


Abstract
Salivary gland dysfunction is one of the common side effects of high-dose radioiodine therapy for thyroid cancer. The purpose of this study was to determine whether an early start of sucking lemon candy decreases salivary gland injury after radioiodine therapy. Methods: The incidence of the side effects of radioiodine therapy on the salivary glands was prospectively and longitudinally investigated in 2 groups of patients with postsurgical differentiated thyroid cancer with varying regimens for sucking lemon candy. From August 1999 to October 2000, 116 consecutive patients were asked to suck 1 or 2 lemon candies every 2–3 h in the daytime of the first 5 d after radioiodine therapy (group A). Lemon candy sucking was started within 1 h after radioiodine ingestion. From November 2000 to June 2002, 139 consecutive patients (group B) were asked to suck lemon candies in a manner similar to that of group A. In the group B, lemon candies were withheld until 24 h after the ingestion of radioiodine. Patients with salivary gland disorders, diabetes, collagen tissue diseases, or a previous history of radioiodine therapy or external irradiation to the neck were excluded. Thus, 105 patients in group A and 125 patients in group B were available for analysis. There were no statistical differences in the mean age (55.2 y vs. 58.5 y), average levels of serum free thyroxine (l-3,5,3′,5′-tetraiodothyronine) (0.40 ng/dL vs. 0.47 ng/dL), and the mean dose of 131I administered (3.96 GBq vs. 3.87 GBq) between the 2 groups. The onset of salivary side effects was monitored during hospital admission and regular follow-up on the basis of interviews with patients, a visual analog scale, and salivary gland scintigraphy using 99mTc-pertechnetate. When a patient showed a persistent (>4 mo) dry mouth associated with a nonfunctioning pattern on salivary gland scintigraphy, a diagnosis of xerostomia was established. Results: The incidences of sialoadenitis, hypogeusia or taste loss, and dry mouth with or without repeated sialadenitis in group A versus group B were 63.8% versus 36.8% (P < 0.001), 39.0% versus 25.6% (P < 0.01), and 23.8% versus 11.2% (P < 0.005), respectively. Permanent xerostomia occurred in 15 patients in group A (14.3%) and 7 patients in group B (5.6%) (P < 0.05). In both groups, bilateral involvement of the parotid gland was the most frequently seen and was followed by bilateral involvement of the submandibular gland. Conclusion: An early start of sucking lemon candy may induce a significant increase in salivary gland damage. Lemon candy should not be given until 24 h after radioiodine therapy.
Salivary glands have the sodium iodine symporter (1–3). Therefore, radioiodine 131I to treat patients with postsurgical thyroid cancer is taken up in the salivary glands. The concentration of 131I in the salivary gland, which is about 30–40 times of that in the plasma (1), is sufficient to cause salivary gland injury. Salivary dysfunction is the most common side effect associated with high-dose radioiodine 131I therapy for differentiated thyroid cancer (1–10). Additionally, salivary gland dysfunction can be observed even when the dose of 131I administered is relatively low (10). Because xerostomia impairs the quality of life of a patient for the life-long period, prevention of salivary damage is an important issue. So far, the only successful strategy to prevent salivary damage after 131I therapy is the prophylactic use of 2-(S)-(3-aminopropylamino)ethylphosphorothioic acid (amifostine) (11–14). Unfortunately, availability of this drug is currently limited. Salivation-inducing snacks, such as lemon candy, have been also presumed to be helpful in prevention of salivary side effects of 131I therapy (15,16). However, there has been no established evidence that lemon candy actually decreases injury of the salivary gland after 131I therapy. Despite its frequent use, the optimal regimen of lemon candy in 131I therapy remains unestablished. The purpose of this study was to determine whether an early start of sucking lemon candy decreases the side effects of radioiodine therapy on the salivary glands.
MATERIALS AND METHODS
Patient Groups
Two groups of postsurgical differentiated thyroid cancer patients, who were referred to our institute for 131I therapy to ablate the remnant thyroid tissue or to treat metastatic tumor, were prospectively studied under varying regimens of lemon candy sucking. The ingredients of the candy consist of sugar, glucose syrup, cornstarch, vegetable oil, ascorbic acid, condensed lemon juice, sorbitol, and natural flavorings. A container of lemon candy (110 g per container; 429 calories) contains 0.1 g of protein, 5.3 g of fat, 97.6 g of carbonate, 370 mg of sodium, and 3,000 mg of vitamin C. From August 1999 to October 2001, 116 consecutive patients were instructed to suck 1 or 2 lemon candies every 2–3 h in the daytime of the first 5 d after 131I therapy (group A). Sucking of lemon candy was started within an hour after ingestion of 131I. From November 2000 to June 2002, 139 consecutive patients (group B) were instructed to suck lemon candy in a manner similar to that of group A. However, lemon candies were not administered until 24 h after the ingestion of 131I. In both groups, thyroid hormone replacement was withdrawn 3 wk before 131I therapy. A low-iodine diet was started 7 d before 131I therapy. The dose of 131I administered ranged from 2.66 to 5.55 GBq. All patients were instructed to drink as much water or iodine-free beverages as possible throughout the first 4 d after the ingestion of 131I. In patients who had developed nausea due to hypothyroidism or had difficulty in drinking a large amount of water, dripped infusion of saline (500–1,000 mL/d) was performed. Patients with a previous history of salivary gland disorders, diabetes, collagen tissue disease, or previous 131I therapy or external irradiation to the neck were excluded from the study. Thus, 105 patients in the group A and 125 patients in the group B were available for analysis. There were no significant differences in the mean age, sex, and mean levels of free thyroxine (l-3,5,3′,5′-tetraiodothyronine) (FT4) (ng/dL) at radioiodine therapy and the average dose of 131I administered between the 2 groups (Table 1). The incidence of side effects on the salivary glands after 131I therapy was prospectively determined. The onset of sialadenitis, taste dysfunction (hypogeusia or taste loss), dry mouth, and xerostomia after 131I therapy was monitored during the period of hospitalization and in the regular follow-up (1- to 6-mo interval) for >24 mo on the basis of interviewing patients, including a questionnaire, a 10-cm visual analog scale (VAS), and salivary gland scintigraphy using 99mTcO4−. Patients fasted for 2 h before salivary gland scintigraphy and were placed spine in the Water’s position. After an intravenous injection of 147 MBq of 99mTcO4−, dynamic anterior images were acquired in a 256 × 256 matrix every 30 s for 30 min using a GCA-9300DI digital γ-camera system (Toshiba) equipped with a low-energy, high-resolution collimator. Lemon juice was administered using a straw at 20 min after injection as a stimulant of salivary discharge. Regions of interest were symmetrically drawn on the combined dynamic images in the bilateral parotid glands, submandibular glands, and backgrounds in the neck to determine time–activity curves for the 4 major salivary glands. Scan images and time–activity curves were interpreted by 2 independent nuclear medicine physicians with classification into 5 patterns: normal, mildly to moderately hypofunctioning, obstructive, severely hypofunctioning, and nonfunctioning (Fig. 1). When a patient complained of persistent dry mouth (>4 mo) associated with a nonfunctioning pattern on salivary gland scintigraphy, xerostomia was diagnosed. In patients with xerostomia, VAS and salivary gland scintigraphy were reexamined 4–6 mo later to determine whether the salivary gland dysfunction was reversible.
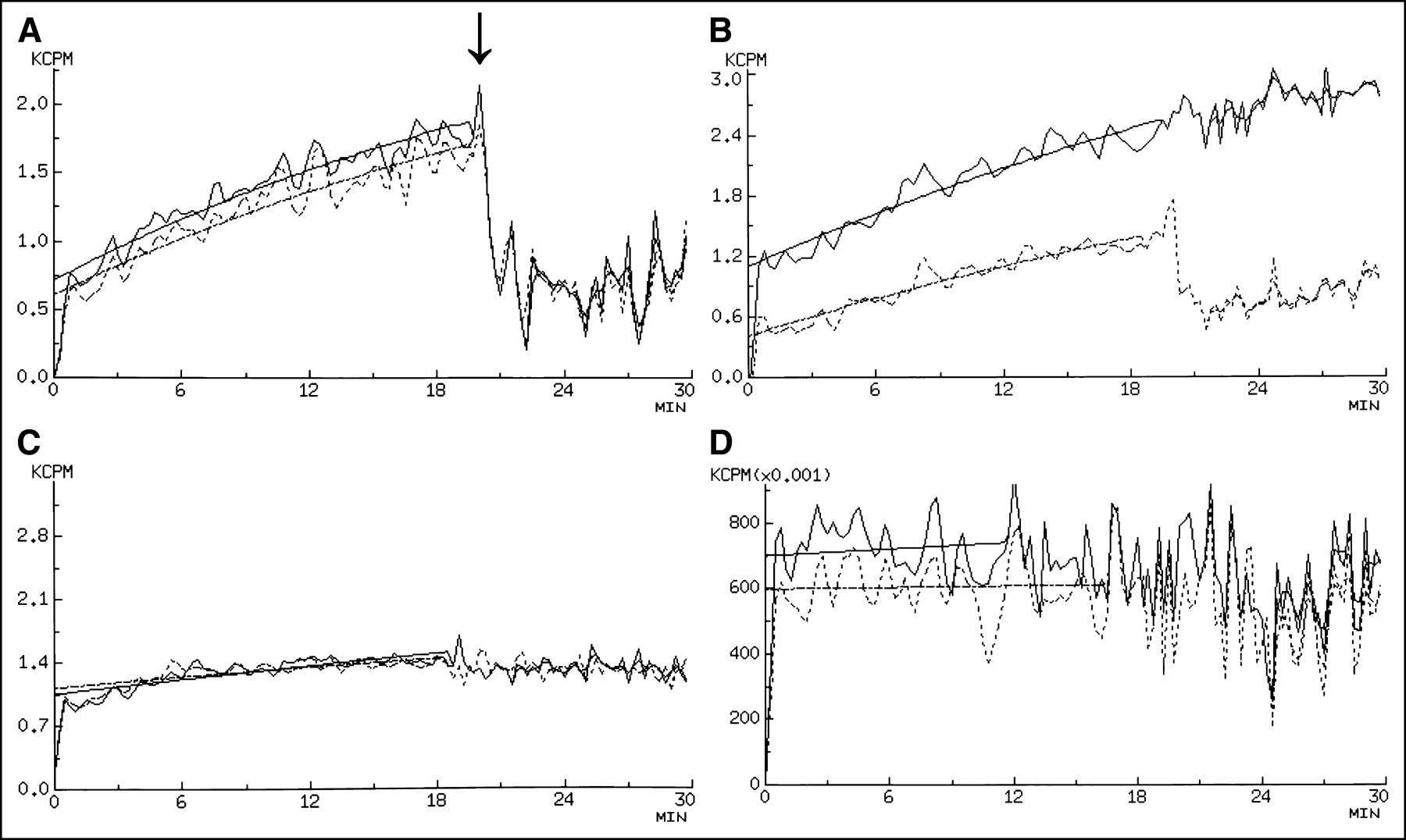
Typical time–activity curves of 99mTcO4− for bilateral parotid glands in patients with postsurgical thyroid cancer after high-dose radiodione therapy. Solid line is curve for right parotid gland; dashed line is curve for left parotid gland. (A) Normal: Lemon juice was administered at 20 min after injection of 99mTcO4− (↓). (B) Mild to moderately hypofunctioning (lower curve) and obstructive (upper curve). (C) Severely hypofunctioning. (D) Nonfunctioning.
Patient Characteristics
Statistical Analysis
Data are expressed as mean ± SD. A nonpaired t test and χ2 test were used for group comparisons. P values < 0.05 were considered significant.
RESULTS
Sialoadenitis and taste dysfunction were observed in 43 and 17 patients in group A and in 34 and 20 patients in group B, respectively. Sialadenitis occurred between 1 to 4 d after 131I therapy. Taste dysfunction developed 4–60 d after 131I therapy. Additionally, 24 patients in group A and 12 patients in group B experienced both sialoadenitis and taste dysfunction. A subjective dry mouth associated with or without repeated sialoadenitis became apparent 4–13 mo after 131I therapy in 25 patients in group A and in 14 patients in group B, respectively. Of 25 patients in group A, 10 had a previous episode of sialadenitis, 3 had taste dysfunction, and 12 had both. Of 14 patients in group B, 6 had a previous episode of sialadenitis, 3 had taste dysfunction, and 5 had both. Subsequently, xerostomia was confirmed in 15 patients in group A and 7 patients in group B (Figs. 2 and 3) 7–17 mo after 131I therapy. Eleven patients in group A and 5 patients of group B had either of the acute side effects of 131I therapy on the salivary glands before development of xerostomia. However, 4 patients in group A and 2 patients in group B had xerostomia without preceding sialoadenitis or taste dysfunction. The incidences of sialoadenitis, taste dysfunction, and dry mouth in group A versus group B were 63.8% versus 36.8% (P < 0.001), 39.0% versus 25.6% (P < 0.01), and 23.8% versus 11.2% (P < 0.005), respectively (Table 2). Xerostomia occurred in 14.3% of patients in group A and 5.6% in group B (P < 0.05). Once developed, xerostomia was not improved in any of the patients during the follow-up period. The incidences of sialoadenitis, taste dysfunction, dry mouth, and xerostomia were significantly higher in group A than in group B. Bilateral involvement of the parotid glands was the most frequently noted, which was followed by bilateral involvement of the submandibular glands and unilateral involvement of either parotid gland or parotid gland (Table 3). Five patients in group A and 2 patients in group B showed involvement of all 4 major glands.

Early and late side effects of high-dose radioiodine therapy on salivary glands in group A patients (pts).

Early and late side effects of high-dose radioiodine therapy on salivary glands in group B patients (pts).
Comparison of Incidence of Salivary Side Effects After High-Dose Radioiodine Therapy Between Group A and Group B
Salivary Gland Involvement
DISCUSSION
To our knowledge, this is the first study to pose a question with regard to the use of a siaolgogue immediately after 131I therapy for preventing radiation injury in the salivary glands. The incidence of sialadenitis, taste dysfunction, dry mouth, and permanent xerostomia was significantly higher in group A than in group B. Moreover, the incidences of dry mouth and xerostomia in group A were increased up to >2-fold of those in group B. An early start of sucking lemon candy did not contribute to reducing radiation injury from 131I to the salivary glands.
The reported frequencies of salivary gland damage caused by 131I therapy for thyroid cancer vary depending on the diagnostic strategy. Studies that investigated the incidence of salivary side effects of 131I therapy by means of questionnaire showed a relatively low frequency of sialoadenitis or xerostomia (8,10). Studies including salivary gland scintigraphy in assessment of salivary function were associated with a higher incidence of side effects. An abnormal uptake or excretion of 99mTcO4− on salivary scintigraphy was observed in about 73% of 33 patients treated with 3.69–38.7 GBq of 131I (9). In 39 patients with subjective salivary symptoms after >37 GBq of 131I, subsequent xerostomia was seen in 44%, whereas salivary gland dysfunction on salivary gland scintigraphy was observed in 65% of the patients (17). The status of lemon candy sucking was not described in these reports. Bohuslavizki et al. concluded that, despite the standard protection regimen using ascorbic acid as a sialogogue, radioiodoine induced the loss of salivary gland parenchymal function (18). However, 83 of 106 patients in their study had benign thyroid diseases and the thyroid function at the time of 131I therapy was not described. Compared with those reports, the patients treated with amifostine had apparently fewer incidences of salivary dysfunction (11,12). We longitudinally investigated the incidences of side effects on the salivary glands after the initial 131I therapy for postsurgical thyroid cancer. The acute side effects were diagnosed on the basis of subjective symptoms, while xerostomia was diagnosed by combination of VAS and salivary gland scintigraphy. Although the precise reason for our finding remains unknown, it is likely that there were certain relationships between the salivary side effects observed and the timing of starting to suck lemon candy since there was no significant difference in patient characteristics, preparations for the 131I administered, and the dose of 131I administered between the 2 groups.
There are possible explanations for the higher incidence of salivary side effects in group A than in group B. Sucking lemon candy has been recommended on the basis of assumptions that lemon candy accelerates clearance of radioiodine from the salivary glands and that the salivary gland function in patients is normal. However, lemon candy increases not only salivary flow but also salivary gland blood flow (Fig. 4). Doppler sonographic studies demonstrated a significant increase in blood flow in the major salivary glands after the use of sialogogue (19–22) in both normal and pathologic conditions. It is anticipated that 131I uptake in iodine-avid tissues, including salivary glands, rises up to 24 h after ingestion of 131I. Because 131I uptake by the remnant thyroid or metastatic thyroid cancer is substantially lower than the normal thyroid gland and clearance of 131I from the systemic circulation may be delayed due to a decreased glomerular filtration rate in the hypothyroid condition, the blood concentration of 131I at an early period after 131I ingestion should be considerably high. If continuous sucking of lemon candy constantly enhances blood flow to the salivary gland, a greater amount of 131I may be delivered to the salivary glands. After 24 h after ingestion, 131I uptake by iodine-avid tissues reaches a plateau and the majority of radioactivity is excreted into the urine. Subsequent sucking of lemon candy does not further increase 131I uptake in the salivary glands and predominantly helps wash 131I out from the salivary glands. Additionally, it is uncertain whether salivary gland function is really preserved in every thyroidectomized patient in a hypothyroid condition. Animal studies suggest that hypothyroidism modifies saliva secretion as well as the morphologic structure of the salivary gland (1,23–25). Caglar et al. pointed out that patients who underwent a large resection tended to show a higher incidence of salivary gland dysfunction after 131I therapy (17). Additionally, enlarged salivary glands are not an uncommon finding in patients with hypothyroidism (26). Sialogogue may inadequately stimulate saliva secretion in a subset of patients with an impaired patency of the salivary duct to enhance stasis of 131I in the duct. The effects of neck dissection and thyroid hormone withdrawal on salivary gland function need to be investigated further. With the use of recombinant human thyroid-stimulating hormone (rhTSH), radioiodine kinetics and salivary or renal functions in the patients are expected to be normal (27–30). It will be interesting to investigate the incidence of salivary side effects in patients undergoing radioimmunotherapy (RIT) with rhTSH treatment.
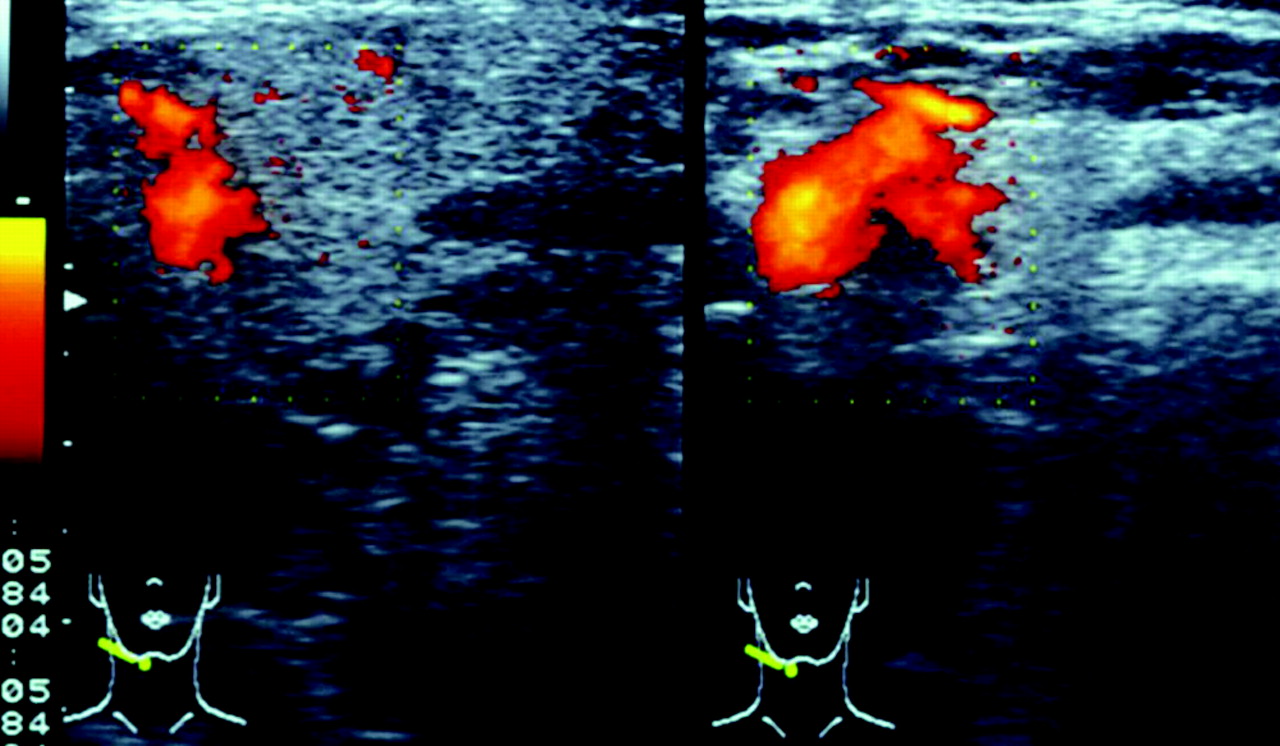
Power mode Doppler ultrasonography in healthy subject at rest (right) and at simulated condition by lemon candy (left). By use of lemon candy, contraction of gland was associated with increase in blood flow (orange color).
The major limitation of our study is that it was neither double blinded nor controlled. We did not have a group without lemon candy sucking. On encountering unexpectedly higher salivary side effects in group A, the patients in group B tended to be treated more intensively with steroids or nonsteroidal antiinflammatory drugs for sialoadenitis and with a drug containing zinc acetate or vitamin B12 for taste dysfunction. The follow-up period after RIT was not identical in the 2 groups. However, all side effects, including xerostomia, were apparent until 17 mo after RIT and the difference in the follow-up period must not have affected the frequency of salivary side effects observed. Another limitation was the diagnostic strategy for salivary gland dysfunction. In the process of this study, we encountered patients showing disagreements between subjective symptoms and salivary gland scintigraphy results with regard to a dry mouth. Some patients complained of dry mouth despite normal or mildly impaired salivary scintigraphy results. Other patients with impaired salivary gland scintigraphy results did not complain of a dry mouth. Such patients did not have a diagnosis of xerostomia. Although salivary gland scintigraphy is a useful tool in assessment of salivary function (31), overlapping in the quantitative parameter of salivary gland scintigraphy between xerostomic patients with Sjögren’s syndrome and healthy control subjects has been reported (32). Similar to previous reports, we did not perform any tests to investigate the absolute salivary flow or take the effects of the drugs for an attempt of treating nonthyroidal complications, such as vasodepressors or tranquilizers, into consideration.
Meanwhile, it seems reasonable that lemon candy is administered in combination with drugs such as reserpine (33), atropine, or, ideally, amifostine since 131I uptake in the salivary glands can be suppressed by these drugs. Moreover, it should be kept in mind that early use of sialgogue may enhance the salivary gland side effects of 131I therapy. For preventing life-long salivary gland complications of 131I therapy, the timing of lemon candy sucking should be carefully selected.
CONCLUSION
Stimulation of saliva flow by means of lemon candy in close temporal proximity to 131I administration is associated with increased side effects on subsequent salivary gland function. Lemon candy should be given after 24 h following 131I therapy.
Footnotes
Received Jul. 16, 2004; revision accepted Sep. 27, 2004.
For correspondence or reprints contact: Kunihriro Nakada, MD, PhD, Department of Nuclear Medicine, Hokkaido University Graduate School of Medicine, Kita-15, Niushi-7, Kita-ku, Sapporo, 060-8638, Japan.
E-mail: metnakada{at}yahoo.co.jp
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Normal-Tissue Tolerance to Radiopharmaceutical Therapies, the Knowns and the Unknowns
- Effect of External Cooling on 177Lu-PSMA Uptake by the Parotid Glands
- The SNMMI Practice Guideline for Therapy of Thyroid Disease with 131I 3.0
- Complications of Radioactive Iodine Treatment of Thyroid Carcinoma
- Influence of Vitamin C on Salivary Absorbed Dose of 131I in Thyroid Cancer Patients: A Prospective, Randomized, Single-Blind, Controlled Trial
- Preparation with Recombinant Human Thyroid-Stimulating Hormone for Thyroid Remnant Ablation with 131I Is Associated with Lowered Radiotoxicity
- Reducing the Incidence of 131I-Induced Sialadenitis: The Role of Pilocarpine
- The Dental Safety Profile of High-Dose Radioiodine Therapy for Thyroid Cancer: Long-Term Results of a Longitudinal Cohort Study
- Role of Radioactive Iodine for Adjuvant Therapy and Treatment of Metastases
- European consensus for the management of patients with differentiated thyroid carcinoma of the follicular epithelium.
- Re: Does Lemon Candy Decrease Salivary Gland Damage After Radioiodine Therapy for Thyroid Cancer?
- Post-surgical use of radioiodine (131I) in patients with papillary and follicular thyroid cancer and the issue of remnant ablation: a consensus report