


Abstract
The pathogenesis of selective neuronal damage in internal carotid artery (ICA) occlusive disease is unclear. Imaging of the central-type benzodiazepine receptor (BZR), which is expressed by most cortical neurons, provides information on the neuronal alterations induced by ischemia in vivo. Hemodynamic ischemia due to ICA occlusive disease may cause not only borderzone infarction but also selective neuronal damage beyond the regions of infarcts, which may be detected by a decrease in BZR in the normal-appearing cerebral cortex. The purpose of this study was to determine whether selective neuronal damage is associated with borderzone infarction in ICA occlusive disease. Methods: We measured BZR using PET and 11C-flumazenil in 62 nondisabled patients with ICA steno-occlusive lesions in the chronic stage. Flumazenil binding potential (BP) was calculated using the dynamic data and the reference tissue model. The infarcts on MRI—which were categorized as territorial, borderzone (external or internal), striatocapsular, lacunar, and other white matter infarcts—were correlated with the mean cerebral/cerebellar cortical BP ratio in the hemisphere with ICA occlusive disease. Results: Patients with borderzone infarction (n = 18) had a significantly decreased flumazenil BP ratio in the hemisphere with ICA occlusive disease compared with patients without borderzone infarction (n = 44) and healthy control subjects (n = 10). Multivariate analysis showed that external borderzone infarction was an independent predictor of the decreased flumazenil BP ratio. Conclusion: In ICA occlusive disease, selective neuronal damage demonstrated as decreased BZR is associated with borderzone infarction, suggesting that hemodynamic ischemia leading to borderzone infarction may cause selective neuronal damage beyond the regions of infarcts in the chronic stage.
Hemodynamic cerebral ischemia due to large arterial occlusive disease may cause not only cerebral infarction but also minor tissue damage in the cerebral cortex that is not detectable as infarction on CT or MRI (1). Studies in animals have shown that selective cortical neuronal necrosis is caused by permanent arterial occlusion accompanied by ischemia of moderate severity (1). Recognizing selective neuronal damage is important in the context of therapy with vascular reconstruction surgery and neuroprotective agents for hemodynamic cerebral ischemia due to large arterial occlusive disease. However, little is known about selective neuronal damage due to cerebral ischemia in humans (1,2).
Imaging of the central-type benzodiazepine receptor (BZR), which is expressed by most cortical neurons, provides information on the neuronal alterations induced by ischemia in vivo (3–6). A few studies have demonstrated reduction in BZR in the normal-appearing cortical areas on CT or MRI in patients with atherothrombotic large artery disease in the chronic stage (7–11), suggesting the presence of selective neuronal damage. However, those studies included only a small number of patients with heterogeneous arterial diseases. Thus, the pathogenesis of selective neuronal damage demonstrated as decreased BZR in patients with atherothrombotic large arterial occlusive disease remains unclear.
Unilateral borderzone infarction has been shown to be associated with internal carotid artery (ICA) occlusive disease and hemodynamic impairment (12,13). Hemodynamic ischemia due to ICA occlusive disease may cause not only borderzone infarction but also selective neuronal damage beyond the regions of infarcts, which may be detected by a decrease in BZR in the normal-appearing cerebral cortex. The purpose of this study was to determine whether selective neuronal damage demonstrated as decreased BZR is associated with borderzone infarction in patients with ICA occlusive disease in the chronic stage.
MATERIALS AND METHODS
Patients
Between December 2002 and February 2005, 66 consecutive patients with atherothrombotic occlusion or stenosis of the ICA were referred to our PET unit for the first time for evaluation of the hemodynamic effect of ICA occlusive disease as a part of comprehensive clinical evaluations to decide whether vascular reconstruction surgery was indicated. Inclusion criteria for the 15O-gas PET study were as follows: (a) occlusion or stenosis (>60% diameter reduction according to the North Amercian Symptomatic Carotid Endarterectomy Trial criteria (14)) of the extracranial ICA documented by conventional or MR angiography; and (b) independence in their daily life (modified Rankin scale, <3). We planned to measure BZR in all of these patients, but 1 patient could not undergo the measurement because of a problem with the synthesis of 11C-flumazenil (11C-FMZ). From the 65 patients who underwent measurements of BZR, we selected 62 patients for the present study (50 men; 65 ± 7 y old [mean ± SD]) (Table 1). The criteria for selection were asymptomatic or history of ischemic attacks in appropriate ICA distribution between 30 and 90 d before PET examinations. The patients >90 d after stroke were excluded to minimize the effect of long-term, secondary neuronal degeneration from stroke. They had no history of previous vascular reconstruction surgery or taking BZR agonists. None had clinical symptoms of ischemia in the vertebrobasilar artery territory or infarcts in the cerebellum or brainstem on MRI. All ICA lesions with stenosis (>60%) were confirmed by conventional angiography. For BZR imaging, we studied 10 healthy control subjects (7 men; 57 ± 7 y old [mean ± SD]), who had no previous history of medical or psychiatric disorder and no history of taking BZR agonists. The protocol of the 11C-FMZ PET study was approved by the Ethics Committee of our center, and written informed consent was obtained from each subject, both patients and control subjects.
Characteristics of Patients
PET Measurements
All subjects underwent PET scans with a whole-body, Advance (GE Healthcare) scanner, which permits simultaneous acquisition of 35 image slices with interslice spacing of 4.25 mm (15). Intrinsic resolution of the scanner was 4.6–5.7 mm in the transaxial direction and 4.0–5.3 mm in the axial direction. Before tracer administration, 68Ge/68Ga transmission scanning was performed for attenuation correction.
First, a series of 15O-gas studies was performed. C15O2 and 15O2 were inhaled continuously through a mask (15). The scan time was 5 min. Bolus inhalation of C15O with 3-min scanning was used to measure cerebral blood volume (CBV). Arterial samples were obtained during the scanning, and the radioactivity of the radiotracer, oxygen content, and hematocrit were measured.
After the 15O-gas study, a 11C-FMZ study was performed (16). 11C-FMZ was synthesized by the 11C-methylation of demethylated-FMZ (Hoffmann-La Roche). Specific activities at the time of injection ranged from 16.2 to 20.2 GBq/μmol (mean, 17.8 GBq/μmol). After slow intravenous injection of 370–555 MBq of 11C-FMZ into the right antecubital vein using an automatic injector over 60 s, a 50-min dynamic PET scan was started at the time of tracer administration with frame durations of 10 s × 6, 15 s × 8, 30 s × 4, 60 s × 5, 5 min × 4, and 10 min × 2.
In the 15O-gas study, we calculated cerebral blood flow (CBF), cerebral metabolic rate of oxygen (CMRo2), and oxygen extraction fraction (OEF) based on the steady-state method (17). CMRo2 and OEF were corrected by the CBV (18). In the 11C-FMZ study, binding potential (BP) was calculated using the dynamic data and the reference tissue model, in which the pons was used as the reference (16). According to the atlas by Kretschmann and Weinrich (19), we selected 2 tomographic planes corresponding to the pons on the average tissue activity image obtained from the early phase of dynamic PET data with time frames of 1–3 min. We manually placed an irregular region of interest (ROI), which included almost all of the pixels that had activity in the range from the maximum pixel value to 50% of the maximum value. These ROIs were transferred to the dynamic PET data for the calculation of BP.
MRI
MRI was performed with a Signa unit (GE Healthcare) operating at a field strength of 1.5 T. The imaging protocol consisted of a T2-weighted spin echo (repetition time/echo time [TR/TE] = 3,000/88.8), T1-weighted spin echo (TR/TE = 550/11.2), and fluid-attenuated inversion recovery (FLAIR) (TR/TE = 8,002/158; inversion time 2,000 ms) imaging series.
Cerebral ischemic lesions were identified as hyperintense lesions on T2-weighted MRI. They were classified as external borderzone infarcts (cortico–subcortical lesions in the anterior border zone between the territory of the anterior cerebral artery [ACA] and the middle cerebral artery [MCA] or in the posterior border zone between the supply territory of the MCA and the posterior cerebral artery) (12); cortical territorial infarcts (cortical lesions not assigned as external borderzone infarcts); internal borderzone infarcts (multiple or confluent white matter lesions located between the deep and superficial arterial system of the MCA in the corona radiata or between the superficial arterial system of the MCA and the ACA in the centrum semiovale) (20); lacunar infarcts (single, well-demarked lesions with a diameter of <20 mm, in the basal ganglia, thalamus, internal capsule, corona radiata, or centrum semiovale); other white matter lesions (subcortical white matter lesions not assigned as internal borderzone infarcts or lacunar infarcts); striatocapsular infarcts (large subcortical lesions with a diameter of >20 mm, in the territory of the lenticulostriate arteries) (21). All ischemic lesions were simply listed as present or absent. FLAIR images were used to distinguish infarcts from dilated perivascular spaces. All scans were reviewed by 1 investigator who was unaware of the clinical status of the patients, including other imaging data.
Data Analysis
We analyzed 10 tomographic planes from 46.25 to 84.5 mm above and parallel to the orbitomeatal line, which corresponded to the levels from the basal ganglia and thalamus to the centrum semiovale. The hemisphere supplied by the symptomatic ICA in symptomatic patients or the hemisphere supplied by the more severely diseased ICA in asymptomatic patients is referred to hereafter as the “ipsilateral” hemisphere. The ROI was placed on the CBF images. Each image was examined by placing a total of 10–12 circular ROIs, 16 mm in diameter, compactly over the gray matter of the outer cortex in each hemisphere. According to the atlas by Kretschmann and Weinrich (19), the ROIs in all 10 images covered the distribution of the MCA as well as the borderzone areas between the ACA and MCA and between the MCA and posterior cerebral artery (22). The same ROIs were transferred to the other images. The mean hemispheric values in the ipsilateral hemisphere were calculated as the average of the values of all circular ROIs. In 23 patients with infarction in the cerebral cortex, the circular ROIs corresponding to the infarcted area were excluded from analysis. A previously described method was used to correlate PET images with MR images (23). The ROIs that included low-intensity areas on T1-weighted MR images were excluded.
On the FMZ-BP image, 3 circular ROIs, 16 mm in diameter, were also drawn on the cerebellar cortices (24). To negate the effect of fluctuations in whole-brain values and to extract the change attributed to ICA disease, we analyzed the regional relative distribution of central BZR: the relative FMZ-BP (mean cerebral/cerebellar cortical FMZ-BP ratio in the ipsilateral hemisphere). The value of FMZ-BP in the ipsilateral cerebellar hemisphere was used because the effect of cerebellar deafferentation on BZR was unclear. In the control subjects, the relative FMZ-BP was calculated as the ratio of the mean of the bilateral cerebral FMZ-BP to the mean of the bilateral cerebellar FMZ-BP.
Statistical Analysis
The values of FMZ-BP ratio obtained in patients with borderzone infarction were compared with those obtained in patients without such infarction and those in healthy control subjects using 1-way ANOVA and post hoc Scheffe analysis; significance was established at P < 0.05. We compared the values of FMZ-BP ratio between patients with and without 6 types of ischemic lesions using the Student t test; statistical significance was accepted at P < 0.008 (0.05/6) by using a Bonferroni correction. Stepwise multiple linear regression analysis was used to test the independent predictive value of the ischemic lesions with respect to the values of FMZ-BP ratio; significance was established at P < 0.05.
RESULTS
Forty-eight patients had infarcts in the hemisphere with ICA disease. Eighteen patients had borderzone infarction: 5 with solitary external borderzone infarcts, 6 with solitary internal borderzone infarcts, and 7 with both. All borderzone infarcts were symptomatic. Twelve were found in patients with ICA occlusion and 6 were found in patients with ICA stenosis. Patients with borderzone infarction had a significantly decreased FMZ-BP ratio (1.10 ± 0.13) in the hemisphere with ICA disease (Figs. 1, 2, and 3), compared with patients without borderzone infarction (1.32 ± 0.17, n = 44; P < 0.0001) and control subjects (1.37 ± 0.12, n = 10; P = 0.0003).
Because some patients had 2 or more categories of ischemic lesions, we analyzed the relationship between the simple presence of ischemic lesions and the FMZ-BP ratio (Table 2). Patients with external or internal borderzone infarction had a significantly decreased FMZ-BP ratio, compared with patients without. However, the value of the FMZ-BP ratio was not significantly different between patients with and without any other type of ischemic lesions. The results were same when the value of the FMZ-BP ratio was compared between patients with 6 types of ischemic lesions and control subjects. When the patient age and the presence of 6 types of ischemic lesions were entered into a stepwise multiple linear regression analysis, it produced a model including only the presence of external borderzone infarction with a correlation coefficient of 0.59 for the FMZ-BP ratio (P < 0.0001). The other variables did not significantly contribute to the magnitude of the correlation. After controlling for the effects of age and the presence of the other 5 types of ischemic lesions, the presence of external borderzone infarction was also a significant independent predictor of the FMZ-BP ratio (Table 3).
Ischemic Lesions and Cerebral/Cerebellar FMZ BP Ratio in Hemisphere with Carotid Artery Disease
Multiple Linear Regression Analysis with Cerebral/Cerebellar FMZ BP Ratio in Hemisphere with Carotid Artery Disease as Dependent Variable
In the 62 hemispheres with ICA disease, the FMZ-BP ratio was significantly correlated with CBF (r = 0.54, P < 0.0001) (Fig. 3A) and CMRo2 (r = 0.61, P < 0.0001) (Fig. 3B). The FMZ-BP ratio also had a significant negative correlation with OEF (r = −0.25, P = 0.047) (Fig. 3C).

Examples of PET images on 2 different levels show parallel decrease of FMZ-BP, CBF, CMRo2, and an increase of OEF in patient with right ICA occlusion who showed internal borderzone infarction (red arrow) with cortical extension (green arrow) on corresponding MR images. In addition to markedly reduced FMZ-BP in region with small cortical infarcts, a decrease of FMZ-BP was found in normal-appearing cerebral cortex beyond borderzone infarcts. Mean hemispheric values of ipsilateral/contralateral hemisphere: FMZ-BP ratio, 1.00/1.16; CBF, 20.4/26.1 mL/100 g/min; CMRo2, 2.37/2.87 mL/100 g/min; OEF, 61.9%/58.3%.

Examples of PET images show distribution of decrease of FMZ-BP in patient with right ICA occlusion (patient in Fig. 1). Although decreases of FMZ-BP predominated in frontoparietal region near borderzone infarction, an extensive decrease of FMZ-BP was found in MCA distribution.
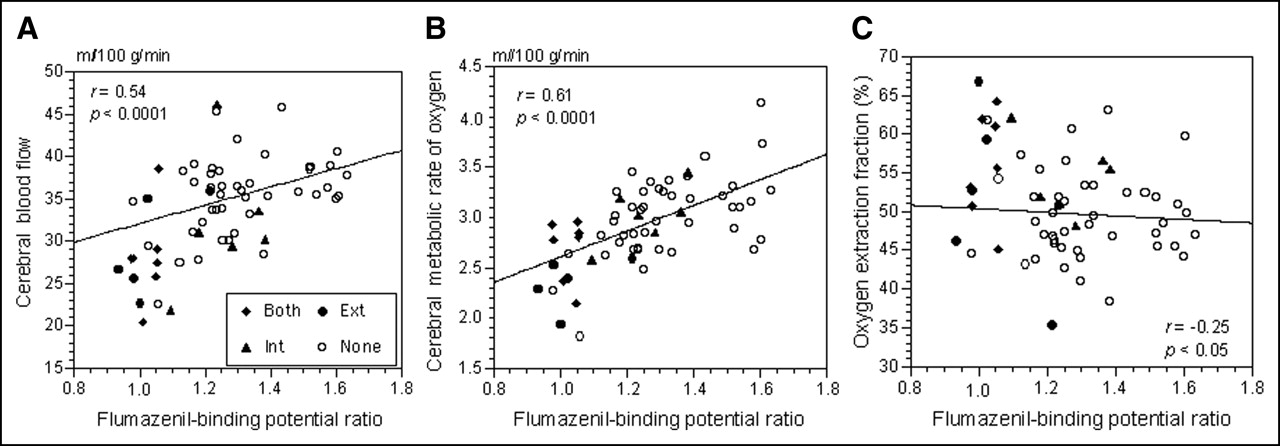
Scatter diagrams plot CBF (A), CMRo2 (B), and OEF (C) against cerebral/cerebellar FMZ-BP ratio in 62 hemispheres with carotid artery disease. The lines were generated by simple linear regression. Ext = solitary external borderzone infarct; Int = solitary internal borderzone infarct; Both = both borderzone infarct; None = no borderzone infarct.
DISCUSSION
This study showed that in atherothrombotic ICA occlusive disease in the chronic stage selective neuronal damage demonstrated as decreased cortical BZR is associated with borderzone infarction. This evidence supports hemodynamic cerebral ischemia as a cause of selective neuronal damage in patients with ICA occlusive disease.
The pathogenesis of selective neuronal damage in patients with atherothrombotic ICA occlusive disease remains unclear. Although the main cause may be hemodynamic cerebral ischemia of moderate severity due to ICA occlusive disease, a direct correlation between the severity of ischemia at the time of symptoms and selective neuronal damage in the chronic stage has not been demonstrated. This study suggests that in ICA occlusive disease, hemodynamic ischemia leading to cortico–subcortical borderzone infarction in the most distal field may cause extensive neuronal damage in the cerebral cortex beyond the region of infarcts in the chronic stage. At the time of the development of borderzone infarction of hemodynamic origin, perfusion pressure in the MCA distribution must be markedly decreased (13). Although ischemia reaches the threshold of infarction in the cortico–subcortical borderzone region, in the cerebral cortex beyond borderzone infarcts there may be ischemia of moderate severity that reaches only the threshold of selective neuronal damage. Then, in the chronic stage, cortico–subcortical borderzone infarction of hemodynamic origin would accompany extensive cortical neuronal damage beyond infarcts, which is detected as a diffuse decrease of BZR in the hemisphere with infarcts, as shown in the present study (Fig. 2). It is less likely that borderzone infarction due to embolism causes extensive decreases of BZR beyond the regions of the infarct, because ischemia is restricted to the cortical borderzone region, although we cannot completely exclude the possibility that concomitant showers of microembolism may cause ischemic damage of the cerebral cortex in a multiple-spot fashion, leading to extensive decreases of BZR without apparent infarction. Another possibility not involving a hemodynamic mechanism is that functional downregulation of the BZR in the perilesional tissue may be caused by focal cortical lesions (25). In the present study, this mechanism was not supported by the finding that cortical infarctions located outside the possible arterial borderzone regions were not associated with a decrease in BZR beyond infarcts. Therefore, we believe that selective neuronal damage demonstrated as decreased BZR beyond cortico–subcortical borderzone infarction resulted from a direct effect of hemodynamic ischemia attributed to ICA occlusive disease.
In ICA occlusive disease, long-lasting ischemia of mild severity may also cause selective neuronal damage. Reduced oxygen metabolism without morphologic changes on CT has been demonstrated in the hemisphere perfused by the diseased ICA, and no change in metabolism after surgical reperfusion suggests selective neuronal damage (26). Some patients with ICA occlusion are reported to show decreased BZR without MRI evidence of infarction (9,11), and some patients without borderzone infarction in the present study showed a low value of the FMZ-BP ratio. In our patients, those with decreased BZR had a tendency to show chronic hemodynamic impairment (increased OEF), which suggests that chronic hemodynamic impairment may be another important factor for the development of selective neuronal damage, in addition to acute hemodynamic ischemia leading to borderzone infarction. However, decreased BZR was more closely associated with decreased oxygen metabolism. Selective neuronal damage caused by hemodynamic ischemia in turn decreases the degree of hemodynamic impairment attributed to ICA occlusive disease through reduced metabolic demand of the tissue (11,27). Therefore, it is not easy to demonstrate an association of decreased BZR with chronic hemodynamic impairment. Long-term follow-up studies of ICA occlusion showed that progression of brain atrophy with deterioration in cerebral metabolism occurs after ICA occlusion in association with a deterioration of cerebral hemodynamics (28,29). A follow-up study should be done to determine whether long-lasting ischemia of mild severity causes selective neuronal damage demonstrated as decreased BZR in ICA occlusive disease (1).
In the clinical setting, the association between selective neuronal damage and borderzone infarction may decrease the value of borderzone infarction as a marker of chronic hemodynamic impairment that is associated with the risk of a future stroke (30–32). In ICA occlusive disease, an association between cortical borderzone infarction and chronic hemodynamic impairment has not been consistently reported (13,33,34). In the present study, the association of decreases of BZR with cortical borderzone infarctions suggests that severe hemodynamic impairment, which was present in the acute stage of infarction, may have disappeared in accordance with the decrease of the metabolic needs of the tissue between the time of infarction and the PET examination. In contrast, several studies have shown that solitary internal borderzone infarction is associated with chronic hemodynamic impairment in ICA occlusive disease (13,33–35). As shown in this study, internal borderzone infarction was not independently associated with a decreased BZR in the overlying cerebral cortex, probably because the severity of hemodynamic ischemia—which caused only minor white matter damage in the most distal region—did not reach the threshold of selective neuronal damage in the cerebral cortex, including the borderzone regions. Then, the preserved metabolic needs of the cortical tissue in the chronic stage may permit the persistence of the hemodynamic impairment that caused internal borderzone infarction. In ICA occlusive disease in the chronic stage, the association between borderzone infarction and hemodynamic impairment is confounded by the concomitant development of selective neuronal damage.
This study has some methodologic limitations. We did not perform correction for partial-volume effects. The decrease in cortical FMZ-BP ratio may also have resulted from cortical atrophy through the partial-volume effect, particularly in the ROIs surrounding irregular cortical infarcts. Therefore, some of the decreases in the FMZ-BP ratio, particularly in patients with cortical infarcts, may reflect cortical atrophy. Cortical atrophy may also contribute partially to the correlation between decreased BZR with decreased oxygen metabolism. However, we believe atrophy does not explain the association of external borderzone infarction with decreased FMZ-BP ratio, because cortical infarctions located outside the possible arterial borderzone regions were not associated with a decrease in BZR beyond infarcts. Our previous study showed that cortical BZR was not correlated with the degree of cortical atrophy in patients with large cerebral arterial occlusive disease (10). However, to confirm our results, corrections of PET data for atrophy based on coregistration of MR and PET scans may be needed.
The histopathologic correlates of the present findings could not be examined in any of our patients. Therefore, it is unclear whether selective neuronal damage demonstrated as decreased BZR indicates loss of neurons, loss of receptors on dendrites or cell body, or downregulation of receptors. Selective cortical neuronal loss has not been reported in patients with ICA disease and borderzone infarcts, although it has been shown in 2 patients with embolic occlusion of the MCA (2). Only a few experimental studies of stroke have shown a correlation between a decrease in BZR binding in vivo and neuronal necrosis on histopathologic examinations (36). Studies in baboons and rats with MCA occlusion showed no necrotic neurons in the cortical regions where BZR binding was reduced (37,38). Decreased BZR without neuronal loss may reflect selective dendritic lesions, which are reported to occur at an early stage of ischemic neuronal damage (39). Furthermore, although our results suggest that the decreased BZR may be primarily of ischemic origin, we could not exclude the possible effect of deafferentaion from subcortical infarcts (receptor downregulation or axon terminal degeneration) in some patients (40). In any case, the association of decreased BZR with decreased oxygen metabolism in our patients indicates that the decreased BZR is accompanied by a process involving a decrease of cerebral cortical metabolism.
CONCLUSION
In ICA occlusive disease, borderzone infarction is associated with extensive decreases of BZR beyond the regions of infarcts, which suggests that hemodynamic cerebral ischemia may cause selective neuronal damage in the chronic stage. Recognizing selective neuronal damage is important for understanding the pathophysiology of hemodynamic cerebral ischemia in patients with ICA occlusive disease.
Acknowledgments
This study was supported in part by a Grant-in-Aid for Scientic Research from the Japan Society for the Promotion of Science (17590910). We thank Hidehiko Okazawa, MD, PhD (Biomedical Imaging Research Center, Fukui University), and the staff of the PET unit, Research Institute, Shiga Medical Center, for their support and technical help. We also thank the staff of the Department of Neurology and the Department of Neurosurgery, Shiga Medical Center, for clinical assistance.
Footnotes
Received Jul. 13, 2005; revision accepted Aug. 29, 2005.
For correspondence or reprints contact: Hiroshi Yamauchi, MD, PhD, Research Institute, Shiga Medical Center, 5-4-30 Moriyama, Shiga 524-8524, Japan.
E-mail: yamauchi{at}shigamed.jp
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Selective neuronal damage and blood pressure in atherosclerotic major cerebral artery disease
- Progressive Cortical Neuronal Damage and Chronic Hemodynamic Impairment in Atherosclerotic Major Cerebral Artery Disease
- History of the Letzte Wiese/Last Meadow Concept of Brain Ischemia
- Central Benzodiazepine Receptor Binding Potential and CBF Images on SPECT Correlate with Oxygen Extraction Fraction Images on PET in the Cerebral Cortex with Unilateral Major Cerebral Artery Occlusive Disease
- Selective neuronal damage and Wisconsin Card Sorting Test performance in atherosclerotic occlusive disease of the major cerebral artery
- Steal physiology is spatially associated with cortical thinning
- Decreased Chronic-Stage Cortical 11C-Flumazenil Binding After Focal Ischemia-Reperfusion in Baboons: A Marker of Selective Neuronal Loss?
- Advances in Imaging 2006