


Abstract
A single, low dose of recombinant human thyroid-stimulating hormone (rhTSH) doubles 24-h RAIU and causes a more homogeneous distribution of radioiodine on thyroid scintigrams of patients with nodular goiter. Pretreatment with rhTSH allows the therapeutic dose of 131I to be reduced by 50%–60% without compromising the result of thyroid volume reduction. The present study focused on the dosimetric aspects of therapy with a reduced dose of 131I after pretreatment with rhTSH in patients with nodular goiter. Methods: Thirty-six patients were treated with 131I to reduce thyroid volume. Nine patients were pretreated with a single dose of 0.01 mg of rhTSH, and 9 patients, with 0.03 mg of rhTSH. Two control groups of 9 patients, matched for thyroid weight and 24-h radioactive iodide uptake, were not pretreated with rhTSH. The therapeutic dose of 131I was aimed at being sufficient to result in retention of 3.7 MBq of 131I per gram of thyroid tissue at 24 h. Thyroid radioactivity after 131I administration was measured every 24 h for 3 d and on days 7, 10, 14, 21, and 28. A model of iodine biokinetics was used to estimate absorbed doses in organs. Protein-bound 131I activity was measured at 1, 2, 3, 7, and 10 d and at 2, 3, and 4 wk after 131I therapy. Results: The administered activities were 1.5 times lower in the 0.01-mg rhTSH group and 1.9 times lower in the 0.03-mg rhTSH group than in the control groups. The absorbed dose in the thyroid was similar in the rhTSH-pretreated groups and in the control groups. In the organs of excretion (bladder) and uptake (stomach) of inorganic iodide, the absorbed doses were 2- to 3-fold lower in the pretreated groups than in the control groups. The effective dose equivalent outside the thyroid was considerably lower in the rhTSH-pretreated groups than in their respective control groups (1.6-fold in the 0.01-mg rhTSH group and 2.3-fold in the 0.03-mg rhTSH group). The time course of protein-bound 131I activity in serum and the cumulated protein-bound 131I activity in serum did not differ significantly between rhTSH-pretreated and control groups. Conclusion: 131I therapy after pretreatment with a single, low dose of rhTSH, with the dose reduced according to the rhTSH-induced increase in 24-h radioactive iodide uptake, caused lower radiation-absorbed doses in extrathyroidal organs and tissues, especially bladder and stomach, and no significant increase in the release of 131I-labeled thyroid hormones into the circulation of patients with nodular goiter. Thus, this mode of therapy can be recommended, especially when the dose of radioiodine to be administered without rhTSH pretreatment is high.
Radioiodine (131I) therapy is effective for reduction of thyroid volume in patients with nontoxic, nodular goiter. Several studies have found that 131I treatment decreased goiter size by approximately 40% after 1 y (1–7) and by 50%–60% after 3–5 y (2,8,9).
In the reported studies, a single dose of approximately 3.7 MBq (100 μCi) of 131I per gram of thyroid tissue, corrected for thyroid radioactive iodide uptake (RAIU) at 24 h, was given. In patients with nontoxic, nodular goiter, RAIU is usually rather low. As a result, high doses of 131I are often needed, causing a relatively high radiation burden to extrathyroidal tissues (10). Therefore, exploration of strategies to enhance RAIU in these patients would be of interest. A method to enhance RAIU in patients with nodular goiter is to increase the serum level of thyroid-stimulating hormone, which is often low normal or below normal.
In 2000, we reported that pretreatment with 0.01 or 0.03 mg of recombinant human thyroid-stimulating hormone (rhTSH) doubled 24-h RAIU in patients with nodular goiter (11). We also found that pretreatment with rhTSH caused a more homogeneous distribution of radioiodine on thyroid scintigrams of nodular goiters (12). Pretreatment with a single, low dose of rhTSH allowed us to reduce the therapeutic dose of radioiodine in patients with nodular goiter by 50%−60% without compromising the result of thyroid volume reduction (13).
The present study focused on the dosimetric aspects of therapy with a reduced dose of radioiodine after rhTSH pretreatment of patients with nodular goiter. We hypothesized that therapy with a reduced dose of 131I after pretreatment with rhTSH would decrease the radiation burden to extrathyroidal tissues. Absorbed doses in the thyroid and in extrathyroidal organs and tissues were estimated for patients treated with radioiodine with and without rhTSH pretreatment, using thyroid radioactivity measurements and a model of iodine kinetics in the body as described by Robertson and Gorman (14).
Furthermore, we investigated whether pretreatment with rhTSH increased the release of 131I-labeled thyroid hormones or thyroglobulin into the circulation after radioiodine therapy. If this were the case, the advantage of lowering the amount of free inorganic 131I in the circulation by using lower therapeutic doses of 131I after rhTSH pretreatment might be outweighed by an increase in circulating protein-bound 131I levels (PB131I).
MATERIALS AND METHODS
Patients
Thirty-six patients with nodular goiter, who were referred for radioiodine therapy to reduce thyroid volume, participated in this study. All patients had normal serum levels of free thyroxine (9.0–22.3 pmol/L) and total triiodothyronine (1.0–3.0 nmol/L). Serum thyroid-stimulating hormone levels were normal (0.2–5.5 mU/L) in 24 patients and below normal in 12 patients. The results of careful palpation of the thyroid, followed by fine-needle aspiration biopsy of dominant nodules and of those that had a different consistency from other nodules within the gland gave no suggestion of thyroid malignancy in any of the patients. None of the patients had recently taken medication known to affect thyroid function or RAIU. Patients had not received iodine-containing agents in the last 6 mo. An electrocardiogram, complete blood count, liver enzyme determination, plasma creatinine and glucose measurement, and screening urinalysis did not show abnormalities in any patients.
Twenty-four hours before radioiodine therapy, a first group of 9 consecutive patients received 0.01 mg of rhTSH and a second group of 9 consecutive patients received 0.03 mg of rhTSH. Afterward, 18 consecutive patients were treated with radioiodine without rhTSH pretreatment; from these, 2 control groups of 9 patients each were selected, matching the rhTSH-pretreated groups with respect to thyroid weight and 24-h RAIU.
The institutional human research committee approved the study, and all patients gave written informed consent to participate.
Diagnostic Investigations Preceding Radioiodine Therapy
A diagnostic dose of 40 MBq of sodium (123I) iodide was administered as an oral solution. RAIU, as a percentage of the administered dose of 123I corrected for physical decay, was measured at 24 h using a 7.62 × 7.62 cm (3 × 3 in.) NaI (Tl) detector. Dead-time corrections were made using standard software. Thyroid scintigraphy in the 159-keV window of 123I was performed 24 h after radioiodine administration. All thyroid scintigrams showed heterogeneous uptake.
In 18 patients, the influence of rhTSH on RAIU was investigated at least 2 wk after radioiodine administration for the baseline investigation. After reconstitution of 0.9 mg of freeze-dried rhTSH (Thyrogen ampules; Genzyme) with 1.2 mL of sterile water, part of the obtained solution was diluted with saline to a final concentration of 0.05 mg/mL. Immediately after dilution, 0.01 mg (0.2 mL; n = 9) or 0.03 mg (0.6 mL; n = 9) of rhTSH was injected in the quadriceps muscle. Twenty-four hours after the administration of rhTSH, a diagnostic dose of 40 MBq of sodium 123I was administered as an oral solution. RAIU, as a percentage of the administered dose of 123I corrected for physical decay, was measured at 24 h.
Radioiodine Therapy
Twenty-three days (median; range, 5–84 d) after the last diagnostic 24-h RAIU measurement, radioiodine therapy was given as a single oral dose to all 36 patients on an in-patient basis. The therapeutic dose of 131I was aimed at being sufficient to result in retention of 3.7 MBq (100 μCi) of 131I per gram of thyroid tissue at 24 h, according to the following formula: administered activity (GBq) = [thyroid weight (g) × 0.37 (GBq/g)]/24-h thyroid RAIU (%) (15). Thyroid weight was estimated from the planimetric surface on the baseline scintigram using the formula of Doering and Kramer (16): thyroid weight (g) = 0.326 × surface (cm2)3/2.
The 18 patients who were treated with rhTSH before radioiodine therapy again received an injection of rhTSH in the quadriceps muscle, using the same rhTSH dose as was given for the diagnostic investigation. The therapeutic dose of radioiodine was given 24 h later. In the rhTSH-pretreated patients, the therapeutic dose of 131I was adjusted to the 24-h RAIU after rhTSH pretreatment, as determined for the individual patients in the preceding diagnostic investigations. The RAIU ratio is defined as the ratio between the 24-h RAIU after rhTSH pretreatment and the baseline 24-h RAIU (Table 1). Neither group of 9 control patients received rhTSH pretreatment.
Patient Characteristics and Results of Radioactivity Measurements After Radioiodine Treatment With and Without rhTSH Pretreatment of Patients with Nodular Goiter
Thyroid Radioactivity Measurements and Dosimetric Calculations
In all 36 patients, thyroid radioactivity was measured every 24 h for 3 d after the administration of the therapeutic dose of radioiodine and on days 7, 10, 14, 21, and 28. A 7.62 × 7.62 cm (3 × 3 in.) NaI (Tl) detector was used, with a lead shield placed in front of it to reduce the counting rate and avoid dead-time effects. Measurements were corrected for a standard with a known activity of 131I, and all values were corrected for background radioactivity and for physical decay.
Thyroid radioactivity measurements were implemented in a simplified model for iodine biokinetics as described by Robertson and Gorman (14), with some amendments, as previously described by Huysmans et al. (10). Serum creatinine levels were within the reference range in all patients. Therefore, a normal urinary excretion rate of radioiodide was assumed for all patients (17). The rate of uptake of radioiodine into the thyroid was calculated from the radioactivity measurements at 24 h and from the radioiodide excretion rate. The fractional excretion of radioiodinated thyroid hormones from the thyroid into the circulation was calculated from thyroid radioactivity measurements from day 2 onward, fitted as a monoexponential function.
Radiation-absorbed doses in organs were calculated using the MIRD method (18). The calculated cumulated fractional activities in the source organs thyroid, urinary bladder, stomach, small intestine, and total body were entered in the MIRDOSE3.1 computer program (Oak Ridge Institute for Science and Education). Absorbed doses in the thyroid were corrected for the ratio of normal thyroid weight (20 g) to individual thyroid weight estimated by thyroid scintigraphy. Tissue weighting factors were used to determine the effective dose equivalent outside the thyroid (19).
Hormone Assays
Free thyroxine and total triiodothyronine were measured by chemiluminescent immunoassay and serum thyroid-stimulating hormone by 2-site immunochemiluminometric assay using an ACS:180 Automated Chemiluminescence System (Bayer).
PB131I Measurements
Blood samples were drawn from all patients at 1, 2, 3, 7, and 10 d and at 2, 3, and 4 wk after radioiodine administration. From each serum sample, 0.3 mL was taken for measurement of total 131I activity in the serum and 0.3 mL for measurement of PB131I activity. The latter 0.3-mL sample was prediluted with 0.9 mL of a solution of 0.05 mol/L phosphate buffer (pH 7.4) and 0.1 mol/L sodium chloride. Protein-bound iodine was precipitated by addition of 1.5 mL of cold trichloroacetic acid, 20%. The resulting samples were left standing for 10 min at room temperature and then centrifuged for 2 min at 2,000 rpm. The precipitate was washed twice with the trichloroacetic acid solution. By this method, 89% ± 6% of the total serum free thyroxine is precipitated (H.A. Ross, unpublished data, 1999). All samples (total serum and precipitate) were measured in a universal γ-counter (1282 Compugamma CS; Wallac). Radioactivity in all samples was compared with a standard curve of sodium-131I with known activity, to calculate the activity in MBq/L.
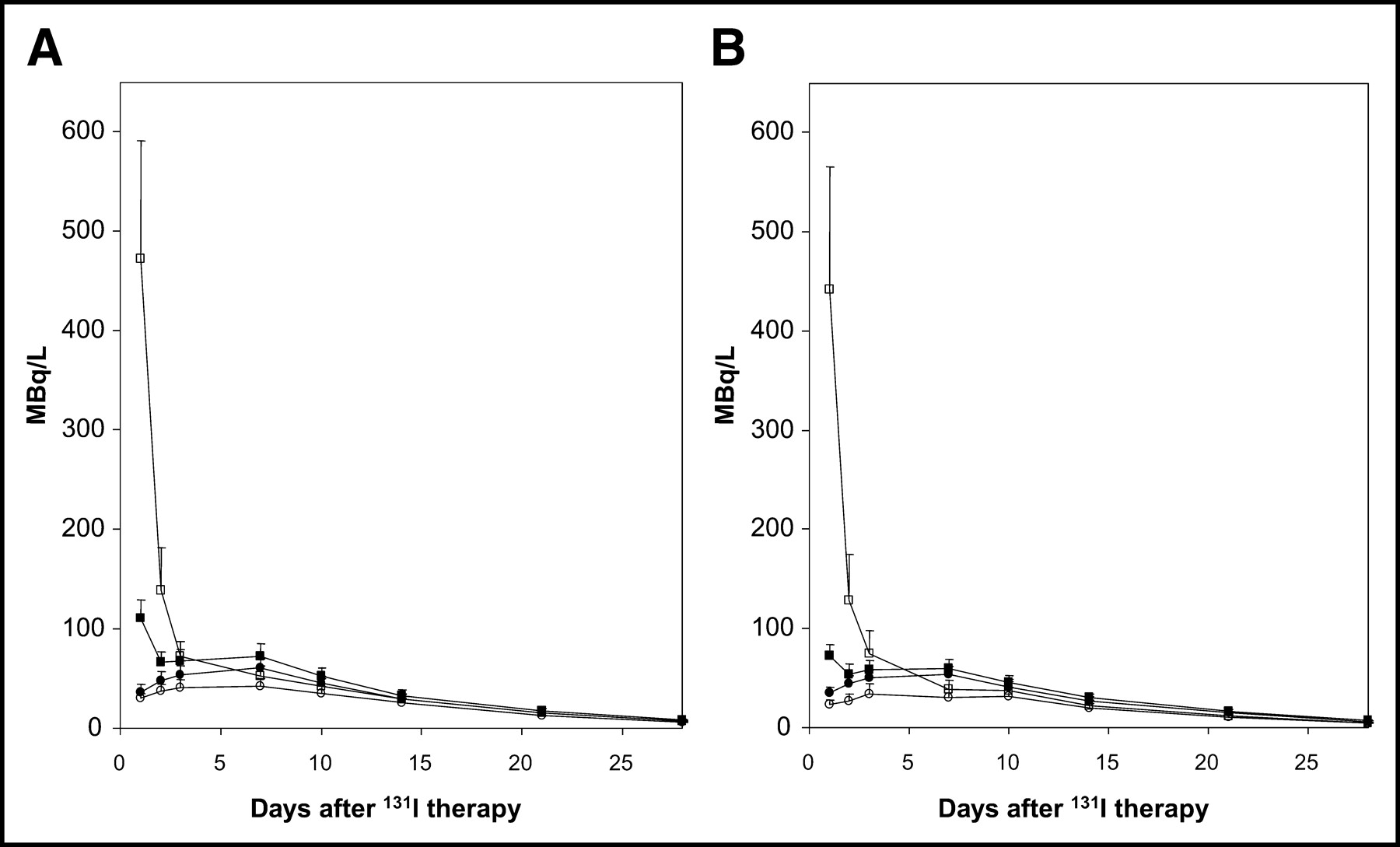
Time–activity curves were created for total 131I activity and PB131I activity in each individual patient (Fig. 1). The area under each PB131I time–activity curve was calculated. This area under the curve represents the cumulated PB131I activity in each serum fraction and is expressed in GBq·L−1·d. The cumulated total 131I activity in the serum was not calculated because, in view of radiation safety regulations in the hospital, measurements on the day of radioiodine therapy had not been performed and because total 131I activity in the serum is highest in the first hours after radioiodine administration, in contrast to PB131I activity, which is low during the first day after radioiodine therapy.
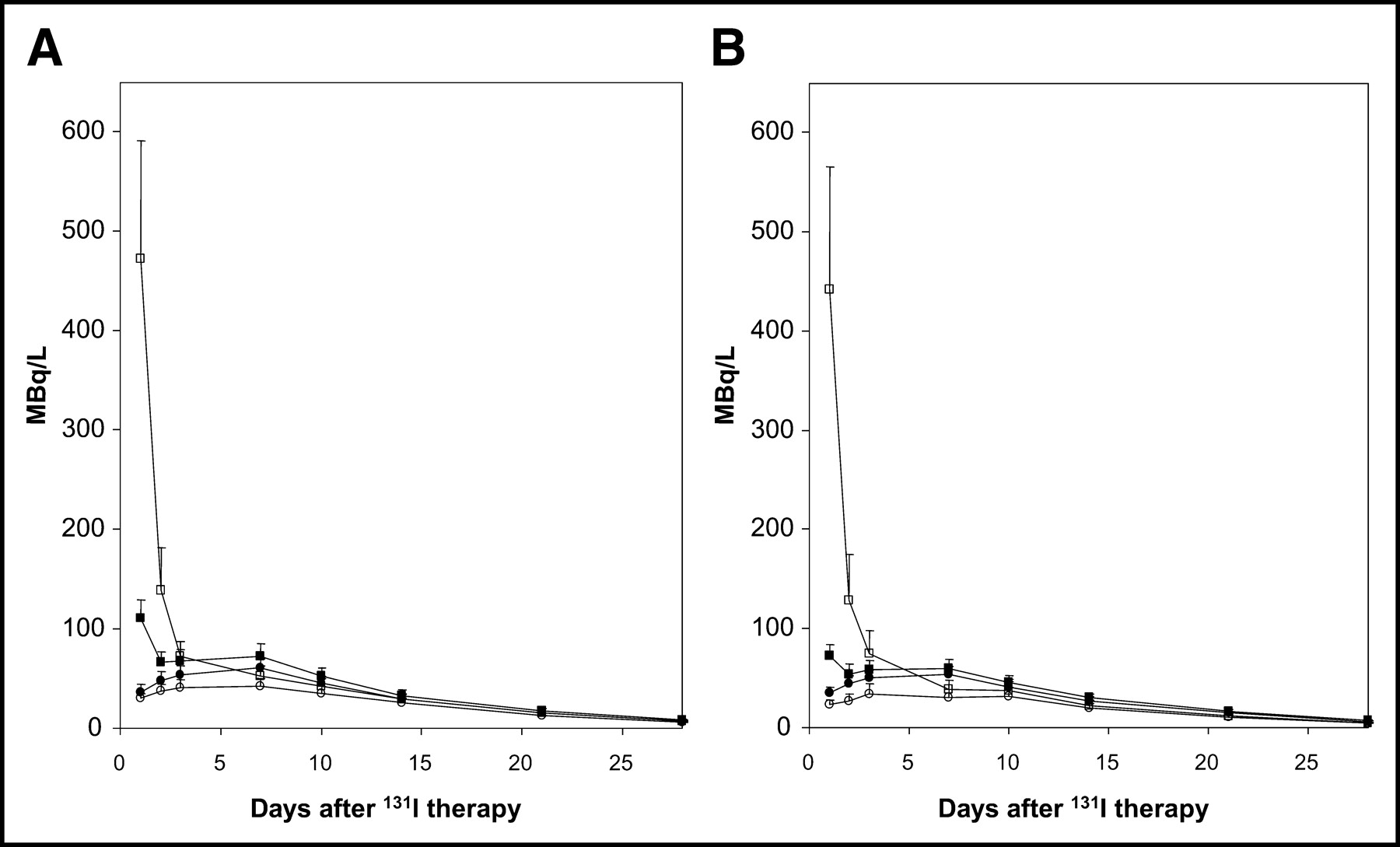
Total 131I activity and PB131I activity per liter of serum on day 0 after radioiodine therapy in patients with nodular goiter. (A and B) Nine patients were pretreated with 0.01 mg of rhTSH (A), and 9 with 0.03 mg of rhTSH (B). The results for each rhTSH group were compared with those for 9 control patients. Mean value + SEM is given. ▪ = total 131I activity in rhTSH-pretreated patients; □ = total 131I activity in control patients; • = PB131I activity in rhTSH-pretreated patients; ○ = PB131I activity in control patients.
Statistical Analyses
The mean value ± SD is given, unless otherwise stated. Statistical analyses were done using the Mann–Whitney U test (with probability values denoted as P) and the Spearman rank correlation test (with probability values denoted as P*). Areas under the time–activity curves obtained from the subjects who received rhTSH were compared with those of the matched controls by means of the Mann–Whitney U test. The time–activity curves themselves were compared by repeated-measures ANOVA, with time after 131I administration as the within-subject factor and rhTSH pretreatment as the between-subjects factor. Probability values < 0.05 were considered to indicate statistical significance.
RESULTS
Table 1 shows the characteristics of all patients and the data on their thyroid radioactivity measurements. As expected, because rhTSH-pretreated groups and control groups were matched for thyroid weight and thyroid 24-h RAIU, thyroid weight, based on planimetric thyroid scintigrams, and baseline thyroid 24-h RAIU were similar in the rhTSH groups and their respective control groups. rhTSH-stimulated 24-h RAIU in the pretreated groups was considerably higher than baseline RAIU in the control groups. Therefore, the average administered activities in the rhTSH-pretreated groups were considerably lower than those in the control groups (in the 0.01-mg rhTSH group, 67% of that in the control group; in the 0.03-mg rhTSH group, 53% of that in the control group; both P < 0.05).
Thyroid radioactivity measurements after radioiodine therapy showed somewhat lower 24-h RAIU of the therapeutic doses when compared with the 24-h RAIU of the previous diagnostic doses. However, this trend was observed not only in the rhTSH-pretreated groups but also in the control groups (Table 1). The effective half-time of 131I in the thyroid did not significantly differ between rhTSH-pretreated patients and control patients (Table 1). The cumulated fractional activity (MBq·h/administered MBq) in the thyroid was approximately 1.7 times higher in the 0.01-mg rhTSH-pretreated group and 2.2 times higher in the 0.03-mg rhTSH-pretreated group than in their respective control groups (Table 1). The cumulated fractional activity in the liver, as calculated from thyroid radioactivity measurements and the biokinetic model (14) with modifications (10), was also longer in the pretreated groups, because their higher thyroid RAIU caused the component of radioiodinated thyroid hormones to be larger. Cumulated fractional activities in the other source organs, mainly determined by inorganic iodide (stomach, small intestine, rest of body, urinary bladder), were significantly lower in the rhTSH-pretreated patients (0.01 mg and 0.03 mg rhTSH) than in their controls.
Table 2 shows the calculated absorbed doses in the tissues and organs for which a tissue-weighting factor has been determined (19), expressed as dose per unit of administered radioiodine (in mGy/MBq) and as dose resulting from the total administered activities of radioiodine (in Gy). The absorbed dose in the thyroid per unit of administered activity was higher in the pretreated groups than in the control groups because of the higher cumulated fractional activity in the thyroid of the pretreated groups.
Radiation-Absorbed Doses in Target Organs After Radioiodine Treatment With and Without rhTSH Pretreatment in Patients with Nodular Goiter
Outside the thyroid gland, the highest absorbed doses calculated per megabecquerel of administered 131I were in urinary bladder, followed by the stomach. For these organs, the absorbed doses per megabecquerel were significantly higher without than with rhTSH pretreatment (P < 0.0001). Absorbed doses per megabecquerel of administered radioiodine inversely correlated with 24-h RAIU for the urinary bladder (r = −0.73; P* < 0.0001) and the stomach (r = −0.74; P* < 0.0001). Absorbed doses per megabecquerel of administered radioiodine in some of the other target organs (bone surface, breast, lungs, red bone marrow, and skin) were determined predominantly by the cumulated fractional activity in the thyroid and were therefore higher in the pretreated groups than in the control groups.
The absorbed dose in the thyroid resulting from the total administered activity was similar in the pretreated groups and their respective control groups. Outside the thyroid, the highest absorbed doses resulting from the total administered activities were in the urinary bladder and the stomach. In these organs of excretion (bladder) and uptake (stomach) of inorganic iodide, the absorbed doses resulting from the total administered activity were 2- to 3-fold lower in the pretreated groups than in their control groups. In all other extrathyroidal organs and tissues, somewhat lower absorbed doses were found in the pretreated groups than in the control groups, but the differences did not reach significance, except for those in colon and gonads.
The effective dose equivalent for the combined organs and tissues outside the thyroid gland was considerably lower in the rhTSH-pretreated groups than in their control groups (0.01-mg rhTSH group vs. control group, 0.21 ± 0.09 Gy vs. 0.33 ± 0.10 Gy [P < 0.05]; 0.03-mg rhTSH group vs. control group, 0.12 ± 0.03 Gy vs. 0.27 ± 0.14 Gy [P < 0.05]).
The cumulated PB131I activity in serum did not differ significantly between pretreated groups and their respective control groups. The cumulated PB131I activity in serum was 0.93 ± 0.15 GBq·L−1·d in the 0.01-mg rhTSH group versus 0.70 ± 0.13 GBq·L−1·d in the control group and 0.85 ± 0.12 GBq·L−1·d in the 0.03-mg rhTSH group versus 0.52 ± 0.13 GBq·L−1·d in the control group (mean value ± SEM; n = 9). Figure 1 shows the time–activity curves of total 131I activity and PB131I activity in serum after radioiodine therapy in the 2 groups of rhTSH-pretreated patients and in the 2 control groups. The time course of PB131I activities did not significantly differ between pretreated and control groups.
DISCUSSION
Our study, based on thyroid radioactivity measurements and the iodine biokinetic model of Robertson and Gorman (14), shows that radioiodine therapy after pretreatment with rhTSH, with the dose of 131I reduced according to the rhTSH-induced increase in 24-h RAIU, caused a lower radiation burden to the extrathyroidal tissues than did radioiodine therapy without rhTSH pretreatment in patients with nodular goiter. The reduction in radiation burden was largest for the urinary bladder and the stomach. These are the extrathyroidal organs that receive the highest radiation doses from radioiodine therapy.
The therapeutic 131I doses given to the rhTSH-pretreated patients were reduced according to the individual increases in diagnostic 24-h RAIU after rhTSH administration. RAIU measurements after therapy showed that the 24-h RAIU of the therapeutic dose was somewhat lower than the 24-h RAIU of the preceding diagnostic dose in most patients. However, this occurred in all 4 groups of patients to a similar degree, and the 24-h RAIU of the therapeutic dose was considerably higher in the rhTSH-pretreated groups than in the control groups. The effective half-time of radioiodine in the thyroid did not differ significantly between pretreated and control groups. Therefore, although we calculated increased absorbed doses in the thyroid per unit of administered activity in the pretreated groups, the total absorbed doses in the thyroid were similar in the rhTSH-pretreated groups and their respective control groups. Thyroid volume reduction by radioiodine has been shown to correlate positively with the administered amount of radioiodine per gram of thyroid tissue corrected for 24-h RAIU (5) and consequently with the absorbed dose in the thyroid. Therefore, reducing the therapeutic dose of radioiodine after rhTSH administration is not likely to have negatively influenced thyroid volume reduction. This is in accordance with recently published data by our group (13).
We used the MIRDOSE3.1 program to calculate the doses that extrathyroidal tissues absorbed from the total administered activity of radioiodine. Extrathyroidally absorbed doses after radioiodine therapy were by far highest in the urinary bladder and stomach, as was expected because inorganic iodine is excreted through the bladder and is concentrated (although not made organic) in the stomach. Enhanced uptake of radioiodine in the thyroid of rhTSH-pretreated patients resulted in lower amounts of circulating inorganic radioiodine during the first days after therapy and in lower cumulated fractional activities of radioiodine in the inorganic radioiodine compartment (including the stomach) and the bladder. Therefore, the absorbed doses in urinary bladder and stomach were reduced by a factor of 2 in the 0.01-mg rhTSH group and by a factor of 3 in the 0.03-mg rhTSH group in comparison with their respective control groups. These reductions are important, because the risk of cancer of the stomach has been reported to be slightly increased after radioiodine therapy in patients with toxic, nodular goiter (20,21). In other studies, the incidences of bladder cancer and breast cancer have been reported to be increased in patients with toxic nodular goiter treated with radioiodine (22–24).
The liver is the organ in which 131I incorporated in thyroid hormones is collected and metabolized. This was accounted for by assigning 40% of the extrathyroidal thyroid hormone compartment to the liver. The amount of 131I-labeled thyroid hormone per megabecquerel of radioiodine administered was higher in the rhTSH-pretreated groups than in the control groups, resulting in a higher cumulated fractional activity of 131I in the liver in the rhTSH-pretreated groups. However, the absorbed dose in the liver was similar in rhTSH-pretreated and control groups because of the reduction in administered dose of radioiodine in the rhTSH-pretreated groups.
Absorbed doses in all extrathyroidal organs were lower in the rhTSH-pretreated groups than in the control groups. However, in the organs, in which the absorbed dose is predominantly determined by the cumulated activity in the thyroid, the difference did not reach statistical significance, because the cumulated activity in the thyroid was similar in rhTSH-pretreated and control groups. The effective dose equivalent outside the thyroid was considerably lower in the rhTSH-pretreated groups than in their respective control groups (1.6-fold in the 0.01-mg rhTSH group and 2.3-fold in the 0.03-mg rhTSH group).
Not only thyroid iodine uptake but also thyroid hormone release is stimulated by thyroid-stimulating hormone. Thyroid stimulation predominantly releases thyroid hormones incorporating iodine that was recently taken up, not iodine that was stored for a longer time (last-come, first-served principle of thyroid iodine release) (25). Therefore, it might be that the administration of rhTSH before radioiodine therapy increases the release of radiolabeled thyroid hormones from the thyroid into the circulation. It has been argued that such an increase in radiolabeled thyroid hormones in the serum (PB131I) might outweigh the advantage of a reduction in radioiodine dose after rhTSH pretreatment (26). Our measurements were reassuring, because no significant difference in the time course of circulating PB131I levels was observed between the rhTSH-pretreated groups and the control groups and because the cumulated PB131I activities did not differ significantly between pretreated and control groups. This is in accordance with our thyroid RAIU measurements after radioiodine therapy, which showed no significant difference in effective half-times of 131I in the thyroid between rhTSH-pretreated patients and control patients.
During the first days after radioiodine therapy, the amount of PB131I was still low and the total 131I activity in serum was determined predominantly by the amount of inorganic 131I in the serum. During these first days, we measured much higher total 131I activities in the control groups than in the rhTSH-pretreated groups. The difference at 24 h after radioiodine therapy exceeded by far the difference in therapeutic dose of radioiodine between rhTSH-pretreated groups and control groups, because the higher uptake of inorganic 131I by the thyroid in the pretreated groups increased the removal rate of radioiodine from the circulation into the thyroid, whereas the removal rate to the urinary compartment was the same in both pretreated and control groups. This finding is in accordance with the iodine biokinetic model of Robertson and Gorman (14).
CONCLUSION
After pretreatment with a single, low dose of rhTSH, radioiodine therapy—of a dose reduced in accord with the rhTSH-induced increase in 24-h RAIU—caused lower radiation-absorbed doses in extrathyroidal organs and tissues, especially in the bladder and stomach, of patients with nodular goiter. No significant increase in the release of 131I-labeled thyroid hormones from the thyroid into the circulation was observed after radioiodine therapy in rhTSH-pretreated patients. Thus, this mode of therapy can be recommended, especially when the dose of radioiodine to be administered without rhTSH pretreatment is high.
Footnotes
Received Nov. 6, 2003; revision accepted Nov. 17, 2003.
For correspondence or reprints contact: Willy-Anne Nieuwlaat, MD, Department of Endocrinology, University Medical Center Nijmegen, P.O. Box 9101, 6500 HB Nijmegen, The Netherlands.
E-mail: wanieuwl{at}knmg.nl
REFERENCES
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- The Role of Nuclear Medicine in the Clinical Management of Benign Thyroid Disorders, Part 2: Nodular Goiter, Hypothyroidism, and Subacute Thyroiditis
- Time to reconsider nonsurgical therapy of benign non-toxic multinodular goitre: focus on recombinant human TSH augmented radioiodine therapy
- Low-dose recombinant human thyrotropin-aided radioiodine treatment of large, multinodular goiters in elderly patients