


Abstract
Plantar fasciitis is a common cause of foot pain and may be disabling. Although localized injection is painful, anesthetics or corticosteroids can relieve symptoms well. Bone scintigraphy can confirm the diagnosis. We hypothesized that blood-pool abnormalities could provide prognostic information on the response to such injections. Methods: We devised scintigraphic criteria that graded the blood-pool abnormalities as being localized to the plantar enthesis, being localized to half the length of the aponeurosis, or involving the whole aponeurosis. We evaluated 24 patients with an established diagnosis of plantar fasciitis, 8 of whom had bilateral disease, leading to a total of 32 feet injected. Results: After injection, pain was relieved either completely or nearly completely in 20 feet. The other 12 feet had short-term or no improvement, with persistent pain and loss of function at 4–5 wk after injection. Of the 20 feet responding to injection, 14 had focal hyperemia on blood-pool images and 6 had minimal extension into the proximal third of the plantar soft tissues. No patient with diffuse hyperemia in the plantar fascia had a response (5/12 feet). On the delayed images of the 20 responders, mild inferior calcaneal uptake was seen in 8 feet, moderate uptake in 6, and severe uptake in 6. These groups did not significantly differ (P > 0.05). The blood-pool studies had good reproducibility, with a κ-value of 0.64. Conclusion: Critical evaluation of plantar blood-pool images provides prognostic information on the response to localized injection into the enthesis. Reporting such studies is simple and reproducible.
Plantar fasciitis is the most common cause of heel pain, reportedly accounting for 11%–15% of all patients with foot pain who present for medical care (1–3). In the sporting population, the condition has been reported to account for 10% of all injuries in runners (2). The incidence peaks between the ages of 40 and 60 y in the general population and earlier in runners, and approximately one third of cases are bilateral (3). Plantar fasciitis patients represent a sizable population that presents for medical care. The differential diagnosis of heel pain can vary widely, encompassing Achilles' tendonitis, retrocalcaneal bursitis, subtalar joint abnormalities, and fractures of the calcaneum.
Bone scanning has been useful in the identification and evaluation of plantar fasciitis (4), with the scans showing the specific appearance of delayed uptake at the common calcaneal insertion of the plantar aponeurosis and flexor digitorum brevis (Fig. 1A) (5–8). Bone scintigraphy has also been shown to be an accurate guide in selecting the injection site for therapeutic corticosteroids or local anesthetics (9). The importance of the early blood-pool phase of bone scintigraphy has been alluded to as a diagnostic feature of plantar fasciitis (10,11), with no implications for therapy being drawn from the results. Clinical observation led us to hypothesize that the extent of the blood-pool abnormalities may have an inverse relationship with the success rate of corticosteroid/local anesthetic injection in abolishing symptoms. The anatomic basis of the hypothesis was explored by the dissection of 2 cadaveric feet.
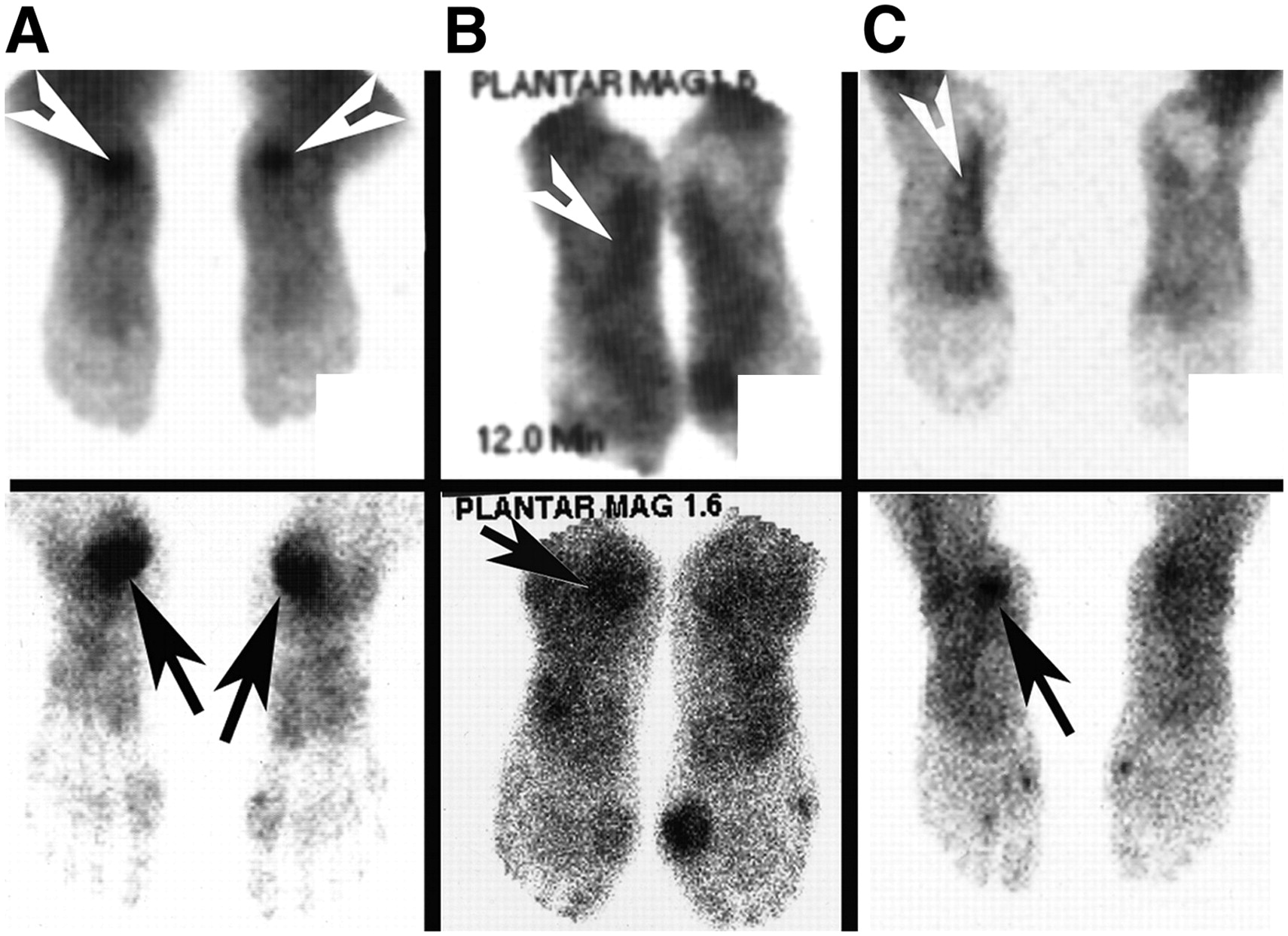
Scan classification showing blood-pool phase at top and delayed phase at bottom: focal hyperemia in plantar fascia and marked delayed uptake in inferior calcaneum (A), hyperemia in proximal third and mild delayed uptake (B), and diffuse hyperemia and moderate delayed uptake. Arrowheads indicate hyperemia; arrows indicate delayed uptake.
MATERIALS AND METHODS
Patient Population
Twenty-four patients (14 women and 10 men; mean age, 42 y; range, 19–55 y) were extracted from a database of patients with various orthopedic and rheumatologic conditions that was created with the approval of the Concord Hospital Ethics Committee. The group comprised consecutive patients in whom plantar fasciitis had been diagnosed on the basis of history and bone scintigraphy findings and who were treated by local injection of steroids or anesthetics. Heel pain had been present for 4–6 wk in 8 patients (10 feet), 6 wk to 3 mo in 7 (11 feet), and more than 3 mo in 9 (11 feet).
Scans from another 10 patients with conditions other than plantar fasciitis were randomly selected and added to the evaluation to test the specificity of the scintigraphic criteria for plantar fasciitis and the interobserver variability of these criteria.
Patients received a mixture of methylprednisolone and bupivacaine injected by the medial approach into the inferior calcaneum. Responses to the injection were canvassed at 4–5 wk as either complete/nearly complete (allowing a return to normal activities) or not. Our previous experience with scaled pain-response surveys had demonstrated poor reproducibility and unreliability, leading to the adoption of the simpler binary system (12).
Scanning Methods
All patients received a 900- to 1,000-MBq injection of 99mTc-methylene diphosphonate, and blood-pool images of the plantar aspect of both feet were obtained at 3–5 min for 3–5 min per image. Delayed images of the anterior, posterior, lateral/medial, and plantar aspects of the feet were acquired at 3 h. Each image was acquired for 7 min without magnification, using a high-resolution collimator fixed to either a Millennium or a 400AC γ-camera (GE Healthcare) interfaced to a computer. Images were displayed on hard-copy film and were submitted for reporting with the patient names masked.
Reporting Criteria
To evaluate abnormalities of the blood-pool phase, we devised a system characterizing them as focal calcaneal hyperemia, extension into the proximal third of the plantar fascia, diffuse involvement of the plantar fascia, or no evidence of hyperemia within the plantar fascia (Fig. 1). The delayed images were classified as showing no calcaneal uptake or as showing mild, moderate, or marked uptake. The findings on combined blood-pool and delayed images were classified using 5 categories: no focal or diffuse hyperemia and mild to marked, or absence of, delayed calcaneal uptake; focal hyperemia and mild to marked delayed uptake; proximal hyperemia and mild to marked focal delayed uptake; diffuse hyperemia in the plantar fascia and mild to marked delayed uptake in the calcaneum; and uptake not characteristic of plantar fasciitis. These were independently scored by 2 nuclear medicine physicians after they had together examined a training set of 6 scans to establish a common understanding of the classifications.
Statistical Analysis
The response to injection of steroids or local anesthetics was analyzed as a percentage of the total number of patients injected. For each group of blood-pool, delayed, and combined-scan abnormalities, the percentage of feet responding and the duration of symptoms were assessed by the Fisher exact test for categoric variables (2-tailed) (13). The interobserver variability of reporting was measured by the κ-statistic (14), which is defined as 0 for interobserver agreement no better than chance and as 1 for perfect agreement. Values of 0.21–0.40 indicate fair agreement; 0.41–0.60, moderate agreement; 0.61–0.80, good agreement; and 0.80–1.0, very good agreement. All statistical analysis was performed on MedCalc (version 4.20.011; MedCalc Software) for Windows (Microsoft).
Human Dissection
Two embalmed feet were dissected from a medial approach in which the plantar skin and fibrous and fatty tissue were removed to reveal the plantar aponeurosis. The plantar aponeurosis was then carefully dissected away from the fibrous sheath around the flexor digitorum brevis to explore the relationship between the 2 structures. Digital photographs of the specimens were obtained for purposes of illustration.
RESULTS
Patient Response to Injection
Of the 24 patients with an established diagnosis of plantar fasciitis, 8 had bilateral disease, leading to a total of 32 feet injected. After injection, pain was relieved either completely or nearly completely in 20 feet. The other 12 feet had short-term or no improvement, with persistent pain and loss of function at 4–5 wk after injection. Patients with symptoms for less than 6 wk had a response rate (8/10 feet) that was not significantly different (P > 0.05) from the response rates of the other 2 groups (6/11 and 6/11 feet), with symptoms for 6 wk to 3 mo and more than 3 mo, respectively.
Scan Findings
The scan findings are summarized in Table 1. Of the 20 feet responding to injection, 14 showed focal hyperemia on blood-pool images and 6 showed minimal extension into the proximal third of the plantar soft tissues. No patient with diffuse hyperemia in the plantar fascia had a response (5/12 feet). Responders with focal hyperemia did not significantly differ from responders with minimal extension (P = 0.023). A significant difference was found between patients with focal hyperemia and diffuse blood-pool abnormalities (P = 0.004). No significant difference was found between the group with extension of blood-pool abnormalities into the proximal fascia and diffuse changes (P > 0.05). On the delayed images of the 20 responders, mild inferior calcaneal uptake was seen in 8 feet, moderate uptake in 6, and severe uptake in 6. These groups did not significantly differ (P > 0.05). When scans were combined, 13 of the 14 feet with focal calcaneal hyperemia and focal uptake responded to therapy.
Clinical Results vs. Scan Findings
Reproducibility of Reporting
The blood-pool studies had good reproducibility, with a κ-value of 0.64 (95% confidence interval [CI], 0.51–0.78). Agreement on reporting the delayed images was also good, with a κ-score of 0.66 (95% CI, 0.53–0.80). Reporting the combined studies showed only fair interobserver agreement (κ = 0.55; 95% CI, 0.40–0.69).
Cadaveric Studies
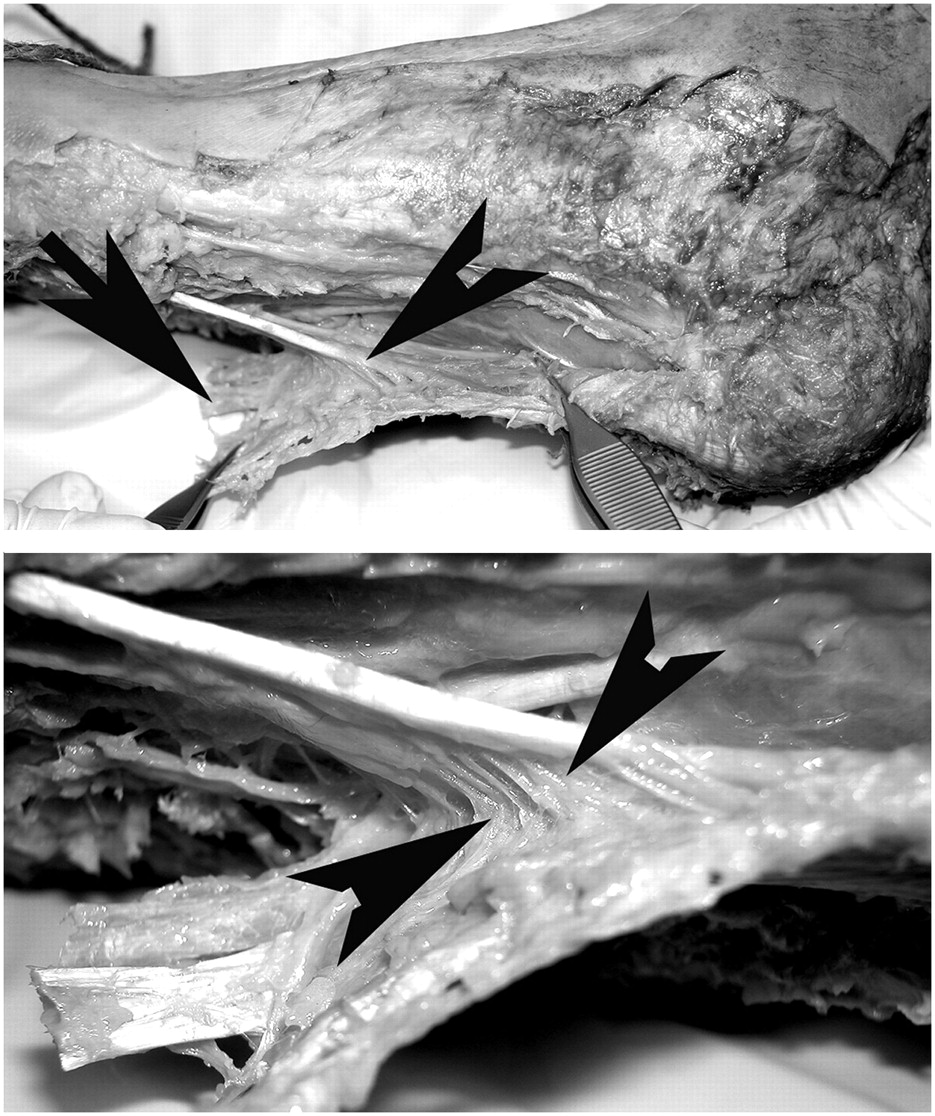
The muscle fibers of the flexor digitorum brevis are attached to the deep surface of the plantar aponeurosis. This tight adherence extends from the level of the calcaneal enthesis to the proximal third of the plantar aponeurosis, almost to the point where the muscle divides into its 4 fascicles (Fig. 2). This muscular attachment that anchors the plantar aponeurosis is so strong that only sharp dissection can separate the latter from the muscle (Fig. 3).
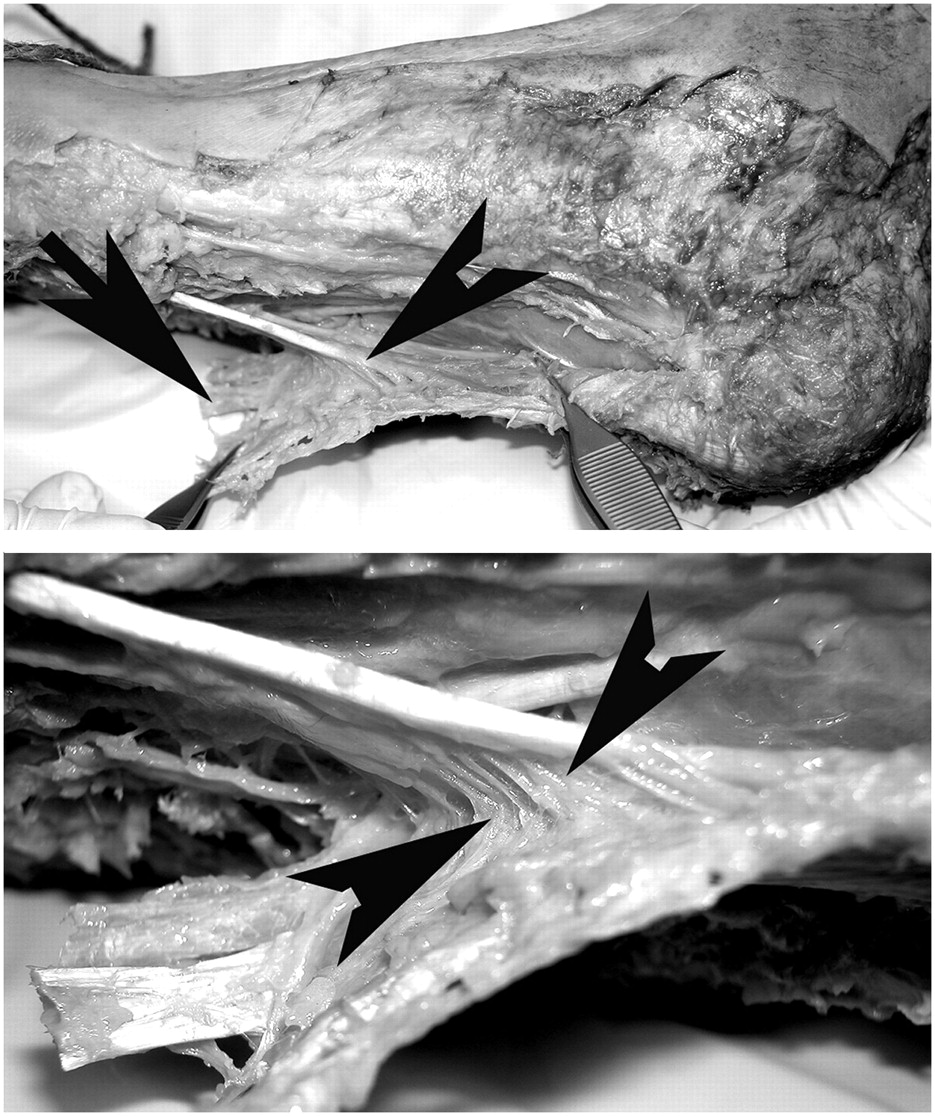
Muscle fibers of flexor digitorum brevis are attached to deep surface of plantar aponeurosis (arrowheads). This tight adherence extends from level of calcaneal enthesis to proximal third of plantar aponeurosis, almost to point where muscle divides into its 4 fascicles (arrow).
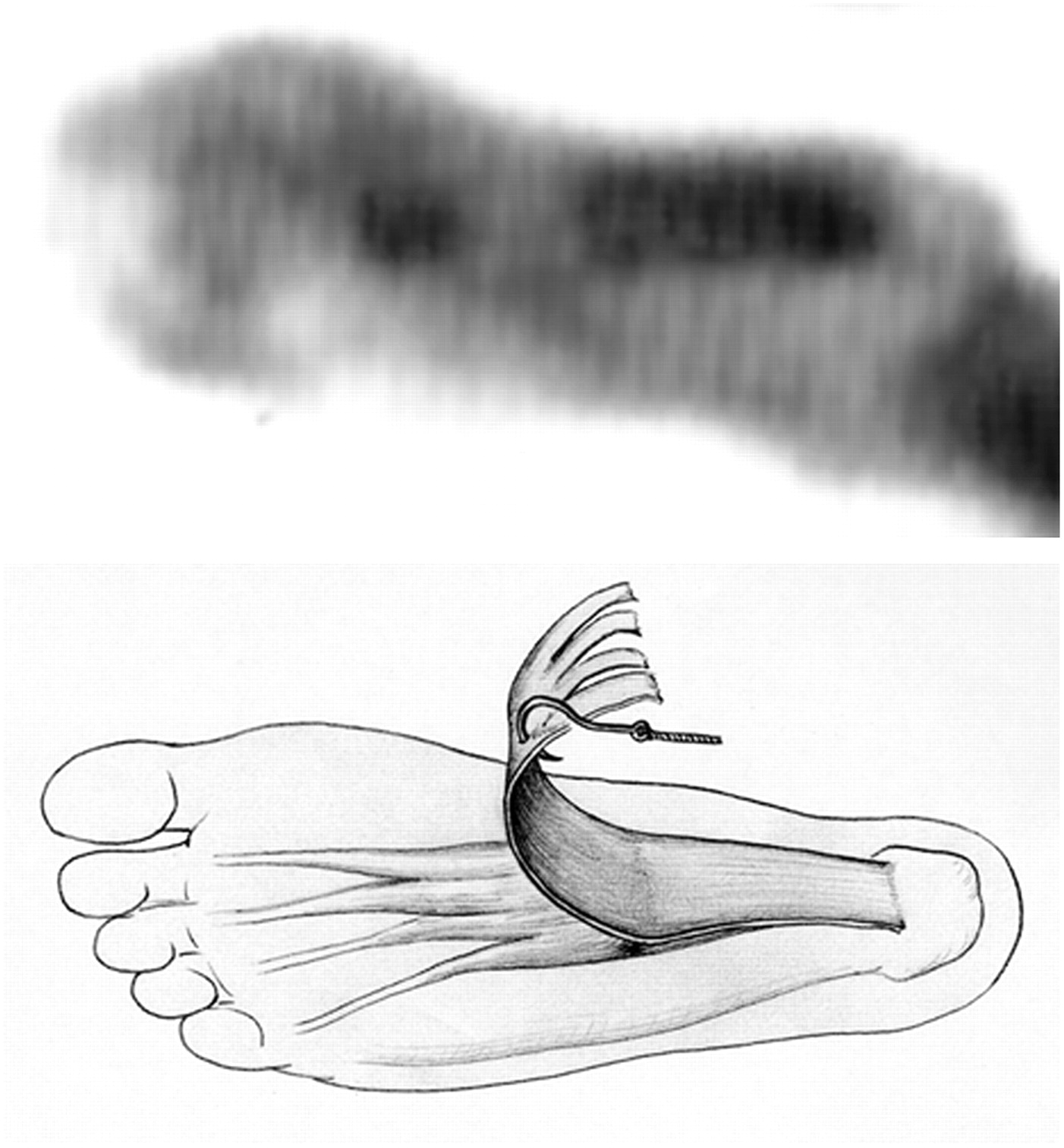
Blood-pool scan of hyperemia in proximal third of plantar fascia and corresponding anatomic illustration of tight adherence of plantar aponeurosis to flexor digitorum brevis, almost to division of muscle. Distal plantar aponeurosis reflects this relationship more clearly.
DISCUSSION
Plantar fasciitis is a common and sometimes difficult problem to treat by conservative measures such as physical therapy, orthotic devices, or injection with corticosteroids or local anesthetics (3). A recent review noted that the natural history of the disease was self limiting within 12 mo in more than 80% of patients, regardless of the type of treatment. Approximately 5% of patients required surgical intervention when symptoms persisted for more than 6–12 mo (3). A single study examined outcomes in 91 patients treated with corticosteroids or local anesthetics or by local anesthetic injection alone by a medial approach (15). No difference was found between the 2 treatments at 3 and 6 mo using a visual analog pain score. However, the rate of patient dropout was high. Regardless of these results, injection of corticosteroids or local anesthetics remains a convenient form of therapy, particularly as it is quick and may be performed as an office procedure.
The diagnosis of plantar fasciitis is empiric and based on a history of heel pain that is worse in the morning. This pain generally lessens with activity and is associated with point tenderness over the anteromedial aspect of the inferior calcaneum. In most cases, a bone scan is obtained to confirm the diagnosis and to guide the injection of corticosteroids or local anesthetics (9). Our results confirmed an additional predictive role for the bone scintigram. Focal calcaneal hyperemia is clearly associated with a high success rate for injection, with extension of hyperemia into the proximal soft tissues being associated with a response in only 50% and diffuse hyperemia with no response. Similar diagnostic findings have also been noted with MRI, which shows high T2 signal intensity both at the calcaneal enthesis and along the proximal third of the plantar soft tissues (16,17). Data on MRI have been only descriptive, with no prognostic role being defined. Just as important, the presence of diffuse hyperemia throughout the plantar fascia is highly predictive of a lack of response to injection. Unlike other groups (18,19), and possibly reflecting the small number of patients in our study, we did not find that a short duration of symptoms was a predictor of response to therapy. Regardless of the intensity of uptake, the pattern of delayed uptake did not predict response to or failure of therapy.
Operative specimens show histologic evidence of degenerative changes in the plantar fascia and chronic inflammatory changes with or without fibroblastic proliferation (20,21). The chronic inflammatory changes may explain the limited response to corticosteroid injection around the enthesis. Although the literature helps define an inflammatory component, it does not define the extent to which the inflammation extends throughout the plantar fascia.
Observations from MRI and bone scan findings do suggest a more extensive inflammatory change spreading from the enthesis into the soft tissues of the plantar fascia. If this is the case, it may indicate more extensive disease, which for anatomic or pathologic reasons may not allow the penetration of localized corticosteroids from around the enthesis into the more distal reaches of the plantar tissues. Our anatomic findings in cadaveric feet provide ample evidence that little penetration occurs. This evidence is supported by the observations of other workers that the proximal third of the plantar aponeurosis is tightly adherent to the flexor digitorum brevis, such that there is no potential space between them (22). Only sharp dissection can detach this muscular anchoring of the plantar aponeurosis. Histologic evidence supports both an inflammatory and a fibroblastic response that may increase the density of the plantar aponeurosis and its adherence to the overlying fibrovascular sheath of the flexor digitorum brevis. Such a barrier would allow only limited egress of a viscous fluid injected around the enthesis, as our results showed. The option of infiltrating the entire plantar fascia in such cases would be prohibitively painful and poorly tolerated, this being one of the reasons why the plantar approach to injection has been eschewed in favor of the medial approach.
CONCLUSION
Plantar fasciitis is a common condition that is often treated with the injection of corticosteroids or local anesthetics around the calcaneal enthesis. We present scintigraphic criteria that can help identify potential responders, thereby avoiding unnecessary injection in a significant proportion of patients. The blood-pool phase is predictive of response, with the pattern of delayed uptake not adding incremental prognostic information.
Footnotes
-
COPYRIGHT © 2006 by the Society of Nuclear Medicine, Inc.
References
- Received for publication April 23, 2006.
- Accepted for publication July 6, 2006.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.