


Abstract
Left bundle branch block (LBBB) is common in patients with heart failure (HF) and contributes to left ventricular (LV) dysfunction. The abnormal septal motion may alter septal metabolic demand but this has not been well characterized in patients with ischemic cardiomyopathy (ICM) and LV dysfunction. The aim of this study was to determine the effect of LBBB on septal metabolism in patients with ICM, LV dysfunction, and LBBB. Methods: Fifty-three patients with LV dysfunction and ICM were identified: 34 with LBBB, 19 with normal QRS (≤100, control patients). PET using 18F-FDG and 82Rb was used to measure myocardial glucose metabolism and perfusion, respectively. Perfusion-metabolism differences were determined. Scar scores (matched decreases in 18F-FDG and 82Rb), mismatch scores (hibernating myocardium with decreased 82Rb relative to 18F-FDG), and reverse-mismatch (R-MM) scores (reduced 18F-FDG relative to 82Rb) were assessed in the septum and lateral wall. Results: 18F-FDG uptake in the septum was reduced in patients with LBBB (64.0% ± 15.4%) compared with control patients (74.9% ± 14.3%; P < 0.05). Mean septal R-MM was greater in patients with LBBB (19.1% ± 15.3%) versus control patients (4.7% ± 10.6%; P < 0.05). However, 32% (11/34) of patients with LBBB did not demonstrate septal R-MM, 91% (10/11) of whom demonstrated lateral wall perfusion defects. Of the 68% (23/34) of patients with LBBB and septal R-MM, 52% (12/23) demonstrated lateral wall perfusion defects (P < 0.05). There was a significant difference in the percentage of the lateral wall with scar between those with septal R-MM (9.3% ± 10.5%) and those without (19.9% ± 14.3%; P < 0.05). Conclusion: Previously, LBBB was believed to be characterized by reduced glucose metabolism relative to perfusion in the septum; however, this is not always the case in ICM. LBBB is not associated with septal R-MM in >30% of this patient population. Absence of this finding was often associated with lateral wall perfusion defects, suggesting an alteration in the metabolic demand on the septum. This may have implications for HF therapies such as resynchronization and requires further study.
Congestive heart failure (CHF) is a debilitating and common disorder affecting approximately 1%–2% of the adult population and 6%–10% of the elderly population in developed countries (1). The most common cause of CHF in North America is ventricular dysfunction due to ischemic heart disease (IHD) (1). Left bundle branch block (LBBB), which has been reported to increase disease severity as well as mortality risk, is present in approximately 25% of patients with CHF and decreased systolic function (2). LBBB is also present in approximately 30% of patients with idiopathic dilated cardiomyopathy (IDC) (3,4).
Cardiac resynchronization therapy (CRT) is an important new treatment for patients with advanced CHF and LBBB. It has been shown to improve left ventricular (LV) function and reduce hard clinical endpoints, including hospitalization and death (5–12). Many questions remain to be answered about CRT; perhaps most important is the issue of nonresponse to this therapy. The nonresponder rate has been estimated to be up to 50% (6,11–17). Furthermore, emerging data suggest that the etiology of CHF is an important factor in determining response. Recent work has suggested that patients with ischemic cardiomyopathy (ICM) gain only a minor and transient benefit from CRT, with LV volumes deteriorating back to preimplant levels after 12 mo (18). This lack of response is not fully understood; hence, it is necessary to achieve a more complete comprehension of the pathophysiology of LBBB.
Changes in metabolism have also been observed in patients with IDC treated with CRT (4,7,9,19). Previous studies evaluating myocardial metabolism in patients with LBBB have focused primarily on the patient population with IDC, with few studies assessing the impact of LBBB in patients with ICM (4,9,20). The aim of this study was to determine the metabolic alterations in the septum of patients with LBBB, LV dysfunction, and ICM.
MATERIALS AND METHODS
Patient Population
The study population was composed of adult patients (age, >18 y old) who met inclusion criteria and who underwent 82Rb perfusion and 18F-FDG viability PET at the University of Ottawa Heart Institute. Study inclusion criteria were documented: (a) IHD by previous myocardial infarction, coronary angiography, prior coronary artery bypass grafting/percutaneous transluminal coronary angioplasty interventions, or a positive stress perfusion scan; and (b) LV dysfunction on radionuclide angiography, echocardiography, gated perfusion SPECT, or left ventriculography.
Eighty-eight patients with QRS > 100 ms were identified. Among these patients, 38 had criteria for LBBB and served as the study group. The remaining 50 patients had an intraventricular conduction delay or right bundle branch block (RBBB). Of the 38 patients with LBBB, the etiology of heart failure (HF) in 4 patients was IDC; thus, these 4 patients were excluded. Nineteen patients with normal QRS duration (≤100 ms) served as the control group. The Human Research Ethics Board of the University of Ottawa Heart Institute approved this study.
LBBB Electrocardiographic (ECG) Criteria
A 12-lead ECG was acquired for each patient. LBBB status was determined by a single board-certified cardiologist who was unaware of the patient's clinical or PET findings. The following criteria were used to confirm LBBB: QRS duration of >0.12 s; absence of Q waves in leads I, V5, and V6; monophasic broad R wave in leads I, V5, and V6; delayed intrinsicoid deflection in leads V5 and V6; and displacement of ST segment and T wave in a direction opposite to the major deflection of the QRS complex (21).
82Rb PET Protocol
Patients were positioned in a whole-body PET scanner (ECAT ART; Siemens), and a 4-min 137Cs transmission scan was performed for attenuation correction (22). Immediately after obtaining the transmission scan, 8 MBq/kg of 82Rb were administered intravenously over 30 s. The PET perfusion imaging was acquired at rest with a standard 82Rb protocol (23–25). A 7.5-min acquisition was initiated 2.5 min after tracer administration, as previously described (23–25).
18F-FDG PET Protocol
After an oral glucose load, a 4-min 137Cs transmission scan was performed for attenuation correction, and 35–215 MBq of 18F-FDG were administered intravenously. For patients with diabetes mellitus, a standard hyperinsulinemic-euglycemic clamp protocol was used (24–26). Forty minutes after injection, a 30-min 18F-FDG PET acquisition was initiated.
PET Image Processing
Perfusion and 18F-FDG images were reconstructed using filtered backprojection with a Hann window of the ramp filter and a cutoff frequency of 0.6 cycle/cm. A custom program (myoPC; Robert deKemp, University of Ottawa Heart Institute) was used to reorient images automatically along the long axis of the heart and sample the LV myocardium into polar maps with 460 sectors (24). The polar maps were expressed as a percentage of maximal uptake and divided into 5 segments, where each of the 4 walls has 180 sectors, and the apex has 100 sectors. In an effort to isolate any regional differences due to the LBBB, which may overlap with anterior or inferior walls, the current study focused on the differences between septal and lateral wall 18F-FDG and 82Rb uptake.
Tissue Characterization
The images were analyzed to assess the metabolic nature of the myocardium based on our viability scoring method (24). Briefly, perfusion was considered to be normal where uptake was ≥80% of maximum, excluding the septal wall. 18F-FDG activity was then normalized to the normal perfusion-zone value. Within the abnormal perfusion zone, a summed hibernating score (mismatch) was calculated from the sectors where 18F-FDG > perfusion, and a summed scar score (match) was calculated as the magnitude of the perfusion defect (100% − perfusion) minus the summed hibernating score. In this way, the perfusion defect is divided into components of hibernating myocardium and scar that can potentially coexist.
A reverse-mismatch score (R-MM) was calculated for each sector from the difference of perfusion minus 18F-FDG score. Thus, sectors with 18F-FDG < perfusion would yield a positive R-MM score. For the entire segment, a R-MM score of >10% was considered abnormal. This was based on similar cutoffs for differences in perfusion and 18F-FDG used to define match and mismatch (27). Hence, patients with LBBB and septal R-MM scores of >10% were considered “R-MM +ve,” whereas those with septal R-MM scores of ≤10% were considered “R-MM −ve.”
Statistical Analysis
Data are expressed as mean ± SD. The nonparametric Wilcoxon Mann−Whitney test for independent samples was performed to identify any significant differences between groups. Paired t tests were performed between septal and lateral walls to assess within-group differences. The Fisher exact or Yates' correction χ2 tests were used to assess any significant differences between groups of categoric data. In all cases, significance was considered valid at P < 0.05. All statistical analyses were performed with SPSS version 10.0 (SPSS Inc.).
RESULTS
Patient Characteristics
Fifty-three patients (35 male, 18 female; age, 66.3 ± 9.8 y) were included in the study, all with LV dysfunction and IHD. The demographic characteristics of the 2 groups of patients (LBBB group [n = 34] and control group [n = 19]) are given in Table 1. Patients with LBBB were older than the control patients (P = 0.03). There was a trend (P = 0.07) for an increased number of women in the LBBB group compared with the control group (previous reports have found a greater proportion of women with LBBB (28)). As expected, there was a significant difference in QRS duration between the groups (P < 0.001).
Demographic Characteristics
Myocardial Tracer Uptake
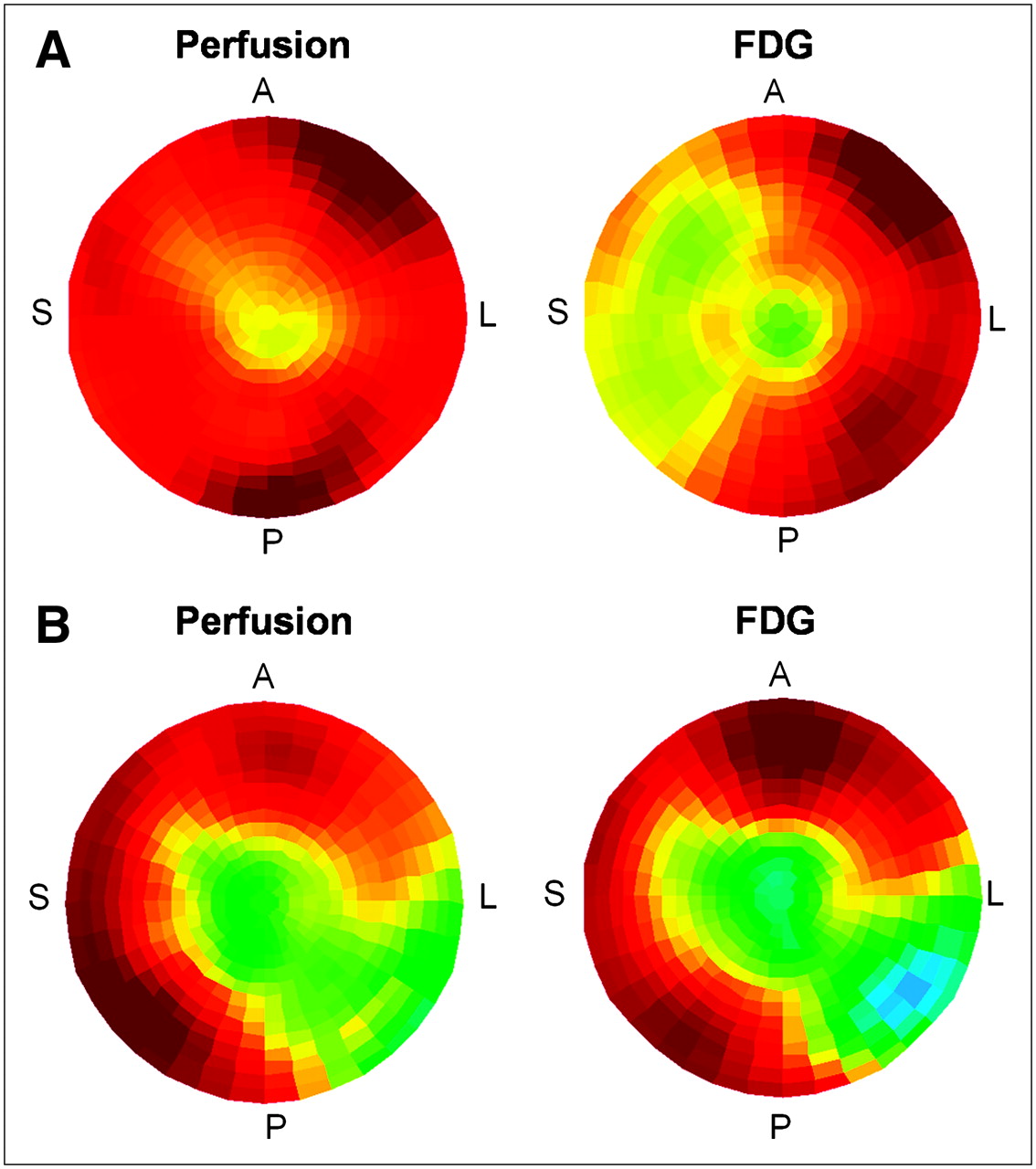
The mean uptake of 82Rb in the lateral wall was significantly reduced in patients with LBBB compared with control patients (79.0% ± 9.0% vs. 84.8% ± 7.5%; P < 0.05). This may reflect a greater amount of scar in the LBBB group, as the mean percentage of the lateral wall with scar for the control group was 4.9% ± 10.9% compared with 12.8% ± 12.7% for the LBBB group (P < 0.05). In the septum, there were no differences in perfusion between groups (LBBB = 83.1% ± 8.1% vs. control = 79.7% ± 10.9%; P = 0.32). There were also no differences in the scar score in the septum. Within each group, there were no significant differences in myocardial perfusion between the lateral and septal myocardial walls. However, there was a trend in the LBBB group (P = 0.07). The average septal wall 18F-FDG uptake was 64.0% ± 15.4% for the LBBB group, which was significantly reduced, compared with 74.9% ± 14.3% for the control group (P < 0.05). However, the mean 18F-FDG uptake in the lateral wall was not significantly different between patients with and without LBBB (P = 0.98). Figure 1 demonstrates example 18F-FDG and 82Rb polar maps for a typical patient with a septal R-MM score of >10% (Fig. 1A) and an R-MM score of ≤10% (Fig. 1B).

Examples of septal R-MM +ve (A) and R-MM −ve (B) polar images reflecting perfusion (82Rb) and 18F-FDG uptake across the myocardium. Red reflects maintained tracer uptake, whereas yellow and green reflect decreased tracer uptake. (A) Note reduced septal 18F-FDG uptake with maintained perfusion. (B) Note large lateral wall perfusion defect and corresponding relatively preserved septal wall perfusion and 18F-FDG uptake. A = anterior wall; S = septal wall; L = lateral wall; P = posterior wall.
R-MM Scores
The R-MM scores for the lateral and septal myocardial segments are shown in Figure 2. There was a significant difference between the LBBB and control groups in both segments. The R-MM score was greater in the septum of patients with LBBB (19.1% ± 15.3%) versus control patients (4.7% ± 10.6%; P < 0.01). Patients with LBBB (but not control patients) demonstrated significant differences in R-MM scores (P < 0.001) between the septum and the lateral wall.
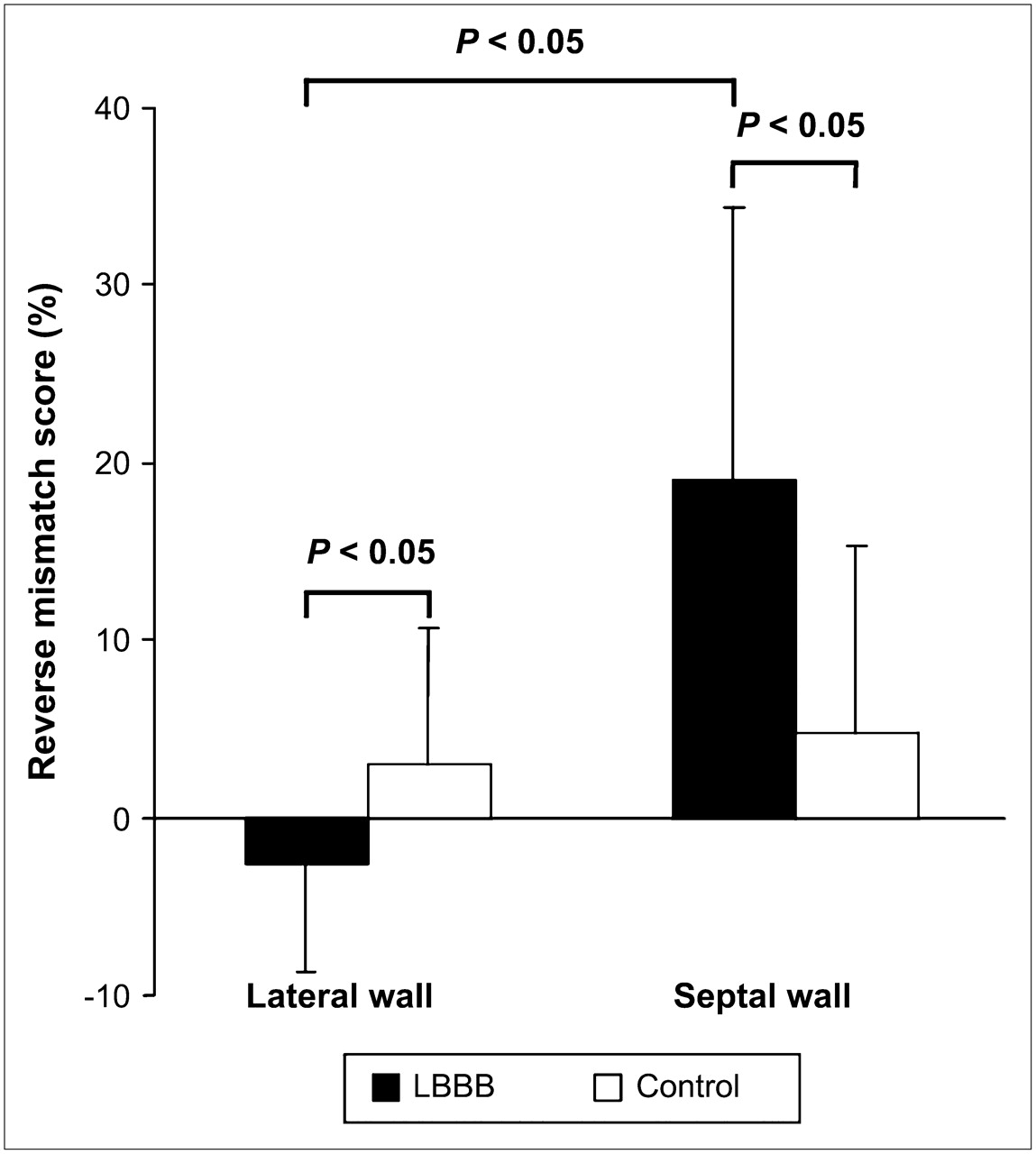
Septal and lateral wall R-MM scores in patients with ICM and LV dysfunction in LBBB and control groups.
Figure 3 demonstrates the relationship between the R-MM score and the QRS for all patients in the study. Among patients with LBBB, 23 of 34 (68%) demonstrated septal R-MM (>10%), whereas 11 of 34 (32%) did not. An almost uniform finding from previous studies in patients with IDC (i.e., nonischemic) is that almost 100% of patients with IDC and LBBB have R-MM (4,9,20). We, therefore, conducted further analyses to better characterize the patients with LBBB in the current study with and without R-MM.
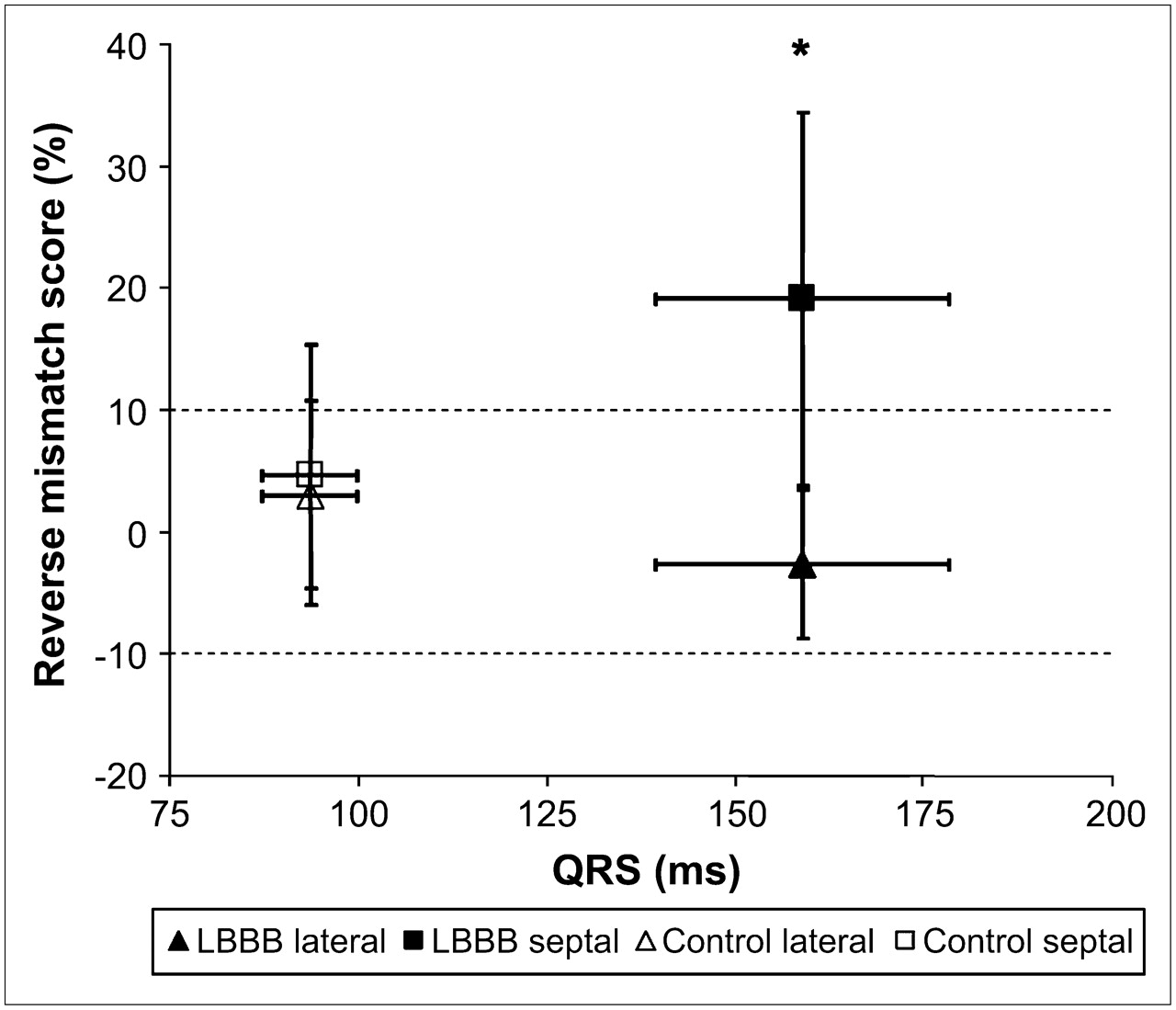
Mean R-MM score vs. mean QRS duration for control and LBBB lateral (triangles) and septal (squares) walls, with vertical and horizontal SD error bars. *P < 0.001 for LBBB septum vs. LBBB lateral wall, control septum, and control lateral wall.
Characterization of LBBB Population
The patients with LBBB and septal R-MM scores of >10% were considered R-MM +ve, whereas those with septal R-MM scores of ≤10% were considered R-MM −ve (27). Comparison of the mean 82Rb and 18F-FDG percentage uptake revealed significant differences in septal wall 18F-FDG and lateral wall 82Rb uptake (Fig. 4). Qualitative and semiquantitative analyses of the polar maps confirmed that all but one of the patients in the LBBB R-MM −ve group (91%) had a perfusion defect in the lateral wall compared with 48% of the patients in the LBBB R-MM +ve group (Table 2).
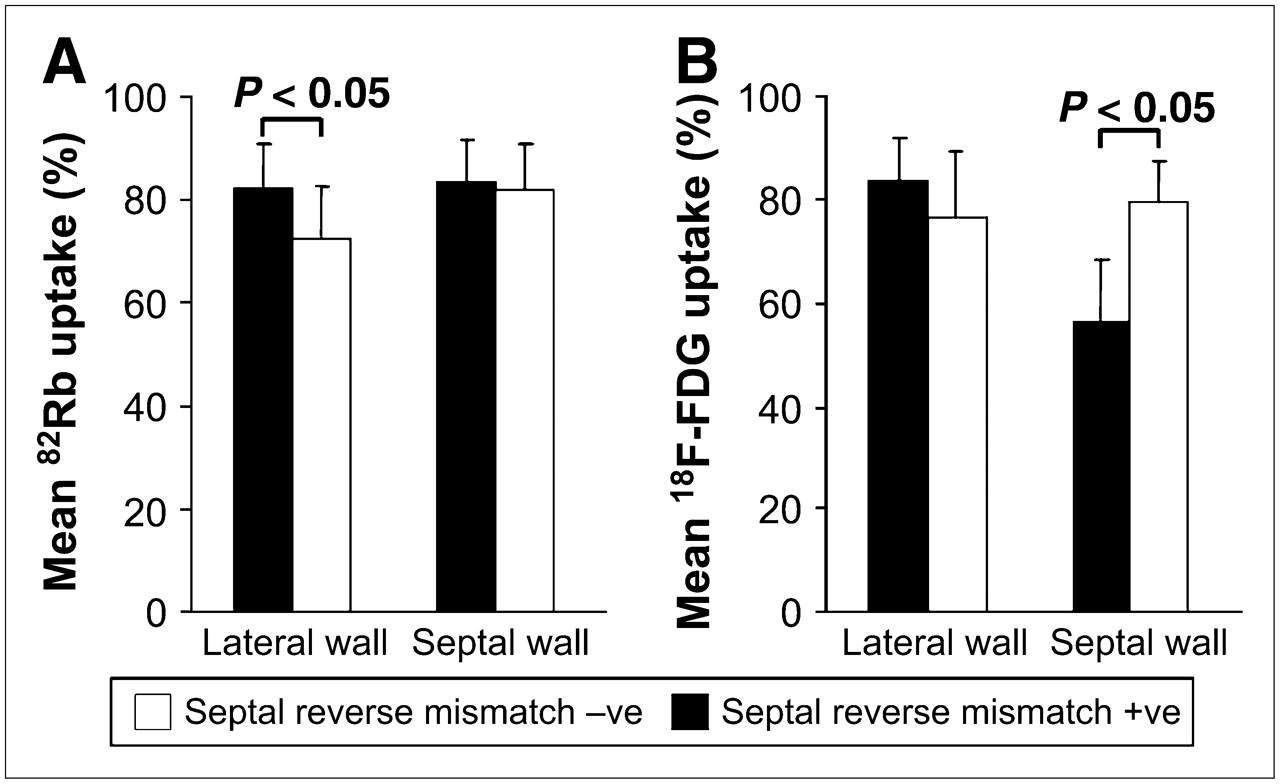
Lateral wall and septal wall mean 82Rb uptake (A) and 18F-FDG uptake (B) for LBBB R-MM −ve and +ve patients only.
Presence or Absence of Lateral Wall Defects in Patients with LBBB
The mean lateral wall scar score in the group of LBBB R-MM −ve patients was 19.9% ± 14.3% compared with 9.3% ± 10.5% in LBBB R-MM +ve patients (P < 0.05). There was no significant difference in the scar scores of the septal wall. However, there was a small, but significant, difference in the amount of hibernating myocardium (or mismatch) in the septum between the LBBB R-MM −ve and R-MM +ve groups (1.7% ± 4.2% and 0.0% ± 0.0%, respectively; P < 0.05). There was no difference in the amount of hibernating myocardium in the lateral wall between R-MM −ve and R-MM +ve groups. There were also no significant differences between the extent of scar in the other myocardial regions (anterior, inferior, apex) when the R-MM +ve and R-MM −ve LBBB subgroups were compared.
DISCUSSION
In the current study, patients with LBBB and ICM often demonstrate septal R-MM. However, this occurrence is not universal. Patients with LBBB without septal R-MM had significantly reduced perfusion in the lateral wall. There was also significantly increased 18F-FDG uptake in the septal wall of LBBB R-MM −ve patients compared with LBBB R-MM +ve patients. To our knowledge, this is the first study of its size to assess myocardial perfusion and metabolism in patients with IHD and LBBB compared with those patients with only IHD.
A small number of published reports have evaluated the effects of IDC and LBBB on septal myocardial function, flow, and metabolism (3,10,19,20). Significantly increased lateral wall perfusion and wall thickening relative to the rest of the ventricle, and in particular the septum, have been reported (10). In the current study, there were no significant differences in myocardial perfusion between the lateral and septal myocardium in either group. Significantly reduced 18F-FDG septal-to-lateral ratios have been reported in patients with LBBB and “no significant coronary stenosis” compared with non-LBBB patients (20). Similarly, this study reported reduced 18F-FDG uptake in the septum compared with the lateral wall in the LBBB group.
Septal R-MM was common (present in 68%) but was not a uniform finding in our study. LBBB R-MM +ve patients revealed significantly reduced septal wall 18F-FDG uptake compared with LBBB R-MM −ve patients. Concomitantly, 82Rb uptake was significantly decreased in the lateral wall of LBBB R-MM −ve patients. Almost all had a moderate-to-large perfusion defect. To our knowledge, these findings have not been reported elsewhere in the LBBB literature. Previously, in 2 case reports and a small study (n = 6) of patients with ICM and LBBB, septal R-MM was demonstrated in each individual (29–31).
The LBBB subgroup of patients with ICM but without R-MM and lateral wall defect demonstrates distinctively different findings. One hypothesis is that the lateral wall is no longer capable of adjusting its workload to compensate for the asynchronous septum because of the reduced perfusion. Thus, previously ineffective early septal wall contractions are crucial for systolic function when opposed by a hypoperfused lateral wall. With PET, this may manifest itself with decreased 82Rb uptake in the lateral wall and maintained 18F-FDG metabolism in the septum despite a LBBB.
With the emergence of CRT, many patients with LBBB are now being treated with biventricular pacing for their HF (32). A relative increase in septal 18F-FDG uptake compared with either baseline or a control population has been clearly demonstrated, which has been linked to improved LV function (4,9,33). However, a large proportion of patients receiving CRT (up to 50%) gains no benefit (6,11–17,34–36). The main factors impacting CRT response have been postulated as (a) the degree of LV dyssynchrony, (b) lead placement within the lateral wall, and (c) the degree of lateral wall scarring. All 3 factors can be markedly altered in the setting of ICM. Thus, it is not surprising to note that recent reports have suggested an association between the etiology of LBBB and the response to CRT (5,8,11,13,34,36–39). Recently, Bleeker et al. reported that patients with IHD, LBBB, and transmural posterolateral scar tissue were “nonresponders” after CRT (34).
In the current study, patients with LBBB, but without a R-MM, frequently exhibit decreased uptake of 82Rb in the lateral wall. We hypothesize that this could drive the septal metabolic demand in some patients such that the septum is contributing more to forward stroke work of the LV. These patients may not respond to the benefits of CRT but this notion remains speculative and requires further study. It is also conceivable that the presence of R-MM may indicate a metabolic imbalance due to the conduction delay and thus reflect a degree of metabolic reserve in the septum with potential for recovery after CRT. Alternatively, the extent of scar in the lateral wall may be the more important factor, countering any metabolic reserve in the septum (8,11,37,39). This too remains speculative and requires further study.
These previous studies, as well as the current study, highlight the need for a comprehensive understanding of the pathophysiology of all etiologies of LBBB, and in particular that of ICM. The rate of nonresponse to CRT is high, particularly in patients with ICM. We have found a distinct difference between patients with ICM and IDC, in that septal R-MM can no longer be considered pathognomonic for LBBB. This is most likely due to the lateral wall scar described in the current study as well as in the study of Bleeker et al. (34). Consequently, this may contribute to the large CRT nonresponder rate in patients with ICM and is likely also the reason for the lack of septal R-MM. Currently, there is still much to be discerned in the setting of ICM and LBBB. PET may prove to be a useful tool not only for uncovering these ambiguities but also for screening patients before CRT.
These data are limited by the lack of a direct measure of LV function and the phase of contraction. Unfortunately, wall motion studies were often not available for the patients included in this study—patients either did not get a wall motion study or were referred from another center. Besides the obvious differences related to LBBB, our patients with LBBB also had a greater amount of lateral wall scar than control patients, although other parameters were comparable. Larger studies will be required to determine if this is true in other LBBB populations.
Future studies are planned to assess the utility of defining R-MM for predicting response to CRT. The R-MM parameter may be useful in this regard but may also have limitations. Specifically, like any cutoff parameters, patients near the cutoff may be inappropriately categorized. Likewise, whereas these R-MM patterns tend to encompass most or all of the septum, this does not necessarily match the artificial boundaries of the septum segment. This could lead to slight overestimation or underestimation of the R-MM score. Normalization to a perfusion defect could also affect the R-MM score but this is unlikely unless there is an extensive perfusion defect. Future prospective studies will need to consider these limitations.
We included only those patients meeting specific LBBB criteria to determine the specific septal metabolism alterations in this condition. The cohort of patients with mixed intraventricular conduction-delay abnormalities has not been included in the current study. Lastly, the study was not intended to evaluate clinical outcomes. This will be addressed in future work.
CONCLUSION
Altered septal glucose metabolism, reflected by a R-MM pattern on PET, is common in patients with IHD, LV dysfunction, and LBBB. However, this phenomenon is not universal, with >30% of patients not exhibiting septal R-MM. More than 90% of patients with LBBB, but without R-MM, have a lateral wall perfusion defect. Further studies are needed to fully elucidate the mechanism, as well as the disparity, of septal metabolism alterations in patients with LBBB and to determine whether such alterations can help predict the therapeutic response.
Acknowledgments
The authors thank Sherri Nipius, Deborah Gauthier, Michaela Garkisch, Mary Ann Maclean, May Aung, Kim Gardner, Ran Klein, Samantha Mason, and Kathy Menchini for their administrative, nursing, and technical expertise and assistance. This study was supported in part by grant MCT 37412 from the Canadian Institute for Health Research (CIHR) (Ottawa, Ontario, Canada), grant 5222 from the Heart and Stroke Foundation of Canada (Ottawa, Ontario, Canada), and grant 00 May 0710 from the Ontario Research and Development Challenge Fund (Toronto, Ontario, Canada). Additional support includes Studentships from the Heart and Stroke Foundation of Ontario, the University of Ottawa International Fellowship, the Toronto Dominion Bank Fellowship Program (Toronto, Ontario, Canada), and the CIHR Research Scientist Award Program.
Footnotes
-
COPYRIGHT © 2006 by the Society of Nuclear Medicine, Inc.
References
- Received for publication May 2, 2006.
- Accepted for publication August 1, 2006.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- 2013 ACCF/ACR/ASE/ASNC/SCCT/SCMR Appropriate Utilization of Cardiovascular Imaging in Heart Failure: A Joint Report of the American College of Radiology Appropriateness Criteria Committee and the American College of Cardiology Foundation Appropriate Use Criteria Task Force
- Effects of Left Bundle Branch Block and Right Ventricular Pacing on Assessing Myocardial Viability by Positron Emission Tomography