


Abstract
Physiologic 18F-FDG uptake in the stomach can often cause false-positive results and lowers the usefulness of 18F-FDG PET in evaluating the remnant stomach. We assessed the role of gastric distension to see whether it is beneficial for the differentiation of recurrent tumors from physiologic 18F-FDG uptake in the remnant stomach. Methods: Thirty patients (22 men and 8 women; age range, 27–80 y; mean age, 58.3 y) with a history of subtotal gastrectomy for gastric cancer underwent 18F-FDG PET for various clinical indications. After whole-body imaging, the patients were asked to drink water, and then spot imaging of the stomach was performed. 18F-FDG uptake in the remnant stomach was considered positive for malignancy if it was persistently increased, whether focal or diffuse, after water ingestion. We used 2 standardized uptake value (SUV) criteria to differentiate benign from malignant uptake. First, a lesion was considered benign if its SUV was less than 2 on whole-body imaging. Second, for a lesion with an SUV of 2 or above, it was classified as benign if SUV decreased by more than 10% after water ingestion. Results: Visual analysis of whole-body images produced 9 true-negative, 4 false-positive, 16 true-positive, and 1 false-negative results. Use of additional spot images produced 12 true-negative, 1 false-positive, 15 true-positive, and 2 false-negative results. When an SUV cutoff of 2 was applied for malignancy before water ingestion, all 17 patients with local recurrence were correctly identified, but 11 of the 13 patients without local recurrence were falsely considered to have a recurrent tumor in the remnant stomach. To reduce the false-positive results, we used the second SUV criterion after water ingestion. Use of that criterion produced 4 false-negative results although it correctly identified the 11 false-positive results as true negative. Conclusion: Gastric distension by having patients drink a glass of water seems to be a simple, cost-effective way of improving the diagnostic accuracy of 18F-FDG PET in patients with suspected recurrence in the remnant stomach. Visual analysis with special attention to the configuration of 18F-FDG activity after water ingestion seems to be more useful than the change in SUV in evaluating the remnant stomach.
Total gastrectomy is the preferred procedure for advanced gastric cancer of the proximal or middle third of the stomach, to eliminate the possibility of recurrence in the gastric stump or the surrounding lymph nodes (1). Subtotal gastrectomy seems more commonly performed on patients with distal gastric tumor because no survival benefit has been proven for total or subtotal gastrectomy (2). When tumor recurs in the remnant stomach, any treatments with curative intent are usually considered futile. Recently, secondary total gastrectomy has been attempted if the local recurrence is confined to the remnant stomach, and long-term survival may occasionally result (3).
Other than periodic surveillance using endoscopy, noninvasive anatomic imaging studies such as a barium study or CT have been used in detecting recurrent tumors of the remnant stomach. Surgical alteration of normal anatomy substantially limits the value of these anatomic imaging modalities for evaluation of recurrent diseases. The main problem with CT is its lack of specificity in differentiating recurrent tumor in the remnant stomach from improperly distended bowel loops, surgical plication, bowel adhesion, or stomal polypoid hypertrophic gastritis (4).
Although 18F-FDG PET has been useful for detecting recurrent diseases of various cancers, its usefulness for evaluating the remnant stomach is limited. A low level of 18F-FDG uptake is commonly seen in the normal stomach, although it can have a standardized uptake value (SUV) of as high as 5.6 (5). The configuration of the activity generally allows identification of physiologic gastric uptake. However, a contracted or nonuniform uptake in the stomach can be mistaken for a pathologic finding, especially in patients with a remnant stomach after subtotal gastric surgery. The remnant stomach often appears contracted and shows a variable degree of 18F-FDG uptake.
We hypothesized that physiologic 18F-FDG uptake in the remnant stomach could easily be made to disappear by distension of the gastric wall and that, therefore, false-positive results might be reduced on 18F-FDG PET. In this study, we assessed whether gastric distension using water ingestion helps differentiate a recurrent tumor from physiologic uptake in the remnant stomach.
MATERIALS AND METHODS
Thirty patients (22 men and 8 women; age range, 27–80 y; mean age, 58.3 y) underwent 18F-FDG PET for the further evaluation of suspected lesions detected on anatomic imaging modalities such as a barium study or CT (n = 23), for evaluation of response after chemotherapy (n = 4), or for routine medical surveillance (n = 3). Of the 23 patients with suspected lesions, 16 had been examined with CT and 7 with both a barium study and CT. The suspected lesions were in the remnant stomach in 17 of the 23 patients and in other abdominal locations in the remaining 6 patients. All patients had undergone a subtotal gastrectomy for the management of gastric malignancy. The mean interval between subtotal gastrectomy and 18F-FDG PET examination was 50 mo (minimum, 6 mo; maximum, 144 mo). The types and stages of the primary tumors are presented in Table 1.
Primary Tumors
All patients were instructed to fast for at least 4 h before the intravenous injection of 18F-FDG. The mean interval between the injection and the beginning of whole-body scanning was 66 min (range, 50–76 min). Images were obtained on either an Advance PET scanner (GE Healthcare) or an Allegro PET system (Philips-ADAC Medical Systems). The Advance obtained images in 2-dimensional mode, and the Allegro in 3-dimensional mode. Transmission scans using 68Ge or 137Cs point sources were obtained to correct for nonuniform attenuation. After initial whole-body imaging, the patients were asked to drink as much water as possible (at least 300 mL). The mean interval between whole-body scanning and the beginning of regional scanning after water ingestion was 6.7 min (range, 3–13 min). Regional imaging of the stomach was performed at a mean interval of 113 min (range, 89–128 min) after the injection of 18F-FDG. The images were reconstructed using an iterative reconstruction algorithm: ordered-subset expectation maximization for the Advance or low-action maximal likelihood for the Allegro. The adequacy of gastric distention after water ingestion was confirmed if the remnant stomach appeared circular or as an elongated tube with a convex margin. No or only minimal 18F-FDG uptake along the gastric wall was expected in well-distended cases.
For visual analysis, 2 experienced nuclear medicine physicians unaware of other clinical or radiologic findings interpreted the PET images on a high-resolution computer screen and reached a consensus for each scan. On whole-body images, the degree and configuration of 18F-FDG uptake were evaluated (Figs. 1 and 2). Any irregular or round masslike configuration with increased 18F-FDG uptake was considered malignant. A linear or curvilinear configuration, regardless of 18F-FDG uptake, was interpreted as benign. On spot images of the stomach after water ingestion, 18F-FDG uptake in the remnant stomach was considered malignant if it showed persistently increased focal or diffuse uptake. For semiquantitative analysis, a region of interest was placed over the area of maximum activity in the remnant stomach. An SUV corrected for total body weight was calculated within the region of interest, and the average SUV was taken for analysis. We used 2 SUV criteria for differentiating between benign and malignant uptake. For the first criterion, uptake was considered benign if its SUV was less than 2 on whole-body imaging. For the second, uptake with an SUV of 2 or above was classified as benign if the SUV decreased by more than 10% after water ingestion. Final conclusions on recurrence in the remnant stomach were based on endoscopic biopsy (n = 16), histopathologic specimens (n = 10), or clinical and imaging follow-up (n = 4).
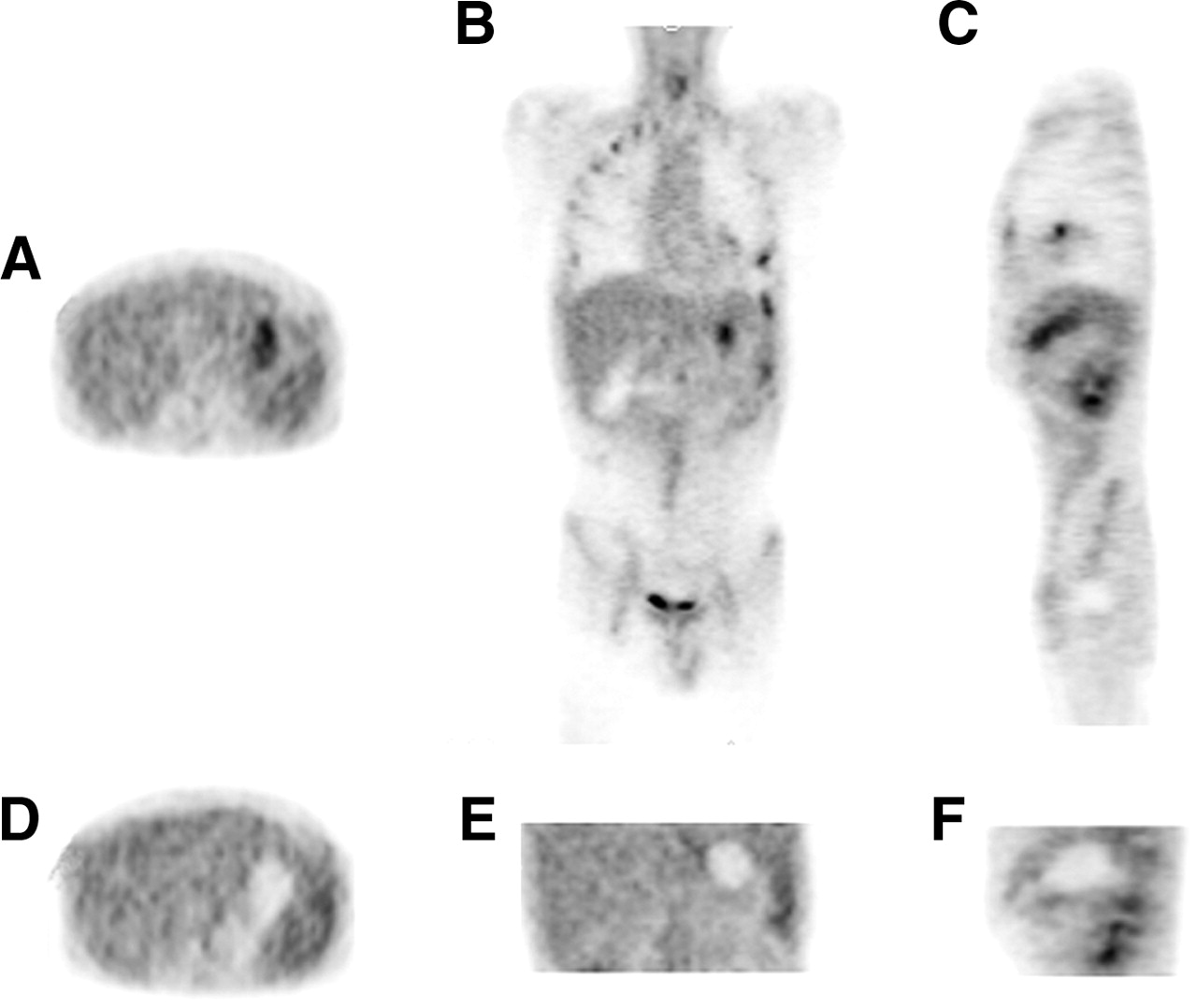
Axial (left), coronal (middle), and sagittal (right) 18F-FDG PET images of patient with physiologic 18F-FDG uptake in remnant stomach. (A–C) Before water ingestion, increased 18F-FDG uptake is seen in remnant stomach. (D–F) After water ingestion, uptake disappears.

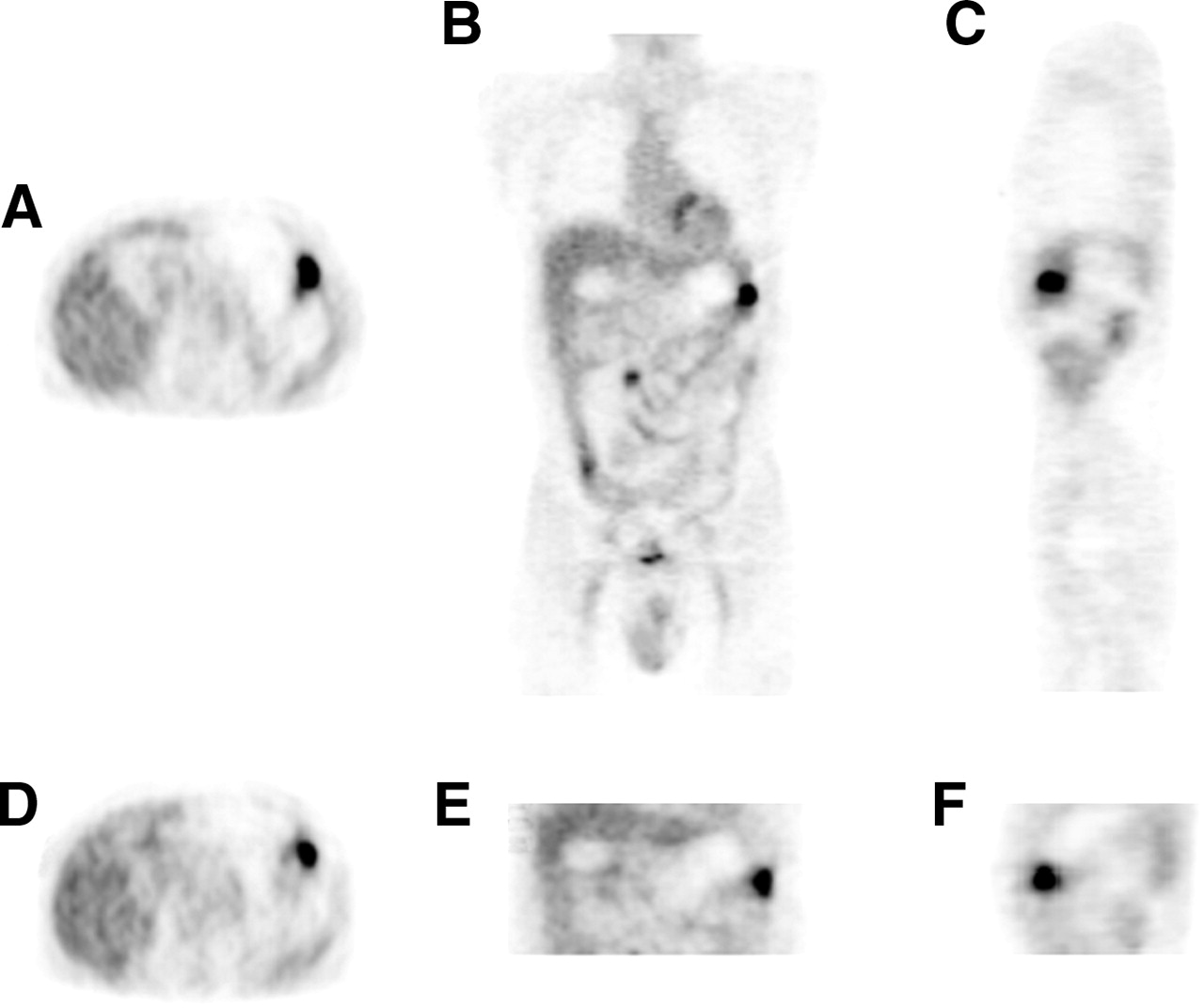
Axial (left), coronal (middle), and sagittal (right) 18F-FDG PET images of patient with recurrent tumor in remnant stomach. (A–C) Before water ingestion, round area of increased 18F-FDG uptake is seen in remnant stomach. (D–F) After water ingestion, uptake persists.
RESULTS
Seventeen of the 30 patients had recurrent tumor in the remnant stomach, and 13 did not (Table 2). For the 13 patients without recurrence, visual interpretation of whole-body images produced 9 true-negative and 4 false-positive results. With spot images after water ingestion, visual analysis produced 12 true-negative results. All 12 of these patients showed a decrease in 18F-FDG uptake in the remnant stomach and no persistent focal or diffuse uptake (Fig. 1). One patient showed a false-positive result after water ingestion. Whole-body PET images showed an area of increased 18F-FDG uptake in the region of the remnant stomach, and spot images of the stomach after water ingestion showed persistently increased 18F-FDG uptake. Endoscopic biopsy of the stomach revealed an ulcer with granulation tissue. By the first SUV criterion, only 2 patients with an SUV of less than 2 were correctly categorized as having benign uptake. The 11 patients with an SUV of 2 or above showed more than a 10% decrease in SUV after water ingestion. Therefore, SUV analysis after addition of the second criterion accurately identified all 13 of the patients who did not have tumor recurrence. The average SUV of the 13 patients with benign 18F-FDG uptake was 5.3 on whole-body images and decreased to 2.4 after water ingestion.
Diagnostic Performance of Visual and SUV Analysis in Patients With or Without Recurrence in Remnant Stomach
For the 17 patients with recurrent disease, visual analysis of initial whole-body images produced 16 true-positive findings and 1 false-negative finding. In the false-negative case, the result was attributed to the curvilinear shape mimicking a collapsed stomach. Visual analysis of spot images showed that 15 patients had persistent focal or diffuse 18F-FDG uptake after water ingestion (Fig. 2), and all proved to have recurrent disease in the remnant stomach. On the other hand, visual analysis of the spot images produced false-negative results for 2 patients (12%). The recurrent tumor was of a signet ring cell histologic type (Fig. 3). No patient among the 17 with recurrent disease had an SUV of less than 2. However, adding the second SUV criterion produced false-negative results (24%) for malignancy in 4 patients, with these patients having SUV decreases of more than 10% after water ingestion. In addition to the 2 patients with false-negative results on visual analysis of spot images, the third patient had an early gastric cancer of poorly differentiated type and the fourth patient had an early gastric cancer of well-differentiated type. Thus, the tumors that showed more than a 10% decrease in SUV were either signet ring cell carcinoma or early gastric cancer. The average SUV of the 17 patients with local recurrence was 6.3 before water ingestion and 6 afterward.

Axial whole-body PET images of patient with recurrent signet ring adenocarcinoma in remnant stomach. (A) On these consecutive images obtained before water ingestion, peculiar area of increased 18F-FDG uptake is seen in remnant stomach (interpreted as true positive). (B) On these consecutive images obtained after water ingestion, decrease in 18F-FDG uptake produces false-negative result. In this case, initial 18F-FDG uptake might have been physiologic rather than due to recurrent tumor, considering tumor histology and result on spot images.
Overall, visual analysis of whole-body images produced 9 true-negative, 4 false-positive, 16 true-positive, and 1 false-negative results. Use of spot images produced 12 true-negative, 1 false-positive, 15 true-positive, and 2 false-negative results. When an SUV cutoff of 2 was applied for malignancy before water ingestion, all 17 patients with local recurrence were correctly identified. However, 11 of the 13 patients without local recurrence were falsely considered to have recurrent tumors in the remnant stomach. To reduce the false-positive results, we used the second SUV criterion after water ingestion. It resulted in 4 false-negative results although it correctly identified the 11 false-positive results as true negative.
DISCUSSION
Even after complete resection with curative intent, tumor is known to recur in more than half of patients with gastric adenocarcinoma (1,3). The most common sites include local recurrence in the gastric bed, peritoneal dissemination, and liver or other distant metastases. Insufficient tumor resection and remaining tumor cells after partial gastrectomy seem to be important factors in recurrence within the gastric remnant. This is particularly true for the diffuse type of gastric cancer, because a discontinuous growth pattern allows tumor cells to remain outside the resection margin. Whether the tumor is a true recurrence in the remnant stomach or a metachronous secondary malignancy, any treatments with curative potential are considered futile. Recently, despite survival hardly exceeding 1 y, surgical therapy for locally recurrent gastric cancer at an early stage has been proposed because of the lack of alternatives with a chance for cure in these patients (3).
Abdominal CT using water as a negative oral contrast agent has been useful to distend the gastric wall for the evaluation of gastric cancer. Distension makes it easier to delineate subtle mucosal abnormalities of the stomach and decreases the possibility of misinterpreting the contracted gastric wall as pathologic (6). We have adopted the water ingestion method to eliminate physiologic 18F-FDG uptake in the contracted remnant stomach. In fact, physiologic 18F-FDG uptake has been a well-known diagnostic pitfall in the detection of disease in the stomach (5). Although the configuration of 18F-FDG uptake in the intact stomach is helpful to correctly identify physiologic uptake, this configuration may be difficult to apply to the remnant stomach, which appears contracted most of time and, therefore, can be seen as a masslike area of variable 18F-FDG uptake on PET. Differentiation of physiologic 18F-FDG uptake in the remnant stomach from recurrent tumor is often impossible when physiologic 18F-FDG uptake is high.
In this study, visual analysis of initial whole-body images resulted in 31% false-positive results (4/13). We used a simple criterion for the interpretation of images after water ingestion to reduce the high false-positive rate on initial whole-body images. A lesion was considered malignant when it showed persistent 18F-FDG uptake after water ingestion. After water ingestion, physiologic 18F-FDG uptake in the remnant stomach showing a masslike area of variable 18F-FDG uptake becomes a cystic structure with mild and even distribution of 18F-FDG along the margin. Visual analysis of spot images after water ingestion produced 27 true-negative or true-positive results, 1 false-positive result, and 2 false-negative results. For SUV analysis, we used a cutoff value of 2 for a malignant lesion on initial whole-body images. The cutoff value was selected because all patients with recurrent tumor had an SUV of 2 or above in this study. This cutoff SUV allowed correct categorization of all 17 patients with local recurrence but produced 11 false-positive results in the 13 patients without local recurrence. In an attempt to reduce the number of false-positive results, we applied the second SUV criterion measuring the change in SUV after water ingestion. Although this criterion correctly identified the 11 false-positive results as true negative, it produced 2 false-negative results in addition to the 2 on visual analysis of spot images. The signet ring histology or small size of the recurrent tumors was the reason for the more than 10% decrease in SUV in these tumors. With signet ring histology, SUV on whole-body images could be overestimated because of physiologic uptake in the adjacent gastric wall. With small tumors, SUV on spot images might be underestimated because of the partial-volume effect whereas visual analysis still recognizes it as a focal lesion even after water ingestion. Therefore, the shape of 18F-FDG activity seems more important than the change in SUV for evaluating recurrent disease in the remnant stomach.
For the 17 patients with locally recurrent tumors, visual analysis of initial whole-body images produced 1 false-negative result. Two false-negative results were seen on spot images after water ingestion as shown in Figure 3. The 2 patients had recurrent tumor of the signet ring cell histologic type. These results are in line with a few recent reports suggesting that primary tumors of signet ring cell, mucinous, or poorly differentiated histologic types tend to show low-grade 18F-FDG uptake (7–9). The usefulness of 18F-FDG PET seems to vary with the pathology of the primary tumor. Moreover, water ingestion had no additional value in detecting recurrence of tumors of the signet ring cell histologic type in our series despite the theoretic advantage of water ingestion seen on CT data. On the other hand, the 31% false-positive rate on visual analysis of whole-body images decreased to only 8% (1/13) after water ingestion. SUV analysis also showed a similar result, remarkably reducing the false-positive rate from 85% to 0%. Our results show that 18F-FDG PET can detect locally recurrent disease in the remnant stomach with a high specificity. However, the absence of increased 18F-FDG uptake cannot exclude the possibility of local recurrence and may not eliminate invasive diagnostic procedures such as periodic endoscopic surveillance. Whether PET/CT enhances diagnostic accuracy for gastric tumors with no or low 18F-FDG uptake remains to be assessed.
It is not clear which portion of the stomach contains 18F-FDG activity. Regardless, it disappears after water ingestion, most likely because of the partial-volume effect of the distended and thinned gastric wall. With this effect, water ingestion seems extremely useful in reducing false-positive results in the evaluation of the remnant stomach. It is also conceivable that water ingestion may improve the sensitivity of 18F-FDG PET by improving contrast between the tumor and the normal, contracted gastric wall with physiologic 18F-FDG uptake. This possibility was not proven in this small series, and further studies will be needed to better elucidate the role of water distention in this regard. In our study, the main advantage of water ingestion was the improved specificity of the study. Before spot imaging, an adequate amount of water ingestion should be ensured. In cases of incomplete distention of the stomach, a region of increased 18F-FDG uptake in the less distended gastric wall may mimic tumor recurrence. Another potential problem with water ingestion in the remnant stomach could be the rapidity of gastric emptying, depending on the type of gastrectomy.
Of our 30 patients studied, 23 were evaluated for suspected recurrences, 4 for treatment response, and 3 for routine surveillance, who had a different pretest probability of tumor recurrence. The numbers of the patients for the last 2 indications were not enough to analyze the value of 18F-FDG PET according to pretest probabilities of recurrence. Further studies are warranted to better evaluate the role of gastric distention on 18F-FDG PET with respect to the prevalence of recurrence.
CONCLUSION
Gastric distension by having the patient drink a glass of water appears to be a simple, cost-effective way of improving the diagnostic accuracy of 18F-FDG PET in patients with suspected recurrence of cancer in the remnant stomach. Water ingestion may also increase the diagnostic confidence in true-negative results since high, physiologic 18F-FDG uptake of linear or curvilinear configuration disappears afterward. However, false-negative results can be seen in patients with recurrent diseases of a signet ring cell variant, which show low 18F-FDG uptake regardless of water ingestion. Visual analysis with special attention to the configuration of 18F-FDG activity after water ingestion seems to be more useful than the change in SUV in evaluating the remnant stomach.
Acknowledgments
We are grateful to Dr. David Yeh for the preparation of the manuscript and his intellectual contribution to this study.
Footnotes
Received Oct. 1, 2004; revision accepted Jan. 26, 2005.
For correspondence or reprints contact: Jong Doo Lee, MD, Division of Nuclear Medicine, Department of Diagnostic Radiology, Yonsei University, College of Medicine, 134 Shinchon-dong, Seodaemoon-ku, Seoul, Korea, 120-752.
E-mail: jdleenuc{at}yumc.yonsei.ac.kr





{kind=link}
{kind=link}
{kind=link}