


Abstract
Stress myocardial perfusion imaging is a useful method for evaluation of coronary artery disease (CAD) in patients with diabetes mellitus. However, its role in predicting all-cause mortality is not well defined. The aim of this study was to determine whether myocardial ischemia on stress myocardial perfusion imaging can predict all causes of death in patients with diabetes mellitus.
Methods: We studied 297 patients with diabetes mellitus and known or suspected CAD by exercise or dobutamine stress 99mTc-tetrofosmin myocardial perfusion tomographic imaging. Ischemia was defined as reversible perfusion abnormalities. The endpoints were death from any cause and hard cardiac events (cardiac death and nonfatal myocardial infarction).
Results: An abnormal scan was detected in 179 (60%) patients. Myocardial perfusion abnormalities were fixed in 76 (26%) patients and were reversible in 103 (35%) patients. During a mean follow-up of 6 ± 2.1 y, 80 (27%) patients died. Nonfatal myocardial infarction occurred in 14 (5%) patients. The annual mortality rate was 2.5% in patients with normal perfusion, 4.5% in patients with fixed defects, and 6% in patients with ischemia. The annual cardiac death rate was 4.2% in patients with ischemia and 2.6% in patients with fixed defects. In patients with normal perfusion, the annual cardiac death rate was 0.9% during the 5 y after the stress test. In a Cox multivariate analysis model, predictors of death were age, history of heart failure, peripheral vascular disease, and reversible perfusion defects.
Conclusion: Myocardial ischemia on stress 99mTc-tetrofosmin myocardial perfusion imaging is associated with an increased risk of all-cause mortality during long-term follow-up among patients with diabetes mellitus. Patients with normal perfusion have a lower mortality rate and may require less frequent follow-up stress perfusion imaging.
Various studies have demonstrated the association of diabetes mellitus with increased risk of overall and cardiac mortality (1–11). The reported annual mortality rate in epidemiologic studies ranged between 4.8% and 9% in diabetic patients who were 44–75 y old (5–7). Coronary artery disease (CAD) is a leading cause of morbidity and mortality in diabetic patients (9–11). Identification of high-risk patients is important for planning the proper management strategy.
Recent studies have demonstrated the value of noninvasive imaging modalities such as stress echocardiography (12–14) and myocardial perfusion scintigraphy (15–22) in the prediction of cardiac death and composite cardiac endpoints in diabetic patients. In recent years, there has been an increasing interest in studying all causes of mortality as a single endpoint, against which the value of diagnostic and therapeutic interventions in CAD is assessed. The use of all causes of mortality as an endpoint has the advantage of avoiding inaccuracies and bias related to determination of cause of death (23). Additionally, the finding of an association of the results of stress imaging with all causes of mortality would suggest that interventions based on these results may improve survival in the studied population.
To our knowledge, there are currently no data that suggest a role of myocardial ischemia on stress myocardial perfusion imaging in the prediction of all causes of mortality in diabetic patients. Additionally, the prognostic utility of stress imaging techniques in diabetic patients was studied during short-term and intermediate-term follow-up, with no available information with regard to long-term follow-up. The aim of this study was to determine whether ischemia on stress 99mTc-tetrofosmin myocardial perfusion imaging provides independent information for prediction of all causes of mortality during long-term follow-up in diabetic patients with known or suspected CAD.
MATERIALS AND METHODS
Patients
The initial study population consisted of 299 consecutive patients with diabetes mellitus who were referred, between November 1995 and December 2002, for exercise or dobutamine stress 99mTc-tetrofosmin SPECT for evaluation of suspected or known CAD at the Thoraxcenter (Rotterdam, The Netherlands). The choice of stress test was based on the ability to exercise. Follow-up was successful in 297 (99%) patients and the data of these patients are reported. All patients gave informed consent before the test. The Ethics Committee of University Hospital Dijkzigt (Rotterdam, The Netherlands) approved the protocol. A structured interview and clinical history were acquired and cardiac risk factors were assessed before nuclear testing.
Diabetes mellitus was defined as a fasting glucose level of ≥140 mg/dL or the need for insulin or oral hypoglycemic agents. Hypercholesterolemia was defined as a total cholesterol of ≥200 mg/dL or treatment with lipid-lowering medications. Overt nephropathy was defined as an albumin excretion rate of >200 μg/min on at least 2 of 3 timed urine samples or, in the absence of urine, a serum creatinine level of >2 mg/dL, renal failure, or renal transplant. Peripheral neuropathy was considered to be present if there was decreased or absent deep tendon reflexes or signs of sensory loss. Peripheral vascular disease was defined by a history of amputation or claudication or an ankle brachial index of <0.9 at rest. Hypertension was defined as blood pressure of ≥140/90 mm Hg or use of antihypertensive medication (24).
Stress Test Protocols
Patients were instructed to discontinue β-blockers at least 24 h before the stress test, whenever applicable. Other medications were not routinely discontinued. An exercise stress test was performed on 68 patients using a symptom-limited upright bicycle ergometry test with stepwise increment of 20 W/min. Dobutamine-atropine stress testing was performed on 229 patients. Dobutamine was infused intravenously, starting at a dose of 10 μg/kg/min for 3 min, increasing by 10 μg/kg/min every 3 min up to a maximum dose of 40 μg/kg/min (21,22). If the test endpoint was not reached at a dobutamine dose of 40 μg/kg/min, atropine (up to 1 mg) was given intravenously. Blood pressure, heart rate, and electrocardiography were continuously monitored. Test endpoints were achievement of target heart rate (85% of maximum age-predicted heart rate), horizontal or downsloping ST-segment depression of >2 mm at an interval of 80 ms after the J point compared with baseline, severe angina, systolic blood pressure fall of >40 mm Hg, blood pressure of >240/120 mm Hg, and significant cardiac arrhythmia. Metoprolol was available to reverse the side effects of dobutamine or atropine if these did not revert spontaneously.
Cuff blood pressure measurements and 12-lead electrocardiography were recorded at rest and every minute during stress and recovery. Significant ST-segment depression was defined as >1-mm horizontal or downsloping ST-segment depression occurring at 80 ms after the J point.
99mTc-Tetrofosmin SPECT
An intravenous dose of 370 MBq of 99mTc-tetrofosmin (Myoview; Amersham) was administered approximately 1 min before termination of the dobutamine or exercise test (25,26). For resting studies, 370 MBq of 99mTc-tetrofosmin were injected at least 24 h after the exercise study. Image acquisition was performed with a triple-head γ-camera system (Prism 3000 XP; Picker International). For each study, 6 oblique (short axis) slices from the apex to the base and 3 sagittal (vertical long axis) slices were defined. Each of the 6 short-axis slices was divided into 8 equal segments. The septal part of the 2 basal slices was excluded from analysis because this region corresponds to the fibrous portion of the interventricular septum and normally exhibits reduced uptake. Consequently, a total of 47 segments was identified (3 long axis and 44 short axis). The interpretation of the scan was semiquantitatively performed by visual analysis. Stress and rest tomographic views were reviewed side by side by an experienced observer who was unaware of each patient’s clinical data. A reversible perfusion defect was defined as a perfusion defect on stress images that partially or completely resolved at rest in ≥2 contiguous segments or slices in the 47-segment model. This was considered diagnostic of myocardial ischemia. A fixed perfusion defect was defined as a perfusion defect on stress images in 2 or more contiguous segments or slices, which persists on rest images in the 47-segment model. An abnormal study was considered in the presence of a fixed or reversible perfusion defect. In our laboratory, the interobserver agreement on the interpretation of stress tetrofosmin images is 93%. The intraobserver agreement is 95%.
The impact of the extent of perfusion abnormalities on the outcome was evaluated by estimation of the number of coronary arterial territories with perfusion abnormalities on the stress images (26). Myocardial segments were assigned to corresponding coronary arteries as follows: the anterior wall and anterior septum to the left anterior descending coronary artery, the posterolateral wall to the left circumflex artery, and the basal posterior septum and the inferior wall to the right coronary artery. The apex was assigned to arterial distribution with concomitant abnormalities. Isolated apical abnormalities were considered indicative of single-vessel CAD. To obtain a semiquantitative assessment of the severity of perfusion abnormalities, the left ventricular myocardium was divided into 6 major segments: anterior, inferior, septal anterior, septal posterior, posterolateral, and apical. Each of the 6 major left ventricular segments was scored using a 4-point scoring system, and a summed stress score was obtained by adding the scores of the 6 myocardial segments at stress (25).
Follow-Up
Follow-up data collection was performed by contacting the patient’s general practitioner and by review of hospital records. In addition, vital status was verified through the civil data registry. The outcome endpoint was death from any cause. Other events noted during follow-up were myocardial revascularization and nonfatal myocardial infarction, defined by cardiac enzyme levels and electrocardiographic changes. Cardiac death was considered to be caused by acute myocardial infarction, significant arrhythmias, or refractory heart failure. Sudden unexpected death occurring without another explanation was included as cardiac death. Hard cardiac events were defined as cardiac death or nonfatal myocardial infarction.
Statistical Analysis
Continuous data were expressed as mean value ± SD. The Student t test was used to analyze continuous data. Differences between proportions were compared using the χ2 test. Univariate and multivariate Cox proportional hazard regression models (BMDP Statistical Software Inc.) were used to identify predictors of events. Parameters considered for multivariate analysis were those with P < 0.05 in the univariate analysis. Variables were selected in a stepwise forward selection manner with entry and retention set at a significance level of 0.05. The probability of survival was calculated using the Kaplan–Meier method. Survival curves were compared using the log-rank test.
RESULTS
Clinical Data
There were 190 (64%) men with a mean age of 60 ± 9 y. Seventy-four (25%) patients had type I diabetes mellitus. Additional risk factors for CAD were hypertension in 182 (61%) patients, hypercholesterolemia in 140 (47%) patients, and smoking in 57 (19%) patients. Eighty-eight (30%) patients had a history of previous myocardial infarction and 61 (21%) patients underwent previous myocardial revascularization procedures. Medications included β-blockers in 113 (38%), angiotensin-converting-enzyme inhibitors in 126 (42%), diuretics in 94 (32%), and calcium channel blockers in 179 (60%) patients.
Stress Test Data
There was a significant increase of heart rate (80 ± 17 vs. 133 ± 18 beats/min) and systolic blood pressure (146 ± 23 vs. 169 ± 34 mm Hg) from rest to peak stress, respectively. ST-segment depression occurred in 59 (20%) patients and angina occurred in 66 (22%) patients with stress. The mean achieved workload with exercise was 121 ± 40 W. The mean maximal dobutamine dose was 33 ± 10 μg/kg/min. Atropine was administered in 95 patients. The target heart rate was achieved in 266 (89%) patients.
SPECT and Follow-Up Results
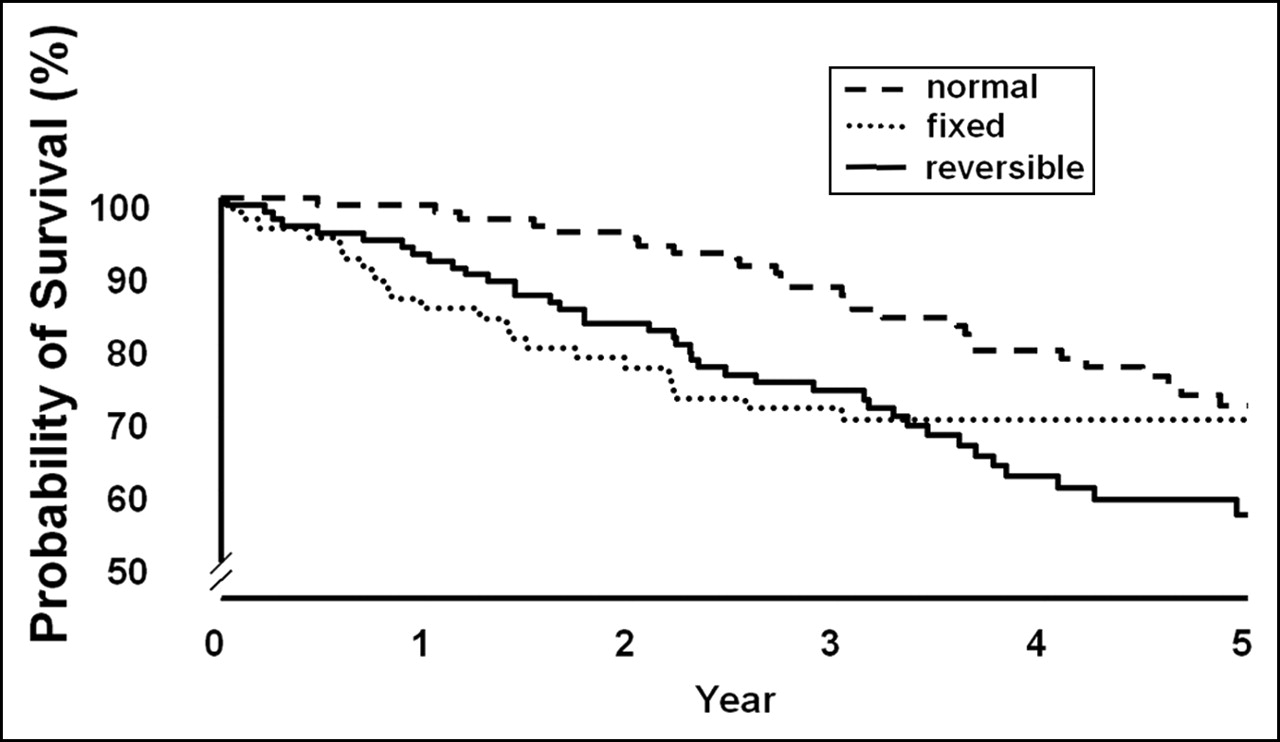
A normal scan was detected in 118 (40%) patients. An abnormal scan was detected in 179 (60%) patients. Myocardial perfusion abnormalities were fixed in 76 (26%) patients and were reversible in 103 (35%) patients. Among patients with reversible defects, 32 had completely reversible defects and 71 had resting perfusion defects as well. Perfusion abnormalities were observed in a single-vessel distribution in 92 patients and in a multivessel distribution in 87 patients. During a mean follow-up of 6 ± 2.1 y, 80 (27%) patients died. Death was considered to be cardiac in 49 (16%) patients. Nonfatal myocardial infarction occurred in 14 (5%) patients, and 53 (18%) patients underwent coronary revascularization. The annual mortality rate was 2.5% in patients with normal perfusion, 4.5% in patients with fixed defects, and 6% in patients with ischemia. The group of patients with both reversible and fixed defects had the worst outcome, with an annual death rate of 7.2%. The annual death rate was 6.5% in patients with multivessel distribution of perfusion abnormalities and 4.3% in patients with a single-vessel distribution (P < 0.05). Survival curves are presented in Figure 1. The annual cardiac death rate was 4.2% in patients with ischemia and 2.6% in patients with fixed defects. In patients with normal perfusion, the annual cardiac death rate was 0.9% during the 5 y after the stress and 1.6% in the sixth to eighth year.
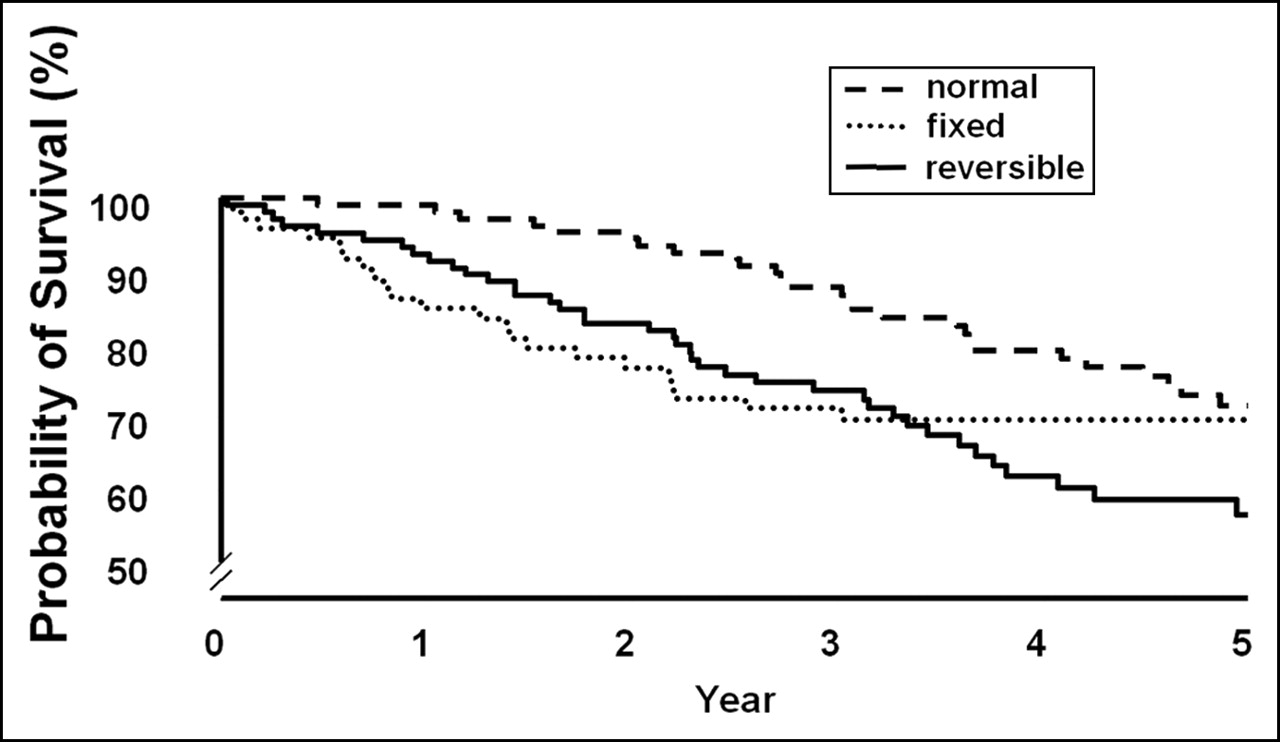
Kaplan–Meier survival curves (total mortality) in diabetic patients with normal perfusion, reversible defects, and fixed defects.
Predictors of Mortality and Cardiac Events
Clinical, stress test, and scintigraphic data of patients who survived versus patients who died are presented in Table 1. Multivariate predictors of mortality are presented in Table 2. Reversible perfusion defects were independently predictive of death. Multivariate predictors of cardiac death and hard cardiac events are presented in Table 2. Both reversible and fixed defects were independently predictive of cardiac events.
Clinical, Stress Test, and Scintigraphic Data of Patients Who Survived and Patients Who Died During Follow-Up
Independent Predictors of Mortality and Cardiac Events in Multivariate Analysis Models
DISCUSSION
In this study, we assessed the independent prognostic value of stress 99mTc-tetrofosmin SPECT for the prediction of all-cause mortality in 297 diabetic patients with known or suspected CAD. Ischemia (reversible perfusion abnormalities) was detected in 35% of patients. During a mean follow-up of 6 y, 80 (28%) patients died. Among the clinical parameters, advanced age, a history of heart failure, peripheral vascular disease, and a lower stress systolic blood pressure were independent predictors of death. Myocardial ischemia was independently associated with an increased risk of total and cardiac death after controlling for clinical data. The annual mortality rate was 2.5% in patients with normal perfusion, 4.5% in patients with fixed defects, and 6% in patients with ischemia. Patients with both reversible and fixed defects had the worst outcome, with an annual death rate of 7.2%. Patients with perfusion abnormalities in multivessel distribution had a higher mortality rate than patients with abnormalities in a single-vessel distribution.
The reported annual mortality rate in epidemiologic studies ranged between 4.8% and 9% in diabetic patients who were 44–75 y old (5–7). Therefore, an annual mortality rate of 2.5% in patients with normal perfusion imaging in our study may represent a significantly lower risk of death than what is expected in the general diabetic population. However, differences in population characteristics are potential confounders for such comparison.
A lower peak systolic blood pressure was associated with an increased risk of death in our study. Some previous studies have shown an association of impairment of systolic blood pressure response to exercise (27) and dobutamine (28) with an adverse outcome. This has been explained by a lower cardiac reserve in patients with impaired systolic blood pressure response. The associated risk of mortality related to ischemia was independent of symptoms and clinical risk factors. The association of combined fixed and reversible perfusion abnormalities with the worst outcome can be explained by the possibility that ischemia superimposed on necrotic myocardium may contribute to myocardial remodeling, with progressive worsening of left ventricular function, and may trigger fatal arrhythmic events on a substrate of myocardial fibrosis, as opposed to ischemia that occurs in a myocardium with no structural abnormalities (29–31). A history of heart failure was an important clinical predictor of both total mortality and hard cardiac events, consistent with previous studies in general populations as well as diabetic populations (32,33). Peripheral vascular disease was associated with an increased risk of death consistent with previous studies (34).
Some studies have shown a good outcome of diabetic patients with a normal stress myocardial perfusion during short-term follow-up. We demonstrated in this study that the relatively low-risk warrantee (as compared with mortality in the general diabetic population) was maintained up to 5 y of follow-up, which suggests that patients with a normal stress tetrofosmin study may require stress testing less frequently during the 5 y after the stress test.
Total Mortality as an Endpoint
The use of “cardiac death” instead of all-cause death as an endpoint in clinical investigations may be limited by inaccuracies or bias of data obtained from death certificates or from medical records and the inherent difficulties in determining cause of death owing to the presence of concurrent comorbid illnesses (23). CAD may, in fact, be present and significant at the time of death and, yet, not be the primary reason a patient may die. This should be considered especially in diabetic patients because other causes of mortality in these patients, such as renal failure and peripheral vascular disease, are strongly associated with the incidence of CAD. Therefore, recently there has been a growing interest in the use of all causes of death as an endpoint against which therapeutic and diagnostic interventions are weighted.
In our study, the annual total death rate was 2.5% in patients with normal perfusion and 6% in patients with ischemia. These data suggest that interventions based on the results of myocardial perfusion scintigraphy in diabetic patients may improve overall survival, which is the ultimate target of therapeutic interventions in patients with known or suspected CAD. It should be emphasized that the results of this study apply to diabetic patients with known or suspected CAD who have either symptoms or additional risk factors; therefore, the results cannot be generalized to a lower risk population. Previous studies have shown that myocardial ischemia is not uncommon in asymptomatic diabetic patients (35,36). In our study, heart failure, but not angina, was predictive of events.
Comparison with Previous Studies
To our knowledge, there are no available data to suggest a role of myocardial ischemia on stress myocardial perfusion imaging in predicting all-cause mortality in diabetic patients. Additionally, the prognostic utility of stress imaging techniques has been demonstrated during short-term and intermediate-term follow-up, whereas long-term follow-up data are missing.
Felsher et al. (17) demonstrated that exercise planar thallium imaging was useful for the risk stratification of 123 diabetic patients. Four cardiac deaths and 8 nonfatal infarctions occurred during the follow-up period of 1.8 ± 0.9 y. Vanzetto et al. (22) evaluated the prognostic value of exercise thallium imaging in 158 diabetic patients. During a mean follow-up of 1.9 y, cardiac death occurred in 8 patients and nonfatal infarction occurred in 14 patients. The authors concluded that the inability to exercise was associated with a high risk of events and suggested that, for the assessment of prognosis in these patients, pharmacologic stress myocardial perfusion imaging be performed. Cohen et al. (21) demonstrated that abnormal dipyridamole stress thallium images were important adverse indictors of prognosis in 101 diabetic patients undergoing peripheral vascular surgery.
Kang et al. (16) evaluated the prognostic value of rest 201Tl/stress 99mTc-sestamibi myocardial perfusion imaging in 1,080 patients with diabetes. During the follow-up period of 2 ± 0.6 y, 50 cardiac deaths and 42 nonfatal infarctions occurred. An abnormal scan provided incremental prognostic information over clinical data. Giri et al. (18) studied 929 diabetic patients after exercise or vasodilator stress myocardial perfusion imaging. During a follow-up period of 2.5 ± 1.5 y, 39 deaths and 41 nonfatal infarctions occurred. The presence and the extent of abnormal stress myocardial perfusion imaging independently predicted subsequent cardiac events. Schinkel et al. (19) demonstrated that dobutamine stress myocardial perfusion imaging provided incremental information for predicting cardiac death and nonfatal myocardial infarction in 207 diabetic patients who were followed for 4.1 y. Rajagopalan et al. (37) studied 1,427 asymptomatic diabetic patients without known CAD during exercise or pharmacologic stress. The study used 99mTc-sestamibi or 201Tl. An abnormal stress SPECT scan was present in 826 (58%) patients and a high-risk scan was present in 261 (18%) patients. Annual mortality rates for patient subsets categorized by SPECT scans were high risk, 5.9%; intermediate risk, 5.0%; and low risk, 3.6%. Independent predictors of mortality were not evaluated in their study.
Limitations
The sample size was relatively small and included a heterogeneous population. Further studies are required to determine whether these results are applicable for patients with known CAD versus those with suspected CAD and for older patients. Gated SPECT data were not available in all patients; therefore, the prognostic information obtained from left ventricular function and transient left ventricular dilation could not be assessed. The diagnosis of myocardial infarction during follow-up was based on clinical data. It cannot be excluded that some patients may have sustained a silent myocardial infarction, because no follow-up imaging study was implemented to assess wall motion. Patients with limited exercise capacity received dobutamine rather than the vasodilator stress test. Earlier studies have shown that the grade of hyperemia induced by dobutamine is less than that induced by vasodilators such as dipyridamole and adenosine (38). However, recent studies have shown that with standard high-dose dobutamine–atropine stress testing, the extent of hyperemia is not less than that observed with dipyridamole (39,40). Although mortality was higher among patients who underwent dobutamine stress compared with patients who underwent exercise stress, the type of stress test was not independently predictive of mortality after adjustment for clinical and perfusion data.
CONCLUSION
Myocardial ischemia on stress 99mTc-tetrofosmin myocardial perfusion imaging is associated with an increased risk of all causes of mortality during long-term follow-up among diabetic patients, after adjustment for clinical data. Patients with a normal perfusion study had a lower death rate during the 5 y after stress testing as compared with the reported death rate in the general diabetic population in epidemiologic studies. Therefore, these patients may require less frequent testing during that period, unless there was a change in the clinical condition.
Acknowledgments
This study was supported in part by a publication grant from GE Healthcare.
Footnotes
Received Feb. 22, 2005; revision accepted Jun. 13, 2005.
For correspondence or reprints contact: Abdou Elhendy, MD, PhD, 982265 Nebraska Medical Center, Omaha, NE 68198-2265.
E-mail: aelhendy{at}unmc.edu
REFERENCES
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- Endothelial Dysfunction in Diabetic Patients with Abnormal Myocardial Perfusion in the Absence of Epicardial Obstructive Coronary Artery Disease
- Incidence and Prognostic Implication of Unrecognized Myocardial Scar Characterized by Cardiac Magnetic Resonance in Diabetic Patients Without Clinical Evidence of Myocardial Infarction
- The Year in Cardiac Imaging