


Abstract
This study evaluated the accuracy of 99mTc-sestamibi scintigraphy and neck ultrasonography in patients with primary hyperparathyroidism (PHPT) and the role of intraoperative hand-held γ-probes in minimally invasive radioguided surgery (MIRS) of patients with a high likelihood of a solitary parathyroid adenoma (PA). The study was undertaken under the aegis of the Italian Study Group on Radioguided Surgery and Immunoscintigraphy (GISCRIS). Methods: Clinical records were reviewed for 384 consecutive PHPT patients undergoing radioguided surgery using a low dose of 99mTc-sestamibi. Selection of patients for MIRS instead of traditional bilateral neck exploration was based on preoperative imaging indicating a solitary PA. 99mTc-Sestamibi (37–110 MBq, or 1–3 mCi) was injected in the operating theater 10–30 min before the start of the intervention. Either 11-mm collimated (309 patients) or 14-mm collimated (75 patients) γ-probes were used. Intraoperative quick parathyroid hormone (IQPTH) assay was used on 308 patients (80.2%). Results: MIRS was successfully performed on 268 (96.8%) of 277 patients. Conversion to bilateral neck exploration was necessary in 9 patients (3.3%) because of either persistently high IQPTH levels after removal of the preoperatively visualized PA (4 patients), intraoperative frozen-section diagnosis of parathyroid carcinoma (2 patients), or hard-to-remove PA (3 patients). MIRS, which was performed under locoregional anesthesia in 72 patients, required a mean operating time of 37 min and a mean hospital stay of 1.2 d. MIRS was successfully performed also on 32 (78.0%) of 41 patients who had previously undergone thyroid or parathyroid surgery. No major surgical complications were observed in the MIRS group, and there were only 24 cases (11%) of transient postoperative hypocalcemia. The probe was of little help in patients with concomitant 99mTc-sestamibi–avid thyroid nodules and not helpful at all in patients with negative scan findings preoperatively. IQPTH measurement helped to disclose some cases of multigland parathyroid disease. Conclusion: 99mTc-Sestamibi scintigraphy, especially if combined with neck ultrasonography, is highly accurate in selecting PHPT candidates for MIRS. The low-dose 99mTc-sestamibi protocol (which entails a low-to-negligible radiation exposure to the surgical team) is safe and effective for MIRS. MIRS plays a limited role in patients with concomitant 99mTc-sestamibi–avid thyroid nodules and should be discouraged in patients with negative 99mTc-sestamibi finding preoperatively. IQPTH can be recommended during MIRS to facilitate intraoperative identification of previously undiagnosed multigland parathyroid disease.
- primary hyperparathyroidism
- solitary parathyroid adenoma
- minimally invasive parathyroidectomy
- radioguided surgery
- 99mTc-sestamibi scintigraphy
- neck ultrasonography
The traditional surgical approach to patients with primary hyperparathyroidism (PHPT) is based on bilateral neck exploration, which allows intraoperative identification of at least 4 parathyroid glands, removal of the enlarged glands, and, in some protocols, biopsy of normal-sized glands to disclose possible glandular hyperplasia (1). In the hands of experienced surgeons, bilateral neck exploration has a success rate proven to be as high as 95% in curing PHPT, with low associated morbidity (2). However, during the last 2 decades, most surgeons have moved to less aggressive surgical techniques such as unilateral neck exploration (3), minimally invasive endoscopic surgery (4,5), and radioguided (6–9) surgery. This trend, which holds true especially in patients with a high preoperative probability that PHPT is sustained by a solitary parathyroid adenoma (PA), is based on the development of imaging techniques such as 99mTc-sestamibi scintigraphy and high-resolution neck ultrasonography allowing more accurate preoperative localization of parathyroid tumors (10–15).
Some additional technical improvements allow such minimally invasive parathyroidectomy approaches. One of these improvements is measurement of the parathyroid hormone serum levels with an assay performed in only 10 min (intraoperative quick parathyroid hormone [IQPTH]) and therefore applicable also in the intraoperative setting (16). Given the extremely short biologic half-life of parathyroid hormone, reduction in its serum level to less than 50% of its preoperative baseline 10 min after removal of a suspect PA is highly predictive of eucalcemia after surgery (9). Another technical improvement is small-sized endoscopes allowing good visualization of thyroid and parathyroid glands through a small skin incision (4,5). A third is hand-held γ-detection probes, which guide the surgeon to precisely identify the 99mTc-sestamibi–avid PA (6–9,17–19).
In the present multiinstitutional study, we evaluated 384 consecutive PHPT patients who underwent parathyroidectomy at 6 Italian centers. Our purpose was to define, first, the accuracy of preoperative localization imaging based on 99mTc-sestamibi scintigraphy and neck ultrasonography in selecting PHPT patients as candidates for minimally invasive radioguided surgery (MIRS) and, second, the role of intraoperative γ-probe detection used during MIRS for PHPT patients with a high probability of solitary PA.
MATERIALS AND METHODS
Between September 1999 and July 2003, 384 consecutive PHPT patients were considered for radioguided parathyroidectomy. Patients were referred to 7 centers affiliated to the Italian Study Group on Radioguided Surgery and Immunoscintigraphy (GISCRIS). All participant surgeons had previously acquired large experience with radioguided sentinel lymph node biopsy in patients with breast cancer or with melanoma and had performed at least 20 radioguided parathyroidectomies, thus guaranteeing adequate training for both components of the combined procedure, radioguidance and limited-access parathyroid surgery.
According to regulations of each participating Institutional Review Board, all patients gave their written informed consent to the procedure of radioguided surgery and to inclusion of their clinical data in the general database used for this observational study. 99mTc-Sestamibi is approved and licensed in Italy for parathyroid imaging as an adjunct to myocardial perfusion scintigraphy as well as mammoscintigraphy for breast cancer.
Biochemical diagnosis of PHPT was obtained in all 384 patients, mean serum calcium level being 10.9 mg/dL (range, 10.7–13.6 mg/dL) and mean serum parathyroid hormone level 186 pg/mL (range, 92–460 mg/dL). There were 257 women and 127 men, with a mean age of 55.2 y (range, 20–83 y). Thyroid surgery had previously been performed on 23 patients, and unsuccessful parathyroid surgery for PHPT on 18 patients.
Table 1 summarizes the preoperative localization imaging procedures used on the patient population. High-resolution neck ultrasonography was systematically performed on all patients at the same time as 99mTc-sestamibi scintigraphy.
Preoperative Imaging Modalities Used on 384 Patients with Primary Hyperparathyroidism
Criteria for selecting patients for MIRS were distinct 99mTc-sestamibi scintigraphic evidence of a solitary PA, absence of concomitant nodular goiter based on 99mTc-pertechnetate scintigraphic and ultrasound pattern, no history of familial hyperparathyroidism or multiple endocrine neoplasia, and no history of prior neck irradiation. A total of 277 (72.1%) of 384 patients met these inclusion criteria for MIRS; this group also included 32 of the 41 patients who had previously undergone thyroid or parathyroid surgery. On the other hand, 107 patients (9 of whom had previously undergone thyroid or parathyroid surgery) were not considered good candidates for MIRS because of concomitant 99mTc-sestamibi–avid thyroid nodules (64/384 patients, or 16.7%), scintigraphic or ultrasound findings suggesting multiglandular parathyroid disease (21 patients, or 5.5%), negative 99mTc-sestamibi scintigraphy findings (20 patients, or 5.2%), or preoperative diagnosis of possible parathyroid carcinoma (2 patients, or 0.5%). The intraoperative γ-probe was used also during a traditional bilateral neck exploration. Altogether, surgery was performed under locoregional anesthesia on 72 patients, 56 of whom were older than 65 y and with concomitant invalidating diseases contraindicating general anesthesia.
At each center, 2 nuclear medicine physicians skilled in parathyroid imaging interpreted scintigraphy results; in cases of discrepancy, diagnosis was reached by consensus. In patients showing a normal thyroid gland on the 99mTc-pertechnetate scan and ultrasound examination, a single focus of preferential/exclusive 99mTc-sestamibi uptake was defined as a solitary PA, whereas the presence of 2 or more 99mTc-sestamibi–avid foci indicated potential multigland parathyroid disease. In patients with concomitant nodular goiter, neck ultrasonography and 99mTc-pertechnetate thyroid scintigraphy were used to distinguish enlarged parathyroid glands from 99mTc-sestamibi–avid thyroid nodules, as previously described (20,21).
Planar scintigraphy was performed using large-field-of-view γ-cameras equipped with a parallel-hole, low-energy, high-resolution collimator or pinhole collimators (or both sequentially). Images of the head and mediastinum were recorded in a 128 × 128 or 256 × 256 matrix, to be subsequently processed by dedicated computers.
SPECT images were generally acquired using dual-head γ-cameras equipped with parallel-hole, low-energy, high-resolution collimators, adopting the following parameters: circular or elliptic orbit, 120 steps over 360°, 25–30 s per step, and a 64 × 64 matrix. Reconstruction was performed using a low-pass filter with a cutoff ranging from 0.2 to 0.25 and an order of 4.5–6.0, to obtain transaxial, coronal, and sagittal sections.
Neck ultrasonography was performed using high-resolution 7.5- to 10-MHz transducers. Longitudinal and transverse scans of the neck were obtained from the angle of the mandible to the sternal notch. Enlarged parathyroid glands were identified on gray-scale imaging as hypoechoic nodules with contours distinct from the thyroid gland.
Table 2 summarizes the sequential steps of radioguided MIRS used on our patients.
MIRS Protocol of the Present Study
Two types of hand-held commercial collimated γ-probe were used (11-mm and 14-mm diameter, used on 309 and 75 patients, respectively), minimum detectable radioactivity being 370 Bq (10 nCi) for either probe.
Intraoperative quick parathyroid hormone (IQPTH) assay was used on 308 patients (80.2%). IQPTH was measured by immunochemoluminescent assay (Liason; Byk Gulden). A reduction in IQPTH levels to less than 50% of the baseline preoperative values 10 min after removal of a PA indicated successful removal of all hyperfunctioning parathyroid tissue. When IQPTH did not decrease by more than 50%, multigland disease was suspected and surgery was extended to explore other possible sites of PA; in that case, additional blood samples for IQPTH measurement were obtained 10 min after removal of any surgical parathyroid specimen.
Postsurgical follow-up ranged from 6 to 44 mo (median, 19 mo) and included a clinical and laboratory (serum calcium and parathyroid hormone serum levels) survey 1 mo after surgery and then every 2–3 mo.
Data are expressed as mean ± SD. The Student t test was used for statistical analysis, with a P value of less than 0.05 considered significant.
RESULTS
As diagrammatically shown in Figure 1, MIRS was successfully performed on 268 (96.8%) of the 277 PHPT patients for whom this approach had been planned on the basis of preoperative scintigraphy and ultrasound findings, especially a clear, well-defined uptake in a solitary PA at 99mTc-sestamibi scintigraphy. The mean parathyroid-to-background ratio in patients of this group was 2.8 ± 0.7 (median, 3.0; range, 1.5–6.7), whereas the parathyroid-to-thyroid ratio was 1.6 ± 0.3 (median, 1.6; range, 1.1–3.2). In 199 (71.8%) of the 277 patients who underwent MIRS, concordant ultrasonography and scintigraphy findings were observed, whereas in 78 patients (28.2%) the hyperfunctioning parathyroid tissue was identified only on scintigraphy.
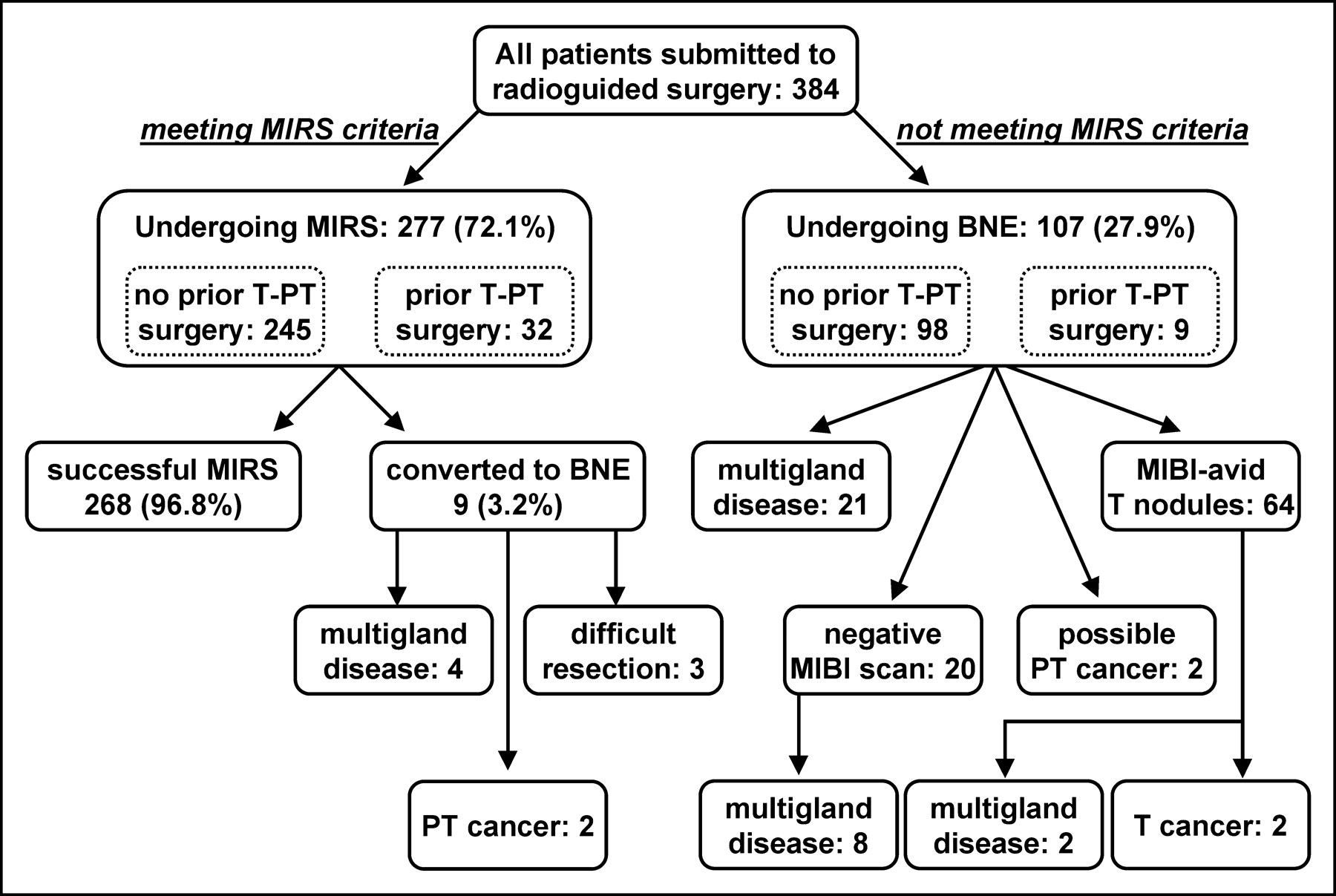
Distribution of patients according to main factors affecting choice of surgical approach. BNE = bilateral neck exploration; T = thyroid; PT = parathyroid; MIBI = 99mTc-sestamibi.
In the surgeons’ opinion, intraoperative γ-probe detection was crucial or very helpful for performing MIRS in 54 (19.5%) of the 277 newly diagnosed patients with a PA located in an ectopic site (27 in the upper mediastinum, 3 at the carotid bifurcation, and 24 deep in the neck in the pararetroesophageal or the pararetrotracheal space) and in all 32 (100%) of the patients who underwent repeated surgery (to detect an ectopic, deep PA in 5 patients and to minimize surgical trauma in 27 patients).
MIRS required a mean operating time of 37 ± 14 min (median, 35 min; range, 15–70 min) and a mean hospital stay of 1.2 ± 0.3 d (median, 1 d; range, 0.42–2 d). Locoregional anesthesia was successful in 72 patients, a result especially useful for 56 elderly patients in whom general anesthesia was contraindicated because of concomitant invalidating diseases. No major surgical complications (laryngeal nerve palsy, permanent hypoparathyroidism) occurred in the MIRS patient group, transient hypocalcemia being observed in 11% of the patients. In addition to the expected favorable cosmetic results, all patients who underwent MIRS remained eucalcemic during long-term postsurgical follow-up and were therefore considered cured.
In 9 (3.3%) of 277 patients, conversion from MIRS to bilateral neck exploration was necessary either because a parathyroid carcinoma was identified in intraoperatively obtained frozen sections (2 patients), because the PA was hard to remove (3 patients), or because IQPTH revealed persistently high hormonal levels after removal of the preoperatively visualized PA (4 patients). In the last 4 patients, the final diagnosis was double PA: In 2 of these patients the second, not preoperatively visualized, PA was identified by intraoperative γ-probe counting, whereas in the other 2 patients the counting rate in the PA was not significantly higher than in the adjacent thyroid tissue (IQPTH remaining therefore the only correct indicator of persistently abnormal parathyroid tissue). Bilateral neck exploration required significantly longer surgical times than MIRS (P < 0.001), both for the surgery per se (mean, 80 ± 26 min; median, 75 min; range, 32–145 min) and for the hospital stay (mean, 2.8 ± 1.7 d, median, 2.8 d; range, 2–4 d).
In the surgeons’ opinion, intraoperative γ-probe counting was very helpful also in the 21 patients treated with bilateral neck exploration de novo because preoperative imaging had revealed multigland disease, as it aided in identifying intraoperatively the abnormal parathyroid glands visualized preoperatively at scintigraphy. Moreover, in 1 patient a previously undetected ectopic parathyroid gland in the thymus was identified by γ-probe counting. However, in patients with multigland parathyroid disease a wide range of counting rate was recorded, with important differences between the dominant and the nondominant abnormal parathyroid glands. This difference was particularly relevant in 3 patients in whom the nondominant glands exhibited counting rates similar to those of the thyroid tissue, an observation potentially misleading the surgeon to believe that all abnormal parathyroid tissue had been removed (false-negative γ-probe results); however, IQPTH did not decrease to less than 50% of the preoperative baseline levels, thus indicating the persistence of hyperfunctioning parathyroid tissue and leading to continued surgery. In general, the ex vivo γ-probe counting rate of the dominant gland was at least 20% higher (and sometimes much higher) than thyroid background activity. Nevertheless, considering altogether the 27 patients eventually classified as being affected by multigland parathyroid disease (either correctly diagnosed preoperatively or identified intraoperatively by γ-probe counting or by IQPTH), 38% of the nondominant parathyroid glands also had an ex vivo γ-probe counting rate 20% higher than thyroid background. On the other hand, in 3 patients both intraoperative γ-probe counting and IQPTH falsely indicated completeness of parathyroidectomy, yet the patients presented with recurrent hyperparathyroidism in the postsurgical follow-up.
In the 64 patients with concomitant PHPT and nodular goiter, the combination of ultrasonography and 99mTc-pertechnetate thyroid scintigraphy with 99mTc-sestamibi scintigraphy was very useful for diagnosing and characterizing concurrent thyroid and parathyroid disease. All patients of this group underwent bilateral neck exploration, during which total or subtotal thyroidectomy was performed at the same time as parathyroidectomy. Sixty-two of these patients had a solitary PA, whereas preoperative imaging correctly identified multigland disease in 2 patients. Interestingly, occult papillary microcarcinoma (maximum diameter < 10 mm) was diagnosed by intraoperative frozen section analysis in 2 patients. In the surgeons’ opinion, intraoperative γ-probe counting was helpful only in 1 patient with an ectopic PA at the carotid bifurcation and in 6 patients with a PA deep in the neck, distant from the thyroid gland. However, in most patients the surgeon found it difficult to distinguish by intraoperative γ-probe counting the radioactivity of the PA from that of the adjacent 99mTc-sestamibi–avid thyroid nodules.
Interestingly, a relatively high fraction of multigland disease (40%) was found at surgery in the 20 patients with negative preoperative imaging results (6 of whom had concomitant multinodular goiter): 6 cases of hyperplasia and 2 cases of double PA. In the surgeons’ opinion, intraoperative γ-probe counting was not helpful in these 20 patients.
No cases of laryngeal nerve palsy were observed in the patients who underwent bilateral neck exploration, whereas permanent hypoparathyroidism was observed in 4 patients on whom total parathyroidectomy had to be performed because of glandular hyperplasia, and transient hypocalcemia was observed in 33 of 107 patients (30.8%). Finally, 3 patients presented with recurrent hyperparathyroidism during follow-up, in all of whom hyperplasia had initially been diagnosed.
The weight of the removed solitary PA was similar in the patients who underwent MIRS and the patients who underwent bilateral neck exploration (mean, 1,050 ± 324 mg vs. 980 ± 293 mg, P = not statistically significant), whereas the parathyroid glands removed from patients with multigland disease were significantly smaller (558 ± 320 mg, P < 0.05 vs. all solitary PAs).
DISCUSSION
Although bilateral neck exploration is still accepted as the gold standard for treatment of PHPT, many surgeons consider this procedure an overtreatment, because in most cases (80%–85% or more) PHPT is due to a solitary PA (22). Therefore, the surgical approach is gradually shifting from bilateral neck exploration to unilateral neck exploration (3) and, further, to minimally invasive endoscopic or to radioguided parathyroidectomy (4–9,17–25). Preoperative localization imaging is mandatory when a minimally invasive approach is contemplated, assuming that hyperparathyroidism is caused by a solitary PA. Invasive localizing techniques such as arteriography and venous blood sampling are now rarely if ever used, whereas the diagnostic relevance of CT and MRI is controversial (22), except perhaps in difficult cases (ectopic or deeply located PAs) and in the reoperative neck. At present, the most widely used preoperative localizing imaging modality is 99mTc-sestamibi scintigraphy, preferably with the dual-tracer subtraction approach or the single-tracer dual-phase SPECT technique (10–15,26,27). Performing thyroid scintigraphy (with either 99mTc-pertechnetate or 123I) along with neck ultrasonography is especially recommended in geographic areas with a high prevalence of nodular goiter, as this combination constitutes the best localizing imaging protocol (20,28). As also observed in the present study, coexisting 99mTc-sestamibi–avid thyroid nodules can trap and retain 99mTc-sestamibi in a manner similar to that of a PA, thus potentially causing false-positive results at MIRS (20,28,29).
After exclusion of patients with multigland disease, nodular goiter, suspicion of malignancy, or negative 99mTc-sestamibi findings, candidates for MIRS represent approximately 70% of all PHPT patients referred to our centers, a fraction that agrees with prior literature (4–9,17–25). MIRS was successfully performed on 96.8% of such patients, whereas it was necessary to convert surgery to traditional bilateral neck exploration in only 3.3% of the patients, all of whom were promptly identified during the surgical procedure, based especially on IQPTH assay to detect previously unknown multigland disease.
No major surgical complications occurred in the patients who underwent MIRS, resulting in a much shorter operating time and hospital stay than is possible with traditional bilateral neck exploration. In addition, some of the MIRS procedures were performed under locoregional anesthesia, followed by same-day discharge from the hospital.
Despite a relatively low sensitivity (especially for ectopic or deep PAs), ultrasonography yielded some important additional information. Concordance of ultrasound and scintigraphic findings indicating an orthotopic PA gave the surgeon greater confidence during MIRS, especially during the learning phase of the procedure. Combined with 99mTc-pertechenate thyroid scintigraphy, ultrasonography was crucial for identifying PHPT patients with concomitant nodular goiter (a major exclusion criterion for MIRS). For upper PAs prolapsed behind the thyroid contour, ultrasonography helped to distinguish a retrothyroidal PA from a 99mTc-sestamibi–avid thyroid nodule. Discordant imaging results (positive planar scintigraphy with negative ultrasonography) indicated that, to better define the depth of the PA, it was preferable to also perform SPECT; this situation occurred in 107 patients, in 32 of whom SPECT correctly localized a deep PA. Moreover, in the patients excluded from MIRS, ultrasonography identified 7 99mTc-sestamibi–negative PAs, 4 of which had a predominant cystic component and 3 of which were in an orthotopic site but masked by a concomitant large multinodular goiter.
On the other hand, application of the γ-probe during MIRS was judged to be particularly useful by our surgeons because it allowed, first, rapid detection of the PAs intraoperatively, particularly those in ectopic sites or deep in the neck; second, evaluation of the completeness of PA removal by repeated radioactivity measurement of the surgical bed; and, third, evaluation of the completeness of surgery by checking of radioactivity in the ex vivo removed PA. Moreover, MIRS was successfully performed on 78% of the patients in our series who had undergone previous thyroid or parathyroid surgery, thus limiting the surgical trauma and possible related complications. In this regard, the reoperative neck has recently been defined by the American Association of Endocrine Surgeons as an absolute contraindication to minimally invasive endoscopic or video-assisted parathyroidectomy but not to MIRS (30).
The main benefits of MIRS over bilateral neck exploration can be summarized as follows: shorter operating and recovery times, with the possibility of same-day discharge; potential use of locoregional anesthesia, especially in elderly patients with concomitant invalidating diseases, in whom general anesthesia might be contraindicated; reduced postsurgical pain; a lower incidence of transient hypocalcemia; potential use of a limited skin incision in the reoperative neck; and favorable cosmetic results.
Two main protocols have been described for MIRS: the protocol in which 99mTc-sestamibi scintigraphy and MIRS are performed on the same day, as first proposed by Norman and Cheda (6), and the protocol in which preoperative imaging (99mTc-sestamibi scintigraphy and ultrasonography) is completed days before surgery, as first proposed by Casara et al. (7). Although attractive from a cost-analysis point of view, the same-day protocol has some disadvantages, mainly because the type and extension of surgery (MIRS vs. bilateral neck exploration) has to be planned on the basis of the preoperative localizing imaging. This problem is more relevant in geographic areas with a high prevalence of nodular goiter; a situation in which the different-day protocol like that used in our study appears preferable. Furthermore, in the different-day protocol the patient is reinjected with a low 99mTc-sestamibi dose (37–110 MBq, or 1–3 mCi) 10–30 min before surgery begins, thus minimizing the radiation exposure to the surgical team.
When applying the same-day protocol to a large group of PHPT patients (n = 345), Murphy and Norman found that every surgical specimen that had activity measuring more than 20% of background activity was a solitary PA (31). By applying the so-called 20% rule derived from such an observation, accuracy in distinguishing PAs from multigland disease was reported to be 100%, thus questioning the necessity of measuring IQPTH during MIRS. Unfortunately, other groups adopting a similar MIRS protocol did not confirm these exciting results (24,25). In our series the ex vivo radioactivity counting was higher than 20% of thyroid background not only in all PAs but also in 38% of the nondominant parathyroid tissue removed from patients with multigland disease.
This discrepancy might be explained by the difference in elapsed time between 99mTc-sestamibi injection and surgery, 3 h in the high-dose protocol of Murphy and Norman (31) versus only 10–30 min in our low-dose protocol. In this regard, the maximum 99mTc-sestamibi uptake both in the PA and in the thyroid gland occurs within a few minutes after injection, after which there is a differential washout from the parathyroid and thyroid tissues (13). These differential 99mTc-sestamibi kinetics can therefore influence the efficacy of the 20% rule, which might not be systematically reliable in low-dose 99mTc-sestamibi protocols such as that adopted in the present study.
From a cost-analysis point of view, 2 points should be emphasized: First, in all our centers the γ-probes were already available because of earlier experience with radioguided sentinel node biopsy in patients with breast cancer or melanoma. Second, because 99mTc-sestamibi is generally used daily in our nuclear medicine centers to perform other examinations (myocardial perfusion scintigraphy and mammoscintigraphy), the additional cost of using a low dose (37–110 MBq, or 1–3 mCi) for MIRS can be considered negligible.
CONCLUSION
Combined imaging with 99mTc-sestamibi scintigraphy (especially the 2-tracer technique or the dual-phase SPECT technique) and ultrasonography is accurate for selecting patients as candidates for MIRS. A different-day protocol (prior full-dose imaging and deferred low-dose surgery) appears preferable in geographic areas with a high prevalence of concomitant nodular goiter and allows better scheduling of daily activity in the operating theater. Administration of a low 99mTc-sestamibi dose 10–30 min before the beginning of the intervention appears adequate for performing MIRS. Such low-dose protocols result in a low-to-negligible radiation exposure to the surgical team.
Acknowledgments
The authors thank all those colleagues who enrolled patients in this study, particularly Drs. Paola Erba, Mariano Grosso, Elena Lazzeri, and Duccio Volterrani (Regional Center of Nuclear Medicine, University of Pisa Medical School, Pisa, Italy); Drs. Marco Puccini and Pietro Iacconi (Institute of General and Endocrine Surgery, University of Pisa Medical School, Pisa, Italy); Dr. Francesco Medi (Division of General Surgery, Town Hospital, Viareggio, Italy); Dr. Andrea Manetti (II Institute of General Surgery, University of Florence Medical School, Florence, Italy); Dr. Dario Casara (Nuclear Medicine Service, University Hospital of Padua, Padua, Italy); Dr. Giancarlo Torre (Institute of General and Endocrine Surgery, “S. Martino” University Hospital, Genoa, Italy); and Dr. Valentino Arcuri (Institute of General Surgery and Organ Transplantation, “S. Martino” University Hospital, Genoa, Italy).
Footnotes
Received Apr. 6, 2004; revision accepted Aug. 30, 2004.
For correspondence contact: Giuliano Mariani, MD, Regional Center of Nuclear Medicine, University of Pisa Medical School, Via Roma 67, I-56126 Pisa, Italy.
E-mail: g.mariani{at}med.unipi.it





{kind=link}