


Abstract
Studies in animal models and epileptic patients have led to the suggestion that the basal ganglia (BG) are involved in seizures. PET with 6-18F-l-3,4-fluorodihydroxyphenylalanine (18F-fluoro-l-DOPA) has recently demonstrated a reduction of striatal dopamine uptake in drug-resistant epileptic patients with ring chromosome 20 (r20) using a multiple-time graphical analysis. The aim of the present study was to evaluate the involvement of dopamine in other epileptic syndromes using a multiple-time graphical analysis and the all-brain statistical parametric mapping (SPM) analysis. Methods: Patients with drug-resistant epilepsy were divided into 3 groups: group 1, with r20 epilepsy (n = 16; mean age ± SD, 21.5 ± 5.4 y); group 2, with resistant generalized “absence-like” epilepsy (n = 10; mean age, 32.3 ± 11.4 y); and group 3, with drug-resistant temporal lobe epilepsy with hippocampal sclerosis (n = 9; mean age, 35.2 ± 10.3 y). We compared 2 strategies of analysis of the 18F-fluoro-l-DOPA uptake constant (Ki, min−1) in BG using a multiple-time graphical analysis using regions of interest (the gold-standard method) and an SPM analysis using a voxel-by-voxel statistical t test to avoid a priori hypotheses in the analysis. Each epileptic group was compared with a group of healthy volunteers (n = 10; mean age, 45.1 ± 16.5 y). Results: A decrease of the mean Ki value was observed in the striatum in all groups of patients with both types of analysis. With multiple-time graphical analysis, the reduction was evident using the averaged Ki values over both hemispheres in each BG. Unilateral decreases in each BG were detected in SPM analysis. A ratio of decrease of 18F-fluoro-l-DOPA uptake was observed in the 3 groups of patients. Only the SPM analysis showed a decrease of 18F-fluoro-l-DOPA uptake ipsilateral to the seizure side in patients with temporal lobe epilepsy. Moreover, the all-brain SPM analysis showed a decrease of 18F-fluoro-l-DOPA uptake in the substantia nigra bilaterally (P < 0.001). Conclusion: This result confirms the involvement of dopamine neurotransmission in seizure control related to the type of epileptic syndrome. The difference in epileptic types may depend in part on the seizure frequency.
The role of the basal ganglia (BG) in epilepsy has been widely discussed recently. Although it is clear that BG circuits cannot generate seizures and are unlikely to be involved in their initiation, seizures are now known to modify the activity of this system (1). Furthermore, pharmacologic and electrophysiologic data from animal models of epilepsy suggest that the BG may function as a control circuit for some seizures (2,3). Thus, long-lasting and frequent seizures could suggest a dysfunction in the seizure control system with a possible involvement of striatal dopamine activity.
6-18F-l-3,4-fluorodihydroxyphenylalanine (18F-fluoro-l-DOPA) is a radiotracer that permits measurements of presynaptic dopaminergic function in the human brain with PET. Although it has frequently been used in studies of Parkinson’s disease (4,5), only a single publication seems to have investigated in vivo the anatomic and functional involvement of the dopamine network in human epilepsy (6). This study was performed on patients with epilepsy in relation to ring chromosome 20 (r20), a recently described epileptic syndrome (7) characterized by long-lasting “absence-like” and drug-resistant seizures. It showed a reduction of 18F-fluoro-l-DOPA uptake suggesting an impairment of striatal dopamine activity. The role of dopamine function in other types of drug-resistant epileptic syndrome remains unclear.
Several analytic methods have been proposed to quantify dopaminergic function using 18F-fluoro-l-DOPA. The method most often used is a multiple-time graphical approach (8,9) that provides the 18F-fluoro-l-DOPA uptake constant values (Ki, min−1) within regions of interest (ROI) placed over the striatal structures. Usually, these ROIs are placed manually by visual inspection of an integrated image. Nevertheless, this method is observer dependant and may not be well suited to small regions, such as the substantia nigra (SN), or regions with a low signal intensity, such as the posterior part of the putamen. An alternative method might be to use the statistical parametric mapping (SPM; Wellcome Department of Cognitive Neurology) software to analyze PET data (10,11). This method allows a voxel-by-voxel analysis of Ki parametric images and could reveal both focal striatal and extrastriatal changes in 18F-fluoro-l-DOPA uptake (12).
In the present study, we compared both methods of analysis to assess the rate of involvement of the BG in 3 different types of refractory epilepsy.
MATERIALS AND METHODS
Subjects
Thirty-five epileptic patients were selected for this study. They were recruited consecutively on the basis of the severity of their epilepsy and their resistance to antiepileptic treatments. Seizures could be either generalized (absence, myoclonic, atonic, tonic, or tonic–clonic) or partial. None of the patients had a brain lesion or cortical malformation. They were categorized into 3 groups.
Group 1 was 16 patients with r20 epilepsy (mean age ± SD, 21.5 ± 5.4 y). Most of the patients (14/16) with r20 had been described in a previous study (6). All had long-lasting nonconvulsive status epilepticus with a variable loss of consciousness.
Group 2 was 10 patients with generalized seizures (mean age, 32.3 ± 11.4 y) and are described in Table 1. They were selected according to several criteria: generalized symptoms (tonic–clonic, myoclonic, tonic, or absence seizures), generalized paroxysmal interictal abnormalities found on electroencephalography, no lesion found on MRI, and treatment with antiepileptic drugs that are recommended for generalized epilepsy (in all patients, seizure control was ineffective or worsening). In this group, seizures were less prolonged but frequent, occurring daily. Absence-like seizures were present in all patients with tonic–clonic seizures (n = 8), tonic seizures (n = 3), or myoclonic seizures (n = 2).
Clinical Characteristics of Patients with Generalized “Absence Like” Epilepsy (Group 2)
Group 3 was 9 patients with partial seizures related to hippocampal sclerosis (mean age, 35.2 ± 10.3 y) and are described in Table 2. They were selected on the basis of the following criteria: partial symptoms (complex or simple seizures), focal paroxysmal interictal abnormalities found on electroencephalography, unilateral hippocampal sclerosis found on MRI, and treatment with antiepileptic drugs that are recommended for partial epilepsy. Seizures were less frequent than in the other groups, occurring weekly.
Clinical Characteristics of Patients with Partial Temporal Lobe Epilepsy (Group 3)
All 35 epileptic patients had severe, drug-resistant epilepsy lasting for many years, with no difference between the 3 groups. All but 2 patients were being treated with at least 2 antiepileptic drugs. The PET studies were performed without stopping the epileptic treatment, because of the significant number of epileptic crises occurring in these patients.
These groups of epileptic patients were compared with a control group of healthy volunteers (n = 10; 5 men and 5 women; mean age, 45.1 ± 16.5 y). None had findings of psychiatric or neurologic illness either by medical history, clinical examination, or MRI. None of the healthy volunteers was taking medication.
This study was approved by the local Medical Bioethics Committee, and all epileptic and healthy subjects gave written informed consent after receiving a full explanation of the procedure. All subjects received 100 mg of carbidopa (an inhibitor of the DOPA decarboxylase; Merck Laboratories) 1 h before injection of the radiotracer.
Data Acquisition
MRI.
Brain MRI was performed on all subjects using a 1.5-T imager (Signa; General Electric Medical Systems). T2-weighted images of each subject were used to detect brain lesions and signal abnormalities in the BG. In addition, a T1-weighted spoiled gradient-echo acquisition with inversion recovery was performed to allow 3-dimensional reconstruction of MR images.
PET.
Subjects were examined using an ECAT EXACT HR+ (CTI/Siemens), a whole-body scanner that can simultaneously acquire 63 slices, each being 2.4 mm thick in 3-dimensional mode. This scanner has transverse and axial intrinsic spatial resolutions of 4.3 and 4.1 mm, respectively, at the center of the field of view (13,14). For all PET examinations, the subjects were positioned in the tomograph using 3-dimensional laser alignment. The attenuation coefficients were measured before injection with a 15-min scan using 3 rod sources of 68Ge (approximately 450 MBq in maximum total activity). Nine frames were acquired during the 90 min after intravenous injection of 144.0 ± 24.6 MBq of 18F-fluoro-l-DOPA. Synthesis of 18F-fluoro-l-DOPA followed a previously described electrophilic procedure (15). Datasets, acquired in 3-dimensional mode, were reconstructed using a Hanning apodization window (0.5 cycles per pixel cutoff) as radial and axial filters, providing an image resolution of 6.6 mm in the 3 directions (16).
Image Analysis
Time frames collected from 30 to 90 min were summed to create an integrated image that was used to define a circular occipital ROI (Ø = 25 mm) on 8–10 contiguous planes on MRI axial slices containing caudate and putamen nuclei (16,17). Circular ROIs of 10-mm diameter were drawn on the head of the caudate nucleus and on the putamen in each hemisphere on these planes. After coregistration between MRI and PET images, the ROIs were transposed over the PET slices and were used to determine the mean activity concentration values. The mean activity concentration values in the ROI for the left and right caudate nucleus, the occipital lobe, and the left and right putamen were calculated and used to generate regional time–activity curves. These time–activity curves were used to calculate the 18F-fluoro-l-DOPA uptake constant (Ki, min−1) in each striatal structure using multiple-time graphical analysis, with the occipital activity as input function (8,9). For each nucleus, Ki values were averaged over both hemispheres and expressed as mean ± SD. The Ki values for each epileptic group were compared with those of the healthy volunteers using ANOVA for repeated measures.
The mean occipital time–activity curve was also used as an input function to generate parametric images of the radiotracer using Patlak plots. Parametric images were normalized onto Talairach stereotactic space with SPM99 (18), using an integrated image from 0 to 90 min after injection to identify the transformation parameters. Scans from 3 temporal patients with hippocampal sclerosis in the right hemisphere were flipped so that the epileptogenic zone could be pooled on the same side. A smoothing procedure using an isotropic gaussian kernel of 6 mm in full width at half maximum was then applied to remove high-frequency noise from the images and to take into account anatomic differences between subjects. The SPM comparisons between the different groups of parametric images and control images were performed using t test analysis, and the changes were considered significant at a level of at least P < 0.005.
RESULTS
Decrease of 18F-Fluoro-l-DOPA Uptake in All Patients
Taking all the patients together (Fig. 1), no differences in Ki values were observed with the multiple-time graphical analysis between the right and left caudate and the right and left putamen (Table 3). No differences were apparent between the 2 sides in the healthy control group (Table 3).
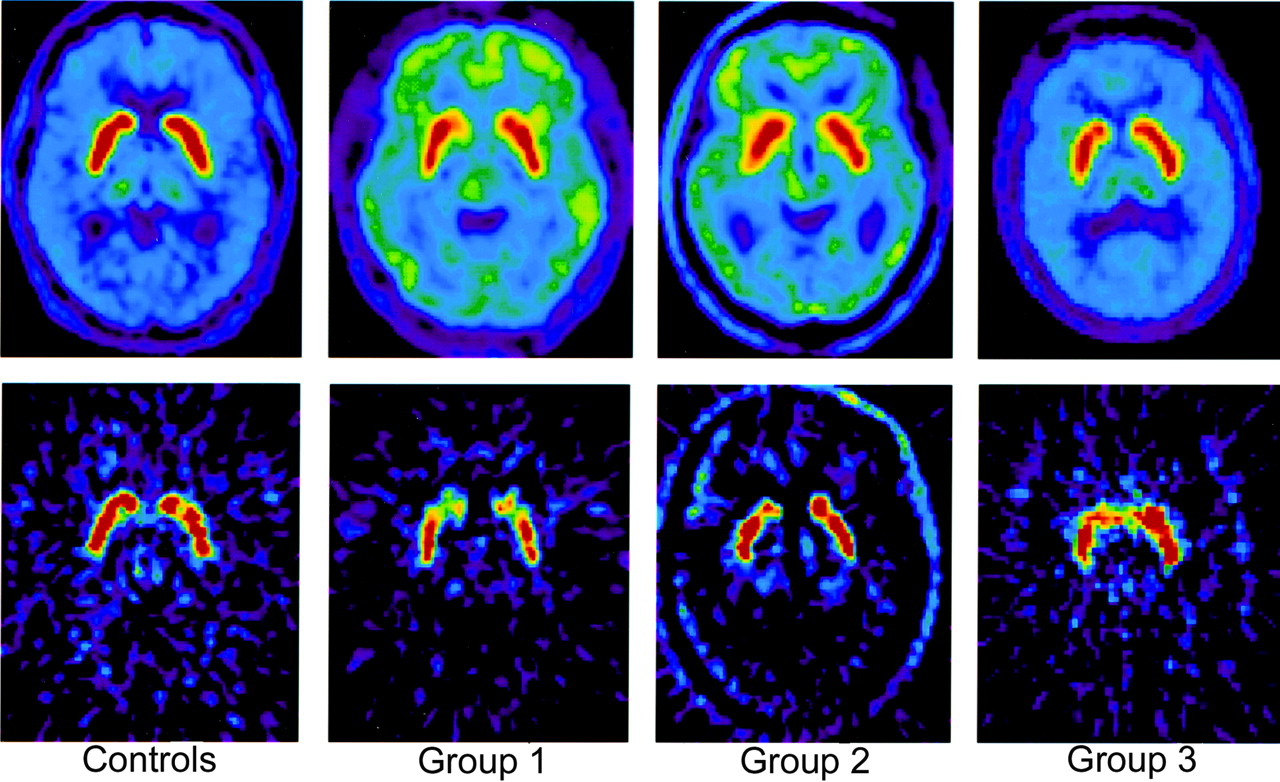
Examples of sum (top) and parametric images (bottom) of single slice at level of striatum from control subjects and epileptic patients. Radiotracer uptake is symmetrically decreased for patients in first 2 groups and asymmetrically decreased for patient with partial epilepsy (decrease is ipsilateral to epileptic focus).
18F-Fluoro-l-DOPA Uptake Constant (Ki, min−1) in Caudate and Putamen Nuclei for Both Cerebral Hemispheres and for Each Group of Subjects
However, a decrease of 18F-fluoro-l-DOPA uptake was detected for the averaged results from both nuclei in both hemispheres (Table 4). The comparison using the mean Ki values between the 35 epileptic patients and the 10 healthy volunteers (caudate, 0.0127 ± 0.0013; putamen, 0.0117 ± 0.0010) showed a significant decrease for the caudate (0.0109 ± 0.0014, P < 0.001, t test analysis) and the putamen (0.0105 ± 0.0016, P < 0.001, t test analysis).
Decrease of 18F-Fluoro-l-DOPA Uptake in Striatum of Patients with Multiple-Time Graphical and SPM Analysis, Compared with Control Group
The SPM analysis (corrected with P = 0.05 and 20 voxels) for the comparison of all 35 patients with the control subjects revealed a decrease of the 18F-fluoro-l-DOPA uptake mainly in the SN (x = 6, y = −24, and z = −14; P < 0.001, z score = 5.63) but also symmetrically in the putamen on both sides (x = 26, y = 12, and z = 4, P < 0.001, z score = 4.9; x = −22, y = 6, and z = −4, P = 0.003, z score = 4.7). No decrease was detected in the caudate nuclei (Table 4 and Fig. 2).
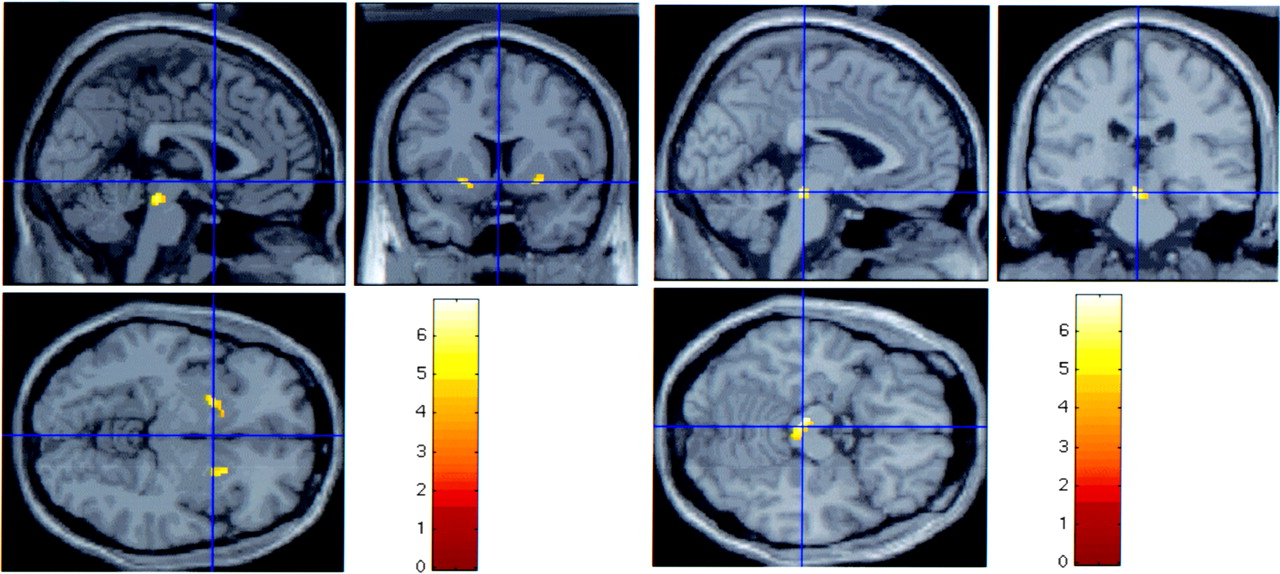
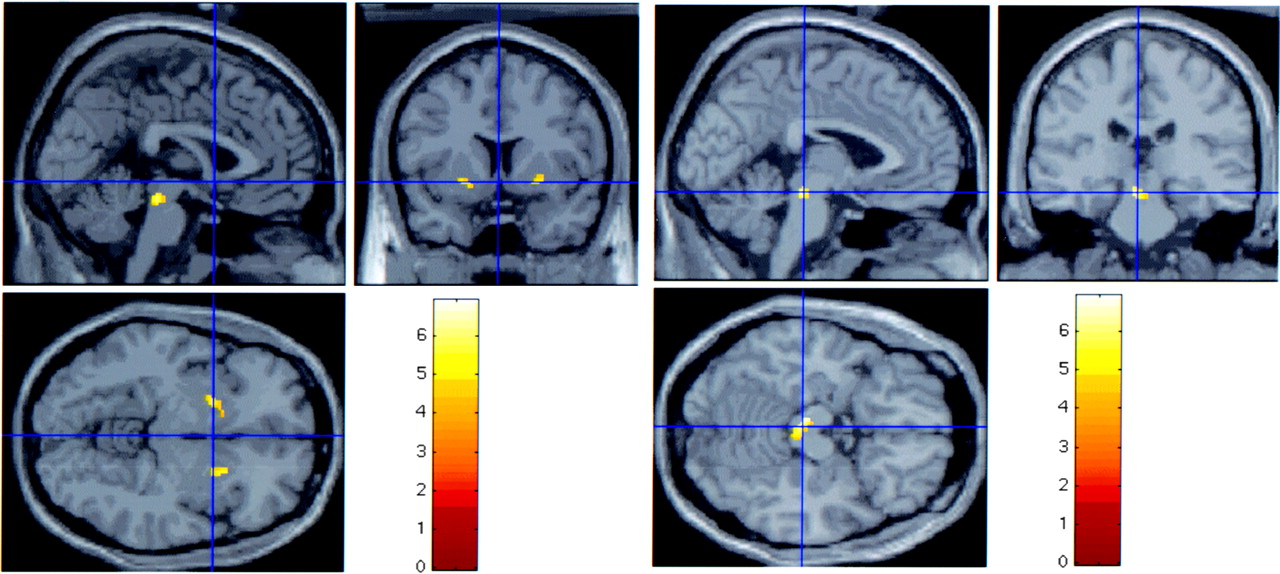
Decrease of 18F-fluoro-l-DOPA uptake in BG in all patients using SPM analysis. SPM analysis (corrected with P = 0.05 and 20 voxels) of all 35 patients reveals marked decrease of 18F-fluoro-l-DOPA uptake in SN and bilaterally symmetric decrease in putamen. Such a decrease is not found in the caudate.
Ratio of Decrease of 18F-Fluoro-l-DOPA Uptake in the 3 Groups of Patients
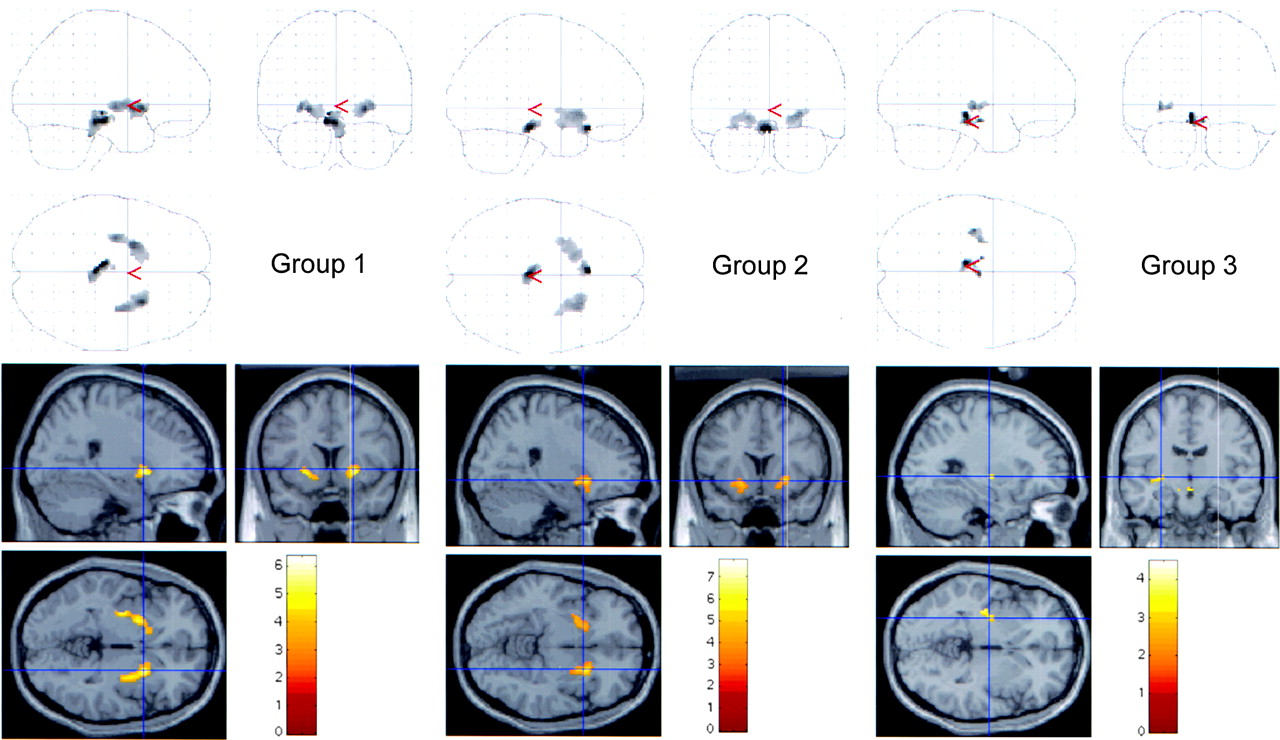
No differences were observed between the right and left Ki values for both nuclei of each epileptic group (Table 3). With the multiple-time graphical analysis, taking into account the right and left caudate and putamen, a significant decrease of the mean Ki values was observed in each patient group (Table 4). The ANOVA for repeated measures comparing each group of epileptic patients with the control subjects revealed significant differences between group 1 and control subjects for caudate and putamen (P < 0.001 for both nuclei). There was also a significant decrease between group 2 and control subjects (P < 0.001 and P < 0.02 for caudate and putamen, respectively). In the last group, no significant differences were observed in the BG, taking into account either both sides or the side ipsilateral or contralateral to the hippocampal sclerosis (P > 0.05 for both structures and both sides). SPM analysis revealed, in the 3 groups of patients, a symmetric decrease of radiotracer uptake in the SN (Table 4 and Fig. 3). 18F-Fluoro-l-DOPA uptake was also decreased in the putamen, bilaterally in patient groups 1 and 2 (P < 0.001) and ipsilateral to the hippocampal sclerosis in group 3, at a lesser degree (P < 0.005). Within groups, the largest decrease of 18F-fluoro-l-DOPA uptake was detected in the SN of group 2 (x = 0, y = −28, and z = −18, P = 0.001, z score = 3.08). There were no statistical differences between the first 2 groups in the putamen.
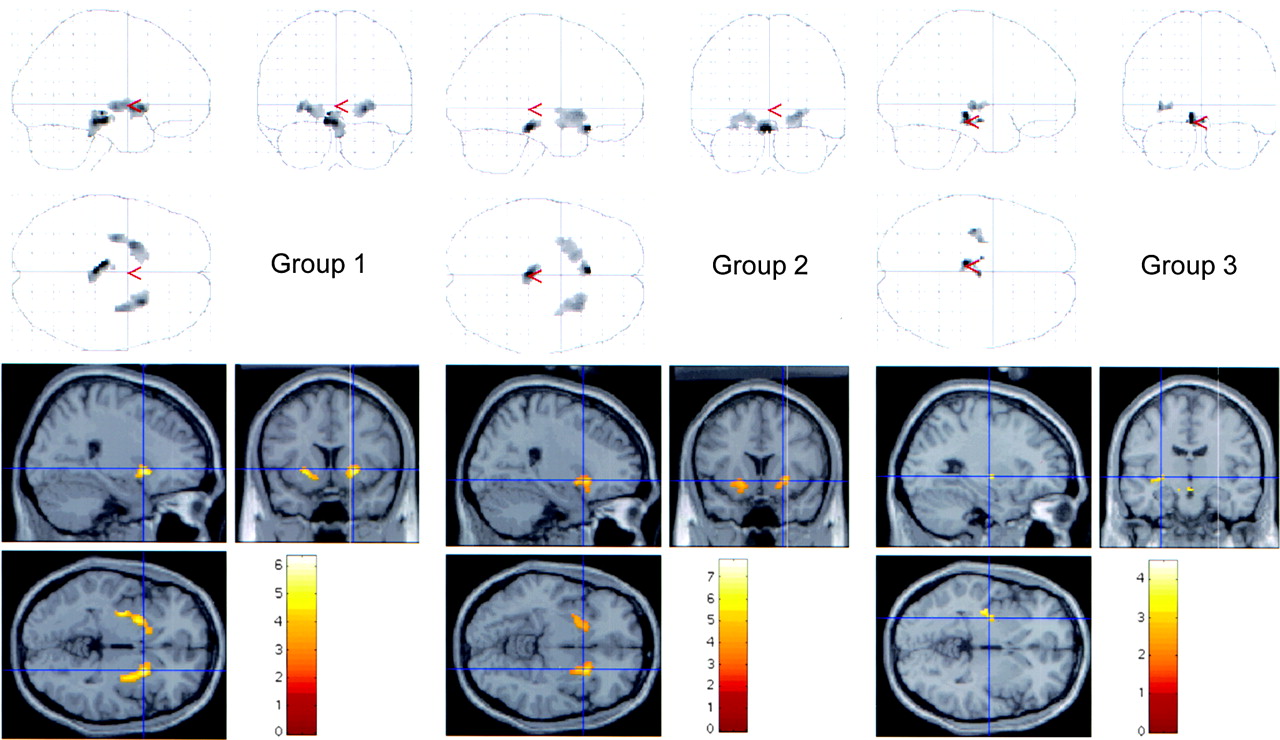
Ratio of decrease of 18F-fluoro-l-DOPA uptake in the 3 groups of patients with SPM analysis. Decrease of 18F-fluoro-l-DOPA uptake occurs mainly in SN but also in putamen. This decrease is bilateral in groups 1 and 2 (P < 0.001) and ipsilateral to hippocampal sclerosis in group 3 at a less conservative statistical level (P < 0.005).
DISCUSSION
We have observed a bilateral decrease of 18F-fluoro-l-DOPA uptake in the BG. Many previous functional imaging studies have demonstrated involvement of the thalamus and the BG in epilepsy (19–22). Usually, this involvement is considered to reflect the spread of seizure to these subcortical structures. Some functional imaging studies have pointed to a role for the BG in dystonic posturing (23–27). Involvement of the BG in epilepsy has not been demonstrated previously using PET. We have observed that 18F-fluoro-l-DOPA uptake in the BG is decreased in both generalized (groups 1 and 2) and focal (group 3) epilepsies, confirming the involvement of the BG in patients with r20 epilepsy (6) and furthermore demonstrating that this involvement is not specific to this syndrome.
Decreases in 18F-fluoro-l-DOPA uptake were largest in the groups with generalized epilepsy (groups 1 and 2). The high frequency of seizures in these patients could be contributing to the decreased dopamine metabolism. The bilateral and symmetric decrease of 18F-fluoro-l-DOPA uptake in these 2 groups contrasted with the unilateral decrease found in patients with partial seizures. The 18F-fluoro-l-DOPA decrease in patients with partial seizures was ipsilateral to the seizure side. This unilateral involvement is probably related to the seizure focus and strongly suggests that the reduced uptake did not depend on the antiepileptic drugs, in contrast to some (but not all) reports in the literature. Some antiepileptic drugs increase extracellular dopamine in animal studies (28–32), whereas others induce reversible Parkinson-like symptoms (33,34). Possibly, a decreased dopamine neurotransmission in BG could affect seizure frequency in distinct epilepsy syndromes. However, no spontaneous seizures were observed after dopaminergic deprivation in experimental studies (35), and further studies are needed to determine whether the decrease of 18F-fluoro-l-DOPA uptake is a cause or a consequence of seizures. In fact, and as our group has discussed in a previous paper (6), use of 18F-fluoro-l-DOPA PET does not allow one to determine whether the deficit of dopamine observed in epileptic patients is due to cell loss or reduced storage. However, the homogeneous aspect of this deficit (for groups 1 and 2), as well as the fact that both caudate and putamen nuclei are affected, suggested that it is not a consequence of a cellular loss of dopaminergic neurons involved in the same mechanism as in Parkinson’s disease. In Parkinson’s disease the deficit is asymmetric, as well as more severe in the putamen than in the caudate (5,17). The possibility that the deficit in the dopaminergic neurotransmission generates the absence-like discharges in epilepsy patients appears unlikely. In humans, neuroleptic drugs may induce seizures by blocking several types of receptors besides dopamine D2 receptors. Finally, previous data from the literature lead us to suggest that the lengthy seizures observed in these patients could be the consequence of a dopaminergic activity deficit.
On the other hand, in our study, the antiepileptic treatments used were clearly different between groups of patients, as shown in Tables 1 and 2, and therefore could not be used to precisely determine their specific effects on dopaminergic neurons. This difference between groups of patients is related to the fact that treatment for generalized epilepsy is not so effective in partial seizures. Treatment for partial seizures could enhance the frequency of generalized seizures. However, these results provide evidence that dopamine might be a new target for antiepileptic treatments and suggest that pharmacologic treatment or cerebral stimulation to enhance dopamine metabolism might be a useful therapeutic option in seizure control.
The ROI with multiple-time graphical analysis is a classic method to assess 18F-fluoro-l-DOPA uptake. We also used SPM analysis because it offered several advantages (10,12,36). First, it permits good spatial normalization of individual images to a standard stereotactic space (36), allowing comparison of the same region among different subjects. This ability avoids systematic errors in ROI positioning or erroneous identification of striatal or extrastriatal regions in PET images with a low signal-to-noise ratio. Second, the SPM technique reveals the site of any change with no need for operator definition of anatomic subdivisions. In the present study, such definition was especially difficult for small structures such as the putamen. Thus, SPM may allow detection of changes in several regions within the striatum. Finally, SPM reveals changes in extrastriatal regions too small to be analyzed using the ROI method (12,36).
In this study, SPM analysis was shown to be more accurate than multiple-time graphical analysis in detecting the decrease of 18F-fluoro-l-DOPA uptake in epileptic patients. It was necessary to average Ki values between the right and left BG to demonstrate differences with ROI analysis, whereas SPM analysis could demonstrate changes separately for each hemisphere. A significant decrease was observed in the 2 patient groups with generalized epilepsies, but in group 3 (focal epilepsies), only SPM analysis showed a decrease in the putamen ipsilateral to the focus. The absence of significant results using the multiple-time graphical analysis is probably related to the small difference between patients and control subjects and the limited size of the anatomic structure. However, ROI graphical analysis detected in the caudate an 18F-fluoro-l-DOPA uptake decrease that was not apparent from SPM analysis. Several hypotheses might explain this discrepancy. First, the loss of dopaminergic terminals might be relatively small but too widespread to be evident in SPM analysis. Second, the ROI was defined to include only the anterior part of the caudate, whereas SPM analyzed the entire structure, possibly masking a predominantly anterior dopaminergic loss.
Some limitations of the graphical analysis in small anatomic structures were apparent in our study. Changes in 18F-fluoro-l-DOPA uptake in SN could not be analyzed adequately with the ROI technique (12,36). However, a reduction in uptake was clearly demonstrated with the SPM analysis. The SN is one of the major output structures of the BG circuit, and its activity is modulated by the cortex through direct and indirect transsubthalamic and transstriatal pathways. Several studies have shown that pharmacologic inhibition of the SN suppresses both behavioral and electroencephalogram expressions in different models of generalized seizures (2,3,37,38). Specific populations of SN neurons appear to be involved in the control of different forms of seizures (3,39). The capacity of SPM analysis to resolve changes in striatal and extrastriatal dopamine metabolism might permit evaluation of new medical strategies.
Atrophy of the BG might contribute to a decreased 18F-fluoro-l-DOPA uptake. However, a relationship between atrophy and the 18F-fluoro-l-DOPA decrease has been discussed in the study of Biraben et al. (6). In the present study, BG MRI findings were normal in all patients and striatal gray-matter volumes were similar in epileptic patients and control subjects.
CONCLUSION
The decreased 18F-fluoro-l-DOPA uptake shown in this study provides the first direct evidence that the BG, and especially the SN, is involved in human epilepsy. The unilateral BG involvement in partial seizure seems unlikely to result from the antiepileptic drugs. However, the rate and identity of the BG structures involved in partial and generalized epilepsy differed. In our opinion, SPM analysis proved to be more accurate than techniques requiring definition of a priori ROIs. SPM analysis allowed detection of changes in BG 18F-fluoro-l-DOPA uptake with good spatial resolution in epileptic patients.
Acknowledgments
The authors thank the radiochemists and nurses of the Service Hospitalier Frédéric Joliot for their assistance and Drs. Richard Miles and Héric Valette for their critical reading of the manuscript.
Footnotes
Received Aug. 18, 2004; revision accepted Nov. 2, 2004.
For correspondence or reprints contact: Maria-João Ribeiro, MD, PhD, Service Hospitalier Frédéric Joliot, DRM/DSV, CEA, 4, place du Général Leclerc, F-91406 Orsay, France.
E-mail: ribeiro{at}shfj.cea.fr
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Enlarged Perivascular Spaces in the Basal Ganglia Across Epilepsy Subtypes
- Converging PET and fMRI evidence for a common area involved in human focal epilepsies
- Dopamine and epilepsy: Hints of complex subcortical roles
- Reduced dopamine transporter binding in patients with juvenile myoclonic epilepsy
- Basal ganglia involvement in temporal lobe epilepsy: A functional and morphologic study