–Yahr stages 3–5) have severe cardiac denervation (3,8,22). Because of this finding, we chose to study subjects with relatively early stages of IPD (Hoehn–Yahr stages 1 and 2) with the goal of including subjects with a wider range of cardiac innervation levels than would be seen in more advanced IPD. A preliminary version of this work was presented elsewhere (25).
MATERIALS AND METHODS
Study Population
The Institutional Review Board of the University of Michigan approved this investigation. Informed consent was obtained from all participants. The subjects studied included 9 patients who had IPD and who were 62 ± 15 y old (mean ± SD; range, 35–77 y; 1 woman and 8 men), 10 patients who had MSA and who were 62 ± 7 y old (range, 53–77 y; 3 women and 7 men), 8 patients who had PSP and who were 71 ± 6 y old (range, 63–80 y; 6 women and 2 men), and 10 healthy control subjects who were 61 ± 9 y old (range, 43–72 y; 6 women and 4 men). The diagnoses were based on published criteria for each of the disorders, IPD (26), MSA (27), and PSP (28).
Cardiac denervation occurs in diabetes mellitus (29–31); hence, subjects with this disorder were excluded. Because cardiac 11C-HED uptake can be influenced by cocaine (32) and tricyclic antidepressants such as desipramine (33), subjects known to be taking these drugs were excluded from the study. Several of the patients with neurodegenerative diseases were taking an antidepressant medication, including the selective serotonin reuptake inhibitors (SSRIs) fluoxetine, paroxetine, citalopram, and sertraline. Among the patients with IPD, 3 took an SSRI and 1 took trazodone. In the patients with MSA, an SSRI was taken by 6, trazodone was taken by 1, and bupropion was taken by 1. Among the patients with PSP, 2 were taking an SSRI and 3 were taking trazodone. Because the uptake of 11C-HED into cardiac sympathetic neurons is mediated exclusively by the norepinephrine transporter (NET) and because none of these antidepressants possesses a high affinity for NET (34), these medications are unlikely to influence cardiac 11C-HED uptake. All 9 patients with IPD were taking dopaminergic medications; 7 were taking carbidopa/levodopa, and 2 were taking pramipexole. Three patients with MSA were taking carbiodopa/levodopa, and 2 were taking pramipexole. Three patients with PSP were taking carbidopa/levodopa.
Radiochemistry
11C-HED was prepared by 11C methylation of (–)-metaraminol as the free base and purified by high-performance liquid chromatography (35). This procedure provided 11C-HED at specific activities of 18.5–55.5 TBq/mmol and radiochemical purities of greater than 98%. 11C-DTBZ was prepared by 11C methylation of α-(+)-9-O-desmethyldihydrotetrabenazine with a solid-phase support system allowing purification and isolation of the product, 11C-DTBZ, without high-performance liquid chromatography purification (36). Specific activities were >59.2 TBq/mmol, and radiochemical purities were greater than 95%.
PET Imaging
With the patient lying comfortably in the PET scanner, 740 ± 74 MBq (mean ± SD) of 11C-HED was injected intravenously, and a dynamic sequence of scans of the heart was acquired for 40 min. At 2 h after the injection of 11C-HED, 666 ± 66 MBq of 11C-DTBZ was injected intravenously, and a dynamic sequence of scans of the brain was acquired for 60 min. All scans were obtained with a Siemens ECAT EXACT-HR+ PET scanner, which has an intrinsic resolution of ∼4.6 mm full width at half maximum (FWHM). Sixty-three planes with a 2.425-mm center-to-center separation were imaged simultaneously. Attenuation correction was performed by reconstruction of measured transmission scan data, which was then segmented and reprojected back into sinogram space. The resolution of the reconstructed images was approximately 8–9 mm at FWHM for the 11C-HED scans and 6.0–6.5 mm at FWHM for the 11C-DTBZ scans. For the 11C-DTBZ studies, pixel-by-pixel fits with a reference region Logan plot analysis were performed (37). This analysis provided parametric images of the total tissue distribution volume ratio (DVR) for 11C-DTBZ relative to a reference region (occipital cortex) and parametric images of ligand transfer from plasma to brain. For measurements in the caudate nucleus, anterior putamen, and posterior putamen, anatomically configured volumes of interest were created from parametric images of the DVR. For 11C-HED, images from the heart scan were resliced by a computer algorithm into short-axis images for further quantitative analysis as previously described (38). A region of interest was placed over the left ventricular chamber in a short-axis slice near the base of the heart, and a time–activity curve for total activity in blood versus time was generated. Next, the left ventricular wall in each of the 8 short-axis slices from the apex to the base was automatically subdivided into 60 angular sectors to generate a total of 480 sectors. The time–activity curve for tissue 11C-HED concentration versus time was determined for each sector. As a semiquantitative measure of nerve density and neuronal integrity, tissue 11C-HED concentrations in the final image frame (30–40 min after injection) were normalized by dividing by the integral of the blood time–activity curve over the 40-min scan. This procedure provided for each myocardial region an 11C-HED retention index (RI; mL of blood/min/mL of tissue), which reflects the ability of the sympathetic neurons to take up and store norepinephrine. RI values for the 10 healthy control subjects were used to define a normal control database, in which the mean and SD for each myocardial sector were calculated and stored in the conventional polar map format used in nuclear cardiology. Measured RI data for each patient with a neurodegenerative disorder were compared with this healthy control database by use of z score analysis. For this analysis, a z score was calculated for each sector in a patient's polar map as follows: zi = (μi − qi)/σi; in this equation, qi is the patient's RI value for the ith sector of the polar map, μi is the healthy population mean RI for that sector, and σi is the corresponding across-subject SD of the healthy population for that sector. Left ventricular sectors with z scores of more than 2.5 (i.e., their 11C-HED RI values were more than 2.5 SDs below the healthy population mean) were considered to have abnormal 11C-HED retention. The fraction of 480 sectors in each patient's polar map that were abnormal was calculated as a measure of the extent of abnormal 11C-HED retention in the left ventricle. In addition, regional extent measures were also generated for 3 large regions of the left ventricle on the basis of the left ventricular regions perfused by the 3 main coronary arteries: left circumflex artery (LCX), left anterior descending artery (LAD), and right coronary artery (RCA).
Statistical Analysis
Analysis of variance was conducted to compare the mean levels of binding of 11C-DTBZ in the striatum between groups. For the mean RI values for 11C-HED in the heart, the use of analysis of variance was considered inappropriate because the distributions of values from patients were clearly nongaussian. Our interest lay in identifying patients with 11C-HED retention outside the normal range rather than the overall mean for each patient subgroup. To test for abnormal 11C-HED retention, a t statistic was computed for values from each patient by subtracting the control mean and dividing by the control SD. One-sided P values were then computed for whether an 11C-HED retention value as small as that observed could have arisen in the healthy population. These P values are presented without corrections for multiple comparisons but remained highly significant even after such corrections.
RESULTS
Patient Characteristics
The patients with IPD were generally in the early to middle phases of the disorder, with disease durations varying from 3 to 9 y and with Hoehn–Yahr scores of 1.5–2.5. Only 1 patient had symptoms of orthostatic hypotension; none had urinary retention or incontinence, and none had diabetes mellitus. The patients with MSA had various durations of symptoms (3–12 y) and had different degrees of ataxia and parkinsonism, but all had sufficient postural hypotension or urinary incontinence to qualify for the diagnosis of probable MSA. Two patients had severe intensity of both parkinsonian symptoms and postural hypotension, and a third patient had severe ataxia and postural hypotension but minimal parkinsonism. None of the patients with MSA had diabetes mellitus. The patients with PSP had various durations of symptoms (3–9 y) and various intensities of parkinsonism, but all had marked impairment of voluntary upgaze, downgaze, or both, absence of convergence, presence of square wave jerks, and positive responses to oculocephalic stimulation. One patient with PSP had a history of borderline diabetes mellitus that was managed without medication.
Cardiac 11C-HED Retention
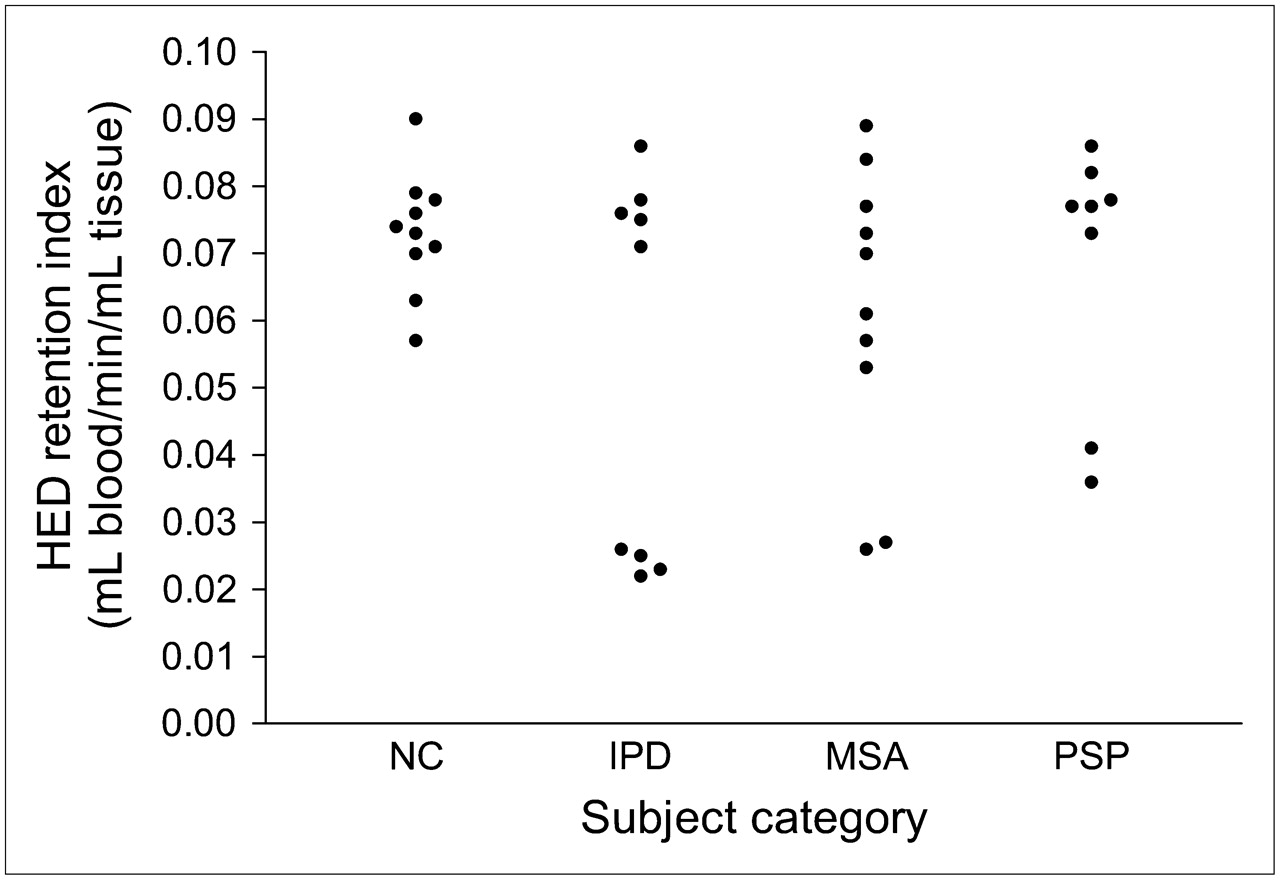
In the 10 control subjects, the mean and across-subject SD of the 11C-HED RI values was 0.073 ± 0.009 mL of blood per minute per milliliter of tissue. Table 1 summarizes the clinical features and 11C-HED retention measures for the patients with neurodegenerative disorders. To facilitate the comparison of cardiac denervation and striatal denervation, 11C-DTBZ binding potential data for the posterior putamen are also provided in Table 1. In Figure 1, the global mean 11C-HED RI values (i.e., average RI for the entire left ventricle) for each subject are plotted. Figure 2 shows representative cardiac PET images and corresponding 11C-HED retention polar maps.
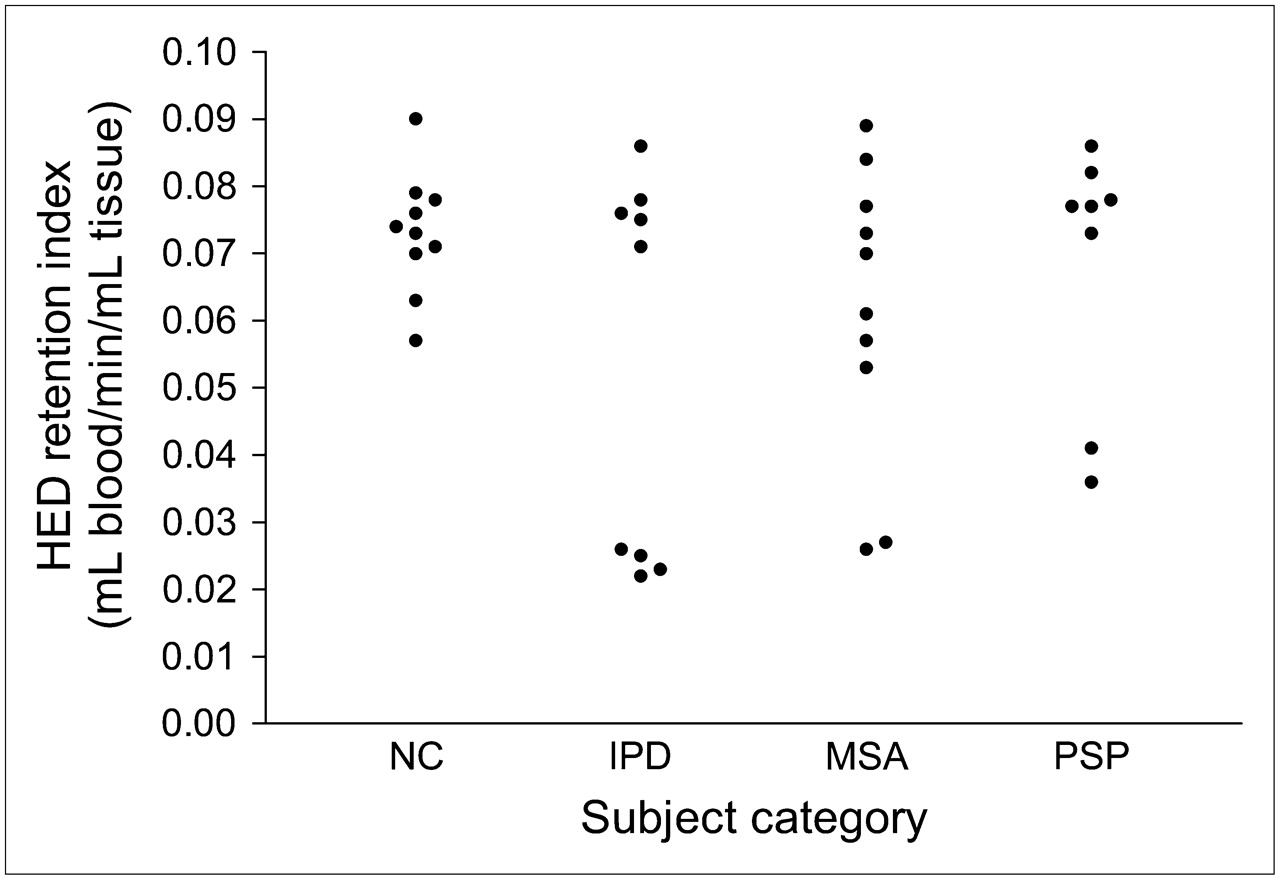
Global mean 11C-HED RI values. NC = normal (healthy) control.
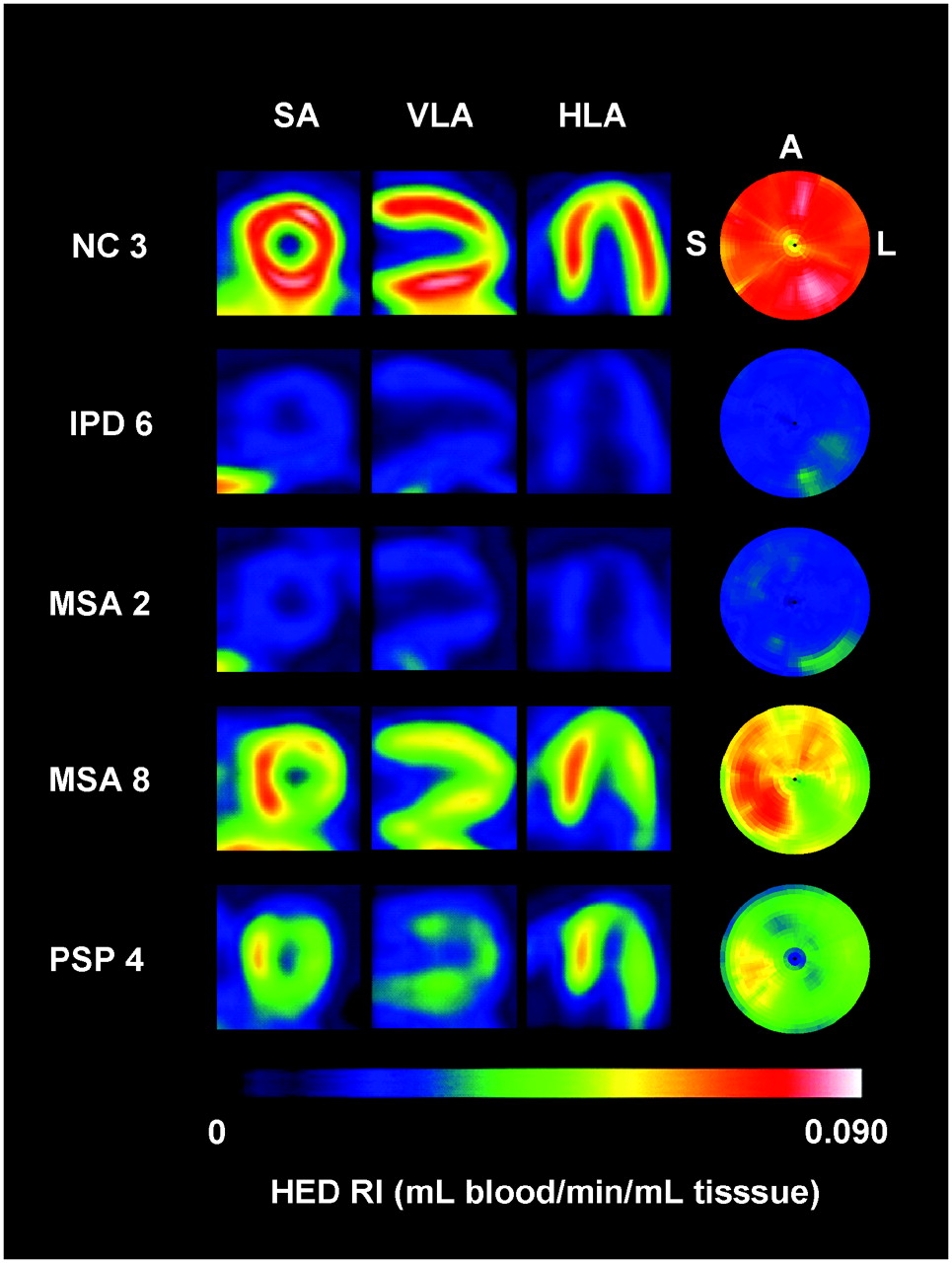
Representative parametric cardiac PET images and polar maps of 11C-HED retention. PET images are short-axis (SA), vertical long-axis (VLA), and horizontal long-axis (HLA) views for each subject. All PET images were normalized to integral of blood curve for each study, providing parametric 11C-HED RI images. PET images and polar maps of 11C-HED retention are all scaled to common maximum of 0.090 mL of blood per min per mL of tissue. For rainbow color table used, areas of low 11C-HED retention are shown in purple, blue and blue–green, moderate retention is shown in green and yellow, and normal retention is shown in orange, red, pink, and white. NC 3 images show high, uniform 11C-HED uptake in healthy control subject. IPD 6 images show extensive and severe denervation, as seen in 4 patients with IPD. MSA 2 images show extensive and severe denervation, as seen in 2 patients with MSA. MSA 8 images show nonuniform, more focal regional denervation, as seen in 2 patients with MSA. PSP 4 images show large regions of cardiac denervation, as seen in 2 patients with PSP. A = anterior wall; L = lateral wall; S = septal wall.
Clinical Features, Cardiac 11C-HED Retention Measures, and 11C-DTBZ Binding to Posterior Putamen in Patients with Neurodegenerative Diseases
Of the 9 patients with IPD, 4 had extensive myocardial denervation, with very low mean RI values (1-sided P values were 0.0002, 0.0002, 0.0003, and 0.0004) and more than 96% of the left ventricle having abnormally low 11C-HED retention values. The remaining 5 patients with IPD had 11C-HED retention values within the normal range.
Of the 10 patients with MSA, 2 had severe and extensive left ventricular denervation (P = 0.0004 for both cases). Two other patients with MSA had marginal global 11C-HED retention deficits (P = 0.03 and 0.06; these 2 P values would not be statistically significant after allowing for multiple comparisons). However, these 2 patients with MSA each had large regions of the left ventricle with statistically significant 11C-HED retention deficits, primarily in the LCX and RCA territories (Table 1; Fig. 2). Both patients with MSA and with severe global myocardial denervation had marked postural hypotension, akinesia, and urinary incontinence. One of these patients died after this study, and autopsy examination verified the diagnosis of MSA, with prominent degeneration of the pons, inferior olive, and cerebellum and with glial cytoplasmic inclusions positive for α-synuclein. Only 1 other patient with MSA had a similar severe level of postural hypotension, and this patient had principally ataxia, with few signs of parkinsonism. This patient and the remaining 5 patients with MSA had global 11C-HED RI values within the normal range.
Two of the 8 patients with PSP had extensive areas of severe denervation (global extent of abnormal values: 66% and 81%) leading to global mean RI values that were significantly lower than control values (P = 0.0017 and 0.0038), but they were not as low as those seen in the IPD and MSA patients with severe denervation. The remaining 6 patients with PSP had normal cardiac 11C-HED retention values.
Cardiac retention of 11C-HED did not appear to be influenced by the medications taken by the patients. In the 11 patients taking an SSRI, 11C-HED uptake was severely and globally decreased in 4, regionally decreased in 3, and essentially normal in 4. Among the 5 patients taking trazodone, 1 had a severe global decrease in 11C-HED uptake, and 4 had normal uptake. The 1 patient taking bupropion had fairly normal 11C-HED uptake. Patients taking no antidepressant included 2 with severe global decreases in uptake and 8 with normal uptake. In the 13 patients taking carbidopa/levodopa, 11C-HED uptake was severely and globally reduced in 6, regionally decreased in 1, and normal in 6. None of the 4 patients taking pramipexole had any 11C-HED retention abnormalities.
Striatal 11C-DTBZ Binding
Table 2 shows 11C-DTBZ binding potential data for the caudate nucleus, anterior putamen, and posterior putamen for the patients with IPD, MSA, and PSP in comparison with the healthy control subjects. All 3 groups of patients showed diminished binding compared with the healthy control subjects, and in the posterior putamen, the values for all 3 groups were more than 2 SDs below the values for the healthy control subjects. All 3 groups of patients also showed a gradient, with lower binding values in the posterior putamen than in the caudate nucleus. These results persisted after adjustment for age by analysis of covariance.
VMAT2 Transporter Densities in Brain
Relationship of Cardiac Retention to Putamen Binding
There was no clear relationship between cardiac 11C-HED retention and 11C-DTBZ binding in the posterior putamen (Fig. 3). Similarly, no correlations were found between cardiac 11C-HED retention and 11C-DTBZ binding in the anterior putamen and the caudate nucleus or between cardiac 11C-HED retention and the ratio of 11C-DTBZ binding potentials in the caudate nucleus and the posterior putamen (data not shown). The 4 patients with IPD, the 2 patients with MSA, and the 2 patients with PSP who showed substantial decreases in global cardiac retention also showed markedly diminished posterior putamen binding potential; however, several IPD and MSA patients with normal levels of cardiac retention also showed markedly diminished posterior putamen binding potential. Two of the patients with MSA, both with the MSA-C type, showed essentially normal posterior putamen binding potential and normal levels of cardiac retention as well. Figure 4 shows parametric images of the 11C-DTBZ DVR at the level of the striatum and corresponding 11C-HED RI polar maps for representative subjects.

Relationship between cardiac innervation and striatal monoaminergic nerve density. Plotted is global mean 11C-HED RI vs. 11C-DTBZ binding potential in posterior putamen. NC = normal (healthy) control.

Representative parametric images of 11C-DTBZ DVR and corresponding 11C-HED RI polar maps. Parametric images of 11C-DTBZ DVR are all scaled to common maximum of 3.5. DVR is related to binding potential (BP) by equation BP = DVR – 1 and is unitless. Polar maps of 11C-HED RI values are all scaled to common maximum of 0.090 mL of blood per min per mL of tissue. NC 5 images show high striatal binding of 11C-DTBZ and high, uniform cardiac retention of 11C-HED in healthy control subject. MSA 1 images show low striatal 11C-DTBZ binding and extensive severe cardiac denervation, as seen in 2 patients with MSA. MSA 4 images show low striatal 11C-DTBZ binding and normal uniform cardiac 11C-HED retention, as seen in 4 patients with MSA. MSA 9 images show normal striatal 11C-DTBZ binding and normal uniform cardiac 11C-HED retention, as seen in 4 patients with MSA. IPD 3 images show low striatal 11C-DTBZ binding and extensive severe cardiac denervation, as seen in 4 patients with IPD. IPD 7 images show low 11C-DTBZ binding in posterior putamen (with uncharacteristically well-preserved 11C-DTBZ binding in caudate nucleus) and normal uniform cardiac innervation, as seen in 5 patients with IPD. PSP 3 images show low striatal 11C-DTBZ binding and nonuniform cardiac denervation, as seen in 2 patients with PSP. PSP 8 images show low striatal 11C-DTBZ binding and normal uniform cardiac denervation, as seen in 5 patients with PSP.
DISCUSSION
MSA presents clinically with symptoms that are difficult to distinguish from those of IPD. Initial reports suggesting that cardiac denervation was exclusive to IPD were of great interest because it appeared that scintigraphic detection of cardiac denervation could be used as a single clinical measure capable of discriminating MSA from IPD. However, in the present study, contrary to many previous investigations (6,8–10,12,13,15), we found extensive denervation of cardiac postganglionic sympathetic fibers in 2 of 10 patients with probable MSA. One of these 2 patients died a few months after the present study, and the diagnosis of MSA was confirmed by neuropathologic examination of the brain. Two additional patients with MSA had substantial regional 11C-HED retention deficits. Sone et al. (39) recently reported neuropathologic changes in MSA that are likely to account for cardiac denervation. These investigators performed immunohistochemical examination of the sympathetic ganglia and brains of 26 patients with MSA and 19 age-matched control subjects. They found α-synuclein–immunoreactive structures in the sympathetic ganglia of 42% of the patients with MSA and none in the control subjects. The immunoreactive structures proved to be Lewy bodies in several of the cases; in the others, they consisted of diffuse or focal neuronal cytoplasmic aggregates and swollen neurites, suggesting that these aggregates were progressing to become Lewy bodies. The mean disease duration for cases of MSA showing α-synuclein–immunoreactive structures was significantly longer than that of cases of MSA not showing these structures. In the present study, our small sample limited our ability to infer the important variables that might lead to cardiac denervation in MSA. The patients with MSA and with extensive cardiac denervation (patients 1 and 2) had symptom durations of 10 and 3 y, respectively, but other patients without cardiac denervation had equal or longer durations of illness. These 2 severely affected patients had marked orthostatic changes and moderate to severe urinary incontinence, suggesting extensive autonomic denervation, but 1 other patient (patient 7) had similarly severe orthostatic changes and urinary incontinence but no cardiac denervation. The 2 patients with MSA and with partial cardiac denervation had moderately severe orthostatic changes and severe urinary incontinence, suggesting that these patients may have later developed more extensive cardiac denervation.
In the present investigation, the cardiac 11C-HED retention studies in patients with PSP also revealed findings contrary to those of several previous investigations, with severe denervation affecting large areas of the heart in 2 of the 8 patients. The 2 patients (patients 3 and 4) with cardiac denervation had disease durations of 5 and 9 y, respectively, but no urinary retention or incontinence and no orthostatic symptoms. The other patients with PSP had variable disease durations, some of 5–6 y but none as long as 9 y. One of the 2 patients with PSP and with cardiac denervation (patient 3) had diabetes mellitus, well controlled by diet alone. Although diabetes is associated with cardiac denervation, the pattern of myocardial sympathetic denervation is entirely different from that seen in this patient. Diabetic involvement of sympathetic cardiac fibers affects the longest neurons initially; hence, denervation proceeds from the apex to the base, initially occurring only in the inferior and lateral walls. Ultimately, this process evolves to a consistent pattern of denervation in which only the neurons in the proximal segments of the septal and anterior walls are preserved (29–31). The striking difference between the regional pattern of cardiac denervation seen in our patient with PSP and the typical pattern seen in diabetics makes it unlikely that diabetes was the underlying cause of the observed myocardial denervation in our patient. One of the 2 patients with PSP who had cardiac denervation (patient 3) was being treated with carbidopa/levodopa, but 2 other patients without denervation (patients 5 and 6) received similar doses of carbidopa/levodopa. Review of the additional clinical findings in the 2 patients with partial denervation revealed no other features that separated them from the other patients with PSP who had normal retention values. The neuropathologic basis for the findings in these patients is not clear, as a literature search revealed no postmortem studies of sympathetic ganglia in PSP suggesting denervation of sympathetic ganglia. Only a single relevant study was found; it demonstrated a severely diminished sympathetic sweat response on the palm to deep breathing in PSP, suggesting an abnormality of sympathetic function in this disorder (40).
Previous studies of IPD with 123I-MIBG documented that cardiac denervation generally occurs after the disease evolves beyond its earliest stages (Hoehn–Yahr stage 1), occurring in nearly all patients with more advanced stages of IPD (Hoehn–Yahr stages 3–5) (3,8,22). The 9 patients with IPD who were studied in the present work all were in the early to moderate stages of IPD (Hoehn–Yahr stages 1.5–2.5). Four of the 9 patients with IPD were found to have extensive cardiac denervation. Disease severity, as measured by Hoehn–Yahr stage, was not predictive of the presence or absence of extensive cardiac denervation. The 4 patients with IPD and with denervation had disease durations of 3–4 y. The 5 patients with 11C-HED retention values in the normal range included 3 patients with disease durations as long as 7–9 y. Thus, within the small group of patients with IPD studied in the present work, there was no correlation between cardiac denervation and disease duration or disease severity.
Our 11C-HED results can be compared with those of a recent report by Nagayama et al. (22), who used 123I-MIBG to study the incidence of cardiac denervation in a large cohort of patients with parkinsonian syndromes. Included in their study were 45 patients with IPD at Hoehn–Yahr stages 1 and 2, 14 patients with MSA, and 7 patients with PSP. The fraction of each group found to have decreased cardiac 123I-MIBG retention at 4 h (expressed as a heart-to-mediastinum [H/M] ratio) was generally consistent with our observations for patients with IPD and MSA but different from those for patients with PSP. For IPD at Hoehn–Yahr stages 1 and 2, they found that 30 of 45 patients (67%) had decreased 123I-MIBG retention, and we found that 4 of 9 patients (44%) had extensive 11C-HED retention deficits. For MSA, they found that 3 of 14 patients (21%) had decreased 123I-MIBG retention, and we found that 2 of 10 patients (20%) had substantial 11C-HED retention deficits, with 2 more (20%) having focal regions of myocardial denervation. For PSP, they found that 6 of 7 patients (86%) had 123I-MIBG H/M ratios below normal, although the H/M ratios were higher than those seen in patients with IPD and with severe myocardial denervation. In contrast, we observed significant 11C-HED retention deficits in only 2 of 8 patients with PSP (25%). This discrepancy in the findings for PSP is compelling and suggests that further studies with larger numbers of patients with PSP are needed to better characterize the impact of PSP on cardiac innervation. Apart from this discrepancy, there is considerable agreement between our 2 datasets.
The neuropathologic basis of cardiac denervation in IPD is neural degeneration with Lewy body deposition in the cardiac sympathetic plexus (20). Orimo et al. (41) used tyrosine hydroxylase (TH) immunohistochemistry to examine heart tissues from 5 control subjects, 11 patients with IPD, 8 patients with MSA, 5 patients with PSP, and several patients with dementia with Lewy bodies and Alzheimer's disease. They used the same methods to study sympathetic ganglia from control subjects and 5 patients with IPD. They found an almost total absence of TH-immunoreactive fibers in the heart tissues of most of the patients with IPD but preserved fibers in patients with PSP and all but 1 patient with MSA. TH immunoreactivity was preserved in the sympathetic ganglia of all but 1 patient with IPD. They concluded that cardiac postganglionic sympathetic denervation affects nerve fibers innervating the heart in advance of neuronal loss in the sympathetic ganglia. These findings are in keeping with the results of the present investigation apart from the absence of cardiac denervation found in PSP. The absence of an abnormality in PSP reported by Orimo et al. (41) may be attributable to the small sample of patients with PSP examined in their study (n = 5).
No correlation was found between cardiac 11C-HED retention and striatal 11C-DTBZ binding. The patients with IPD, MSA, and PSP and with diminished cardiac retention also showed markedly decreased striatal presynaptic monoaminergic innervation, but several other patients with IPD, MSA, and PSP but without cardiac denervation showed striatal denervation. Four patients with MSA had normal or slightly decreased striatal innervation, and these patients showed principally ataxia with autonomic failure and relatively few features of parkinsonism. The lack of correlation between cardiac 11C-HED retention and striatal 11C-DTBZ binding suggests that the degenerative processes affecting the substantia nigra and the postganglionic cardiac sympathetic neurons occur independently. However, in contrast to our findings, a recent study of early IPD that assessed cardiac innervation with 123I-MIBG and striatal dopaminergic neurons with the dopamine reuptake inhibitor 123I-N-ω-fluoropropyl-2β-carbomethoxy-3β-(4-iodophenyl)tropane (123I-FP-CIT) did find a strong correlation between cardiac denervation and nigrostriatal denervation (42). In that study of 18 patients with early IPD, Spiegel et al. found that binding of 123I-FP-CIT in the more affected striatum was highly correlated with 123I-MIBG retention (H/M ratio) (42). Using our 11C-HED retention data for cardiac innervation and striatal 11C-DTBZ binding data for only the more affected striatum, we found no such relationship for our patients with IPD. One difference between our study and that of Spiegel et al. is that the latter investigators examined patients with early IPD (Hoehn–Yahr stage 1), whereas our patients with IPD had somewhat more advanced disease (Hoehn–Yahr stages 1.5–2.5). Some of their patients had normal or intermediate striatal binding of 123I-FP-CIT in the affected striatum, whereas all of our patients with IPD had substantial striatal denervation, as demonstrated by greatly reduced 11C-DTBZ binding. However, this difference in the stage of IPD between the 2 groups does not completely explain the difference in the findings. The data of Spiegel et al. suggest that if marked striatal denervation is observed in a patient with IPD when 123I-FP-CIT or 11C-DTBZ is used, then extensive cardiac denervation should also be found when either 123I-MIBG or 11C-HED is used. However, in the present study, we found that several patients with IPD (5/9) had greatly reduced striatal 11C-DTBZ binding but normal cardiac 11C-HED retention. In the cohort of patients with early IPD who were studied by Spiegel et al., no patients with this combination of normal heart innervation and substantial striatal denervation were seen. Thus, with the available data, we are unable to explain the apparent difference between our findings and those of Spiegel et al. A more focused study, ideally following the progression of striatal denervation and cardiac denervation in a large group of patients with early IPD, is likely needed to better characterize the relationship between these 2 processes.
The reductions in cardiac 11C-HED retention and striatal 11C-DTBZ binding observed in the present study are unlikely to have been caused by medication effects. It is well established that 11C-HED is taken up into cardiac sympathetic neurons exclusively by NET (23), which is not significantly affected by SSRIs, trazodone, or bupropion (34). Although we observed severe global decreases in 11C-HED uptake in some patients taking SSRIs and trazodone, we also observed completely normal uptake in other patients taking these same medications at comparable doses. Levodopa is a very low-affinity substrate for NET (43), but no correlation was found between its use and the presence of 11C-HED retention deficits. In 11C-DTBZ studies of VMAT2 density in the brain, although many of our patients were taking either levodopa (a dopamine precursor) or pramipexole (a dopamine receptor agonist), the neuronal processing of these medications is different from that of 11C-DTBZ. Experimental in vivo studies have demonstrated that levodopa and dopamine receptor agonists do not affect the uptake of VMAT2 radioligands such as 11C-DTBZ (44). Thus, it seems likely that the substantial deficits in 11C-HED uptake and 11C-DTBZ binding observed in several of our patients resulted from denervation and not from medication effects.
CONCLUSION
PET with 11C-HED demonstrated that significant losses of myocardial sympathetic nerve fibers occur not only in patients with IPD but also in some patients with the parkinsonian syndromes MSA and PSP. In all patients with IPD and with reduced 11C-HED retention, sympathetic denervation consistently was found to occur throughout the entire left ventricle. Although some patients with MSA also had complete left ventricular denervation, some patients with MSA and PSP had only focal regions of denervation. In light of these findings, it appears that the scintigraphic detection of cardiac sympathetic denervation alone cannot be used to differentiate IPD from MSA and PSP. Cardiac denervation was found not to be correlated with striatal denervation, suggesting that the neurodegenerative processes in these tissues occur independently. These findings advance the understanding of the incidence and progression of cardiac denervation in parkinsonian syndromes.
Acknowledgments
We thank the staff of the University of Michigan Cyclotron/PET Facility for assistance in preparing the PET radiopharmaceuticals and performing the PET imaging studies. This work was supported by grants from the National Institutes of Health (National Institute of Neurological Disorders and Stroke grant P01 NS15655; National Institute on Aging grant P50 AG08671; and National Heart, Lung, and Blood Institute grant R01 HL079540).
References
- Received for publication June 16, 2006.
- Accepted for publication August 21, 2006.





{kind=link}
{kind=link}
{kind=link}
{kind=link}