


Abstract
The aim of this study was to investigate the pharmacokinetics, organ dosimetry, and toxicity after the intraarterial administration of 188Re-labeled 4-hexadecyl-1,2,9,9-tetramethyl-4,7-diaza-1,10-decanethiol/lipiodol (188Re-HDD/lipiodol) for palliative treatment of hepatocellular carcinoma (HCC). A secondary objective was to document the response. Methods: A mean activity of 3.60 GBq 188Re-HDD/lipiodol (range, 1.86–4.14 GBq) was administered to 11 patients (16 treatment sessions) via a transfemoral catheter. The pharmacokinetic and dosimetric data were collected by means of venous blood samples, urine collections, and 4 or 5 γ-scintigraphies over 76 h. Absorbed doses to the various organs were calculated according to the MIRD formalism, using the MIRDOSE3.1 software. The toxicity was assessed until 6 wk after administration by means of the Common Toxicity Criteria scale. The response was evaluated on MRI and by monitoring of the tumor marker. Results: A fast blood clearance of the injected activity was observed with a calculated effective half-life of 7.6 ± 2.2 h (±SD) in blood. The predominant elimination of the activity was through urinary excretion with a mean renal clearance of 44.1% ± 11.7% (±SD) of the injected activity within the 76 h after administration. Fecal elimination was negligible. The calculated whole-body effective half-life was 14.3 ± 0.9 h (±SD). The absorbed dose to the liver tissue, the lungs, the kidneys, and the thyroid was 4.5 ± 1.9, 4.1 ± 1.2, 0.9 ± 0.7, and 0.3 ± 0.1 Gy, respectively. Treatment was well tolerated, except in 2 patients. One Child B patient experienced a worsening of his liver dysfunction (hyperbilirubinemia) and another patient experienced dyspnea and coughing. Response assessment on MRI showed 1 case of partial response, disease stabilization in 11 treatments, and progressive disease in 1 treatment. In 5 of 8 treatment sessions with an initially elevated α-fetoprotein, a reduction (range, 19%–90%) was observed 6 wk later. Conclusion: After the intraarterial administration of 3.60 GBq 188Re-HDD/lipiodol, a fast clearance of the activity appearing in the blood is observed and the predominant elimination is through urinary excretion. The tolerance as well as the preliminary response rates of the present phase I study are encouraging.
- hepatocellular carcinoma
- lipiodol
- 188Re
- radionuclide therapy
- 4-hexadecyl-1,2,9,9-tetramethyl-4,7-diaza-1,10-decanethiol
Hepatocellular carcinoma (HCC) is the most prevalent primary liver cancer. It constitutes the third cause of cancer-related deaths and is responsible for >500,000 deaths worldwide annually (1). Although the overall incidence of HCC in the West is low compared with that in Southeast Asia, Sub-Saharan Africa, and Japan, its incidence is rising (2,3). Due to the underlying carcinogenic risk factors, such as chronic viral hepatitis and alcohol intake, most patients presenting with HCC have cirrhosis, a condition limiting the therapeutic possibilities. Surgery, either by means of hepatectomy or liver transplantation, is the mainstay of curative treatment. Overall, if the degree of liver dysfunction and the tumor load are taken into consideration, most patients are not eligible for surgery (4).
Percutaneous alcohol injection, (chemo)embolization, and radiofrequent ablation are among the most common treatment modalities (5). Survival advantages have been identified with chemoembolization in well-selected patients (6). Other treatment modalities producing response rates exceeding 20% are the use of lipiodol mixed with chemotherapeutic agents or radiolabeled with 131I without subsequent embolization (7). Encouraging results have been obtained using 131I-lipiodol, but the use of 131I has hampered its routine clinical implementation (8,9). 131I has a physical half-life of 8 d and emits a high-energy γ-ray (364 keV, with an abundancy of 82%), necessitating delayed hospitalization for radioprotection purposes. Although 131I-lipiodol therapy is generally well tolerated, to our knowledge, a dose-escalation study has not been conducted so far because the administration of activities exceeding 2.22 GBq is restricted by the practical issues. 188Re has favorable characteristics for radionuclide therapy and, considering the limited success of 131I-lipiodol for treatment of relatively large tumors, the switch toward a radionuclide with a higher-energy β-emission (2,120 and 1,960 keV for 188Re vs. 606 keV for 131I) might yield improved response rates (10). 188Re emits a γ-ray of 155 keV with an abundancy of 15%, allowing γ-camera imaging, and it has a relatively short physical half-life of 17 h, limiting radiation protection problems. Additionally, the radionuclide is eluted from a 188W/188Re generator, which has a long useful shelf life of several months and provides a good yield of carrier-free 188Re routinely (11).
During the past 10 y, promising preclinical results using 188Re-labeled lipiodol for treatment of HCC have been reported (12–14). Only recently, however, were the first clinical results using 188Re-labeled 4-hexadecyl-1,2,9,9-tetramethyl-4,7-diaza-1,10-decanethiol/lipiodol (188Re-HDD/lipiodol) reported by Sundram et al. (15,16). The aim of our study was to assess the biodistribution and feasibility of a locoregional administration of 3.7 GBq of 188Re-HDD/lipiodol for palliative treatment of HCC patients.
MATERIALS AND METHODS
Synthesis and Quality Control of Radioconjugate
188W/188Re generators were purchased from Oak Ridge National Laboratory and the Institut des Radio-Eléments. Lyophilized kits containing an HDD chelator (4-hexadecyl-1,2,9,9-tetramethyl-4,7-diaza-1,10-decanethiol) were provided by the Seoul National University Hospital, and 188Re-HDD/lipiodol was synthesized as described by Jeong et al. (13). Briefly, the concentrated eluate (6 mL) from a commercially available 188W/188Re generator containing 11.1 GBq was heated with the HDD/SnCl2 kit at 100°C for 1 h to produce 188Re-HDD complex (17). Three milliliters of lipiodol were added and mixed on a vortex to extract the 188Re-HDD into the lipiodol. After centrifugation at 4,000g, the 188Re-HDD/lipiodol fraction was separated. Finally, the 188Re-HDD/lipiodol layer was washed with a 0.9% NaCl solution. Quality control was performed according to the method described by Jeong et al. by instant thin-layer chromatography (ITLC-SG plates [mobile phase, 0.9% NaCl and acetone]; Gelman Sciences) (13). In all cases, radiochemical purity was >95%. The total radiochemical yield was 53% ± 4.5%.
Patient Selection
The diagnosis of HCC had to be established by means of CT, MRI, or arteriography, eventually in conjunction with an elevated α-fetoprotein level or biopsy. Exclusion criteria were eligibility for liver resection or transplantation, pregnancy and breast feeding, age < 18 y, Child C status according to the modified Child-Pugh score, Okuda III disease stage, poor general condition (Karnofsky < 70%), white blood cell count < 1,500/μL, and potentially toxic anticancer treatment in the preceding 3 mo. Additional contraindications for the arteriography and isolation procedure were as follows: serum creatinine level > 2 mg/dL, prothrombin time < 50% of the normal value, platelet count < 50,000/μL, inability to care for oneself, encephalopathy, and incontinence. The institutional ethics committee approved the study, and informed written consent was obtained from all patients.
Administration
Under local anesthesia, a 5-French catheter was inserted transfemorally and introduced into the proper hepatic artery. After obtaining a diagnostic hepatic arteriogram, approximately 4 mL 188Re-HDD/lipiodol were injected slowly into the proper hepatic artery under fluoroscopic control. Whenever an aberrant arterial supply was present, the radioconjugate was injected selectively into the right and left hepatic arteries separately. The 4-mL volume was divided over the different hepatic arteries proportionately to the volume of liver parenchyma supplied by the respective artery. To reduce uptake of free perrhenate in the thyroid or gastric mucosa, patients received 0.5 g sodium perchlorate before 188Re-HDD/lipiodol administration followed by 1 g daily until discharge.
Pharmacokinetic and Dosimetric Study
After 188Re-HDD/lipiodol administration, patients were hospitalized in a dedicated radionuclide therapy room for 4 d. Whole-body scintigraphies (±SD) were acquired in all patients at 1.7 ± 1.2, 20.0 ± 1.9, 27.6 ± 1.9, 51.7 ± 1.8, and 75.4 ± 1.8 h after administration using a triple-head γ-camera (IRIX; Philips) equipped with medium-energy, parallel-hole collimators. The imaging window was set at 155 keV (20%). Scan speed varied from 30 to 10 cm/min depending on the time elapsed since administration. For quantification purposes, a syringe containing a known activity of 188Re was included in the whole-body scan.
During the hospitalization period, patients collected their urine. Before each whole-body scan, urinary volumes were recorded and samples were taken. On these occasions, venous blood samples were also taken. Blood and urine samples were analyzed in a NaI(Tl) 3 × 3 in. γ-well counter calibrated for 188Re (Cobra II; Perkin Elmer). Time-activity curves were generated for blood and urinary activity and fitted monoexponentially (SPSS software version 10.0).
For data analysis, whole-body images were transferred to a HERMES system (Nuclear Diagnostics). Regions of interest (ROIs) were drawn around the syringe, the total body, the liver (including tumor), the lungs, and a background region on the first scan. ROIs were mirrored to the posterior image and copied to subsequent scans. The background-corrected geometric mean of the total counts in the ROIs was used to calculate the total amount of activity in the total body, the liver, and the lungs, using the known activity in the syringe. Experimental factors were determined on an anthropomorphic phantom (Alderson Heart/Thorax SPECT phantom; Capintec Inc.) for the conversion of the syringe activity into organ activity. The overall uncertainty using this methodology for the activity calculation was <18%.
Monoexponential time-activity curves were generated for the total body, the liver, and lungs using SPSS 10.0 software. Source organ residence times were determined from integration of the time-activity curves. Absorbed doses to the various organs were calculated according to the MIRD formalism, using the MIRDOSE3.1 (Oak Ridge Associated Universities) software package (18). Using the time-activity curves of the blood samples, red marrow absorbed dose was calculated according to the methodology described by Sgouros (19).
The patient’s dose rate was regularly measured at a 1-m distance from the liver region using a survey meter.
Toxicity and Response Assessment
Laboratory testing of red and white blood cells and platelets, liver function, renal function, and serum α-fetoprotein were performed shortly before treatment, on the third day, and at 2 and 6 wk after injection. Clinical evaluation of toxicity was performed daily during hospitalization and 2 and 6 wk later. Toxicity was scored by means of the Common Toxicity Criteria (Cancer Therapy Evaluation Program. Common Toxicity Criteria, version 2.0; Division of Cancer Treatment and Diagnosis, National Cancer Institute, National Institutes of Health, Department of Health and Human Services, March 1998). Laboratory findings were compared by means of Wilcoxon statistical testing, and the significance level was set at P < 0.05 (SPSS version 10.0). Radiologic response was assessed by means of the RECIST response criteria (response evaluation criteria in solid tumors) on MR images acquired 6 wk after treatment (20). Patients without evidence of progressive disease were eligible for repetitive treatment sessions with a 12-wk interval.
RESULTS
Eleven patients underwent 16 treatment sessions. The mean administered activity per session was 3.60 GBq (range, 1.86–4.14 GBq). Eight patients were treated once, 1 patient was treated twice, and 2 patients were treated 3 times. Patient characteristics are summarized in Table 1.
Patient Characteristics
Pharmacokinetic Data and Organ Dosimetry
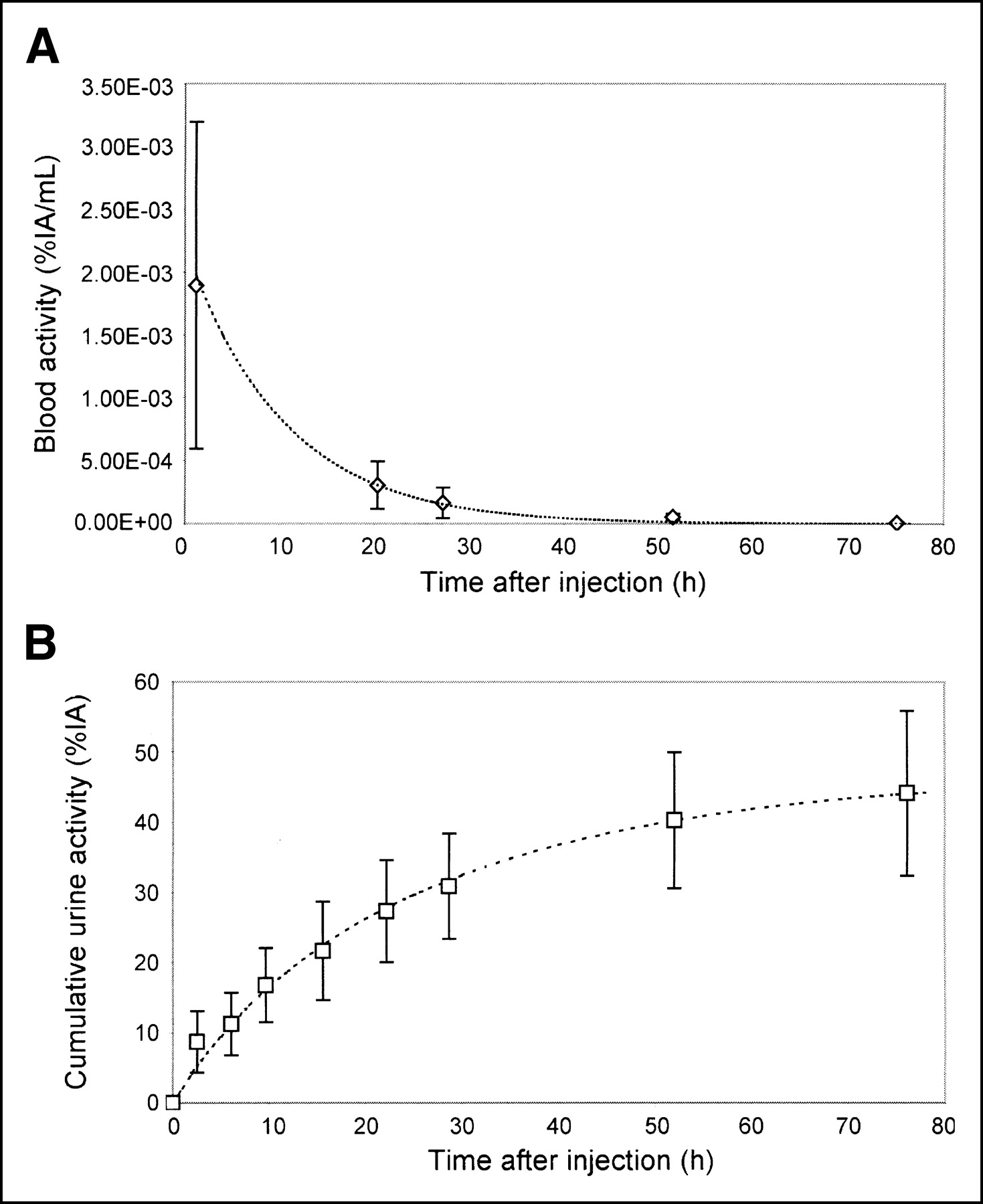
In 7 treatment sessions, a minimum of 4 blood samples were taken within 76 h of administration. A fast blood clearance of the injected activity was observed, with a calculated mean effective half-life of 7.6 ± 2.2 h (±SD) in blood. The estimated blood activity at time 0 was 77.2 ± 64.4 kBq/mL (±SD).
Urinary excretion was assessable during hospitalization in all treatments. A mean of 44.1% ± 11.7% (±SD) of the administered activity was excreted within 76 h after administration. The largest fraction was excreted within the first 21 h (25.9% ± 6.3%). ITLC analysis showed that the activity in the urinary samples was perrhenate. Blood activity levels and cumulative urinary excretion of the injected activity are plotted as a function of time in Figure 1. Based on the urinary excretion levels, a mean whole-body effective half-life of 14.3 ± 0.9 h (±SD) was calculated using a monoexponential fitting.

(A) Blood activity levels in percent of injected activity per milliliter blood (%IA/mL) as function of time after injection. (B) Cumulative urinary excretion of activity in percent of injected activity (%IA) plotted as function of time after injection.
Feces were collected on 3 occasions; fecal elimination proved negligible (0.9% ± 0.2%; mean ± SD of the administered activity). Scintigraphies showed activity in the small bowel and colon, which was faint on 4 occasions and significant on 1 occasion.
The absorbed doses to the organs were calculated in all treatment sessions except one (session 7c) because of technical problems (Table 2). The MIRDOSE red marrow absorbed dose (0.30 ± 0.08 Gy) is in good agreement with the red marrow dose calculation based on the methodology of Sgouros (0.44 ± 0.21 Gy). No thyroid activity was seen on the scintigraphies (Fig. 2). The mean effective dose estimation was 1.0 ± 0.2 Sv (±SD).
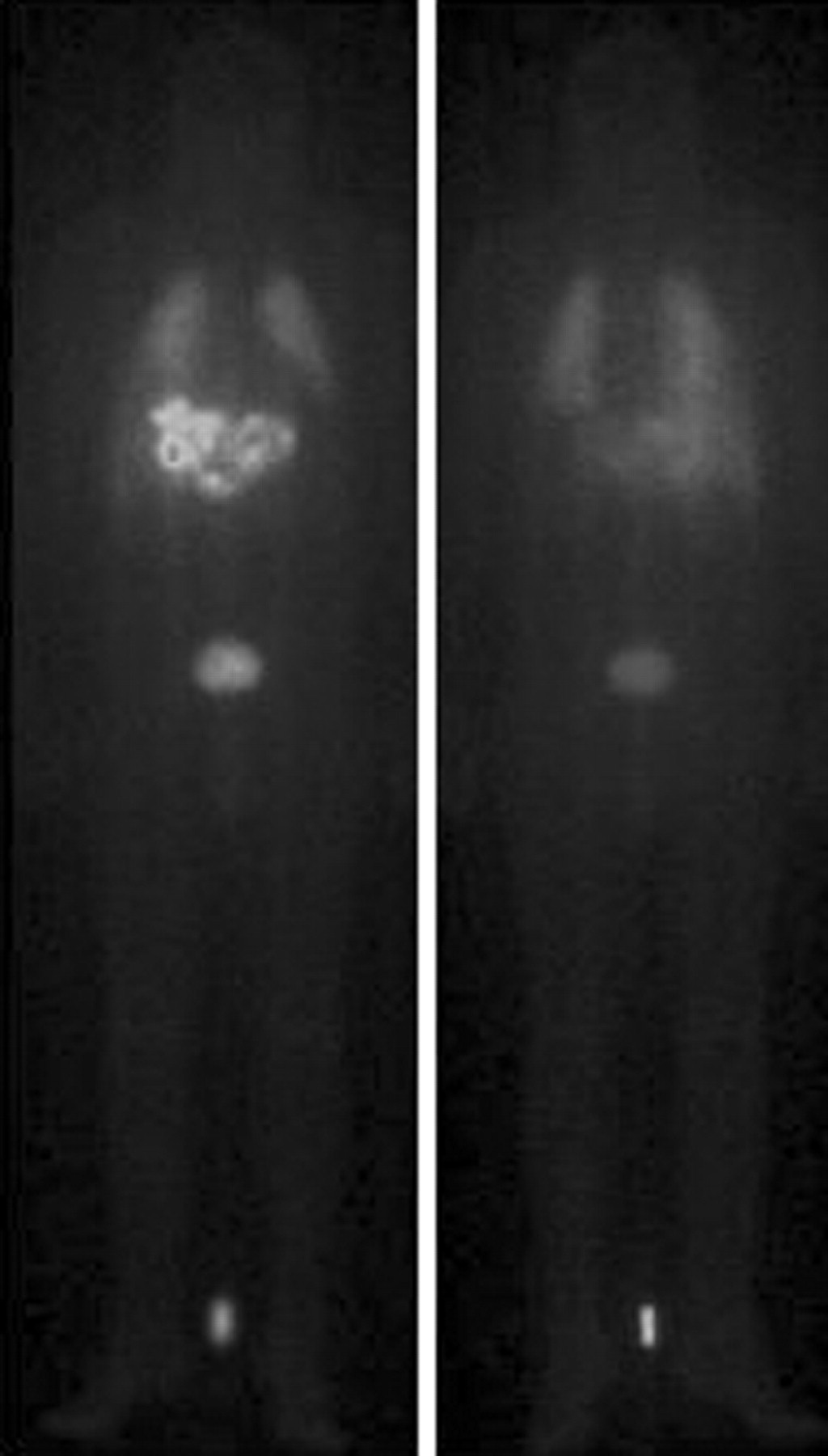
Whole-body scans (right, anterior image; left, posterior image) of patient 4 performed 30 h after administration of 4.12 GBq 188Re-HDD/lipiodol. Significant uptake is seen in multifocal HCC and in bladder. Faint uptake is observed in lungs and no uptake is evident in thyroid or gastric mucosa.
Absorbed Doses for Various Normal Organs After Treatment with 3.34 ± 0.93 GBq 188Re-HDD/Lipiodol (Mean ± SD)
The dose rate at 1 m dropped below 20 μSv/h within the first 24 h after administration and did not exceed 5 μSv/h on day 2.
Toxicity
In Table 3, the adverse events are scored according to the Common Toxicity Criteria, version 2.0. Only the events reflecting a worsening compared with the baseline values are tabulated. Patient 1 received a “special request” liver transplantation after 5 wk, excluding him from subsequent toxicity assessment, and patient 11 did not attend follow-up consultations because of his limited general condition.
Scoring of Adverse Events According to Common Toxicity Criteria, Version 2.0
Hematology.
No significant changes in blood counts were observed at week 2. At week 6, there was a borderline significant decrease in white blood cells and platelets (P = 0.048 and 0.045, respectively). Subanalysis indicated that there were no significant changes in the blood counts if patient 6 was not taken into consideration. In this patient, transient grade 2 leukopenia and grade 3 thrombocytopenia developed. Values for white blood cells and platelets before therapy and at week 6 are depicted in Figures 3A and 3B.

(A) White blood cell counts before therapy and at week 6. (B) Platelet counts before therapy and at week 6. Dashed lines represent sessions 6a and 6b. (C) Bilirubin levels before therapy and at weeks 2 and 6 after therapy. (D) AST levels before therapy and at weeks 2 and 6 after therapy.
Liver Function.
No clinical liver toxicity was encountered, except in patient 1. This Child B patient had a preexisting elevated bilirubin level and a history of spontaneous liver decompensation. Grade 2 fatigue and an aggravation of his icterus developed. Overall, no significant increases were seen in the bilirubin, aspartate aminotransferase, or alanine aminotransferase levels at weeks 2 and 6 (Figs. 3C and 3D). There was no significant change in the modified Child-Pugh score 6 wk after treatment.
Lung Function.
No acute pulmonary symptoms were reported during the hospitalization. A cough developed in patient 6 after his first treatment session. Lung function testing did not reveal any contraindications for further treatment with 188Re-HDD/lipiodol. However, after the second session, dyspnea and cough reoccurred and subsequent lung function testing showed a deterioration of the diffusion capacity (diffusing capacity of lung for carbon monoxide, 43% of the predicted value) and bilateral fibrotic changes were observed on a high-resolution CT scan of the lungs. After oral steroid treatment, spirometric changes resolved and symptomatic relief was rapidly achieved. Because the patient’s compliance to the steroid treatment was unsatisfactory in the late follow-up, symptoms reoccurred several months later.
Other.
No significant changes were observed in the creatinine levels 2 and 6 wk after the procedure. Besides the toxicity possibly related to the investigational agent, some adverse events were due to the catheterization: a small groin hematoma in 3 patients and a grade 1 allergic reaction in 1 patient, with a history of a similar reaction after 131I-lipiodol treatment.
Response
Response on MRI.
Patient 10 had a rapidly progressive multifocal tumor with grade 4 anaplastic disease on pathology. In this patient a partial response was obtained with a reduction of the sum of largest diameters by 41%. Patient 3 had progressive disease after her third treatment with 188Re-HDD/lipiodol. Patients 1 and 11 dropped out from response assessment 6 wk after treatment and patient 5 was not assessable because imaging was performed on different scanners. The remaining patients had stable disease.
Response on α-Fetoprotein.
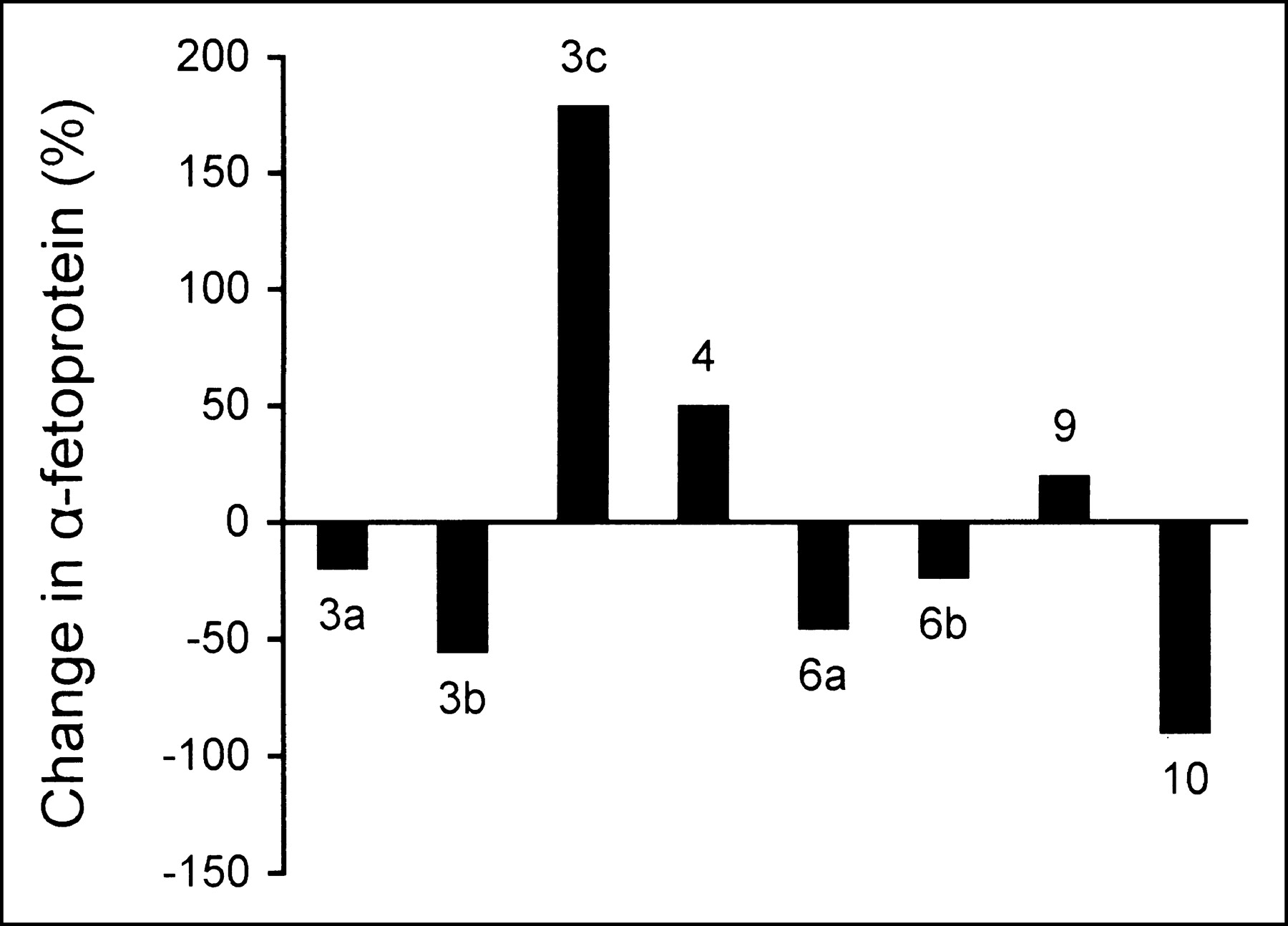
Figure 4 depicts the change in serum α-fetoprotein of baseline values at week 6. In 8 treatment sessions, α-fetoprotein levels were elevated before treatment. In 5 of these treatment sessions, a reduction in tumor marker (range, 19%–90%) was observed 6 wk later.
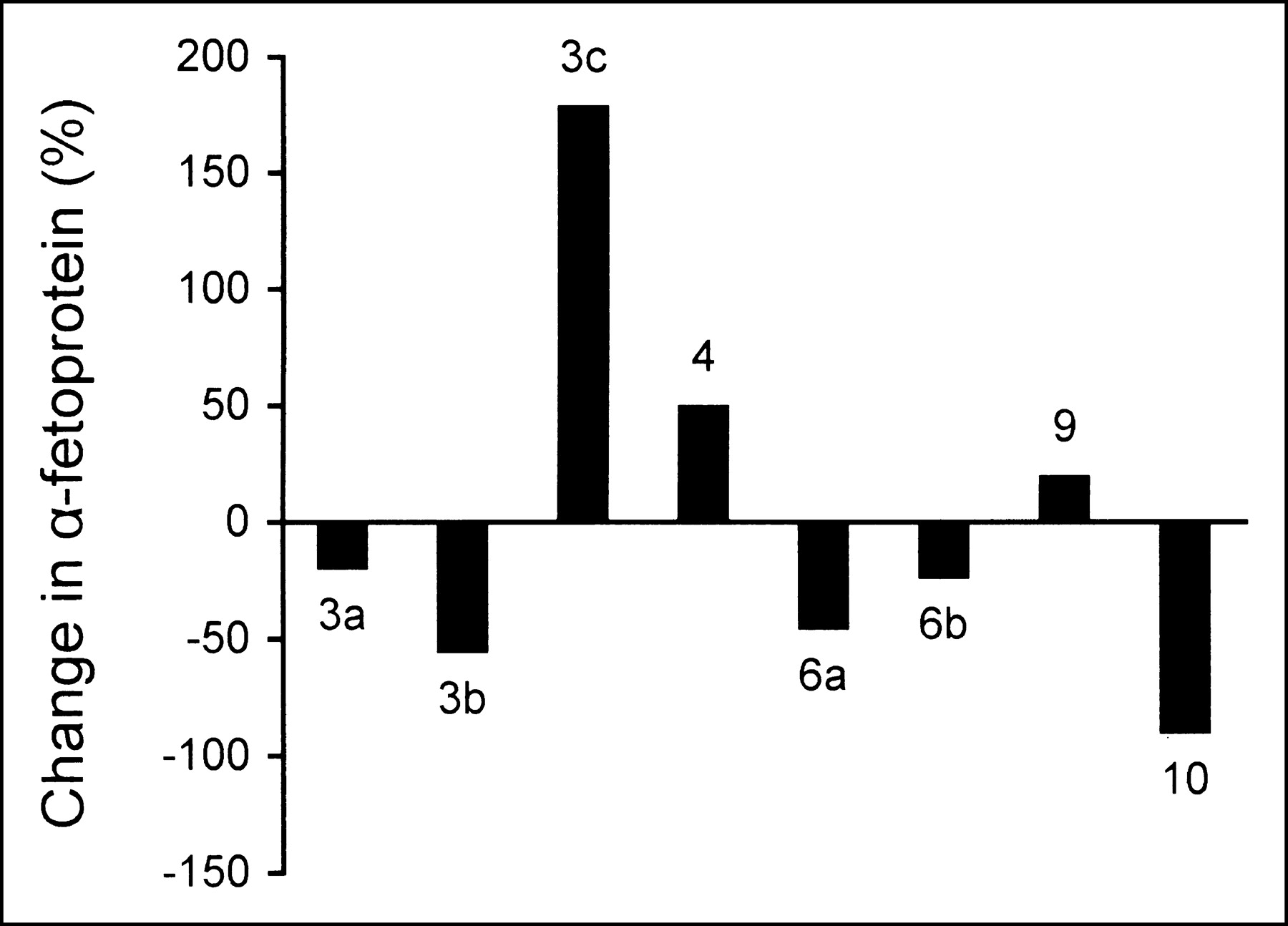
Change in serum α-fetoprotein from baseline values at week 6 in 8 treatment sessions with initially elevated tumor marker level.
DISCUSSION
Taking into account the effective half-life, β-energy, and dose rate, the same effect on the tumor may be expected by 188Re-HDD/lipiodol and 131I-lipiodol when the administered 188Re activity is 60% higher than the 131I activity (21). This calculation is based on isoeffect curves for different dose rates used in brachytherapy (22). Therefore, in the present study we aimed at an administration of 3.7 GBq 188Re-HDD/lipiodol because, before initiation of this study, a fixed activity of 2.2 GBq 131I-lipiodol was usually applied at our institution. A nonselective administration in the hepatic arterial vessels was preferred because development of metachronous HCC in the nontreated segments is described in case the administration of the activity is restricted to the affected segments or lobe (23).
With regard to the labeling procedure, no major technical problems were encountered in 15 of 16 syntheses. In certain European countries, the hospital stay in isolation for up to 7 d to comply with radioprotective guidelines is among the most important constraints of the use of 131I-lipiodol. The patient’s dose rate measured at 1 m dropped below the local limit of 20 μSv/h within 24 h after administration of 188Re-HDD/lipiodol, allowing a significantly shorter hospitalization. The shorter stay in the shielded therapy room and the use of the on-site 188W/188Re generator improved the flexibility in treatment planning.
Because 188Re is attached differently to lipiodol (coordinative binding with a chelator) compared with 131I-lipiodol (covalent binding), differences in metabolism can be expected. We observed a significant accumulation of the radioconjugate in the liver and lungs and, to a much smaller extent, uptake in the gastrointestinal tract and kidneys. The significant lung uptake is in agreement with the initial clinical experiences with 188Re-HDD/lipiodol reported by Sundram et al. and with the previous studies on the biodistribution of 131I-lipiodol (15,16,24–26).
We calculated a biologic half-life in the lungs for 188Re of 8.7 ± 4.9 d (±SD), and this result is in line with our earlier report on the biologic half-life in the lungs after 131I-lipiodol therapy, 10.3 ± 5.2 d (±SD) (27). The relatively long biologic lung half-life in both cases suggests that the activity in the lung is present under a stable formulation from which diffusion to blood is minimal.
In the present study, a considerable number of patients showed faint uptake in other organs, such as the kidneys and parts of the gastrointestinal tract. The data available in the literature concerning the elimination of 131I-lipiodol are scarce, but all investigators agree on the predominant urinary excretion and negligible elimination of 131I in stool. The largest observation, comprising measurements in 10 patients with HCC, yielded a median of 42% urinary excretion of the administered 131I within the first 8 d (24). Nakajo et al. obtained comparable results with a daily excretion from 4.3% to 7.1% (25). In a small biodistribution study conducted by Madsen et al. in 4 patients, a lower daily excretion of 131I (1%–3%) was observed (26). In the experience with 188Re-HDD/lipiodol reported by Sundram et al., a faint visualization of the kidneys was described and they concluded that renal elimination was negligible. However, the urinary excretion was not quantified (16). According to our measurements, a mean of 44.1% of the administered 188Re was excreted in the urine within 76 h. If the shorter physical half-life of 188Re is considered, this value compares favorably with the observations of Raoul et al. (24) and Nakajo et al. (25).
No visualization of the gastrointestinal tract was described in the biodistribution studies using 131I-lipiodol or in the initial reports on 188Re-HDD/lipiodol (15,16,24–26). However, in our experience, in 5 of 16 administrations, transient uptake in the small or large bowel was observed, which was very faint in all patients but one. In the animal study conducted by Lee et al. (14), intestinal uptake was observed after intravenous administration of 188Re-labeled long-chain alkyl diaminedithiol derivatives in mice and the intestinal activity was thought to be the result of bile excretion. In our study, the uptake pattern and its transient character suggested biliary excretion rather than gastrointestinal wall uptake.
Few data are available on the blood activities after 131I-lipiodol administration. Measurements performed by Nakajo et al. (25) and Madsen et al. (26) pointed out that <0.9% of the administered activity was retrieved in the total blood volume with a peak in blood activity after 3 d. This was in contrast to the activities measured in the present study, indicating an initially significant higher blood activity of about 10% of the administered activity of 188Re-HDD/lipiodol, with a rapid decrease over the first 3 d. Sundram et al. performed activity measurements in 5 patients shortly after the administration of a “scout dose” of 200 MBq 188Re-HDD/lipiodol. The obtained activities were considered negligible but the biodistribution data are difficult to compare because most studies vary in the selectivity of administration of the radioconjugate (15,16).
Absorbed doses to the liver, lungs, and thyroid calculated for 1.90 ± 0.20 GBq 131I-lipiodol therapy are significantly higher (7.8 ± 1.8, 6.8 ± 2.9, and 7.2 ± 2.2 Gy, respectively) compared with the absorbed doses in this 188Re-HDD/lipiodol study population (27). The mean effective dose of the 188Re-HDD/lipiodol patients (1.0 ± 0.2 Sv) was significantly lower compared with that of 131I-lipiodol (2.0 ± 0.6 Sv).
The initial clinical experience using 188Re-HDD/lipiodol was described by Sundram et al. (15,16). In this study, about 35 of 70 patients did not experience any adverse event. The most frequent adverse events consisted of mild anorexia, right hypochondriacal discomfort, and low-grade fever (16). We had a similar observation with the occurrence of, in general, only mild toxicity in 9 of 16 treatment sessions. Patient 1 had a significant worsening of his liver dysfunction. Although this patient had a history of frequent liver decompensation and his tumor marker was steeply increasing at week 2, we recommend that additional data be acquired to confirm the safety of 188Re-HDD/lipiodol therapy in patients with Child B liver cirrhosis. No cases of liver failure were reported by Sundram et al. (15,16). However, in that trial, the activity was administered as close to the tumor feeding artery as possible, whereas the present study aimed to treat the whole liver and, therefore, the radioconjugate was injected nonselectively. Sundram et al. reported 2 cases of pleural effusion and these were attributed to radiation-induced pneumonitis (16). In our study, grade 3 lung toxicity developed in patient six 6 wk after his second treatment. The absorbed lung doses of sessions 6a and 6b were estimated to be 4.6 and 5.8 Gy, respectively—hence, too low to explain this evolution. The timing of the occurrence of his symptoms and the associated bone marrow depression are suggestive of an increased sensitivity to ionizing radiation in this patient. No bone marrow depression was observed in the other patients, including the population described by Sundram et al. (16). Although it was unclear whether the occurrence of lung fibrosis in this patient was related to the 188Re-HDD/lipiodol therapy, we advocate that in the future particular attention be paid to patients who have pulmonary complaints. If radiation-induced pneumonitis is detected, adequate prevention of fibrosis by means of steroid treatment is recommended.
Besides the excellent tolerance of the treatment in most patients, the preliminary response rates in this study were encouraging, as 6 of 11 patients had clear evidence of progressive disease at inclusion.
Future research should attempt to elucidate various issues concerning the maximum tolerated activity and the long-term effects of the treatment on the lung tissue. Future work should also focus on the optimization of the administration protocol in terms of selectivity and the use of a fixed activity instead of estimating the optimal activity after administration of a scout dose. In addition, efforts should be made in these studies to perform SPECT tumor dosimetry. As more data on the recommended activities and treatment intervals become available, the cost-effectiveness of this treatment modality should be investigated.
CONCLUSION
A mean activity of 3.60 GBq 188Re-HDD/lipiodol was administered to 11 patients in 16 treatment sessions. A fast blood clearance of the injected activity was observed with a calculated effective half-life of 7.6 ± 2.2 h (±SD) in blood. The predominant elimination of the activity was through urinary excretion, with a mean renal clearance of 44.1% ± 11.7% of the injected activity within the 76 h after administration. The calculated whole-body effective half-life was 14.3 ± 0.9 h (±SD). Treatment was well tolerated, except in 2 patients. The results of the present phase I study are encouraging and, according to the dosimetric estimations, a further dose-escalation study is warranted.
Acknowledgments
The authors thank Dr. Boudewijn Brans for his support and the Institut des Radio-Eléments, Fleurus, Belgium) for their technical assistance. The work was supported by a grant of the Bijzonder Onderzoeksfonds (Ghent University, grant 011D9501).
Footnotes
Received Apr. 2, 2004; revision accepted Aug. 12, 2004.
For correspondence or reprints contact: Bieke Lambert, MD, Nuclear Medicine Division, Ghent University Hospital, De Pintelaan 185, 9000 Ghent, Belgium.
E-mail: Bieke.Lambert{at}Ugent.be





{kind=link}
{kind=link}
{kind=link}
{kind=link}