


Abstract
This study determined the role of the combined use of 99mTc-sestamibi and 99mTc-pentavalent dimercaptosuccinic acid (V-DMSA) scintigraphy in evaluating the effectiveness of chemotherapy in patients with multiple myeloma. Methods: In 20 patients with multiple myeloma who had received or were receiving chemotherapy, 99mTc-sestamibi and 99mTc-V-DMSA scanning was performed to evaluate the effectiveness of chemotherapy. Results: In group A (11 patients with active disease), 42 99mTc-sestamibi–positive lesions were found. Thirty-seven of those lesions were also positive for 99mTc-V-DMSA uptake, as were 16 additional lesions (nonactive) (NAL). Thus, in group A, the total number of positive lesions (TPL) detected was 58 and the NAL/TPL ratio was 16:58. In group B (9 patients in remission), 5 99mTc-sestamibi–positive lesions were found. A further 22 lesions were also positive for 99mTc-V-DMSA uptake. Thus, in group B, the NAL/TPL ratio was 22:27. Therefore, the NAL/TPL ratios considered to represent effectively treated lesions were 27.6% and 81.5% for groups A and B, respectively. Conclusion: Combined use of the 2 agents allows the effectiveness of chemotherapy to be evaluated through a comparison of NAL and TPL multiple myeloma lesions even in the absence of a baseline study.
Multiple myeloma (MM) is a neoplastic disease characterized by the proliferation of monoclonal myeloma cells that seed throughout the bone marrow. Standard diagnostic imaging methods, such as skeletal radiography and bone scanning, have certain limitations for detecting the presence and extent of bone disease for staging and particularly for following up patients with MM.
The usefulness of follow-up 99mTc-sestamibi (MIBI) scanning in detecting active disease in patients with MM is well established. Uptake of 99mTc-MIBI has been reported as correlating well with the degree of bone marrow MM involvement, in particular when used in the follow-up of treated patients with already documented bone lesions (1–4). However, if baseline data are not available it is not possible to estimate the chemotherapy effect using a single 99mTc-MIBI examination.
99mTc-Pentavalent dimercaptosuccinic acid (V-DMSA) has been shown to concentrate in some tumors (5,6), including MM (7,8), as well as in inflammatory conditions such as osteomyelitis (5), psoas muscle abscess (9), bone and joint infection (10), intestinal inflammation (11), and active inflammatory bowel disease (12) in which several cell types, such as macrophages, histiocytes, and fibroblasts, are present.
Effective chemotherapy dramatically reduces viable MM cells because of apoptosis. We hypothesize that unlike 99mTc-MIBI, 99mTc-V-DMSA will continue to concentrate in MM lesions after chemotherapy because of factors other than viable MM cells such as macrophages. Thus, we believe that a relatively increased 99mTc-V-DMSA uptake, compared with 99mTc-MIBI uptake, should be a good index of chemotherapy effectiveness.
The aim of the study was to determine the role of the combined use of 99mTc-MIBI and 99mTc-V-DMSA scintigraphy in the evaluation of chemotherapy effectiveness in patients with MM.
MATERIALS AND METHODS
Patients
Twenty MM patients (11 women and 9 men) with a mean age of 63 y (range, 26–87 y) were included in the study. All patients had received or were receiving chemotherapy. The onset of the disease ranged from 1 to 70 mo (mean ± SD, 25 ± 23 mo) before the study. The criteria of Salmon and Durie were used for initial staging of tumor burden, and the staging system of Bataille was used for disease activity. Eleven patients (group A) had clinically active disease, and 9 patients (group B) had disease that was in complete or partial remission (at least a 50% decrease in M protein in serum or urine).
Fifteen patients were receiving chemotherapy: 11 of 11 from group A and 4 of 9 from group B. The remaining 5 of 9 patients from group B had undergone chemotherapy between 5 mo and 2.5 y before the study. The conventional chemotherapy that was administered was vincristine, doxorubicin, and dexamethasone or pegylated doxorubicin, vincristine, and reduced-schedule dexamethasone. Various combination therapies were also used as salvage therapies. Thalidomide, an oral agent, was also often used as salvage therapy for myeloma patients, alone or in combination with dexamethasone or melphalan and dexamethasone. One to 6 therapies (2.8 ± 1.9) were administered to group A patients and 1–3 therapies (1.9 ± 0.8) to group B patients (P = not statistically significant [NS]). The duration of remission in group B was 1–30 mo.
Imaging
The 99mTc-MIBI (Cardiolite; Bristol Myers Squibb GmbH) was prepared according to the manufacturer’s instructions. Each patient received 666 MBq of 99mTc MIBI intravenously, and the scans were obtained 10 min after injection. 99mTc-V-DMSA was prepared using a commercially available kit (DMS(V)/Demoscan; National Center of Physical Sciences, Institute of Radioisotopes and Radiodiagnostics “Democritus”), 740 MBq were injected intravenously, and 2 h later the scintigrams were obtained. The studies were performed at intervals of at least 48 h to avoid carryover of image data and, for patients who were receiving chemotherapy, were performed in the middle of a chemotherapy cycle (ninth–12th posttherapy days). All scintigrams were obtained on a single-head tomographic γ-camera (Sophycamera DS7; Sopha Medical Vision International) coupled to a dedicated NXT computer system (Sophy NxT; Sopha Medical Vision International). Spot images of the whole body were obtained with a low-energy all-purpose collimator using a 20% window centered at 140 keV.
Two experienced nuclear medicine physicians unaware of the patient’s disease status, disease stage, and other clinical data reported scintigraphic findings. The 99mTc-MIBI findings were classified as pattern N when only normal physiologic uptake was present, pattern D when diffuse bone marrow uptake was present, pattern F when areas of focal uptake were present, or pattern F + D when both patterns were present. The presence of focal increased 99mTc-V-DMSA activity was characterized as a positive finding. Disagreement was resolved by consensus or by obtaining a third opinion.
Statistical Analysis
The 2-tailed Mann–Whitney nonparametric test was used to evaluate differences. P values < 0.05 were considered statistically significant.
RESULTS
An overview of the patients, their disease, and scintigraphic data are summarized in Tables 1 and 2.
Group A: Patient Data and Scintigraphic Results
Group B: Patient Data and Scintigraphic Results
There was no statistically significant difference either in the time from onset of the disease in the 2 groups, which ranged from 1 to 60 mo before the study (27 ± 25 mo) in group A and from 5 to 70 mo (23 ± 21 mo) in group B, or in the number of therapies they had received. No correlation was found in efficacy among different chemotherapy regimens.
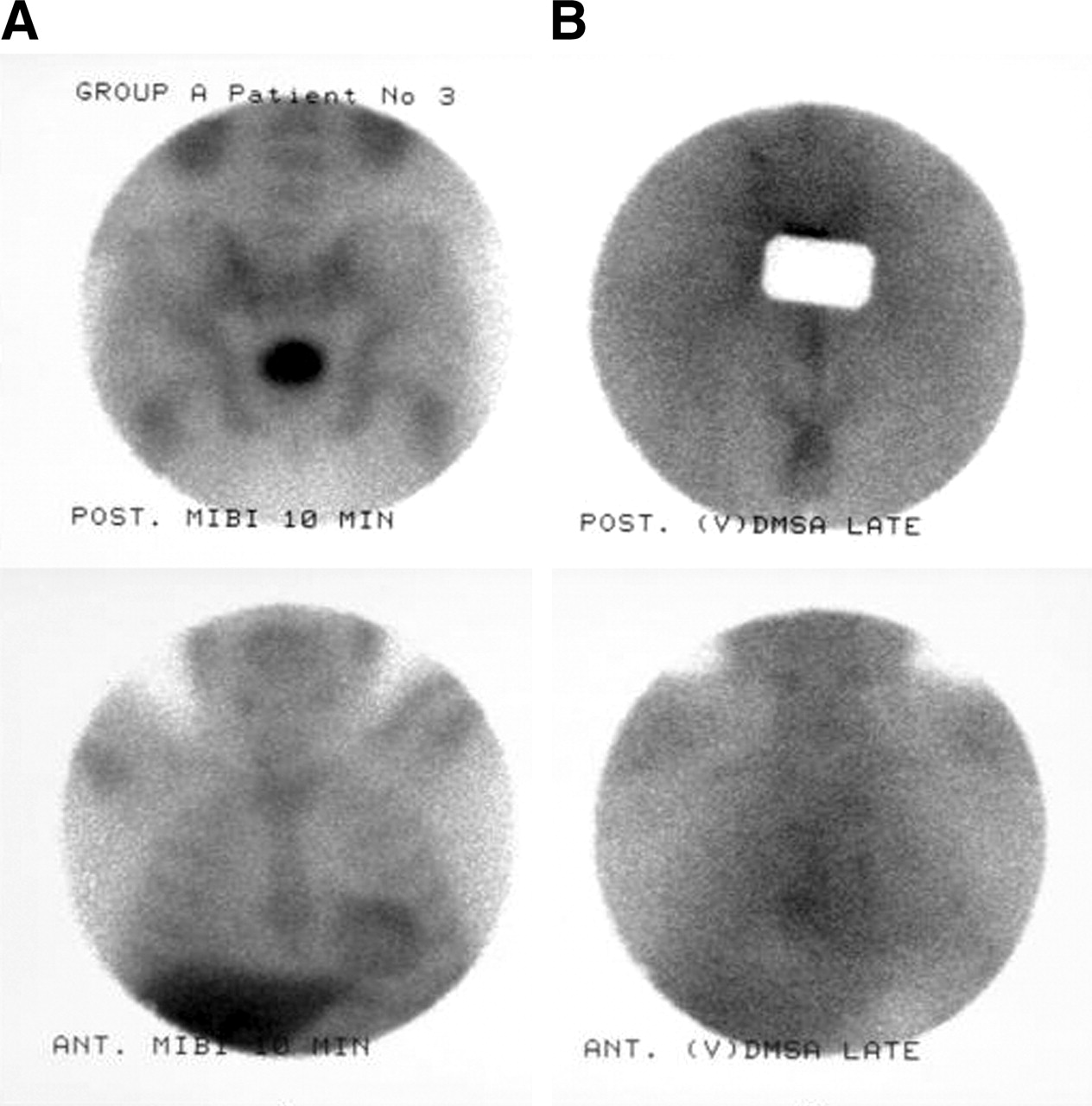
Of the 11 patients from group A, 4 patients showed a diffuse pattern of 99mTc-MIBI uptake (Fig. 1). Focal areas of 99mTc-MIBI uptake were the only pathologic finding in 4 patients and were combined with a diffuse pattern of bone marrow uptake in 3 patients. 99mTc-V-DMSA findings were focally positive in 8 patients, and 3 patients had normal 99mTc-V-DMSA findings.
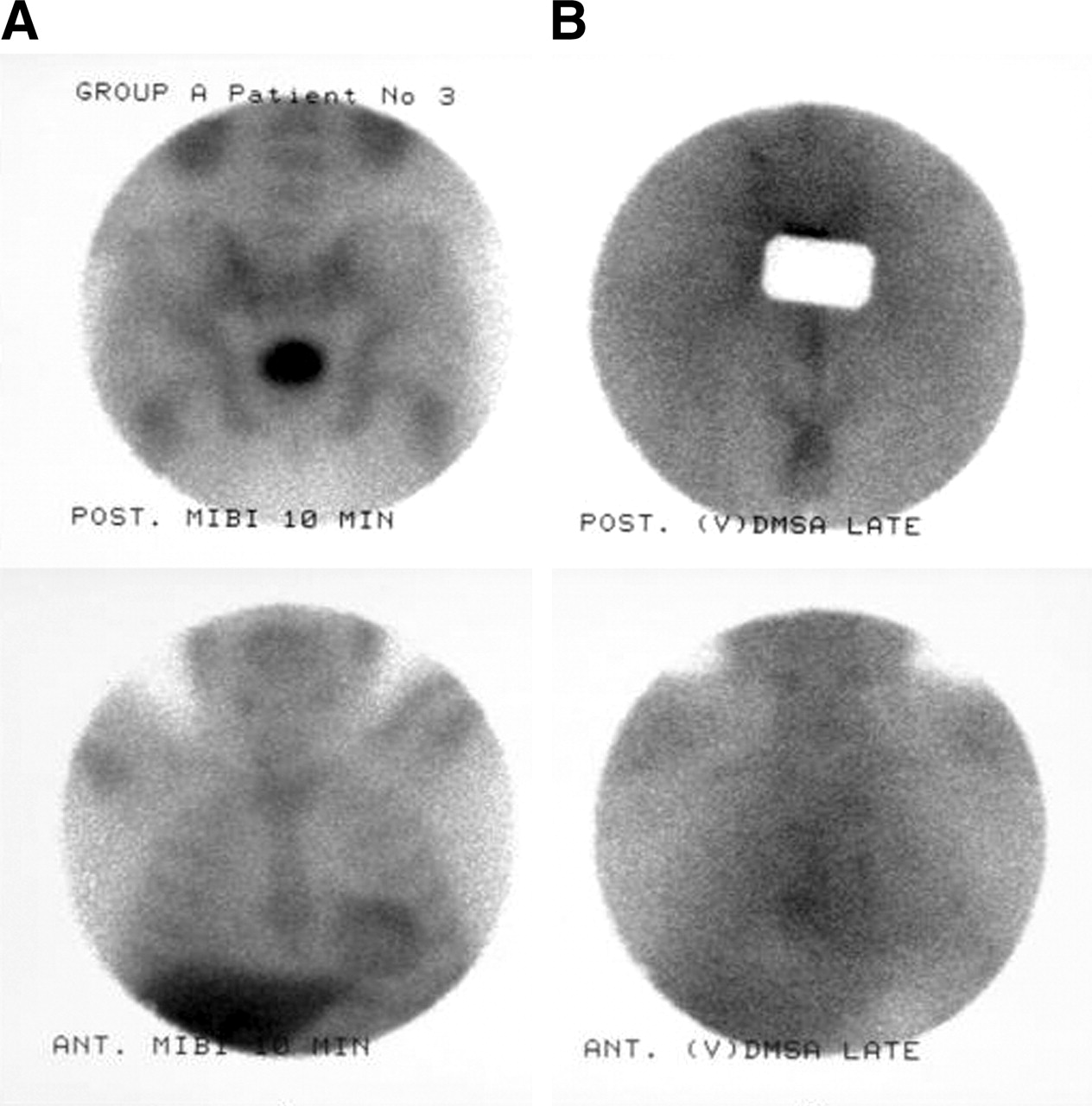
Patient 3 from group A, with diffuse pattern of 99mTc-MIBI findings (A) and negative 99mTc-V-DMSA findings (B). At top is posterior view of pelvis; at bottom is anterior view of thorax. NAL/TPL ratio = 0.
In group B, 6 patients had normal 99mTc-MIBI findings and 3 patients showed focal areas of uptake. 99mTc-V-DMSA findings were focally positive in 8 patients.
The total number of 99mTc-MIBI–positive or 99mTc-V-DMSA–positive lesions (TPL) was determined. Lesions that were 99mTc-V-DMSA–positive but 99mTc-MIBI–negative were considered to be nonactive lesions (NAL). The NAL/TPL ratio was calculated for both groups.
In group A, 42 99mTc-MIBI–positive lesions were found. Thirty-seven of those lesions were also positive for 99mTc-V-DMSA uptake, as were 16 additional lesions that did not accumulate 99mTc-MIBI (Fig. 2). Thus, a total of 58 MM lesions were detected. In group B, 5 99mTc-MIBI–positive lesions were found, all of which were also positive for 99mTc-V-DMSA uptake, as were 22 additional lesions that did not accumulate 99mTc-MIBI (Figs. 3 and 4). Thus, a total of 27 MM lesions were detected.

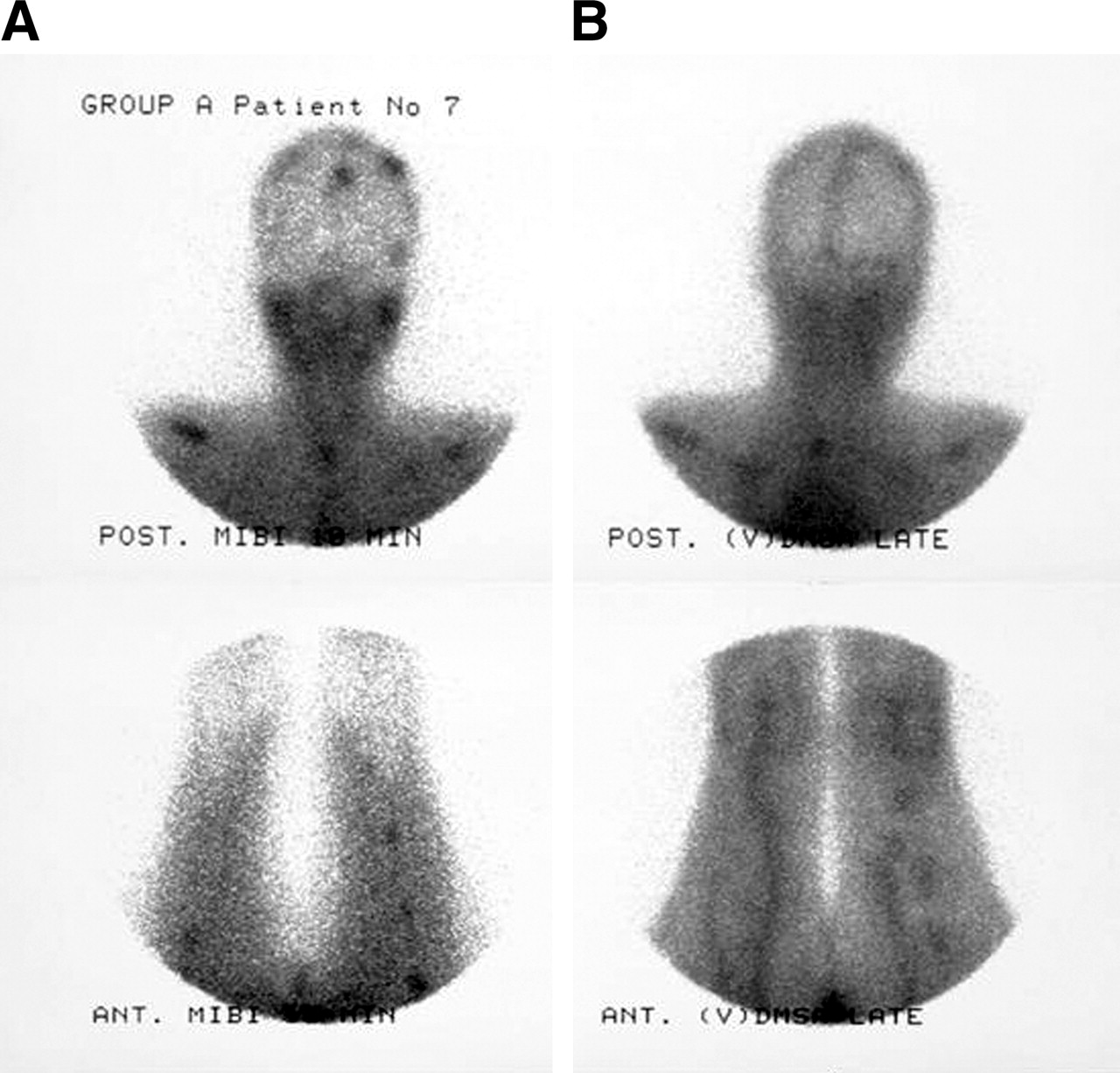
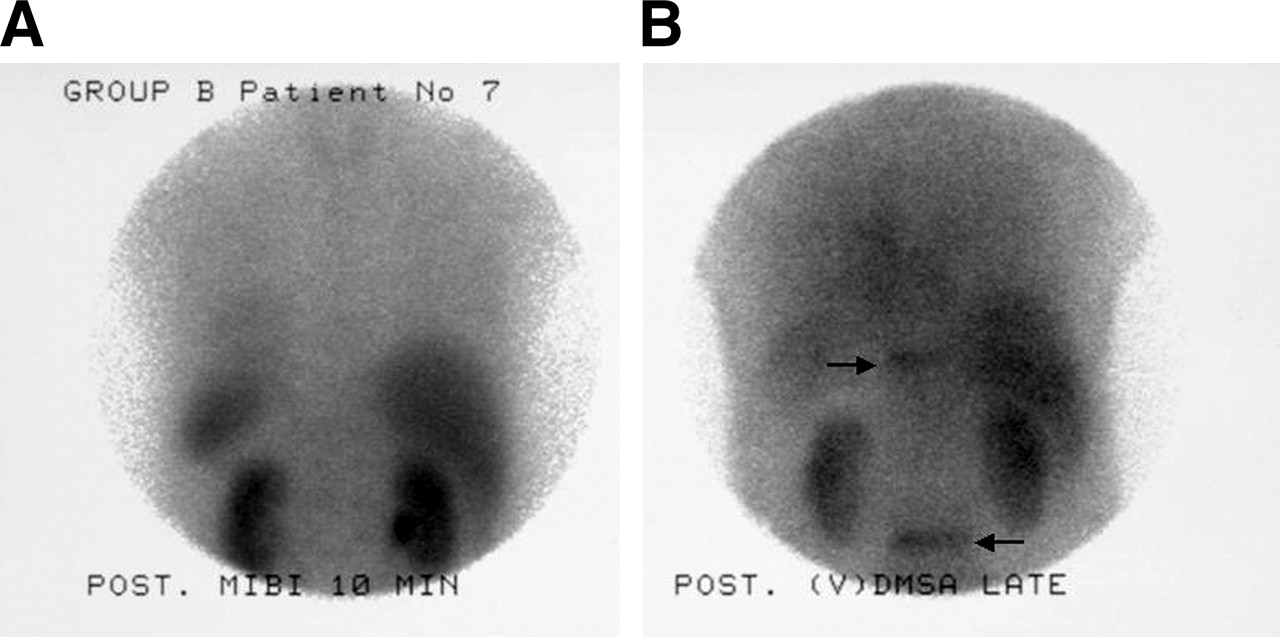
Patient 7 from group A, with 16 99mTc-MIBI–positive lesions (A) and 15 99mTc-V-DMSA–positive lesions (B). At top is posterior view of head, neck, and upper thorax; at bottom is anterior view of thighs. NAL/TPL ratio = 5/21 = 0.24.

Patient 2 from group B, with normal pattern of 99mTc-MIBI findings (A) and 2 99mTc-V-DMSA–positive lesions (arrows) in lower right ribs (B). Images are posterior view of thorax and upper lumbar region. NAL/TPL ratio = 2/2 = 1.

Patient 7 from group B, with normal pattern of 99mTc-MIBI findings (A) and 2 99mTc-V-DMSA–positive lesions (arrows) in vertebra bodies (B). Images are posterior view of thoracic and lumbar region. NAL/TPL ratio = 2/2 = 1.
The overall NAL/TPL ratio in group A was 16:58, which means that 27.6% of the lesions were considered as having been effectively treated. In group B, the NAL/TPL ratio was 22:27, which means that 81.5% of the lesions were considered as having been effectively treated (P < 0.001) (Fig. 5). The individual NAL/TPL ratios ranged from 0 to 0.75 (mean, 0.17) for patients in group A and from 0.50 to 1 (mean, 0.88) for patients in group B (P < 0.001) (Fig. 6).

NAL and 99mTc-MIBI or 99mTc-V-DMSA TPL detected in all patients in the 2 groups.
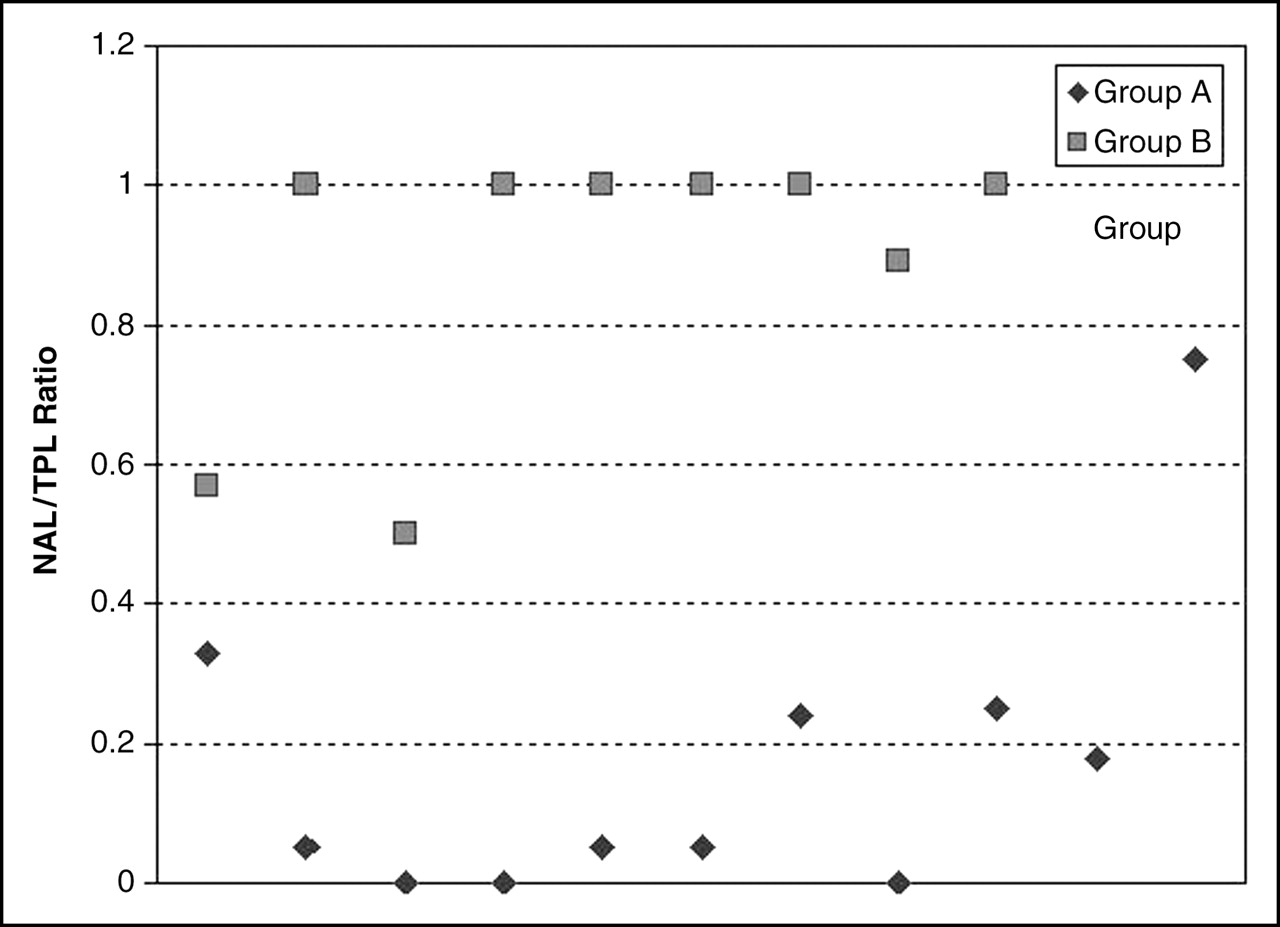
Distribution of individual NAL/TPL ratios for the 2 groups.
A negative correlation was observed between NAL/TPL ratio and the number of therapies in all patients (r = −0.27; P = NS). A correlation between NAL/TPL ratio and the number of therapies was observed in group A patients (r = −0.015; P = NS). In group B, the NAL/TPL ratio was inversely correlated with the duration of remission (r = −0.19) and the number of therapies (r = - 0.06), but not significantly so.
The disease status for the studied patients 2 y after the scintigraphies was as follows: From group A, 4 patients were stable (with active disease), 1 patient was in remission, and 6 patients had died. The mean NAL/TPL ratio for the 6 patients who died was 0.087. In group B, 8 patients were still in remission and 1 patient had died.
DISCUSSION
99mTc-MIBI, a myocardial perfusion agent, has been proposed as a tracer for several neoplasias, including multiple myeloma (1–4). 99mTc-MIBI is thought to be taken up by malignant tissues through accumulation in the mitochondria of viable tumor cells. In addition, retention of 99mTc-MIBI in tumor cells may be governed by the multidrug resistance 1 system. Therefore, the sensitivity of 99mTc-MIBI scanning is considerably affected by many conditions, such as multidrug resistance and chemotherapy (2,13).
99mTc-V-DMSA is a well-known tumor-seeking agent that accumulates in primary tumors and in metastatic lesions. Its accumulation is independent of multidrug resistance (14). The ability of 99mTc-V-DMSA to accumulate in tumor cells is thought to depend, in part, on the acidification of the tumor cell environment (15). The high glycolysis rate found in aggressive or malignant tumors results in increased production of lactic acid, which is thought to be a cause of acidic pH in tumors. Acidification induced by glucose administration results in increased 99mTc-V-DMSA accumulation in tumors (16). White cells and fibroblasts also use glucose as an energy source during their high metabolic activity and proliferation, allowing imaging of infections and inflammation by 18F-FDG PET (17,18). This may explain the accumulation of 99mTc-V-DMSA in inflammatory processes.
In a previous study, 99mTc-MIBI was compared with 18F-FDG PET in a patient with diffuse MM during preparation for bone marrow transplantation (19). 99mTc-MIBI appeared to indicate the extent of the disease, whereas 18F-FDG PET showed activity in only some of the areas that demonstrated 99mTc-MIBI uptake. These areas demonstrated active disease progression associated with pain. The authors inferred that inflammatory activity associated with tumor proliferation might be an additional factor leading to increased 18F-FDG uptake. No areas of exclusively 18F-FDG uptake were found, although no imaging took place after high-dose chemotherapy.
99mTc-V-DMSA accumulation in infection and inflammation has been well documented. Lee et al. (10) found that 99mTc-V-DMSA showed greater sensitivity and accuracy than did 67Ga in the assessment of bone and joint infection, although the difference was not statistically significant. Koutroubakis et al. (12) reported that 99mTc-V-DMSA scintigraphy had 92% sensitivity and 86% specificity in the detection of active inflammatory bowel disease. Those authors also found a significant correlation between disease activity indices and scintigraphy score.
In a report of ours, an important role for inflammation or fibrosis in 99mTc-V-DMSA uptake by tumors was proposed (8). We compared the 99mTc-MIBI and 99mTc-V-DMSA uptake changes in MM focal lesions in response to high-dose chemotherapy. The high-dose chemotherapy eliminated all 99mTc-MIBI uptake by the lesions, whereas 99mTc-V-DMSA uptake was increased in lesions presenting significant initial 99mTc-MIBI uptake. In 1 lesion that demonstrated this phenomenon, MRI showed necrosis of the MM tumor. This reversed result after chemotherapy implies that 99mTc-V-DMSA accumulation in MM lesions does not necessarily reflect viable tumor tissue.
In our study, we found that patients with active disease had a significantly lower ratio of 99mTc-V-DMSA–positive but 99mTc-MIBI–negative lesions to total scintigraphically demonstrable MM lesions (NAL/TPL ratio) than did patients in remission, in whom 99mTc-V-DMSA–positive lesions were much more numerous than 99mTc-MIBI–positive lesions.
Prognosis in MM depends on the extent of disease and the appropriate therapy. From the standpoint of disease extension alone, 99mTc-MIBI scintigraphy distinguished group A from group B since no patient from group A had normal 99mTc-MIBI findings whereas 6 of 9 patients from group B had normal 99mTc-MIBI findings. The 99mTc-MIBI–positive lesions numbered 42 and 5 in groups A and B, respectively. The NAL/TPL ratio appears to be a separate parameter in the determination of therapeutic effectiveness. The NAL/TPL ratio of group A was significantly lower than that of group B (0.276 vs. 0.815). In addition, those group A patients who died within 2 y of the scintigraphic studies had a mean NAL/TPL ratio of 0.087—even lower than for the group as a whole (mean NAL/TPL ratio, 0.17)—which strengths the value of this ratio.
No significant correlation was found between the NAL/TPL ratio and either the number of pretherapies for all patients or the duration of remission for group B patients. Also, no correlation was found in efficacy among different chemotherapy regimens. But since the number of our patients is still limited, we believe that we need more studies with larger numbers of patients to reach more accurate conclusions about these parameters and to determine any threshold for the NAL/TPL ratio.
CONCLUSION
Our results indicate that combined use of 99mTc-MIBI and 99mTc-V-DMSA scanning during chemotherapy allows evaluation of the effectiveness of the administered chemotherapy. Also, the large percentage of NAL in patients in remission supports the hypothesis that 99mTc-V-DMSA is not only a tumor-dependant analog. We believe that we need more studies with a greater number of patients to prove this hypothesis and to determine the ratio threshold above which the patients’ therapy can be considered effective.
Footnotes
Received Jul. 12, 2004; revision accepted Jan. 23, 2005.
For correspondence or reprints contact: John Koutsikos, MD, 44-48 Martinegou St., N. Filothei, 11524, Athens, Greece.
E-mail: jtkoutsik{at}yahoo.gr
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.