


Abstract
Because of the difficulty of predicting the response of patients with idiopathic dilated cardiomyopathy (IDC) to β-blocker therapy, this study was performed to evaluate whether gated myocardial SPECT (gated SPECT) could be useful for predicting that response. Methods: We performed gated SPECT with 99mTc-sestamibi on 38 patients with IDC before treatment with a β-blocker and standard medication. Perfusion abnormalities, left ventricular (LV) function, and spheric distortion were assessed by a quantitative software program. Results: We classified patients into 2 groups according to improvement in LV function after 4 mo of therapy. The groups consisted of 16 poor responders whose LV ejection fraction (LVEF) increased less than 10% and 22 good responders whose LVEF increased by 10% or more. The patient characteristics before therapy, including LV volume and LVEF, did not significantly differ between the 2 groups, but the size of the myocardial perfusion defect and spheric distortion were significantly greater in poor responders than in good responders. Conclusion: Gated SPECT, by allowing simultaneous assessment of perfusion, function and geometry, might be useful for predicting the response of patients with IDC to β-blocker therapy.
The medical approach to heart failure has changed radically over the past 10 y. Despite negative inotropic effects, β-adrenergic blocking agents improve the symptoms, left ventricular (LV) function, and survival of patients with congestive heart failure (1–3). On the other hand, the effect of β-blocker therapy varies in heart failure patients, who may show no change or may deteriorate after treatment (4,5). Therefore, predicting whether patients will respond to β-blocker therapy remains difficult.
Electrocardiographic gated myocardial SPECT (gated SPECT) using a 99mTc-labeled myocardial perfusion agent can assess both myocardial perfusion and LV function within a single study (6). LV volumes measured by gated SPECT are reproducible and correlate well with findings from echocardiography, contrast left ventriculography, and MRI (7–11). In addition, endocardial and epicardial contours of LV could be obtained automatically using a quantitative gated SPECT program (6). This information seems to be useful for the assessment of LV geometry with methods such as echocardiography, because the shape and size of the failing heart progressively change (12–14).
This study evaluated the feasibility of gated SPECT for predicting improved LV function in patients with idiopathic dilated cardiomyopathy (IDC) after β-blocker therapy.
MATERIALS AND METHODS
Patients
Thirty-eight patients with IDC (mean age, 50.6 ± 11.3 y; range, 24–72 y) gave written informed consent, according to a protocol approved by the Human Investigations Committee of our institute, to participate in this study. All had experienced at least 1 episode of exacerbated heart failure requiring short-term hospitalization and underwent baseline cross-sectional echocardiography, left ventriculography, and coronary angiography. The LV ejection fraction (LVEF) of all patients was <40% before entry into the study. None had received β-blockers or β-agonists within 3 mo of the study. Otherwise, medication, including oral digitalis, diuretics, or angiotensin-converting enzyme inhibitors, remained unchanged during the study period. None of the patients had significant coronary stenosis on coronary angiography (narrowing > 50% of the artery lumen). Patients with atrial fibrillation or other arrhythmias were excluded because irregular beats can affect the assessment of LV function by gated SPECT.
Gated SPECT Acquisition
All patients underwent gated SPECT before β-blocker therapy. A 600-MBq dose of 99mTc-sestamibi was administered by intravenous injection at rest. Approximately 1 h later, SPECT was performed using a dual-head angular rotating γ-camera (VERTEX+MCD; ADAC Laboratories) equipped with a low-energy general-purpose collimator. Image acquisition parameters were 180° (30 steps; 6° per step) using a 64 × 64 matrix and a 20% main window centered at the photopeak energy of 99mTc (140 keV). At each projection, a total of 8 individual electrocardiographic gated frames or cardiac cycles was acquired (50 beats per step). Projection data were reconstructed using 12 maximum-likelihood expectation maximization iterations using a Butterworth filter (cutoff = 0.45 cycle/cm, order = 10).
With the workstation system, the resulting transaxial image sets were reoriented into short-axis sets, to which an automatic LVEF measuring algorithm developed by Cedars-Sinai Medical Center was applied (6). The algorithm operates in 3-dimensional space. It segments the left ventricle, estimates and displays endocardial and epicardial surfaces for all gating intervals in the cardiac cycle, calculates the LV cavity volumes, and derives the global LVEF from the end-diastolic and end-systolic volumes, all without operator interaction. To investigate the effect of LV spheric distortion on clinical outcome, we defined the sphericity index as the ratio of the LV long axis to the LV vertical diameter on end-diastolic long-axis images with overlaid endocardial and epicardial contours as performed in previous studies using echocardiography (12–14). The long axis of the LV was measured from the mid portion of the mitral annular plane to the LV apex. The vertical diameter was assessed as the perpendicular line dropped through the midpoint of the long axis, extending from the LV anterior wall to the LV inferior wall (Fig. 1). We assessed myocardial perfusion abnormalities using segmental perfusion polar maps that showed pixels corresponding to the maximum ventricular perfusion to be equal to 100% of the summed gating data. The extent of the perfusion defect was defined as the sum of the number of profile points falling below the normal limit and was expressed as a percentage. The software for assessing myocardial perfusion defects was also developed by Cedars-Sinai Medical Center (15).

Assessment of LV shape using the sphericity index of gated SPECT. Bold lines represent tracing of LV contours using quantitative gated SPECT algorithm on end-diastolic images. Lines with arrowheads represent measurements of the long and vertical axes of the left ventricle. L = long axis of left ventricle; V = vertical axis of left ventricle.
β-Blocker Therapy and Assessment of Response
In addition to the standard therapy for heart failure, β-blockers were administered to the patients, taking into consideration their individual medical histories and other accompanying diseases. Thus, the initial recommended starting doses of the 2 β-blockers, carvedilol and bisoprolol, approved for treatment of chronic heart failure (1–3) were 2.5 and 0.5 mg daily, respectively. The dosage was gradually increased according to weekly titration. The daily target doses were 20 mg for carvedilol and 5 mg for bisoprolol (16,17). Twenty-one and 17 patients received carvedilol and bisoprolol, respectively.
After having been observed in the hospital for 4 more weeks, the patients were discharged and monitored through the outpatient clinic. We reassessed LVEF by gated SPECT approximately 4 mo (131 ± 43 d) after the patients began receiving the drugs. The duration of follow-up was defined in a previous study (14). The patients were classified into 2 groups (good and poor responders), according to changes in LVEF after 4 mo of β-blocker therapy. Good responders were patients whose LVEF increased by 10% or more after therapy. Poor responders were those with less than a 10% increase in LVEF, compared with the value before treatment.
Statistical Analysis
Data are expressed as mean ± SD. Baseline variables were compared using the Mann–Whitney U test for discrete variables and the unpaired t test for continuous variables. Serial changes in the LV volumes and LVEF values derived from gated SPECT in response to β-blockers were compared using the paired t test. Probability values less than 0.05 were considered significant.
RESULTS
All 38 patients were eventually able to take the full dose of β-blocker without any problems. According to the criteria of functional recovery in this study, 22 of 38 patients with IDC responded well to β-blocker therapy, whereas the remaining 16 had a poor response. Age, sex, functional class, type of β-blocker, cardiothoracic ratio, and hemodynamic variables such as heart rate, systolic and diastolic blood pressure, pulmonary capillary wedge pressure, and cardiac index did not significantly differ between the 2 groups at admission into the study (Table 1).
Clinical Characteristics Before β-Blocker Therapy
All gated SPECT studies were considered technically adequate, and image quality was suitable for reconstruction. In no instance did the QGS algorithm fail. Table 2 shows gated SPECT parameters before and 4 mo after β-blocker therapy. The follow-up periods did not significantly differ between good (144 ± 65 d) and poor (129 ± 51 d) responders. Although end-diastolic and end-systolic LV volumes and LVEF at baseline did not significantly differ between good and poor responders, the LV end-diastolic (235.6 ± 59.4 to 160.9 ± 34.3 mL, P < 0.01) and end-systolic (185.3 ± 54.8 to 94.6 ± 26.2 mL, P < 0.01) volumes significantly decreased and LVEF distinctly increased (22.1% ± 6.4% to 41.8% ± 7.5%, P < 0.01) in the good responders. In contrast, end-diastolic (238.9 ± 73.3 to 223.2 ± 75.5 mL) and end-systolic (188.3 ± 71.4 to 167.3 ± 71.4 mL) LV volumes and LVEF (22.7% ± 9.3% to 26.6% ± 8.9%) did not significantly change among the poor responders. In the comparison of baseline parameters, the extent of perfusion defect was greater in poor responders than in good responders (7.56% ± 6.70% vs. 2.36% ± 1.47%, P < 0.05) and the sphericity index was significantly smaller in poor responders than in good responders (1.52 ± 0.15 vs. 1.77 ± 0.26, P < 0.05). In good responders, the sphericity index significantly increased 4 mo after β-blocker therapy (1.77 ± 0.26 to 1.86 ± 0.14, P < 0.05).
Gated SPECT Parameters Before and 4 Months After β-Blocker Therapy
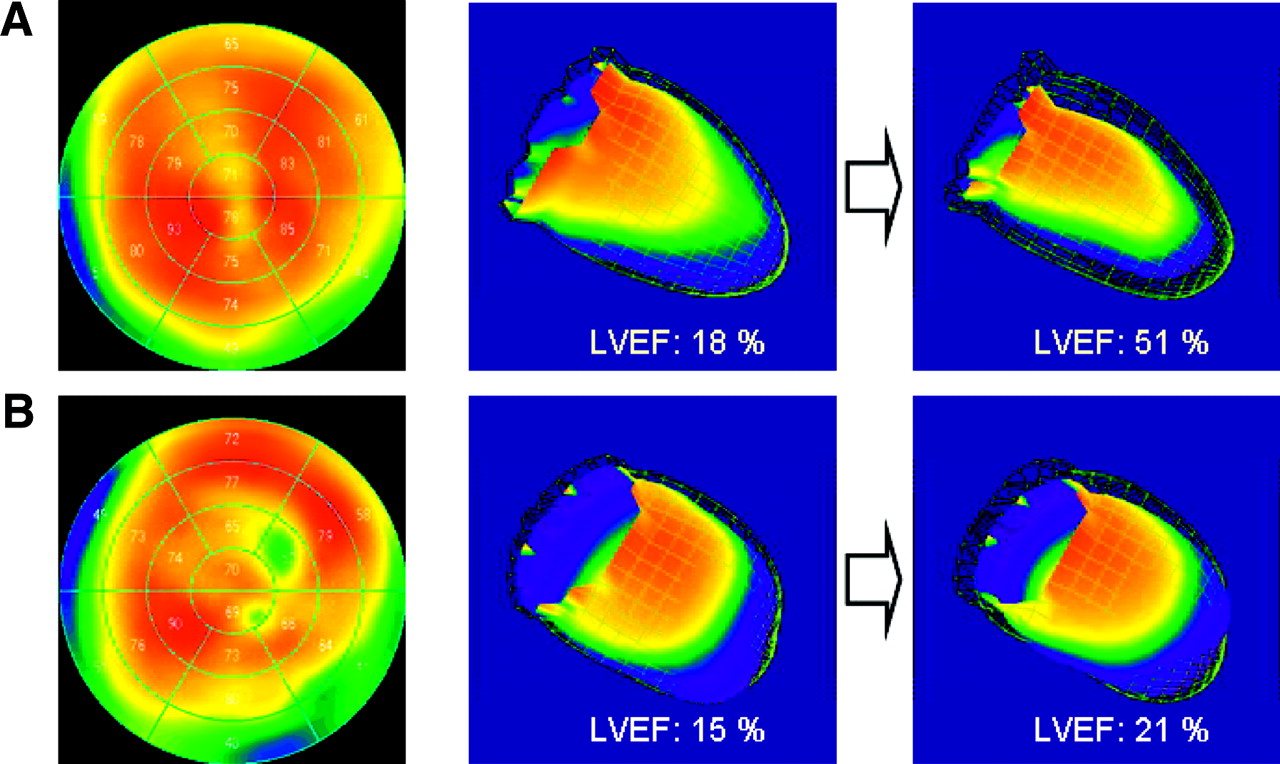
Representative gated SPECT images from good and poor responders are shown in Figure 2. The ungated perfusion polar maps represent the degree of myocardial perfusion abnormalities, and the 3-dimensional display of the LV endocardial surfaces represents the distortion of cardiac geometry. Poor responders had larger perfusion defects and a more spheric LV than did good responders.
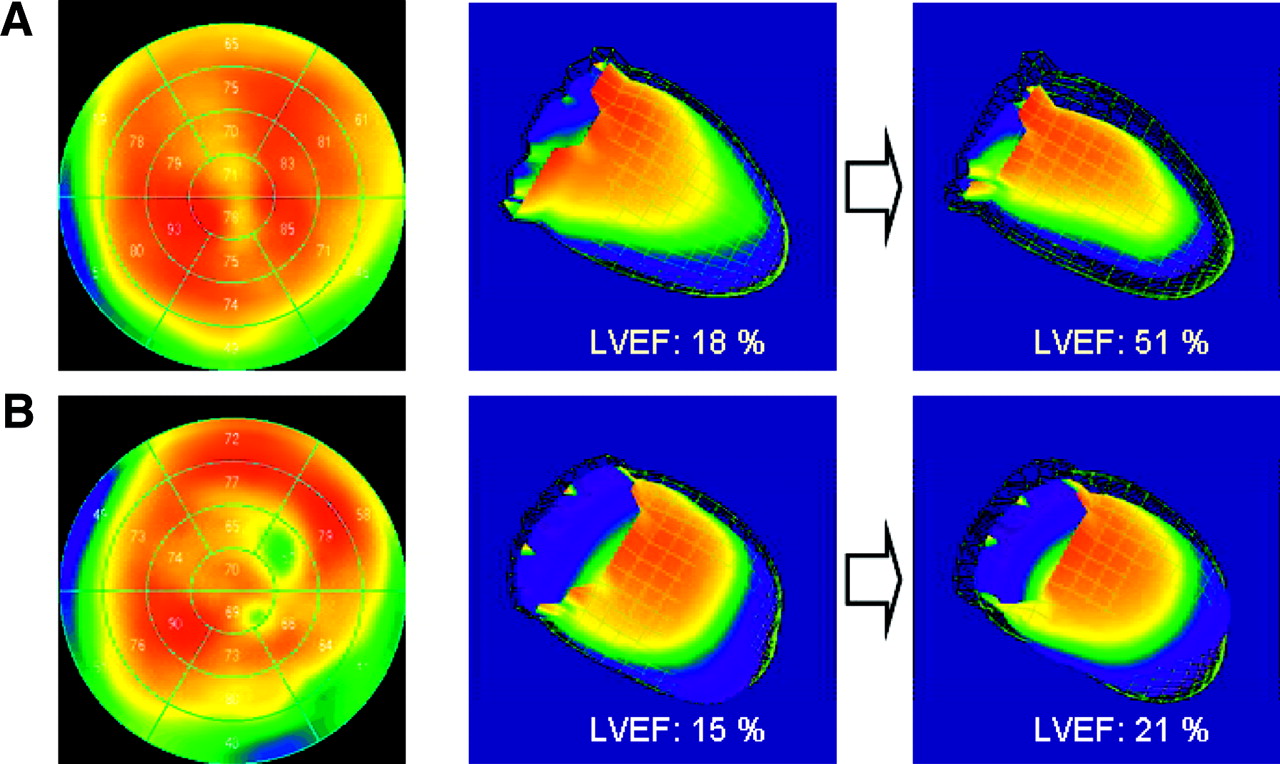
Representative gated SPECT images from good responders (A) and poor responders (B). Shown are ungated perfusion polar maps before therapy (left panels) and serial 3-dimensional displays of end-diastolic (grid) and end-systolic (solid) surfaces from a right anterior oblique 30° view (middle and right panels). Small perfusion defects are present in apical and posterior myocardium of good responders (extent of defect, 4%). Three-dimensional displays show that LV shape is preserved as a prolate ellipse (sphericity index, 1.7). LVEF increased by 33% after β-blocker therapy. In contrast, multiple perfusion defects were observed in poor responders (extent of defect, 11%) and the LV cavity is spheric (sphericity index, 1.3). LVEF increased by only 6% after 4 mo of β-blocker therapy.
DISCUSSION
All available trials of β-blockers versus a placebo show that the administration of β-blockers for at least 3 mo is associated with improved LV systolic function (13,18). However, a subgroup of patients with IDC responds to β-blocker therapy with symptomatic and functional improvement (4,5). Few reports have examined the characteristics of patients likely to respond to β-blocker therapy (16,17,19,20), yet such features should be defined. The present study established that β-blocker therapy would be more effective in patients with fewer myocardial perfusion defects and less spheric distortion of the LV cavity. Both of these predictive characteristics can be demonstrated by a single gated SPECT acquisition.
Myocardial perfusion defects are frequent and are associated with worse cardiac function in patients with IDC. The present study found that patients with extensive perfusion abnormalities on SPECT responded negatively to β-blocker therapy, whereas those with smaller perfusion abnormalities responded positively. Yamada et al. demonstrated that patients with mild fibrosis on myocardial biopsy responded to β-blocker therapy better than did those with severe fibrosis (19). Our results were similar to theirs, perhaps because myocardial perfusion abnormalities on SPECT could represent the loss of myocardial mass and decreased tissue blood flow to the fibrotic myocardium in patients with IDC. Because of the difficulty of adequately performing myocardial biopsies on all IDC patients before starting β-blocker therapy, myocardial SPECT could be used to noninvasively assess histologic changes.
Perfusion abnormalities associated with IDC have historically been assessed using 201Tl SPECT (17,21–23). Suwa et al. reported that visual assessment of 201Tl SPECT images showed no difference in the extent of perfusion defects between responders and nonresponders with IDC (17). The reason for the discrepancy between their results and ours remains unclear, but we used 99mTc-sestamibi for gated SPECT because it has a better photon energy and a higher injected dose than does 201Tl. These advantages better eliminate diaphragmatic attenuation, and the distribution of myocardial perfusion is accurate even in patients with an enlarged LV cavity. In addition, the software that we used can quantitatively and automatically estimate a large defect or multiple small, fixed defects. Thus, 99mTc-sestamibi combined with quantitative software might better assess perfusion abnormalities in IDC patients than does 201Tl with visual analysis.
End-diastolic LV volume, end-systolic LV volume, and LVEF before β-blocker therapy did not significantly differ between good and poor responders. However, the spheric index of the LV cavity was greater in good than in poor responders. Our findings confirm previous reports that LV volume and LVEF were not consistently important in determining prognosis in IDC (20,24,25) and that poorer survival was associated with a more spheric LV cavity in patients with IDC (12). A change in LV shape from the normal ellipsoid to a spheric configuration is associated with increased afterload, abnormal distribution of fiber shortening, more depressed contractility, and a blunted response to infused dobutamine (26). Interestingly, the sphericity index improved after β-blocker therapy in good responders but did not change in poor responders. Although the exact mechanism of the effect of β-blockers on IDC remains unclear, distortion of LV shape may be related to β-blocker resistance in patients with IDC and LV dysfunction. However, Harjai et al. reported that the degree of spheric LV distortion did not correlate with the prognosis of patients with nonischemic cardiomyopathy (27). The baseline characteristics of their patients and ours did not differ, but their patients did not receive β-blocker therapy. This difference is one explanation for the discrepancy between their findings and ours, because β-blockers can improve both LV shape and LV function (13,14,18,28). Although the relationship between the degree of LV sphericity and the prognosis of β-blocker therapy is unknown, our results suggest that LV distortion might be more important to the success of β-blocker therapy. Further studies, including a prospective application to a larger patient population, are needed to confirm this observation and to fully explain the importance of LV shape in predicting the value of β-blocker therapy.
This study had some limitations. First, the study applied 2 β-blockers to treat IDC. In the absence of studies that directly compare these drugs, no specifics substantiate a preference for either. Similar results in terms of modality and mortality reduction have been obtained with second- or third-generation β-adrenergic blockers (29,30). Therefore, carvedilol and bisoprolol are the agents of choice for treating patients with heart failure. Second, the dose of both β-blockers was relatively lower than that used in Western countries. The dose that we used in this study was the standard dose in Japan (16,17). The reason for the discrepancy remains unclear, but there might be some differences in response to β-blockers between Japanese and non-Japanese individuals. A Japanese multicenter trial revealed that 20 mg of carvedilol improves LV function in chronic heart failure (31). Moreover, the CIBIS II trial found no difference in outcomes among low, medium, and high doses of bisoprolol (3). Thus, the dose of β-blocker we chose for our present study might not have affected its outcome. Third, the sphericity index was obtained using only gated SPECT. We did not directly compare gated SPECT and echocardiography, which is considered a standard procedure for measuring cardiac geometry. Nevertheless, gated SPECT has a wide field of view, including the entire LV cavity without consideration of the adjacent lung structure, and the sphericity index was obtained by applying the same principle as is applied in echocardiography. Therefore, the sphericity index obtained from gated SPECT might be reliable to evaluate LV geometry.
CONCLUSION
Improvement in LV function with β-blocker therapy was associated with the extent of perfusion abnormalities and the spheric LV distortion. Gated SPECT might be useful for predicting the effectiveness of β-blocker therapy in patients with IDC through the simultaneous assessment of myocardial perfusion, LV function, and cardiac geometry.
Acknowledgments
The authors thank the nuclear medicine technologists of National Cardiovascular Center Hospital for excellent assistance in performing the SPECT studies.
Footnotes
Received Sep. 15, 2003; revision accepted Dec. 2, 2003.
For correspondence or reprints contact: Kazuki Fukuchi, MD, Department of Radiology, National Cardiovascular Center, 5-7-1 Fujishiro-dai, Suita, Osaka, 565-8565, Japan.
E-mail: kfukuchi{at}hsp.ncvc.go.jp
REFERENCES
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.