


Abstract
Using gated SPECT, we evaluated the relationship between admission troponin I, risk area, and myocardial salvage in patients with a first myocardial infarction treated with abciximab and primary percutaneous coronary intervention within 6 h. Methods: In 43 patients, 99mTc-sestamibi was injected before primary percutaneous coronary intervention. Gated SPECT was acquired immediately thereafter and was repeated 7 and 30 d later. The initial risk area and subsequent infarct size were expressed as a percentage of the left ventricle; salvage index was the ratio between salvaged myocardium and initial risk area; left ventricular ejection fraction was calculated using the quantitative gated SPECT software. Results: On admission, 20 patients showed elevated troponin I and had a larger risk area (P < 0.03) than did the group with normal troponin I. Infarct size at 30 d (15% ± 12% vs. 13% ± 13%) and salvage index (0.63 ± 0.27 vs. 0.60 ± 0.28) were not significantly different between the 2 groups. Ejection fraction was lower in the group with high troponin I on admission (36% ± 10% vs. 41% ± 11%, P < 0.05) and at 7 d (41% ± 11% vs. 48 ± 10, P < 0.03). At 30 d, improvement was greater in the group with high troponin I, and ejection fraction became comparable. Conclusion: Patients with high troponin I on admission have a larger initial risk area, but if they undergo primary percutaneous coronary intervention within 6 h and are treated with abciximab, myocardial salvage and functional recovery are similar to those observed in patients with normal troponin I, and no unfavorable relationship between high troponin I values on admission and myocardial salvage is registered.
Elevated plasma levels of cardiac troponin identify patients with acute coronary syndromes at high risk for subsequent cardiac events (1). Also in acute myocardial infarction treated by primary percutaneous coronary intervention, elevated troponin levels on admission are associated with a worse short- and long-term prognosis (2–4). The relationship between high troponin and negative clinical outcome remains unclear, but microvascular dysfunction may play a role (4). In infarct patients, administration of the glycoprotein IIb/IIIa inhibitor abciximab improves the rate of successful percutaneous coronary intervention after stent deployment, microvascular perfusion, left ventricular functional recovery, and clinical outcome (5–7). These benefits are more evident when abciximab administration is started before percutaneous coronary intervention (6). Therefore, one might speculate that abciximab treatment begun before percutaneous coronary intervention, by limiting microvascular damage, would be particularly helpful in infarct patients with elevated troponin on admission, according to what has been reported for patients who have acute coronary syndromes without ST elevation (8,9).
Directly visualizing the area at risk on admission and the residual perfusion defect early and late after reperfusion, and then deriving an estimate of the extent of salvaged myocardium, could be an effective method to verify this hypothesis. 99mTc-Sestamibi SPECT represents a suitable tool to assess myocardial salvage in infarct patients undergoing reperfusion therapy (10–12). Furthermore, the use of gated SPECT offers the unique opportunity to also measure ejection fraction (13,14) and, thus, assess functional recovery after primary percutaneous coronary intervention (15). The aim of this study was to use gated SPECT to examine the changes in both myocardial perfusion and ventricular function in patients treated with abciximab and primary percutaneous coronary intervention, taking into account their troponin I level on admission.
MATERIALS AND METHODS
Patient Population
Between September 2001 and June 2003, 129 consecutive patients with a first acute myocardial infarction were admitted to our emergency department and scheduled for primary percutaneous coronary intervention within 6 h of symptom onset. The diagnosis of acute myocardial infarction was based on typical chest pain lasting for >30 min and associated with >0.1 mV ST-segment elevation in at least 2 contiguous electrocardiographic leads. Because of the limited time that the nuclear medicine laboratory was available, only 46 patients could be included in the study protocol. In 3, however, clinical instability precluded transport to the nuclear medicine laboratory after percutaneous coronary intervention. Thus, the final study population included 43 patients (35 men, 8 women; mean age; 62 ± 12 y). None had heart disease other than coronary artery disease, and all were willing to participate in the study.
Study Protocol
On admission to the emergency department, all patients received aspirin (500 mg), heparin (bolus of 60 U/kg of body weight, to a maximum of 5,000 U, followed by a continuous infusion of 7 U/kg/h), clopidogrel (300 mg), and abciximab (bolus of 0.25 mg/kg of body weight, followed by a continuous infusion of 0.125 μg/kg/min, to a maximum of 10 μg/min, for 12 h). The patients were then transferred to the catheterization laboratory, where 99mTc-sestamibi (1,110 MBq) was injected. Immediately after tracer injection, the patients underwent selective coronary angiography and primary percutaneous coronary intervention. Gated SPECT was performed within 6 h of tracer injection to assess the extent and severity of the initial perfusion defect and ejection fraction. Subsequently, patients underwent baseline resting gated SPECT at 7 and 30 d of index infarction to assess changes in the extent of myocardial perfusion defect and in ejection fraction. All patients gave informed consent to participate in the study, which was approved by the Ethics Committee of our institutions.
Coronary Angiography and Mechanical Revascularization
Selective coronary angiography followed by primary percutaneous coronary intervention was performed using standard material. Two experienced angiographers reviewed the angiograms without knowledge of patient data. Coronary flow in the infarct-related artery before and after percutaneous coronary intervention was graded according to the classification of the Thrombolysis in Myocardial Infarction (TIMI) trial (16). Percutaneous coronary intervention was considered successful in the presence of TIMI grade 3 coronary flow in the treated vessel, with a residual stenosis < 20% (17).
Sample Collection and Analysis
Venous blood for troponin I analysis was collected immediately after the patient arrived in the emergency department. Cardiac troponin I was determined using an immunometric method (Dimension RxL; Dade Behring). Its lowest measurable troponin I concentration is 0.04 μg/L, and the lowest troponin I concentration that can be reproducibly measured with an interassay coefficient of variation < 10% is 0.15 μg/L (18). This latter value was the cutoff used to discriminate troponin I status.
Gated SPECT
Images were acquired using a previously described method (19). Data were processed and perfusion defect extent and ejection fraction were calculated by an automated and validated method (13,15). Initial perfusion defect (area at risk) and infarct size at 7 and 30 d were calculated; the difference between infarct size and area at risk indicated the extent of myocardial salvage. Initial perfusion defect, infarct size at follow-up, and extent of myocardial salvage were expressed as a percentage of the left ventricle. The salvage index was calculated as the ratio between myocardial salvage and area at risk (12).
Statistical Analysis
Results are expressed as mean ± SD. Comparisons within groups were made with the Wilcoxon signed rank test. Comparisons between groups were made with the Mann–Whitney U test. Proportions were compared using the Fisher exact test. Correlations were calculated using the Pearson correlation coefficient. A P value < 0.05 was considered statistically significant.
RESULTS
Baseline Clinical and Angiographic Characteristics
The study population was stratified according to troponin I level on admission: 20 patients showed elevated values (mean, 2.39 ± 2.52 μg/L; range, 0.16–7.86 μg/L), whereas 23 patients had troponin I values within the normal range (mean, 0.08 ± 0.04 μg/L; range, 0.05–0.14 μg/L). Table 1 compares the features of these 2 groups. No significant differences were observed between patients with and patients without high troponin I on admission for most baseline clinical characteristics. There was a longer delay between symptom onset and admission and between symptom onset and reperfusion therapy in the patients with high troponin I. Similarly, if the 86 patients excluded from the study because the initial gated SPECT study was not feasible were stratified according to the admission troponin I level, the intervals between symptoms, admission, and reperfusion were the only significantly different parameters (patients with high troponin I showed longer intervals).
Comparison of Clinical and Angiographic Characteristics Between Patients With and Patients Without Elevated Troponin I Level on Admission
In the patient population, the time from symptom onset to presentation correlated significantly with the admission troponin I level (r = 0.65; P < 0.0001). All patients included in the study received a coronary stent. Percutaneous coronary intervention was successful in 39 (91%) patients, whereas recanalization with postintervention TIMI flow 2 was observed in 4 patients, 3 of whom had high troponin I on admission. Table 2 compares some indicators of reperfusion effectiveness in the 2 groups and shows the absence of significant differences.
Comparison of Angiographic, Laboratory, and Electrocardiographic Indicators of Reperfusion Results Between Patients With and Patients Without Elevated Troponin I Level on Admission
Clinical Outcome
Only 1 patient with high troponin I died in the hospital before the 30-d scintigraphic evaluation. Therefore, the 30-d data of the group with high troponin I include 19 patients only. During the 30-d follow-up, no patient experienced acute coronary syndromes or underwent revascularization of the target vessel.
Gated SPECT
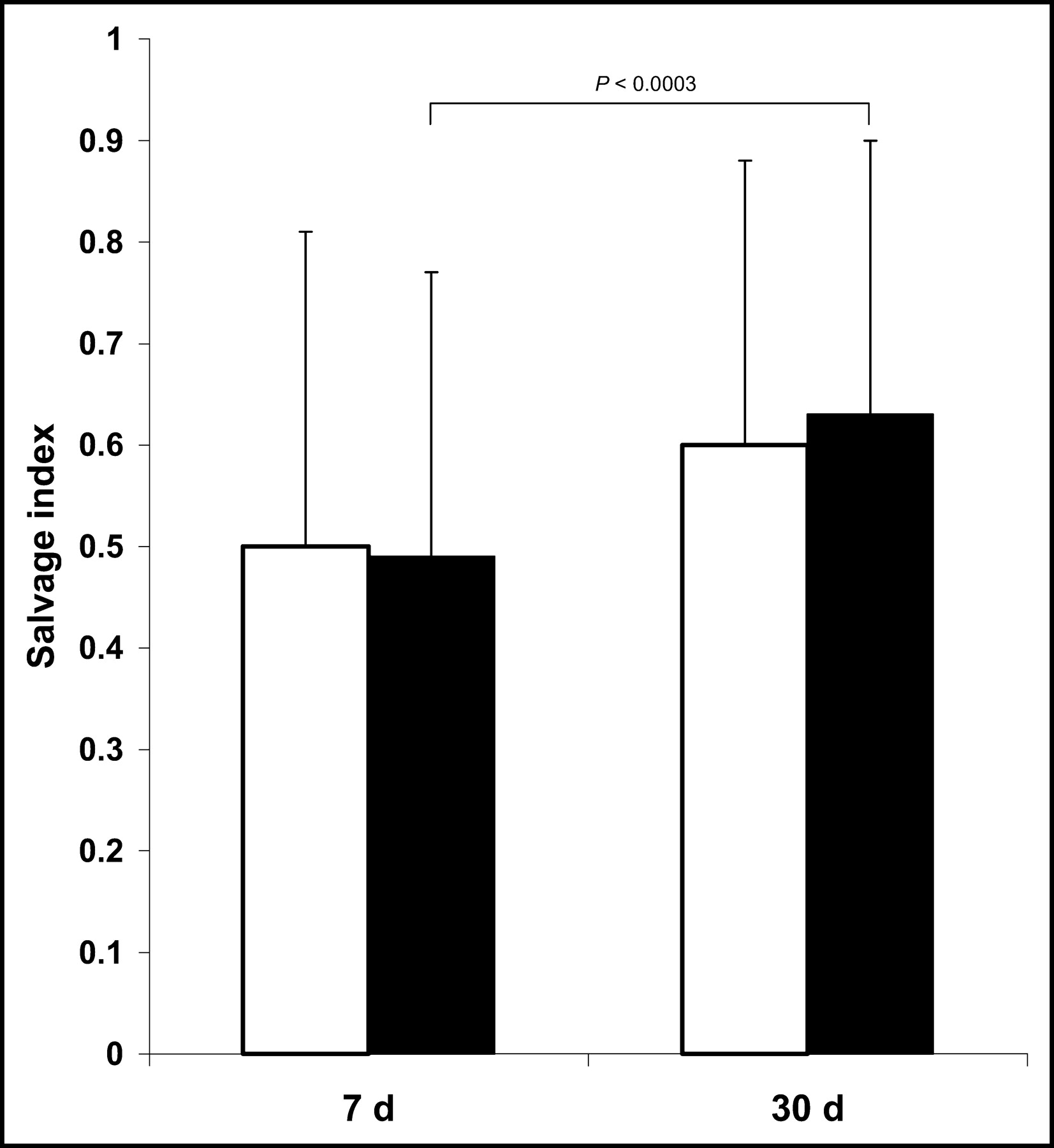
The scintigraphic findings of the entire population are reported in Table 3. The initial area at risk was larger (P < 0.03) in the group with high troponin I than in the group with normal troponin I. However, at 7 d the perfusion defects already were no longer significantly different, and at 30 d the final infarct size was similar in the 2 groups (Fig. 1). The salvage index at 7 and 30 d was not significantly different between the 2 groups (Fig. 2).

Myocardial perfusion changes in study patients. Patients with elevated troponin I level on admission are indicated by black bars; those with normal troponin I level, by white bars. LV = left ventricle.
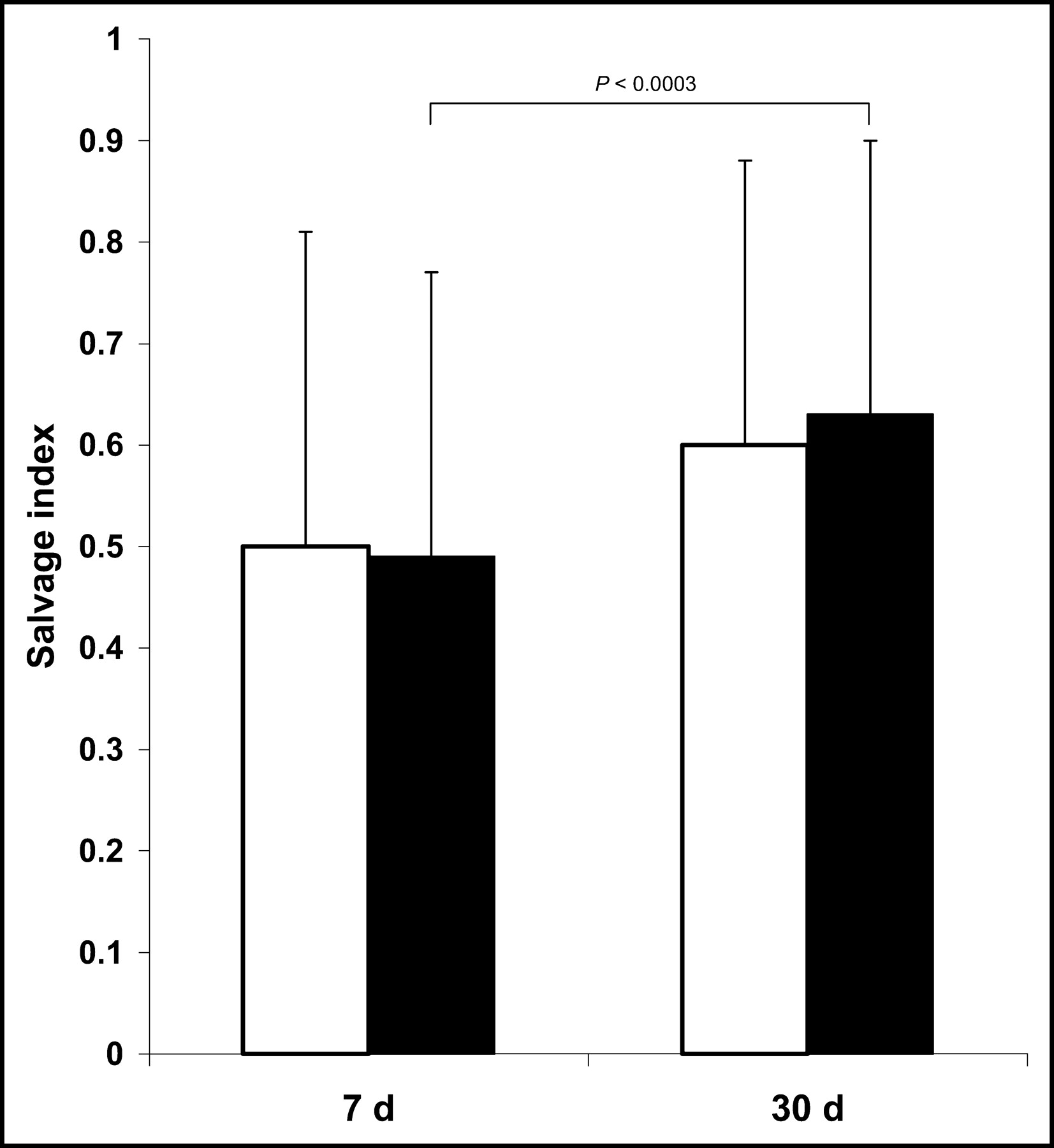
Salvage index in study patients. Patients with elevated troponin I level on admission are indicated by black bars; those with normal troponin I level, by white bars.
Comparison of Perfusion and Functional Data in Study Population Stratified by Troponin I Level on Admission
The admission ejection fraction was significantly lower in the group with high troponin I (P < 0.05). The improvement in ejection fraction at 7 d was significant in both groups, and at the 7-d evaluation, ejection fraction was still significantly lower (P < 0.03) in the group with high troponin I. Between 7 and 30 d, however, the improvement in ejection fraction was larger in the group with high troponin I, and hence ejection fraction at 30 d was similar in the 2 groups (Fig. 3).

Changes in left ventricular ejection fraction (LVEF) after primary percutaneous intervention. Patients with elevated troponin I level on admission are indicated by black bars; those with normal troponin I level, by white bars.
Taking into account the longer interval between symptoms and admission for the group with high troponin I, data on the patients of the 2 groups admitted within 3 h of symptom onset were analyzed separately. There were 11 patients with high troponin I and 21 with normal troponin I. The risk area was larger in the group with high troponin I (40% ± 13% vs. 30% ± 17%), but the difference was not significant (P = 0.09). However, the subsequent evolution of the perfusion defect led to an equal extent at 30 d, with the same salvage index (0.66 ± 0.29 vs. 0.61 ± 0.27). Similarly, the left ventricular ejection fraction, which was slightly lower in the group with high troponin I on admission (38% ± 10% vs. 41% ± 11%), reached the same value at 30 d (52% ± 12% vs. 50% ± 11%).
Because the left anterior descending artery showed a higher likelihood of being the infarct-related artery in the group with high troponin I, we also performed a separate analysis excluding patients with involvement of the left anterior descending artery. The initial risk area was larger in the 8 patients with high troponin I than in the 16 with normal troponin I (32% ± 11% vs. 22% ± 9%, P = 0.065); however, the salvage index (0.57 ± 0.30 vs. 0.65 ± 0.28) and the left ventricular ejection fraction (56% ± 8% vs. 52% ± 7%) at 30 d were similar in the 2 groups.
DISCUSSION
Recent studies have shown that among patients with acute myocardial infarction undergoing primary percutaneous coronary intervention, an elevated troponin level on admission identified a subgroup at higher risk for in-hospital and long-term cardiac events (2–4). A lower success rate of primary percutaneous coronary intervention, the presence of microvascular dysfunction that limits myocardial salvage, and a higher incidence of malignant reperfusion arrhythmias have been proposed as possible mechanisms of the worse outcome in patients with an elevated troponin level on admission (2,4,20).
In our study, suboptimal epicardial flow (TIMI flow < 3) after percutaneous coronary intervention was more frequently observed in the group with high troponin I, in agreement with previous studies that showed elevated troponin levels on admission to be an independent predictor of a lower success rate for primary percutaneous coronary intervention (2,4). In these studies, failure to achieve optimal reperfusion was associated with a worse outcome. However, this was not the only mechanism to explain the relationship between high troponin and adverse clinical outcome, because troponin I elevation remained an independent predictor of cardiac events also in patients undergoing successful percutaneous coronary intervention (2).
Microvascular dysfunction that compromised myocardial perfusion despite normal epicardial flow after percutaneous coronary intervention might be another involved mechanism. Giannitsis et al. showed that, despite TIMI 3 flow after revascularization, infarct patients with an elevated troponin level on admission had more severely impaired myocardial perfusion as indicated by serum marker release kinetics and resolution of ST-segment elevation (4). The microvascular dysfunction that impairs myocardial perfusion, however, could be suspected to limit myocardial salvage as well. Thus, pharmacologic interventions able to reduce the extent of microvascular damage could be particularly useful in these patients. In our study, we examined a patient population who received coronary stents and the glycoprotein IIb/IIIa antagonist abciximab before percutaneous coronary intervention to improve epicardial and microvascular flow (5–7). Glycoprotein IIb/IIIa inhibitors have been demonstrated to be more effective in patients with non-ST elevation acute coronary syndromes and elevated troponin levels than in those with normal troponin levels (8,9). We did not find a significant difference in salvage index at 7 and 30 d between the patient groups stratified according to troponin I level on admission. Because the group with high troponin I had a larger area at risk, the extent of myocardial salvage was even greater than that observed in the group with normal troponin I. Consequently, in our study, an elevated troponin I level was not associated with impaired tissue reperfusion. These results support the hypothesis that the use of coronary stenting and administration of abciximab before percutaneous coronary intervention prevent the unfavorable relationship between elevated troponin I on admission and myocardial salvage. Indeed, the different results observed by Giannitsis et al. might be explained by their having placed coronary stents in 75% of patients and given abciximab to just a minority (35%) of patients—those with suboptimal angiographic results and compromised epicardial flow after percutaneous coronary intervention (4). Conversely, data in agreement with ours have recently been reported for patients with elevated C-reactive protein level on admission (21).
The use of gated SPECT to assess left ventricular function from perfusion data is a novel contribution of this study. The evaluation of risk area and final infarct size is accepted as a reliable surrogate endpoint for studies about therapeutic options for acute myocardial infarction (22). On the other hand, the prognostic implications of left ventricular ejection fraction after acute myocardial infarction are well known (23). Therefore, the advantages offered by gated SPECT over the traditional nongated technique could be particularly important for studies comparing different treatment strategies for acute myocardial infarction, because in this setting a reproducible assessment of both perfusion and functional changes is mandatory (10–12,24–26). To our knowledge, this was the first study to show that the value of repeated perfusion imaging in acute myocardial infarction can be increased by adding repeated measurements of left ventricular ejection fraction. However, this approach has limitations for the evaluation of left ventricular function. Although an inverse relationship between infarct size and left ventricular ejection fraction has been demonstrated, no data are available directly comparing the 2 parameters on the basis of a single gated SPECT study. One must also consider that the first ejection fraction was measured after revascularization and that, therefore, the presence of some degree of very early improvement was possible although quite unlikely because of myocardial stunning (10).
Other limitations of the present study must be considered. Because of the small number of patients, confounding effects from the longer reperfusion delay and higher incidence of anterior infarctions in the high troponin I group cannot be excluded with certainty. As for the interval between symptom onset and reperfusion, however, the finding of equally effective myocardial salvage in the group with high troponin I is confirmed when the analysis is restricted to patients admitted within 3 h. The observation that the left anterior descending artery had a higher likelihood of being the infarct-related artery in patients with high troponin I is consistent with previous reports (2,4,27). In our series, however, the location of the culprit lesion apparently did not influence the effectiveness of reperfusion, as confirmed by the finding that patients without involvement of the left anterior descending artery showed a similar salvage index and ejection fraction at 30 d independently of the presence or absence of high troponin I at admission. The microvascular dysfunction in patients with high troponin I was previously demonstrated (4), but because abciximab treatment was not randomized in our series, we have no data about the potential consequences of high troponin I levels on subsequent myocardial salvage in the absence of abciximab administration. Because of the small number of patients in the population and the shortness of the follow-up, we could not establish whether the absence of differences in myocardial salvage in patients with and patients without high troponin I also implies a similar prognosis. However, the direct demonstration of myocardial salvage is a widely accepted endpoint for testing the effectiveness of treatment in patients with acute myocardial infarction (22), and the finding of preserved left ventricular function reinforces its positive prognostic implications. Because we selected patients treated with primary percutaneous coronary intervention early (<6 h) after symptom onset, the results of our study might not be valid in patients whose revascularization was more delayed or who underwent other types of reperfusion therapy. However, the time independence of treatment effectiveness in primary percutaneous coronary intervention has recently been reported (28).
CONCLUSION
An elevated troponin I level on admission identifies a high-risk subgroup of patients with acute myocardial infarction. Microvascular dysfunction limiting myocardial salvage has been proposed as one of the possible mechanisms that link a high troponin I level on admission to a worse outcome. According to our results, patients with high troponin I levels on admission have larger initial risk areas than do other infarct patients. However, for our patients to whom administration of abciximab started before percutaneous coronary intervention, myocardial salvage was equally effective both in those with and those without elevated troponin I levels, so that the suspected unfavorable relationship between elevated troponin I level and myocardial salvage was not registered.
Footnotes
Received Oct. 17, 2003; revision accepted Dec. 29, 2003.
For correspondence or reprints contact: Roberto Sciagrà, MD, Nuclear Medicine Unit, Department of Clinical Physiopathology, University of Florence, Viale Morgagni 85, 50134 Florence, Italy.
E-mail: r.sciagra{at}dfc.unifi.it





{kind=link}
{kind=link}
{kind=link}