


Abstract
The aim of this retrospective study was to evaluate the sensitivity and prognostic significance of whole-body 18F-FDG PET for nasopharyngeal carcinoma (NPC) patients for whom there was a suspicion of recurrence or metastasis by conventional radiologic or clinical findings during their follow-up examinations. Methods: Whole-body 18F-FDG PET examinations were performed on 64 Taiwanese NPC patients (14 female, 50 male; mean age ± SD, 45.8 ± 13.0 y; age range, 16–75 y) 4–70 mo (mean ± SD, 14.1 ± 13.5 mo) after radiotherapy or induction chemotherapy followed by concurrent chemoradiotherapy from February 1997 to May 2001. The accuracy of 18F-FDG PET detection for each patient was determined by the histopathologic results or other clinical evidence. Results: The sensitivity, specificity, accuracy, positive predictive value, and negative predictive value of 18F-FDG PET images in the diagnosis of NPC recurrence or metastases and secondary primary cancers were 92%, 90%, 92%, 90%, and 91%, respectively. Furthermore, the presence of 18F-FDG hypermetabolism was highly correlated with the survival time of NPC patients. Conclusion: Whole-body 18F-FDG PET is a sensitive follow-up diagnostic tool for the evaluation of NPC recurrences and metastases. It is also an effective prognostic indicator for NPC patients. To determine the optimized utilization of 18F-FDG PET in the follow-up for NPC patients, further cost-effectiveness analysis of 18F-FDG PET in combination with conventional management is necessary.
Nasopharyngeal carcinoma (NPC) is one of the most common malignant tumors in Southern China and Southeast Asia (1). It occurs in 10–30 persons per 100,000 people per year. The locoregional recurrences and distant metastases are crucial prognostic factors for NPC patients after radiotherapy (RT) or RT with adjuvant chemotherapy (2,3). The conventional structure-based diagnostic tools, such as MRI and CT, have not been proven to be effective in the early detection of residual, recurrent, or metastatic foci (4–6).
It has been demonstrated in previous studies that 18F-FDG PET is a promising tool to distinguish recurrent tumors from posttreatment changes in the nasopharynx (7–10). To the best of our knowledge, the prognostic significance of whole-body 18F-FDG PET for patients with NPC has not been reported previously. The aim of this retrospective study was to evaluate the sensitivity and prognostic significance of whole-body 18F-FDG PET for NPC patients for whom there was a suspicion of recurrence or metastasis.
MATERIALS AND METHODS
Patients
The database consisted of 14 female and 50 male Taiwanese NPC patients (mean age ± SD, 45.8 ± 13.0 y; age range, 16–75 y) treated in the National Taiwan University Hospital. These patients had received RT or induction chemotherapy followed by concurrent chemoradiotherapy (CCRT) and there was a suspicion of recurrence or metastasis by conventional radiologic or clinical findings during their follow-up examinations. Whole-body 18F-FDG PET examination was performed on each patient 4–70 mo (mean ± SD, 14.1 ± 13.5 mo) after RT or CCRT during the period from February 1997 to May 2001. All patients had given consent to use their 18F-FDG PET results and relevant clinical data for this study.
Whole-Body 18F-FDG PET
For the 18F-FDG PET examination, each patient was injected with 370 MBq (10 mCi) of 18F-FDG intravenously after a fasting period of 6 h or longer. The emission data were collected for each patient 45 min after the injection using an Advance PET scanner (General Electric Medical Systems). From the collected emission data that had been corrected for scatter, random events, and dead time, the image was reconstructed by the filtered backprojection method without attenuation correction. Although the signal-to-noise ratios might be improved to some extent with attenuation correction (11–13), the image resolutions without attenuation correction were adequate for the purpose of this study. Image pixel size was 3.0 mm in a 128 × 128 array. Besides the whole-body images, additional coronal and sagittal planes of the head and neck were reoriented to obtain a better view of the nasopharynx and neck region.
Image Interpretation
All 18F-FDG PET images of these 64 NPC patients were interpreted qualitatively by 2 nuclear medicine physicians without prior knowledge of the follow-up status of these patients. The rate of consistency between the 2 observers was high (62/64). Images with inconsistent interpretations were subsequently perused together by both physicians until consensus was reached.
A biopsy was performed in 20 of the 64 patients after PET. Their biopsy results offered the references for verifying their 18F-FDG PET results in our study. For the rest of the patients, the accuracies of their PET results were determined by their subsequent follow-up clinical examinations or conventional imaging.
Statistical Analysis
All numbers are expressed as mean ± SD. The comparisons between different groups of numbers were made according to the 2-tailed paired and unpaired Student t tests. The censoring date for this study was August 31, 2003. The survival time was defined as the period from the date of PET examination to the date of death for patients who died before the censoring date or the date of last contact for patients who failed to keep their follow-up appointments or the censoring date. The average follow-up period was 43.33 ± 20.14 mo. Long-term survival and mortality were estimated by the life-table method. The log-rank test was used to assess cumulative survival between the 2 groups. Statistical analyses were performed with the SAS system for Windows, version 8.1 (SAS Institute).
RESULTS
Patients
The whole-body 18F-FDG PET of the 64 patients in this study consisted of 28 negative and 36 positive readings. Table 1 lists patient characteristics, pathologic TNM status, censored status, and post-PET survival time. Table 2 summarizes the follow-up results.
Patient Characteristics According to 18F-FDG PET Results
Individual Clinical Outcomes According to 18F-FDG PET Results
All 28 patients with negative readings of 18F-FDG PET were still alive at the time of data analysis, although metastasis developed in 3 patients after the PET examination. One was found to have lung metastasis 40 mo after PET, another had pericardial metastasis confirmed by CT-guided biopsy 17 mo after PET, and the other had a subcentimeter lymph node metastasis 7 mo after PET. The detailed follow-up results of these 28 patients are summarized in Table 2.
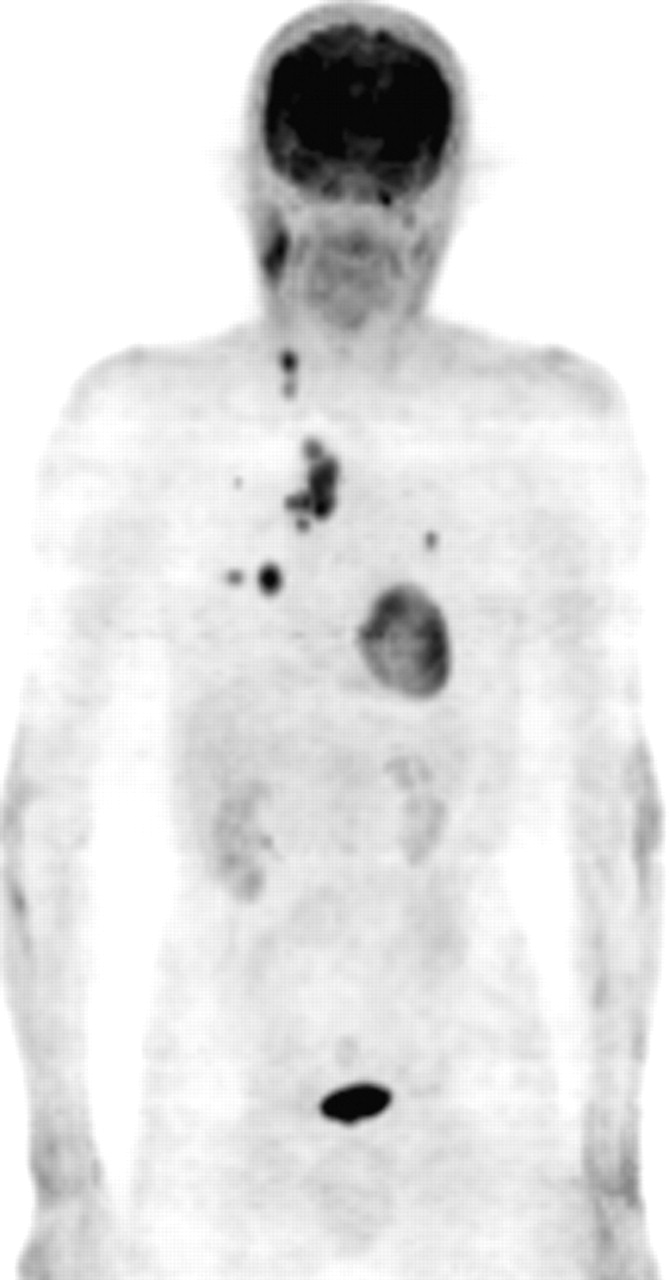
There were 36 18F-FDG PET-positive patients. Three of the 14 patients who exhibited abnormal 18F-FDG uptake in the nasopharyngeal area did not have recurrent NPC or other metastases. One patient had only neck lymph node metastasis (Fig. 1). Nine patients had both nasopharyngeal recurrent metastases and neck lymph node metastases. One patient had axillary and mediastinal lymph node distant metastases, 3 patients had lung metastases, 4 patients had bone metastases, and 2 patients had both neck lymph node metastasis and lung metastases (Fig. 2). One patient, whose PET image showed abnormal 18F-FDG uptake in the lung, was proven to have a second malignancy of nonsmall cell lung cancer. The last of the 36 PET-positive patients had nasopharyngeal recurrence and neck lymph node, lung, and bone metastases. The detailed results of these 36 patients are summarized in Table 2.

18F-FDG PET images of 51-y-old male patient who underwent PET examination 8 mo after CCRT (pretherapy stage IVA) show a biopsy-proven cervical lymph node metastasis at left submandibular region (arrows) and intense 18F-FDG uptake in right cervical muscle (arrowhead). No lymph node metastasis in the right neck was observed during clinical follow-up in this patient.

Image of 63-y-old male patient who underwent 18F-FDG PET examination 8 mo after completion of CCRT reveals multiple 18F-FDG hypermetabolic lesions in right neck, mediastinum, and bilateral lungs. Patient died 13 mo after PET study.
Diagnostic Accuracy
As shown in Table 3, the sensitivity and specificity of 18F-FDG PET in this study for the diagnosis of NPC recurrence or metastases and secondary primary cancers were 92% (33/36) and 90% (25/28), respectively. The positive predictive value was 92% (33/36). The negative predictive value was 90% (25/28). The overall accuracy was 91% (58/64).
Diagnostic Value of 18F-FDG PET in Detection of Recurrence or Metastatic NPCs and Secondary Primary Cancers for 64 NPC Patients
Survival
All 28 patients in the PET-negative group were still alive at the time of data analysis. Eight of the 36 patients in the PET-positive group had already died from the cancer. The survival rate difference is statistically significant (P < 0.001).
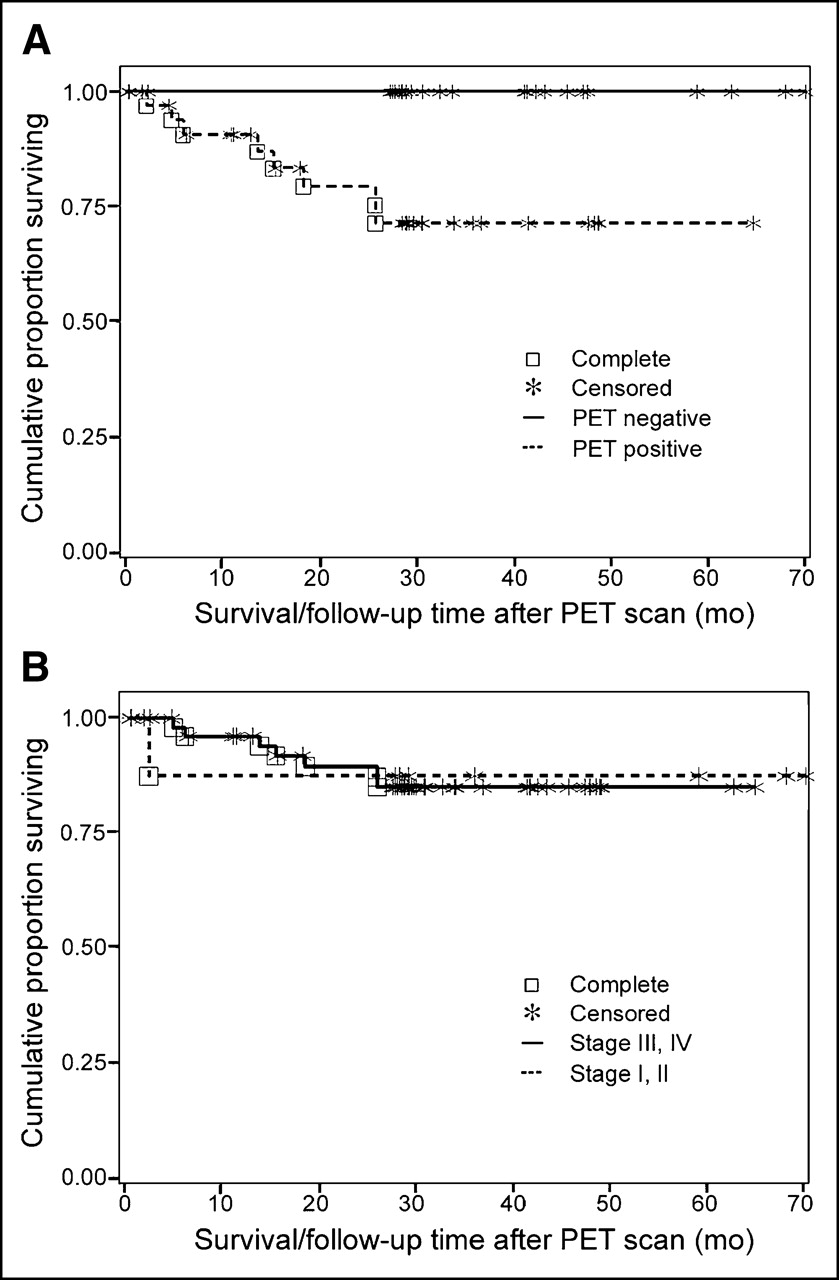
Survival analysis for the entire patient group using a life-test procedure showed a longer survival in the PET-negative group (36.99 ± 14.62 mo) than that in the PET-positive group (24.83 ± 16.21 mo) (P = 0.003) (Fig. 3A). On the other hand, the survival time for patients with a lower (I and II) (n = 10) pretherapy stage was not statistically different from that for patients with a higher (III and IV) (n = 54) pretherapy stage (P = 0.9233) (Fig. 3B).

Survival for PET-positive and PET-negative patient groups (A) and stage I, II and stage III, IV patient groups (B).
DISCUSSION
The ability of conventional anatomic imaging modalities, such as CT and MRI, to differentiate residual or recurrent tumor from tumor necrosis and tissue fibrosis after RT is limited. Therefore, it has been proposed that 18F-FDG PET—a whole-body imaging technology based on glucose metabolism—can be useful to differentiate viable tumor from necrosis or fibrosis. Several studies have already provided evidence (7–10) that 18F-FDG PET is more effective in the detection of local recurrent or residual NPC than CT and MRI. Nevertheless, 18F-FDG PET data should be carefully interpreted. RT-induced inflammatory process may lead to a transient increase of 18F-FDG uptake and result in false-positive 18F-FDG PET readings. On the other hand, false-negative 18F-FDG PET results may occur as the metabolic mechanism of the residual tumor tissue may be temporarily inhibited after RT (14–16). Therefore, we adopted the proposal of Greven et al. and performed the 18F-FDG PET scans at least 4 mo after the completion of RT in this study (15).
However, 2 of the 3 false-positive patients, with 18F-FDG PET performed 6 and 19 mo, respectively, after RT, still showed 18F-FDG hypermetabolism at the nasopharynx as a result of inflammatory processes, which were evident in their subsequent pathologic examination. Both patients were free of NPC recurrence during the clinical follow-up periods, 29 and 6 mo, respectively, after their 18F-FDG PET studies.
Fischbein et al. reported that 18F-FDG PET might not be reliable for patients who had received paranasal sinus surgery, which might induce mucosal inflammation (8). The postsurgical inflammation may account for the third false-positive reading. This patient had chronic paranasal sinusitis since the completion of RT and had received a bilateral sphenoidotomy 6 mo before the 18F-FDG PET scan. His 18F-FDG PET scan showed intense 18F-FDG accumulation in the right paranasal region, whereas fluid accumulation in the bilateral mastoids was demonstrated by MRI. This patient was monitored for more than 30 mo after the 18F-FDG PET scan and no tumor recurrence was detected.
To detect recurrent tumor foci in cervical lymph nodes, anatomic imaging modalities locate cervical lymph node metastases according to information such as size, central necrosis, rim contrast enhancement, and structural changes of the lymph nodes (17,18), whereas 18F-FDG PET detects abnormal glucose metabolism in the metastatic cervical lymph nodes (19,20). Although 18F-FDG PET can detect cervical lymph node metastases with high sensitivity and a high negative predictive value (19,20), it may not be sensitive enough to detect metastases that are less than 1 cm in diameter (21). At this time, neither anatomic nor metabolic imaging provides sufficient resolution power for the detection of microscopic metastases (22). This also explains the finding that the first of the 3 false-negative patients in this study was found clinically to have a subcentimeter cervical metastasis 7 mo after his 18F-FDG PET scan.
It is known that lung and bones are the most frequent sites of NPC metastases (23) and 18F-FDG PET can detect metastatic foci in these organs with high sensitivity (24). However, the second patient with a false-negative reading had lung metastasis 40 mo after 18F-FDG PET. The lung metastasis was confirmed by biopsy in this patient. Since there was a considerable time span between the 18F-FDG PET examination and the verification of his lung metastasis, it is possible that the lung metastasis might not have existed at the time of 18F-FDG PET or was too small to be detectable by 18F-FDG PET.
The last of the 3 false-negative patients had pericardial metastasis 7 mo after his 18F-FDG PET examination. This is explained by the fact that frequent existence of the intense 18F-FDG uptake in myocardium may interfere with the detection of abnormal pericardial metabolism.
No muscle relaxant was given to any of the patients in our study, although it has been suggested (25–27) that muscle relaxants may be administered to patients before PET to avoid nonspecific uptake of 18F-FDG by muscle (Fig. 1). We are fully aware that false-positive readings may occur by physiologic uptake in nontumor areas and uptake in cervical muscles may mask the uptake of nearby lymph nodes to result in false-negative readings. Therefore, we took these possibilities into consideration in interpreting PET images. The follow-up results confirmed that none of the PET images in our study were misinterpreted because of cervical muscle uptake.
It has been documented that locoregional recurrences and distant metastases are the most important prognostic factors for NPC (2,3). The results of this study show that whole-body 18F-FDG PET has high sensitivity in detecting recurrence or residual malignancy, cervical lymph node metastases, distant metastases, and secondary primary cancer and has high specificity in predicting the absence of malignancy. We have also demonstrated that there is a significant correlation between the presence of 18F-FDG hypermetabolism and the survival time of NPC patients (Fig. 3A). On the other hand, it is evident that the cancer stage at the time of diagnosis for each patient was unrelated to the survival time in this study.
Goerres et al. (28) have reported that 18F-FDG PET has high accuracy for patients with suspected residual or recurrent head and neck cancers. Due to the prohibitive cost of 18F-FDG PET, this imaging modality is not regularly scheduled for follow-up of NPC patients in our center (29). PET examinations after RT for the 64 NPC patients in this study were arranged only when recurrences or metastases were suspected on the basis of the results of conventional radiologic or clinical findings during the follow-up periods. In this study, we have shown that 18F-FDG PET is very effective for NPC patients with suspected recurrences or metastases. Under certain circumstances, it may still be cost-effective to perform 18F-FDG PET for NPC patients after RT even before the symptoms of recurrence or metastasis appear. Therefore, a cost-effectiveness analysis to determine the optimized timing for PET follow-up of NPC patients is necessary.
CONCLUSION
Whole-body 18F-FDG PET is a sensitive follow-up diagnostic tool to evaluate NPC recurrences and metastases. It is also an effective prognostic indicator for NPC patients. To determine the optimized utilization of 18F-FDG PET in the follow-up of NPC patients, further cost-effectiveness analysis of 18F-FDG PET in combination with conventional management is warranted.
Acknowledgments
The authors acknowledge Chien-Chung Chen (PET Center, National Taiwan University Hospital) for his technical assistance and also thank Shiang-Yih Ho (Department of Oncology, National Taiwan University Hospital) for her assistance in data collection.
Footnotes
Received Aug. 4, 2004; revision accepted Dec. 15, 2004.
For correspondence or reprints contact: Tony Hsiu-Hsi Chen, PhD, Institute of Preventive Medicine, National Taiwan University College of Public Health, No. 19, Hsu Chow Rd., Taipei, 100, Taiwan.
E-mail: stony{at}episerv.cph.ntu.edu.tw
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- 18F-FDG PET/CT for the Diagnosis of Residual or Recurrent Nasopharyngeal Carcinoma After Radiotherapy: A Metaanalysis
- The impact of 18F-FDG PET/CT on assessment of nasopharyngeal carcinoma at diagnosis
- PET scanning and Gamma Knife(R) radiosurgery in the early diagnosis and salvage "cure" of locally recurrent nasopharyngeal carcinoma
- Utility of 18F-FDG PET/CT Uptake Patterns in Waldeyer's Ring for Differentiating Benign from Malignant Lesions in Lateral Pharyngeal Recess of Nasopharynx
- Differential Roles of 18F-FDG PET in Patients with Locoregional Advanced Nasopharyngeal Carcinoma After Primary Curative Therapy: Response Evaluation and Impact on Management