


Abstract
Transplant vasculopathy is a major cause of morbidity and mortality in heart transplantation. The proliferation of coronary vascular smooth muscle cells is a hallmark of transplant vasculopathy. The goal of this study was to detect coronary vascular smooth muscle cell proliferation in a swine model by imaging regions of uptake of a monoclonal antibody (Z2D3) labeled with 111In. Methods: Coronary-to-right carotid artery transplantation was performed in 10 Yucatan minipigs with coronary arteries from farm pigs as donors. In 5 of these experiments, the right carotid artery was also grafted to the left carotid artery as a homograft. In 1 farm pig, the left and right carotid arteries were switched. After 44 ± 22 days (mean ± SE), animals were injected with 5-bromo-2-deoxyuridine (BrDU) and 111In-Z2D3 F(ab′)2. Approximately 24 h later, the pigs underwent planar and SPECT imaging. After the imaging session, the pigs were sacrificed and the vessels were removed. Ex vivo autoradiography of all grafts was performed. Next, the tissues were immersion fixed, paraffin embedded, sectioned, and stained for histologic or immunohistologic examination. Quantitative morphometry was performed. A smooth muscle cell proliferation index, calculated as (BrDU- and actin-stained cells/actin-stained cells) × 100, was correlated with in vivo and ex vivo radiotracer uptake. Results: Patency or neovascularization was demonstrated in 10 of 10 allografts and 5 of 6 homografts. Ten of the scans were positive for focal tracer uptake in the neck in the area corresponding to the graft site, and 6 were negative. Actin- and BrDU-stained cells were seen in the media of allografts and in the recanalized lumen of occluded homografts. A smooth muscle cell proliferation index of 30 was used as a cutoff for scan positivity, on the basis of previous work. Analysis by the χ2 test indicated significant concordance (P < 0.01). Ex vivo vessel count ratios were significantly correlated with the smooth muscle cell proliferation index (r2 = 0.528, P < 0.01). Conclusion: The use of monoclonal antibody Z2D3 tagged with 111In allows the detection of proliferating smooth muscle cells and correlates with the intensity of cell proliferation. This diagnostic method could allow early noninvasive detection of transplant vasculopathy.
Transplant vasculopathy is one of the major causes of morbidity and mortality after heart transplantation (1). This disease, of multiple etiologies, affects the coronary arterial and venous system without involving the vessels outside the transplanted grafts (2–4). Because of denervation of the transplanted heart, patients generally do not present with symptoms of angina related to myocardial ischemia or infarction. They usually present with symptoms of heart failure, cardiac arrhythmia, or sudden death.
Noninvasive and invasive diagnostic modalities are used for the detection of transplant vasculopathy (5–8). Intravascular ultrasound in cardiac catheterization laboratories has shown intimal thickening of the coronary arteries 1 year after heart transplantation in up to 75% of heart transplant patients (9). Standard noninvasive diagnostic testing, including dobutamine stress echocardiography and myocardial perfusion nuclear imaging, is not highly accurate for detecting transplant vasculopathy (5). It is therefore important to investigate new noninvasive techniques that would allow the detection of early transplant vasculopathy with increased accuracy.
Radiolabeled monoclonal antibodies have been used in the diagnostic imaging of other diseases, such as prostate and colon cancer (10,11), as well as for the targeting of therapeutic agents into certain neoplastic tissues (12–14). A novel monoclonal antibody (Z2D3) tagged with 111In has been shown to have a high specificity for proliferating vascular smooth muscle cells (10). A comparison of staining of Z2D3 antibody and antimacrophage antibody in serial frozen sections of a human atheroma has shown that although both antibodies stain in the region of the atheroma, the 2 stained regions are not the same but are complementary. The area of the atheroma stained by Z2D3 is not stained by antimacrophage antibody and vice versa. Furthermore, the neointima stained by Z2D3 also is stained by antibody to proliferating nuclear cell antigen and antibody to actin (15). Subsequently, the lipid antigen targeted by Z2D3 was identified to be a mixture of 7-dehydrocholesterol and a quaternary ammonium salt (16). Because the hallmark of transplant vasculopathy is smooth muscle cell proliferation, the purpose of this investigation was to evaluate the use of monoclonal antibody Z2D3 in the early noninvasive detection of transplant vasculopathy in a swine model.
MATERIALS AND METHODS
To perform this investigation, a coronary-to-carotid artery model of transplant vasculopathy previously described by Tixier et al. (17) was used. All experiments were performed within National Institutes of Health guidelines for the care and use of laboratory animals and with the approval of the Rhode Island Hospital Animal Care Committee. A coronary artery segment from farm pigs was transplanted in the carotid artery position of Yucatan minipigs. Animals were sacrificed at various time intervals after implantation, designed to capture the period of maximal intimal proliferation. Before they were sacrificed, all animals were injected with 111In-labeled monoclonal antibody Z2D3 and 5-bromo-2-deoxyuridine (BrDU), a pyrimidine analog. Before euthanasia, all animals were imaged by use of a nuclear γ-camera. After euthanasia, the transplanted grafts were harvested. Explanted grafts were submitted to autoradiography. Histologic analyses were performed with hematoxylin–eosin stain, Movat’s pentachrome stain, and double immunohistochemical staining with anti-BrDU and antiactin antibodies. An index of smooth muscle cell proliferation was correlated with 111In-Z2D3 uptake in the transplanted grafts.
Surgical Procedures
Seven domestic farm pigs and 10 Yucatan minipigs were used for this investigation. Yucatan minipigs were all castrated males weighing between 25 and 30 kg and were obtained from Charles River Laboratories. Castrated male domestic farm animals weighed, on average, between 50 and 55 kg. Before the surgery, all animals were injected with xylazine and tiletamine–zolazepam (0.5–1.0 mL/22.5 kg [50 lb]) to immobilize the animals and for the placement of intravenous lines in the ear veins. Animals then were anesthetized with thiopental sodium (Pentothal; Abbott Laboratories) (300–700 mg) and maintained in that state by inhalation anesthesia with isofluorane (0.25%–1.25%) and nitric oxide (0.5%).
Donor farm pigs were prepared in a sterile fashion before a lateral thoracotomy was performed. The heart was exposed, and the 3 main coronary arteries were identified. The animals were euthanized with thiopental sodium and KCl, the heart was explanted, the right coronary artery was dissected, and 1 or 2 segments approximately 20 mm in length were removed. After the arteries were harvested and placed in heparinized saline, recipient pigs were prepared in a sterile fashion. A midline incision approximately 10 cm in length was made to expose the right carotid artery. Once exposed, approximately 2 cm of the native carotid artery was removed, and the coronary artery segment obtained from a donor animal was implanted by use of an end-to-end anastomosis in most cases. In a similar manner, Yucatan minipigs underwent homograft transplantation of the explanted carotid artery into the contralateral position to serve as a self-control. During the postoperative period, the animals received 325 mg of aspirin for at least 1 wk. A subset of animals received subcutaneous heparin at 5,000 U twice a day for 1 wk as well as azathioprine at 0.5 mg/kg twice a day until the time of sacrifice. Antibiotic prophylaxis was used in all animals.
Monoclonal Antibody Z2D3 Labeling and Imaging
F(ab′)2 fragments of chimeric IgG antibody Z2D3 were prepared as previously described (18). Before injection, 150 μg of antibody Z2D3 was labeled with approximately 74 MBq of 111In by column chromatography to separate bound antibody from free 111In. The animal was lightly sedated, and the radiolabeled antibody was injected via the ear vein. At the same time, BrDU was injected at 50 mg/kg. At 18–24 h after tracer injection, the animal was again sedated and anesthetized. A second dose of BrDU at 50 mg/kg was given. Animals underwent planar and SPECT imaging by use of medium-energy collimators with an energy window centered on the 174- and 247-keV photopeaks of 111In interfaced to a Nuclear Mac (NC Systems). All in vivo images were obtained with a 128 × 128 matrix for planar imaging and with a 64 × 64 matrix for SPECT imaging. Ex vivo images of the vessels were obtained with a 128 × 128 matrix. Planar images were obtained with anterior, posterior, and lateral orientations during an acquisition time of 20 min. SPECT images were obtained at 1-min intervals in a 360° acquisition. After the completion of imaging, the animals were euthanized with an overdose of thiopental sodium and saturated KCl, and the grafts were dissected.
Images were interpreted for focal uptake in the region of the neck by consensus of 3 readers who did not know the site of the allograft or homograft placement. Planar ex vivo images of allografts and homografts were obtained during an acquisition time of 30 min. Target-to-background count density ratios were obtained for each graft. Image count density ratios were correlated with number of counts by use of a well counter.
Histologic Staining and Analyses
After the transplanted segments were explanted, the tissues were fixed with 10% formalin and placed in paraffin to allow sectioning. Histologic staining was performed with hematoxylin–eosin stain, Movat’s pentachrome stain, and double staining with antiactin and anti-BrDU antibodies. Histologic images were evaluated for the following criteria: patency, neovascularization, inflammation, intimal proliferation, and recanalization of the vessel. A smooth muscle proliferation index was determined with the following formula: (BrDU- and actin-stained cells/actin-stained cells) × 100. Optical microscopy at ×60 was used to determine the number of cells per visual field. Ten observations were obtained, and the mean of these observations was calculated. We previously demonstrated that a smooth muscle cell proliferation index cutoff of 30 correlated with uptake detected by a γ-camera in an in-stent restenosis model with 111In-Z2D3 (19).
Statistical Methods
The smooth muscle cell proliferation index was compared with scan-positive and scan-negative groups by χ2 analysis. Statistical significance was set at P < 0.05. The vessel count ratio (target to background) was plotted against the proliferation index by simple linear regression analysis.
RESULTS
Radiotracer Uptake
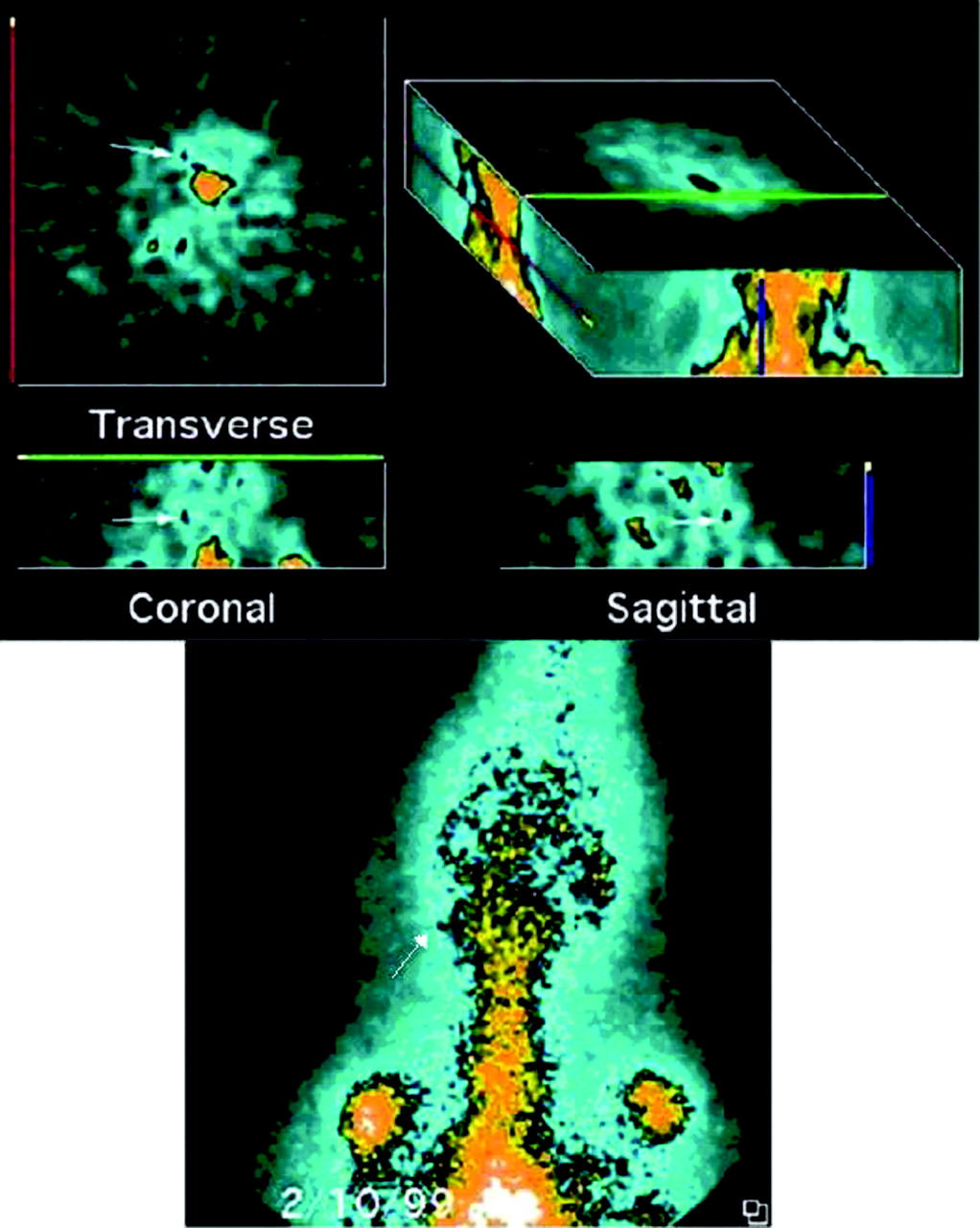
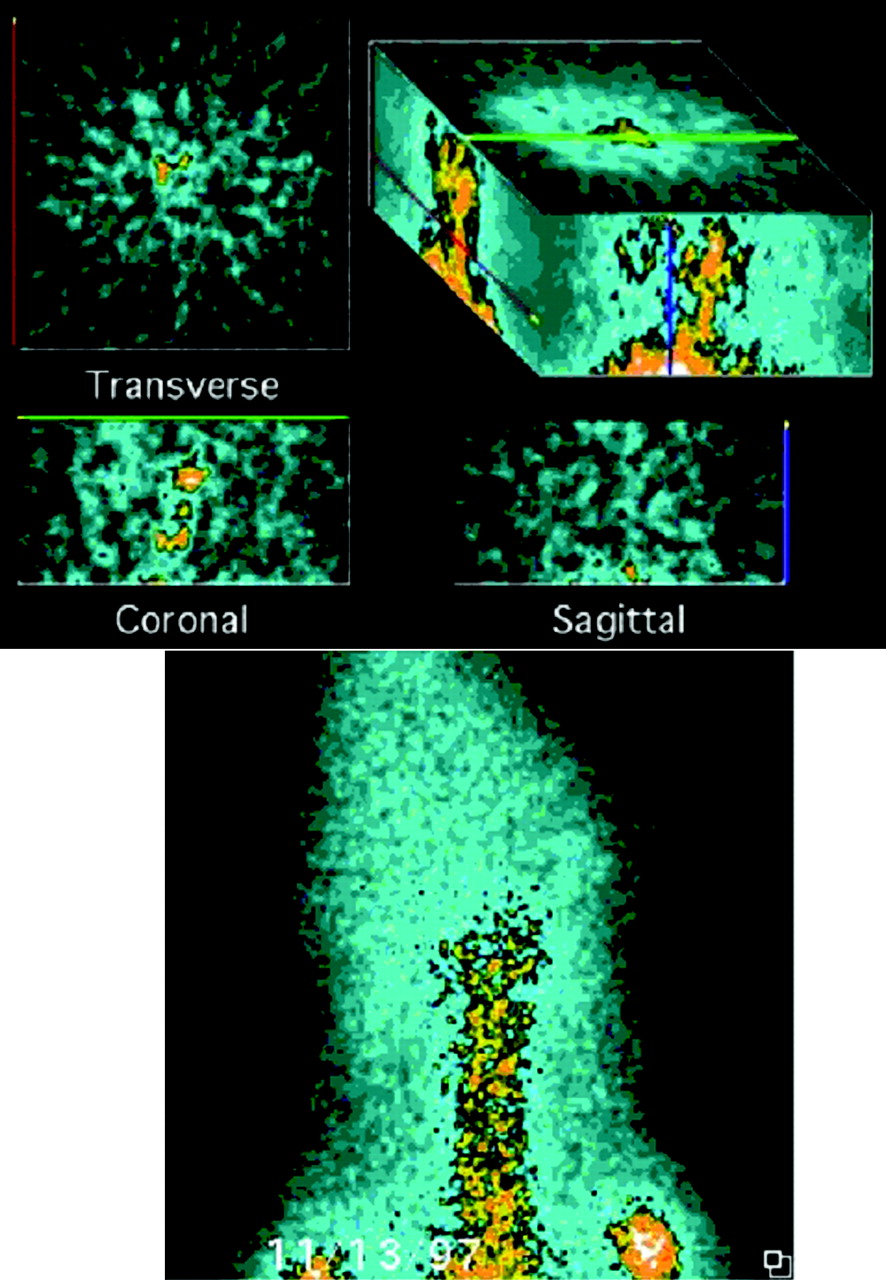
The mean ± SE labeling efficiency was 43.7% ± 0.13%, and the mean ± SE doses of 111In injected were 48.5 ± 4.8 MBq in the allografts and 61.8 ± 8.1 MBq in the homografts. Fifty percent of the allografts showed focal tracer uptake in the neck, and 43% of the homografts showed focal uptake. Examples of SPECT images with and without focal uptake are shown in Figures 1 and 2.

Transplant pig 8 on postprocedure day 42. An allograft of the left circumflex coronary artery to the right carotid artery site and a homograft of the right carotid artery to the left carotid artery position are shown on SPECT images in transverse, coronal, and sagittal views (top) and on a planar image (bottom). White arrows indicate focal 111In tracer uptake at the allograft site. No uptake was seen at the homograft site.
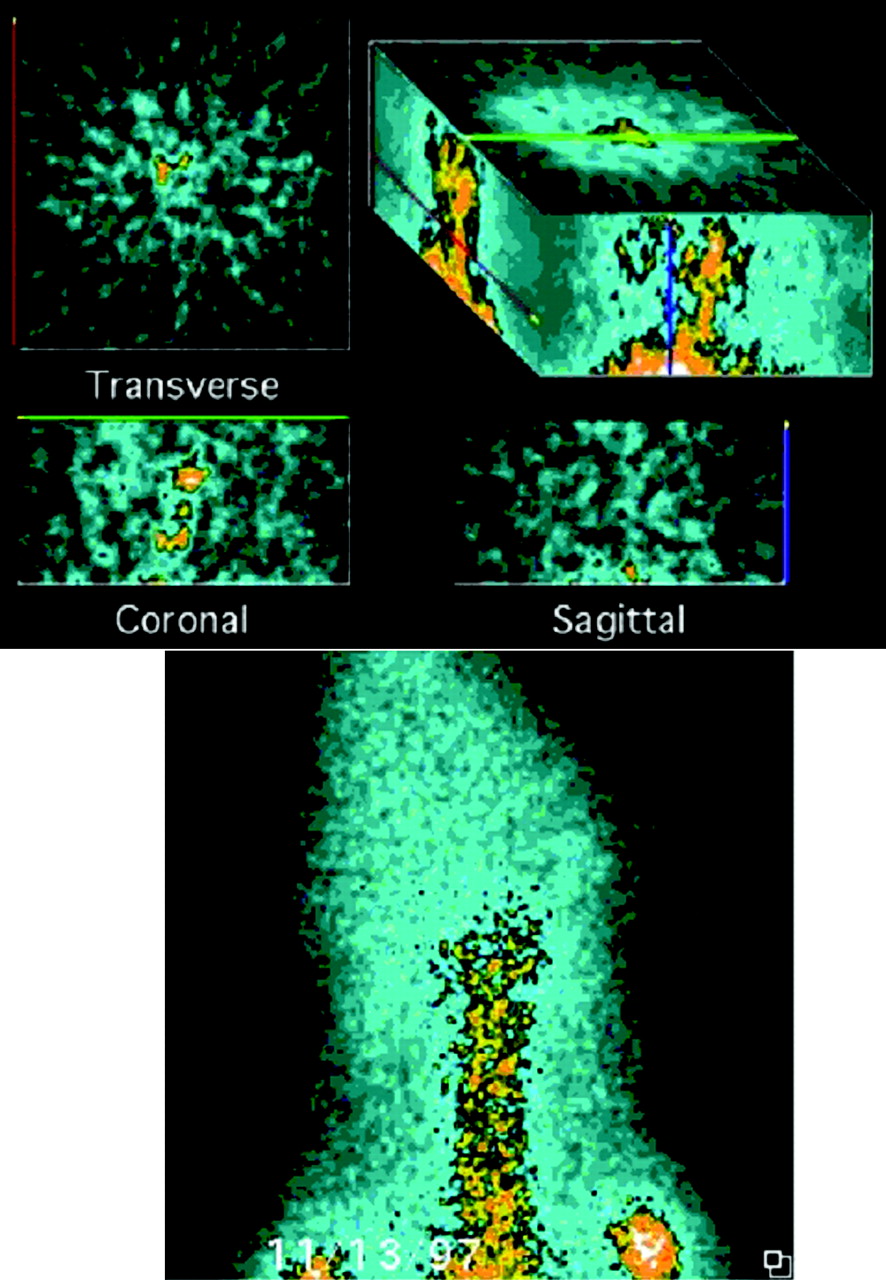
Transplant pig 11 postprocedure day 14. A homograft of the left carotid artery to the right carotid artery position is shown on SPECT images in transverse, coronal, and sagittal views (top) and on a planar image (bottom). No uptake was seen at the homograft site.
The target-to-background count ratios ranged from 1.3 to 3.9. All scan-positive vessels had count ratios of ≥1.8. A target-to-background ratio of ≥1.8 was found in 60% of the allografts and in 57% of the homografts.
Histologic Analyses
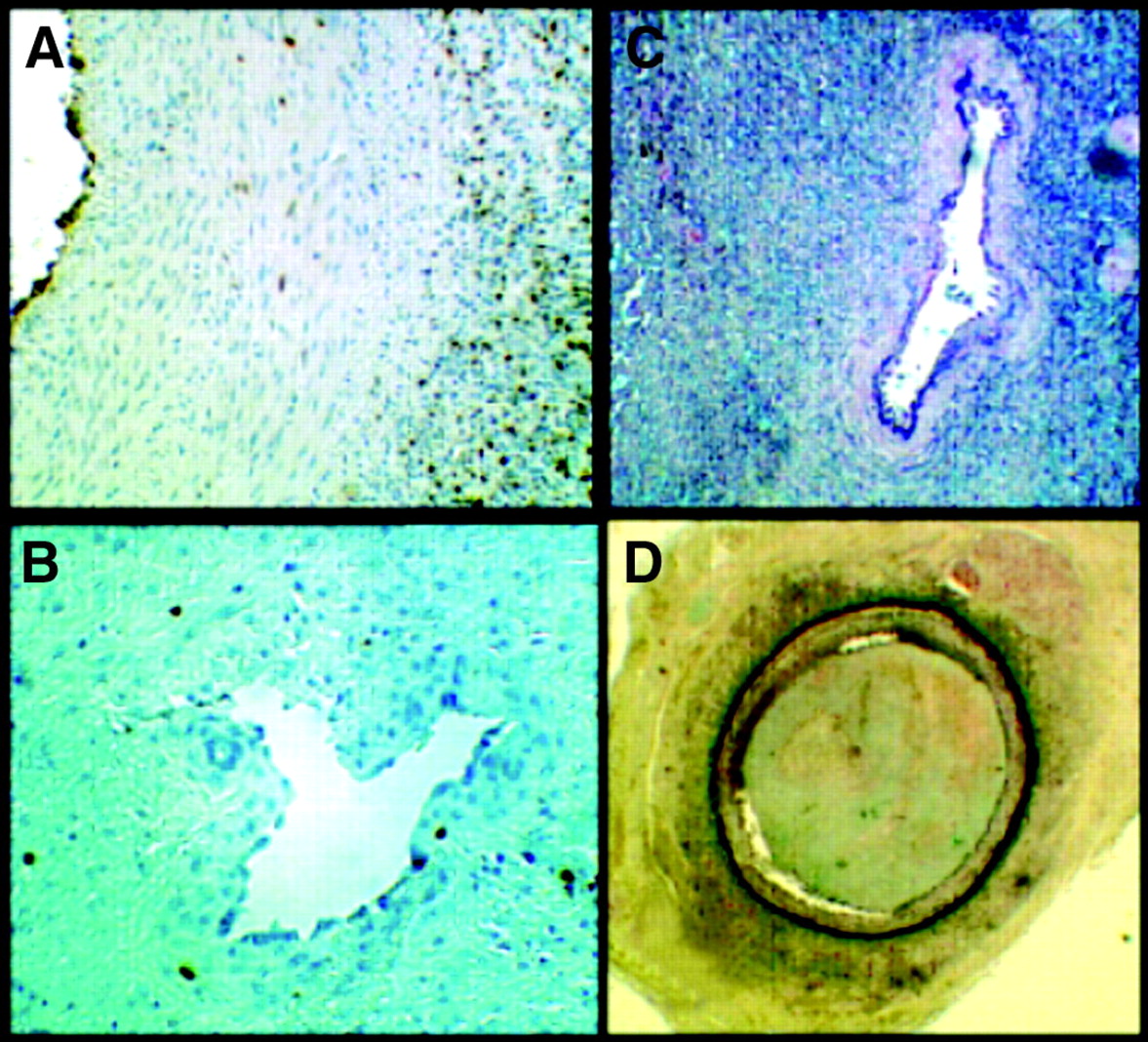
Two (20%) of the allograft vessels were patent, without evidence of a fresh or old thrombus, whereas all of the homograft vessels were occluded. Intimal proliferation was seen in the 2 patent allografts. Inflammatory infiltrates were seen in all of the allografts and in few of the homografts. Various degrees of recanalization of an old thrombus was observed in 70% of the allografts and in 30% of the homografts. Neovascularization within occluded grafts and in the periadventitial area was observed in 80% of the occluded allograft vessels and in 83% of the occluded homograft vessels. Representative histologic images are shown in Figure 3.

(A) Anti-BrDU antibody immunostaining with hematoxylin counterstaining showing a patent vessel with marked intimal proliferation in the lumen. (B) Anti-BrDU antibody immunostaining with hematoxylin counterstaining showing an occluded vessel with thrombus recanalization. (C) Trichrome stain showing an occluded vessel with neovessel formation. (D) Movat’s pentachrome stain showing an occluded vessel with old thrombus formation.
Correlation Between Intimal Proliferation and Nuclear Imaging Uptake
The correlation between count ratios for the in vivo imaged grafts and the smooth muscle cell proliferation index is shown in Table 1. A significant relationship between in vivo uptake and a smooth muscle cell proliferation index of >30 was indicated by χ2 analysis (P = 0.008). A significant correlation was demonstrated between ex vivo count ratios and the smooth muscle cell proliferation index (r2 = 0.528, P = 0.0032) (Fig. 4).
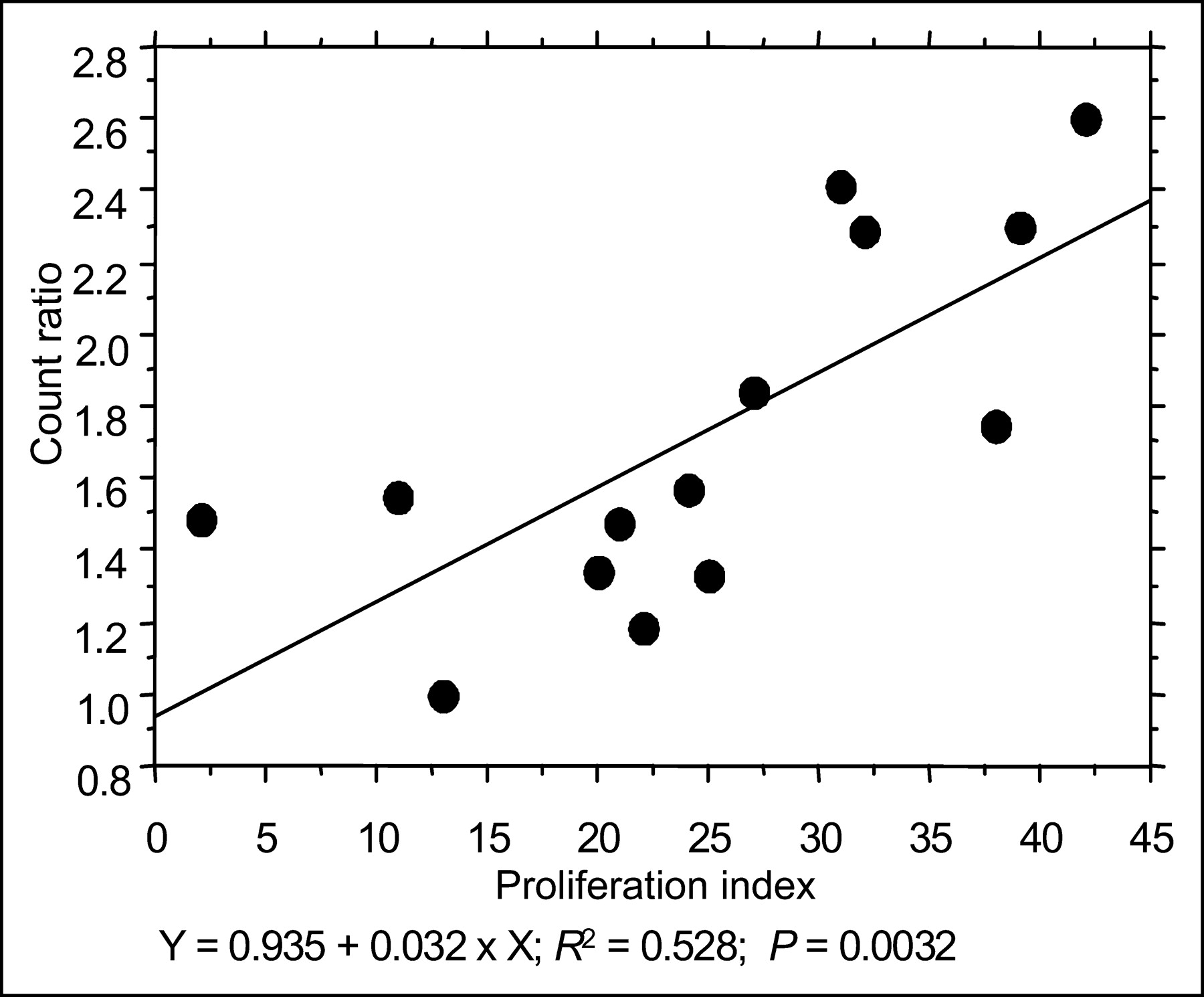
Correlation between ex vivo counts and the smooth muscle cell proliferation index.
Correlation Between In Vivo Uptake and Smooth Muscle Cell Proliferation Index
DISCUSSION
In this study we tested the hypothesis that monoclonal antibody Z2D3, targeting a lipid antigen complex produced by proliferating vascular smooth muscle cells and tagged with 111In, can detect transplant vasculopathy in an animal model. Despite a high rate of graft thrombosis, we were able to show a correlation between radiotracer uptake and proliferation of vascular smooth muscle cells in the neointima of the few patent allografts and in neovessels in occluded allografts and homografts. The smooth muscle cell proliferation index correlated statistically with in vivo (P = 0.008) as well as ex vivo (P = 0.0032) imaging data. This high degree of correlation confirms the ability of this noninvasive imaging technique to detect smooth muscle cell proliferation by use of a nuclear γ-camera and monoclonal antibody Z2D3 tagged with 111In.
Neovascularization in occlusive atherosclerotic antegrade perfusion was previously described (20,21). In all of the allografts in our study, inflammatory infiltrates were noted, especially at the level of the media and adventitia and at the suture level, whereas minimal inflammation was seen in the homografts. In the process of histomorphometry, only actin- and BrDU-positive cells were counted; inflammatory cells were excluded. There was no correlation between the extent of inflammation and scan positivity. Our data indicate that the radiotracer was labeling only proliferating vascular smooth muscle cells.
Z2D3, an IgM class, κ light-chain monoclonal antibody, was produced by fusion of spleen cells from BALB/c mice immunized with homogenized human atherosclerotic plaque tissues and murine myeloma cells. Z2D3 is specific for a lipid antigen complex produced by proliferating smooth muscle cells of the intima of a human atheroma (22). The antibody was demonstrated to colocalize in tissues staining positively for proliferating nuclear cell antigen and α-actin, identifying the cells as proliferating smooth muscle cells. The antigen recognized by antibody Z2D3 was known to contain a complex of 2 or more chemically dissimilar, low-molecular-weight molecules with sterol moieties. The surrogate antigens are now known to be a mixture of 7-dehydrocholesterol and benzyldimethylhexadecylammonium chloride and a mixture of 7-dehydrocholesterol and palmitoylcholine. Before the advent of the surrogate antigens, the relative affinity of the antibody was assessed to have an immunohistochemical staining score of 3+ (23). A hybridoma Z2D3 IgM subclone then was genetically engineered to produce a chimera with a human IgG1 constant region (15), allowing enzymatic degradation of the chimeric antibody to F(ab′)2 fragments by pepsin digestion. Focal accumulation of high-affinity 111In-Z2D3 was subsequently demonstrated in the rabbit atherosclerotic aorta, whereas low-affinity nonspecifically radiolabeled antibodies did not show appreciable uptake (15). We previously showed neointimal uptake of rhodamine-labeled Z2D3 in the swine model of overexpansion restenosis to be localized to areas of proliferating vascular smooth muscle cells (18,24). Carrio et al. showed the localization of human atherosclerotic lesions with 111In-labeled monoclonal antibody Z2D3 in human atherosclerotic plaques within the carotid artery (25).
To improve counts per pixel and target-to-background ratios in single-photon imaging with antibodies, Khaw et al. and Torchilin et al. modified antibodies with negatively charged chelating polymers. This process permitted the chelation of a large number of trivalent metallic radiolabel molecules per modified antibody molecule (26,27) and improved target-to-background ratios by simultaneously increasing the amount of radiolabeled antibody delivered to the target and reducing the electrostatic attraction to nontarget cells with an overall weak negative charge. Using 111In-labeled diethylenetriaminepentaacetic acid–modified succinylated polylysine Z2D3 F(ab′)2 in animal experiments, Narula et al. demonstrated that with higher specific radioactivities and lower antibody doses, lesions could be visualized earlier (28). Furthermore, 111In-Z2D3 (Fab′)2 uptake in vivo in proliferating neointimal tissue in a swine model of coronary stent restenosis was reported (18), and this uptake also was reported to correlate with the strength of the biologic signal (19). In this study, we provide a novel application for the use of a 111In-tagged monoclonal antibody by imaging neointimal proliferation under a different pathologic condition—transplant vasculopathy. In addition, we were able to confirm the ability to quantify ex vivo the degree of vascular smooth muscle cell proliferation with the intensity of the signal. These results provide enough evidence to support the further development of this antibody for the imaging of disease conditions that involve the proliferation of smooth muscle cells.
We used a published model of transplant vasculopathy in which a segment of the coronary artery of a farm pig is transplanted into the carotid artery position of a Yucatan minipig (17). This model has several advantages over other transplant vasculopathy models: surgery of low complexity, use of a coronary artery versus a peripheral resistant vessel, and early postoperative recovery. We were unable to duplicate reported results for vessel patency. Despite the lack of patency in most grafts, we saw on in vivo imaging focal uptake corresponding to high target-to-background count ratios. We demonstrated the development of neovessels with proliferating smooth muscle cells in occluded vessels.
CONCLUSION
Although we were unable to obtain a high vessel patency rate, the development of neointima in patent allografts as well as neovascularization in occluded grafts allowed the identification of proliferating smooth muscle cells by use of monoclonal antibody Z2D3 tagged with 111In. There was a high correlation of the intimal proliferation index with ex vivo count ratios and with in vivo uptake detected by a nuclear γ-camera. For this reason, Z2D3 tagged with 111In appears to be a candidate for further development as a marker for the early detection of transplant vasculopathy.
Footnotes
Received Mar. 9, 2004; revision accepted Oct. 29, 2004.
For correspondence or reprints contact: Javier Jimenez, MD, Division of Cardiology (D-39), School of Medicine, University of Miami, Jackson Memorial Medical Center, 1611 N.W. 12th Ave., Miami, FL 33136.
E-mail: Jjimenez2{at}med.miami.edu
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.