


Abstract
Myocardial salvage assessed by 99mTc-sestamibi scintigraphy is a marker of myocardial tissue reperfusion in patients with acute myocardial infarction. The prognostic value of myocardial salvage index in patients with acute myocardial infarction after reperfusion therapy has not, however, been investigated. Methods: We analyzed 765 patients with acute myocardial infarction randomized to treatment by coronary stenting (383 patients), primary coronary angioplasty (251 patients), or thrombolysis (131 patients) in the setting of 3 randomized trials. Initial (before reperfusion therapy) and follow-up (7–14 d after reperfusion therapy) scintigraphic examinations were performed to assess the initial perfusion defect, final infarct size, and salvage index. Patients were categorized into 2 groups defined by the median salvage index (0.5): the group with salvage index < 0.5 (374 patients) and the group with salvage index ≥ 0.5 (391 patients). The primary endpoint of the study was mortality at 6 mo after the index event. Results: Six-month mortality was 5.1% (19 deaths) in the group with salvage index < 0.5, compared with 1.0% (4 deaths) in the group with salvage index ≥ 0.5 (odds ratio, 5.1; 95% confidence interval, 1.9–13.3; P = 0.001). Salvage index (median [25th, 75th percentiles] was significantly smaller in nonsurvivors than in survivors (0.19 [0.05, 0.37] vs. 0.50 [0.26, 0.80], P = 0.0004). The Cox proportional hazards model showed that myocardial salvage index (P = 0.0007), initial perfusion defect (P = 0.0007), and age (P = 0.04) were independently associated with 6-mo mortality. Conclusion: Myocardial salvage achieved by reperfusion therapy predicts mortality in patients with acute myocardial infarction. Our findings support the use of salvage index as a surrogate of mortality in clinical trials designed to test the efficacy of reperfusion therapies among patients with acute myocardial infarction.
Reperfusion therapy for acute myocardial infarction has been shown to reduce mortality (1–3). Because the primary objective of reperfusion therapy is complete and sustained reperfusion of the jeopardized myocardium rather than simple restoration of epicardial blood flow, a clinical tool that assesses reperfusion efficacy in terms of the amount of myocardial salvage is of paramount clinical importance. Mortality is the strongest clinical outcome measure of the efficacy of various reperfusion strategies in patients with acute myocardial infarction (4). However, demonstration of superiority or noninferiority of any new reperfusion therapy using mortality as an endpoint requires large numbers of patients. Indeed, earlier trials of reperfusion therapy in patients with acute myocardial infarction have included large numbers of patients (1–3). Testing a new therapy of still unknown efficacy and safety in large numbers of patients is impractical. Thus, markers that can be used as a surrogate for mortality in trials assessing the efficacy of novel reperfusion therapies are badly needed (5). A candidate marker has to correlate closely with the amount of myocardium salvaged by reperfusion therapy and be a predictor of mortality.
Myocardial salvage is the principal mechanism by which patients with acute myocardial infarction benefit from reperfusion therapies (6). It can reliably be quantified by 99mTc-sestamibi imaging (4). Repeated myocardial imaging with 99mTc-sestamibi performed early after symptom onset and days after primary reperfusion treatment allows reliable assessment of the area at risk, final infarct size, and salvage index or the proportion of area at risk that is salvaged by reperfusion therapy (4,7,8). However, no information is available on the prognostic value of myocardial salvage in patients with acute myocardial infarction treated with reperfusion therapy.
We undertook this study to investigate the value of myocardial salvage as a predictor of mortality in patients with acute myocardial infarction treated with currently available reperfusion therapies.
MATERIALS AND METHODS
Study Population
Eligible for this study were 913 patients with acute myocardial infarction who were randomized to treatment with coronary stenting, primary percutaneous coronary angioplasty, or thrombolysis, in the framework of 3 randomized trials: Stent Versus Thrombolysis for Occluded Coronary Arteries in Patients with Acute Myocardial Infarction (STOPAMI) trials 1 and 2 (7,8) and Stent or PTCA for Occluded Coronary Arteries in Patients with Acute Myocardial Infarction Ineligible for Thrombolysis (STOPAMI 3) (9). The diagnosis of acute myocardial infarction was based on the presence of chest pain lasting at least 20 min associated with typical electrocardiographic changes (ST-segment elevation of at least 0.1 mV in 2 or more extremity leads, ST-segment elevation of at least 0.2 mV in 2 or more contiguous precordial leads, or left bundle branch block of new onset) or elevation of creatine kinase activity in the serum by at least twice the upper normal limit. Exclusion criteria were onset of symptoms > 48 h before admission, stroke (within the previous 3 mo), active bleeding or bleeding diathesis, trauma or major surgery (within the last month), suspected aortic dissection, oral anticoagulation with coumarin derivatives, severe uncontrolled arterial hypertension (systolic value > 180 mm Hg), and noncompressible vascular puncture sites. The study protocols of the 3 randomized trials from which the patients came were approved by the institutional ethics committee. All patients gave written consent before recruitment in the studies.
Study Protocol and Treatment Assignment
Detailed information about the randomly assigned treatment has been published previously (7–9). Briefly, before assignment to therapy, all patients received aspirin (500 mg) and intravenous heparin (60 mg/kg of body weight, to a maximum of 5,000 U). In total, 457 patients were assigned to treatment with coronary stenting, 306 patients were assigned to treatment with percutaneous transluminal coronary angioplasty (PTCA), and 150 patients were assigned to treatment with thrombolysis. Coronary stent placement and primary percutaneous coronary angioplasty were performed as previously described (7). In the group with thrombolysis, alteplase (Actilyse; Boehringer Ingelheim) was used as a full-dose therapy in 69 patients or as a half-dose therapy plus abciximab in 81 patients. In all patients treated with stenting or PTCA, in the absence of contraindications, abciximab (ReoPro; Lilly Deutschland GmbH) was used as an adjunct therapy. Abciximab was used as a bolus of 0.25 mg/kg of body weight followed by a continuous infusion of 0.125 μg/kg/min for 12 h.
In the groups with stenting and PTCA, coronary angiography was performed before and at the end of the procedure. Digital angiograms were analyzed offline in the angiographic core laboratory with an automated edge-detection system (CMS; Medis Medical Imaging Systems).
99mTc-Sestamibi SPECT
Before initiation of the assigned therapy, patients received an intravenous injection of 1,000 MBq (27 mCi) of 99mTc-sestamibi. Single-photon emission CT was performed within 6–8 h after injection of the radioactive agent. Follow-up 99mTc-sestamibi imaging was performed 7–14 d after the reperfusion therapy. Initial perfusion defect (area at risk) and final infarct size were determined according to previously described methods (7,8). All measurements were performed in the scintigraphic core laboratory by investigators unaware of the type of therapy received. Paired 99mTc-sestamibi imaging enabled calculation of 3 parameters: initial perfusion defect and final infarct size (perfusion defects in the initial and follow-up 99mTc-sestamibi imaging), both expressed as percentage of the left ventricle, and myocardial salvage index (initial perfusion defect minus final infarct size divided by the initial perfusion defect), which represents the proportion of the initial perfusion defect that was salvaged by reperfusion therapy or a myocardial salvage parameter that is normalized for the initial perfusion defect.
Paired 99mTc-sestamibi imaging could not be performed on 148 of the 913 patients (74 patients in the group with stenting, 55 patients in the group with PTCA, and 19 patients in the group with thrombolysis). The remaining 765 patients (84%) with paired 99mTc-sestamibi imaging (383 patients in the group with stenting, 251 patients in the group with PTCA, and 131 patients in the group with thrombolysis) represent the patient population of this study.
Definitions and Follow-up Protocol
The median of salvage index for the whole study population was 0.50. Patients were divided into 2 groups: the group with salvage index < 0.5 and the group with salvage index ≥ 0.5. The primary endpoint of the study was mortality at 6 mo after the index event.
After discharge, the patients were followed up clinically by phone interview at 1 mo and by an office visit at 6 mo after the acute event. Furthermore, patients were advised to contact our outpatient clinic or their referring physicians if chest pain or other cardiac symptoms arose.
Statistical Analysis
Data are presented as median (25th, 75th percentiles), counts, or proportions (percentages). Categoric data were compared by the χ2 or Fisher exact test whenever an expected cell value was <5. Continuous data were compared with the Wilcoxon rank sum test. Survival was analyzed by the Kaplan–Meier method. Differences in survival were assessed with the log-rank test. We used the Cox proportional hazards model to assess the independent impact of myocardial salvage index on mortality while adjusting for other potentially confounding variables. All analyses were performed using the S-PLUS software package (Insightful Corp.). A P value < 0.05 was considered statistically significant.
RESULTS
Patient Characteristics
The initial perfusion defect and the salvage index (median [25th, 75th] percentiles) for the entire study population were 24.0% (13.7, 40.2) of the left ventricle and 0.50 (0.25, 0.79), respectively. No correlation between the initial perfusion defect and salvage index was found (r = 0.009; P = 0.80). Baseline characteristics of the patients are shown in Table 1. There were several differences between the groups. Patients with myocardial salvage index ≥ 0.5 had a greater proportion of women, less often had a history of myocardial infarction, and had smaller initial perfusion defects than did patients with salvage index < 0.5. In addition, PTCA and stenting were used more often in patients with myocardial salvage index ≥ 0.5 than in patients with salvage index < 0.5.
Differences Between Groups of Patients Defined by Salvage Index
In the group of patients with myocardial salvage index ≥ 0.5, the values (median [25th, 75th percentiles]) of final infarct size, absolute salvage (both expressed as percentage of the left ventricle), and myocardial salvage index were 4.0% (0.3, 8.5), 16.5% (8.7, 27.0), and 0.78 (0.63, 1.0), respectively. In the group of patients with myocardial salvage index < 0.5, the values of final infarct size, absolute salvage, and myocardial salvage index were 22.0% (12.0, 33.5), 6.0% (1.1, 12.0), and 0.25 (0.06, 0.35), respectively. Peak values of creatine kinase activity (upper limit of normal = 80 U/L) were 814.5 U/L (352.8; 1480.8) in the group with salvage index < 0.5 and 513 U/L (293.5; 856.0) in the group with salvage index ≥ 0.5 (P < 0.001).
Clinical Outcome
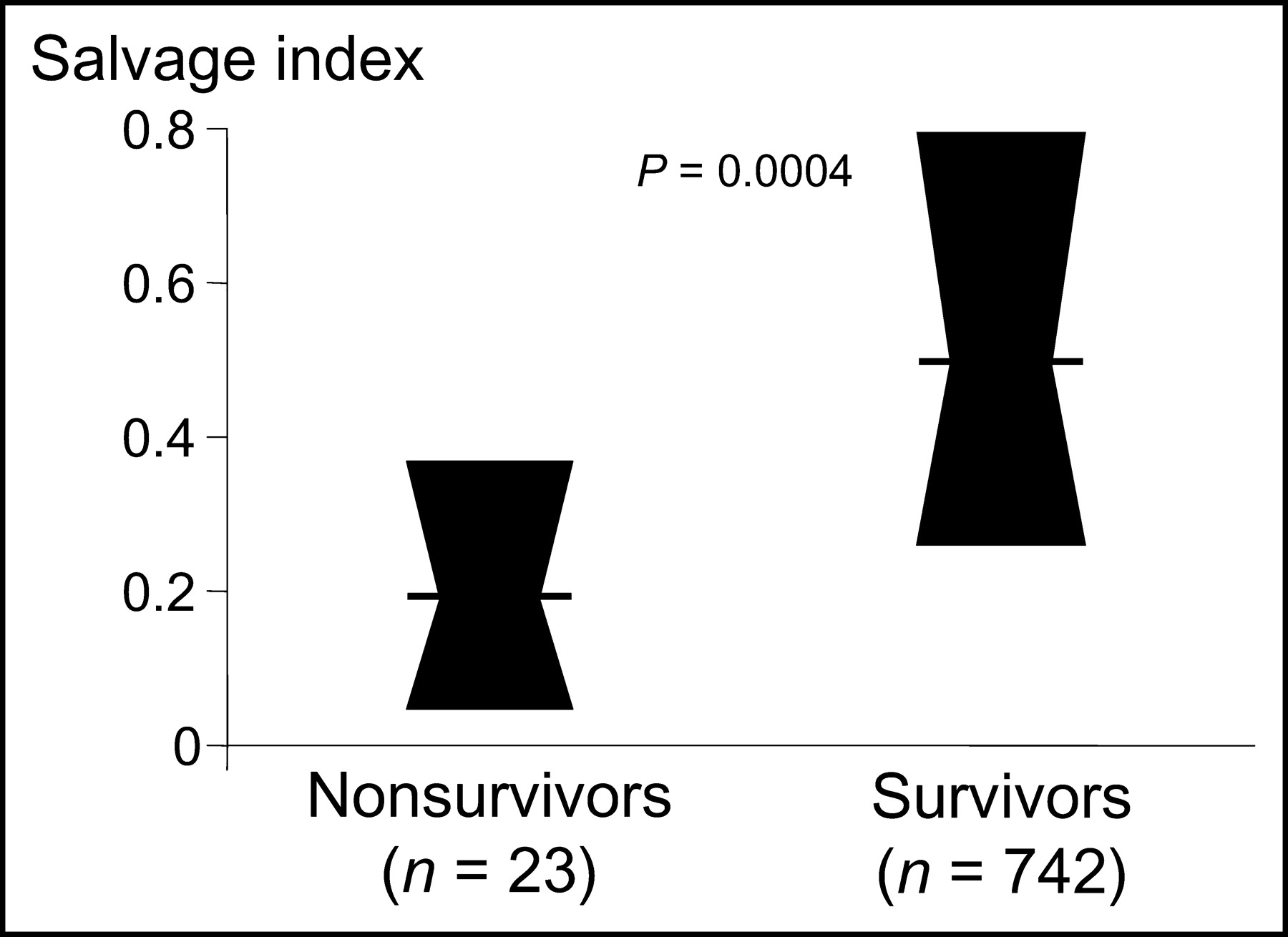
During the 30 d after acute myocardial infarction, 4 deaths (1.1%) occurred in the group of patients with myocardial salvage index < 0.5 but none in the group of patients with myocardial salvage index ≥ 0.5 (P = 0.11). At 6 mo after the acute myocardial infarction, the differences in mortality between the 2 groups were further increased. Thus, at 6 mo, 19 deaths (5.1%) had occurred in the group of patients with myocardial salvage index < 0.5, compared with 4 deaths (1.0%) in the group of patients with myocardial salvage index ≥ 0.5 (odds ratio, 5.1; 95% confidence interval, 1.9–13.3; P = 0.001). Survival curves are shown in Figure 1. In the 23 patients who died during follow-up, salvage index was 0.19 (0.05, 0.37), which was significantly smaller than the salvage index of 0.50 (0.26, 0.80) in the 742 patients who survived the 6-mo follow-up (P = 0.0004; Fig. 2). In addition, if the absolute value of myocardial salvage (percentage of the left ventricle) is analyzed without normalization for initial perfusion defect, nonsurviving patients had a myocardial salvage of 6.7% (1.0, 15.8), compared with 11.0% (4.7, 20.0) for surviving patients (P = 0.08).

Survival curves of the 2 groups of patients defined by salvage index.

Box plot presentation of salvage index values in patients who died (nonsurvivors) and those who survived the 6-mo follow-up (survivors). Values are presented as median (horizontal lines) and interquartile range.
We adjusted for differences in baseline characteristics between the 2 groups of patients by using the multivariate Cox proportional hazards model. In this model, we included age, sex, previous myocardial infarction, initial perfusion defect, type of reperfusion therapy (thrombolysis or mechanical reperfusion), and salvage index as independent variables and mortality at 6 mo as a dependent variable. The c index of discrimination of the multivariate model was 0.80 (a c value of 0.5 indicates random prediction, whereas a c value of 1.0 indicates a perfectly discriminating model). The model showed that salvage index (χ2 = 11.4; P = 0.0007), initial perfusion defect (χ2 = 11.4; P = 0.0007), and age (χ2 = 4.1; P = 0.04) were independently associated with 6-mo mortality.
DISCUSSION
It has recently been demonstrated that 99mTc-sestamibi SPECT is the best available tool for infarct size measurement in clinical medicine (4). Indeed, numerous experimental and clinical studies have demonstrated the validity of 99mTc-sestamibi myocardial imaging for determination of infarct size (10–15) and fibrosis in myocardium (16). In other studies, 99mTc-sestamibi infarct size has been shown to be a predictor of subsequent mortality (17–19). In a series of 274 patients with acute myocardial infarction, Miller et al. (17) found that sestamibi infarct size was strongly associated with 2-y mortality. In a recent multicenter study from the same group comprising a series of 249 patients with acute myocardial infarction, a strong association between 99mTc-sestamibi infarct size at hospital discharge and 1-y mortality was reported (18). With respect to 6-mo mortality, a similar finding has recently been published by Burns et al. (19) for a series of 1,164 patients with acute myocardial infarction treated with thrombolysis. Although infarct size is an important predictor of subsequent mortality after acute myocardial infarction, and its reduction is the main objective of reperfusion therapy, it cannot be used to reliably assess the efficacy of reperfusion therapy. Final infarct size depends on multiple factors such as extent of area at risk, collateral blood flow, duration of myocardial ischemia, and metabolic demand (20,21). In these carefully conducted experimental and clinical studies, determinants of infarct size have only partially been accounted for (20,21). Paired 99mTc-sestamibi studies, before and after the application of reperfusion therapy, allow reliable estimation of area at risk and final infarct size and, consequently, of myocardial salvage normalized for initial perfusion defect (salvage index).
To our knowledge, this was the first study to demonstrate the prognostic value of myocardial salvage index in a large series of patients with acute myocardial infarction treated with thrombolytic or mechanical reperfusion therapy. In the multivariate analysis, we found that myocardial salvage index was the strongest predictor of 6-mo mortality, followed by initial perfusion defect (area at risk) and age. In line with the findings of Miller et al. (17), if the degree of myocardial salvage is not normalized for initial perfusion defect, this parameter is not significantly different between patients who died and those who survived the follow-up period.
Previous studies have proven the value of salvage index as a predictor of successful myocardial reperfusion and a marker of myocardial tissue reperfusion in patients with acute myocardial infarction (22–25). Milavetz et al. have shown that in patients with acute myocardial infarction, successful reperfusion therapy within 2 h from symptom onset is associated with the highest values of salvage index (22). In the study of Laster et al. (23), restoration of Thrombolysis in Myocardial Infarction (TIMI) grade 3 flow was necessary for optimal myocardial salvage. In patients with TIMI grade 3 flow, salvage index was significantly greater than in patients with TIMI grade 2 flow (23). In the STOPAMI trials 1 and 2, salvage index was a sensitive tool to evaluate the efficacy of different interventional and thrombolytic reperfusion therapies in patients with acute myocardial infarction (7,8). Salvage index closely correlated with TIMI myocardial perfusion grade (24) and with resolution of ST-segment elevation on electrocardiography (25), both of which are considered markers of myocardial tissue reperfusion. In a recent study from our group, salvage index was used to uncover the mechanisms responsible for the different time dependence of the efficacy of interventional and thrombolytic reperfusion therapies in patients with acute myocardial infarction (26). The present study added a new dimension to the value of salvage index, that is, that it may serve as a predictor of mortality in patients with acute myocardial infarction after reperfusion therapy.
The study had some limitations. The series of patients with acute myocardial infarction that we included was unselected in terms of both presentation (with or without ST-segment elevation) and reperfusion therapy (thrombolysis, primary coronary angioplasty, or stenting). Although this may be considered a strength of the study, the availability of some parameters depended on the protocols of the studies in which the patients were originally enrolled. Thus, some parameters such as TIMI flow grade or angiographic left ventricular ejection fraction and dimensions were not available in the group treated with thrombolysis. Furthermore, other indexes such as severity of heart failure, or the need for implantable cardioverter defibrillators, were not in the original protocols and thus could not be assessed in this study. Another limitation resided in the low number of events (deaths), which did not allow a comprehensive analysis of all potential prognostic factors after acute myocardial infarction.
CONCLUSION
This study clearly demonstrated that salvage index predicts mortality in patients with acute myocardial infarction after reperfusion therapy. Our results support the use of salvage index as a surrogate for mortality in clinical trials designed to test the efficacy of reperfusion therapies among patients with acute myocardial infarction.
Footnotes
Received Oct. 14, 2003; revision accepted Dec. 12, 2003.
For correspondence or reprints contact: Adnan Kastrati, MD, Deutsches Herzzentrum, Lazarettstrasse 36, 80636 Munich, Germany.
E-mail: kastrati{at}dhm.mhn.de
REFERENCES
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Myocardial Edema on T2-Weighted MRI: New Marker of Ischemia Reperfusion Injury and Adverse Myocardial Remodeling
- Remote ischaemic conditioning and healthcare system delay in patients with ST-segment elevation myocardial infarction
- Intravenous {beta}-Blockers in Primary Percutaneous Coronary Intervention: New Hope for an Old Therapy
- The Assessment of Area at Risk and Myocardial Salvage After Coronary Revascularization in Acute Myocardial Infarction: Comparison Between CMR and SPECT
- Effect of Iron Chelation on Myocardial Infarct Size and Oxidative Stress in ST-Elevation-Myocardial Infarction
- Long-term prognostic value of myocardial salvage assessed by cardiovascular magnetic resonance in acute reperfused myocardial infarction
- Myocardium at Risk in ST-Segment Elevation Myocardial Infarction: Comparison of T2-Weighted Edema Imaging With the MR-Assessed Endocardial Surface Area and Validation Against Angiographic Scoring
- Growth-differentiation factor 15 as predictor of mortality in acute reperfused ST-elevation myocardial infarction: insights from cardiovascular magnetic resonance
- Prognostic Significance and Determinants of Myocardial Salvage Assessed by Cardiovascular Magnetic Resonance in Acute Reperfused Myocardial Infarction
- 5-Year Prognostic Value of No-Reflow Phenomenon After Percutaneous Coronary Intervention in Patients With Acute Myocardial Infarction
- Predictive Factors and Impact of No Reflow After Primary Percutaneous Coronary Intervention in Patients With Acute Myocardial Infarction
- Myocardial Salvage by CMR Correlates With LV Remodeling and Early ST-Segment Resolution in Acute Myocardial Infarction
- Impact of Myocardial Salvage Assessed by 99mTc-Sestamibi Scintigraphy on Cardiac Autonomic Function in Patients Undergoing Mechanical Reperfusion Therapy for Acute Myocardial Infarction
- Evolution of Left Ventricular Ejection Fraction and its Relationship to Infarct Size After Acute Myocardial Infarction
- Diagnostic Value of Contrast-Enhanced Magnetic Resonance Imaging and Single-Photon Emission Computed Tomography for Detection of Myocardial Necrosis Early After Acute Myocardial Infarction
- The Impact of the Capability of Circulating Progenitor Cell to Differentiate on Myocardial Salvage in Patients With Primary Acute Myocardial Infarction
- Impact of Unrecognized Myocardial Scar Detected by Cardiac Magnetic Resonance Imaging on Event-Free Survival in Patients Presenting With Signs or Symptoms of Coronary Artery Disease
- Myocardial Salvage: Retrospection, Resolution, and Radio Waves
- Gated SPECT Evaluation of Outcome After Abciximab-Supported Primary Infarct Artery Stenting for Acute Myocardial Infarction: The Scintigraphic Data of the Abciximab and Carbostent Evaluation (ACE) Randomized Trial