


Abstract
This prospective clinical study used 99mTc-sestamibi (MIBI) brain SPECT to assess residual tumor volume and determine whether it would be prognostic of survival at the end of cranial irradiation in patients with malignant glioma. Methods: Fifty-seven patients with supratentorial malignant glioma were included in this clinical trial. Tomoscintigraphy was performed 4 h after an intravenous injection of MIBI (1,110 MBq). The images were obtained from a dual-head γ-camera using fanbeam collimators. Transverse, coronal, and sagittal views were reconstructed. Metabolic tumor volume (MTV), using an ellipsoid model, was calculated from the 3 slices. The first posttherapeutic neuroradiologic evaluation was performed at the end of each patient’s radiation therapy. Results: 99mTc-MIBI brain SPECT performed at the end of cranial irradiation provided data that allowed the identification of residual tumor and could be used to accurately predict survival of malignant glioma patients, taking into account the established prognostic factors. Patients with an MTV < 32 cm3 had a median survival of 358 d, as opposed to 238 d in patients with an MTV ≥ 32 cm3 (P = 0.05). Moreover, half of CT scans performed at the same time were considered to show doubtful or only suggestive findings. No diagnosis of tumor progression or inflammatory changes was possible. Conclusion: 99mTc-MIBI brain SPECT may help in establishing the prognosis of glioma patients at the end of radiation therapy. Consequently, the management of patients can be adapted. These new data should be considered in the design of future clinical studies of malignant glioma patients as a way to quickly assess the efficiency of therapies.
Malignant gliomas account for 60% of all primary brain tumors (1), and patients with this tumor type have a dismal prognosis. The standard for treatment has essentially been unchanged for many decades, that is, surgical resection of as much of the tumor as can safely be done, followed by radiation therapy and chemotherapy. Even under the best of circumstances, in those patients in whom essentially all of the tumor visualized through MRI is surgically resected or in whom high-grade gliomas have received the maximally tolerated doses of radiation and chemotherapy, the mean survival is extended from 2–3 mo to only 1 y (1–3). This uniformly poor response to treatment remains a critical problem in the management of these patients (3).
Early and reliable assessment of therapeutic response and of individual patient prognosis is essential in decisions on whether to continue therapy. The results of both CT and MRI performed at the end of cranial irradiation are difficult to interpret because of the inflammation resulting from surgery or the radiation and offer only an imperfect indication of tumor viability. Functional imaging with 201Tl brain SPECT is now known to be useful in detecting the presence of recurrent glioma after radiation therapy. For this purpose, 201Tl brain SPECT has been shown to have an accuracy similar to that of 18F-FDG PET (4,5). However, for primary brain tumors, 99mTc-sestamibi (MIBI) brain SPECT has demonstrated better specificity than have 201Tl studies (6–8).
Patient survival after therapy for malignant gliomas has been correlated with a variety of factors including the type of tumor, age of the patient, histologic findings, score on the Karnofsky performance scale (KPS), and completeness of tumor resection (1–3); however, few investigators have assessed the utility of 99mTc-MIBI brain SPECT for this purpose. To our knowledge, no previous reported studies have assessed the correlation of survival time with the findings of brain SPECT using MIBI as the radiotracer. We set up a prospective study that used 99mTc-MIBI brain SPECT to measure residual tumor volume at the end of cranial irradiation and assessed the correlation of tumor volume with survival.
MATERIALS AND METHODS
Population
From May 1995 to May 1998, 57 patients with a supratentorial malignant glioma of grade 3 or 4, based on the Sainte Anne–Mayo classification, were included in a phase II clinical study approved by the local ethical review committee (9). After a total or incomplete macroscopic tumor resection or a stereotactic biopsy, partial-brain irradiation was administered to limited fields. The treatment volume was determined by defining the volume of the contrast-enhanced tumor on a preoperative CT scan, adding a 2-cm margin beyond the edema surrounding the tumor. Between 2 and 2.5 Gy per day were delivered 5 times per week for 5 wk, up to a maximum of 50–55 Gy. Etoposide, used as a single agent for chemotherapy, was given at a dose of 100 mg/m2 for 3 consecutive days. The first course of etoposide was administered on days 1, 2, and 3 of radiotherapy and during the week after the end of radiotherapy. Treatment was consolidated by 4 additional rounds of etoposide intake, with an interval of 4 wk.
Imaging Protocol
Commercially available MIBI kits (Cardiolite; Dupont-Pharma) were labeled with 99mTc according to the manufacturer’s recommendations. Brain SPECT was performed 4 h after an intravenous injection of 99mTc-MIBI (1,110 MBq, i.e., 30 mCi) in an antecubital vein. Images were acquired using a dual-head γ-camera (Helix; Elscint), with a 128 × 128 matrix, a 360° rotation, a 6° step-and-shoot technique, and an acquisition time of 30 s per frame. Images were reconstructed in a 128 × 128 matrix with a Butterworth-filtered backprojection (cutoff = 0.25 × Nyquist frequency; order of 5). Thick transverse, coronal, and sagittal views including the total representation of the tumor were generated; slice thickness was determined by visual selection of the first and last slices showing MIBI uptake in the tumor area. The thick transverse slice generated was used for quantitative analysis. These thick sagittal, coronal, and transverse slices allowed us to estimate metabolic tumor volume (MTV). The tumor was considered a sphere (7). The sphere volume was calculated by (4/3)πr3; the radius is half the diameter, d/2, so (4/3)πr3 = (4/3)π ((d/2)3) = (4/3)π (d3/8). The sphere volume is approximately d3/2. In the whole-tumor slices, the diameter of the tumor was evaluated in the 3 projections, and the tumor volume was calculated as (d1 × d2 × d3)/2 (d1, d2, and d2 were calculated by the algorithm of the filtered backprojection; for details, see Soler et al. (7)). Two experienced readers interpreted the MIBI images; they were not aware of the CT results. The first posttherapeutic neuroradiologic evaluation (CT scan and brain tomoscintigraphy) was performed on all patients within the first 10 d after completion of radiation therapy. In no patients was surgical resection performed on the basis of their having a certain volume of MIBI uptake. The results from MIBI SPECT imaging after radiotherapy were not used to alter the management of patients.
Statistical Analysis
Overall survival time was defined as the period between the date of surgery and the date of death, regardless of whether its cause was related to the malignant glioma. Overall survival time was calculated using the Kaplan–Meier method (10). Differences in survival times were tested for statistical significance using the log-rank test. To determine truly independent variables (i.e., prognostic factors), multivariate analysis using the Cox proportional hazards model was performed using a stepwise entry for variables, with P ≤ 0.05 for entry into the model and P > 0.10 for exclusion (11). The variables used in the analysis were age, KPS score, type of surgery, tumor volume, and interaction (type of surgery × tumor volume).
RESULTS
Patient Population
The characteristics of the patient population were consistent with similar patient populations reported in the literature. The sex ratio was 2:1 (36 male patients and 21 female), the median age was 61 y, 13 had grade 3 disease and 44 had grade 4, and the median KPS score was 80. Among the 57 patients, 24 underwent total macroscopic tumor resection (no contrast enhancement was detected on CT performed within 72 h of surgery), an incomplete resection was performed on 10 patients, and a stereotactic biopsy was performed on 23 patients. The patients then underwent radiotherapy and chemotherapy.
CT
Because of limited access to MRI, all but 1 patient in the study underwent brain CT as the routine radiologic evaluation. CT was performed within the first 10 d after radiation therapy. Eight patients had negative CT findings (no contrast enhancement or edema suggesting a tumor; they all previously had a complete tumor resection). Twenty-three patients had positive CT findings (a tumor was diagnosed; these 23 patients previously had a stereotactic biopsy). Twenty-five patients had suggestive CT findings (the interpretation of images was doubtful, and the diagnosis of a tumor, a radionecrosis, or an artifact was not allowed). All these patients underwent a complete or incomplete tumor resection. CT scans were reviewed by 2 independent neuroradiologists.
Brain SPECT
The tomoscintigraphy was performed on all 57 patients. Only 4 patients displayed negative 99mTc-MIBI brain SPECT findings; no MIBI uptake was found in the tumor area or in the opposite cerebral hemisphere. These 4 patients had undergone a complete tumor resection. MTVs, calculated on brain tomoscintigraphy, ranged from 0 to 126.71 cm3; the mean was 25.19 cm3 and the median volume, 16.19 cm3. The results of CT and 99mTc-MIBI brain SPECT were matched and analyzed. No concordance between CT and tomoscintigraphy was found (Table 1). For the 8 patients with negative CT findings, the brain tomoscintigraphy findings were negative in 2 patients, and the MTV was inferior to the median volume in 5 patients. In the 26 cases of doubtful CT findings, 99mTc-MIBI brain SPECT findings were negative in 1 patient, and the MTVs were superior to the median volume in 10 patients.
Comparison of MTV as Determined by CT and 99mTc-MIBI SPECT
Survival Analysis
The overall survival time ranged from 104 to 1,463 d. The median survival time (MST) was 337.5 d and the mean survival time, 412.6 d, including four 2-y survivors. When a univariate analysis using the log rank test was performed, age, KPS score, complete tumor resection, MTV calculated on tomoscintigraphy, and negative CT findings all were found to be statistically related to survival (Table 2). No statistical difference was found for histology grade (grade 3 vs. grade 4) (P = 0.38); however, because only a biopsy could be done for many patients, many were probably classified as grade 3 but instead were grade 4. Younger patients (age ≤ 60 y) had an MST of 384 d, as opposed to 273 d for older patients (P = 0.029). Patients with a KPS score ≥ 80 had an MST of 366 d, versus 318 d in patients with a KPS score < 80 (P = 0.006). Patients who underwent a complete tumor resection had an MST of 456 d, versus 294 d in patients with a residual tumor (P = 0.008). Patients with an MTV < 32 cm3 (corresponding to the third quartile of the volume distribution) had an MST of 358 d, versus 238 d for patients with an MTV ≥ 32 cm3 (P = 0.05) (Fig. 1). The 4 patients with completely negative MIBI SPECT findings had an MST of 465 d. Patients with negative CT findings (for CT performed during the first 10 d after radiation therapy) had an MST of 500 d, versus 238 d in patients with positive CT findings (P = 0.0008).
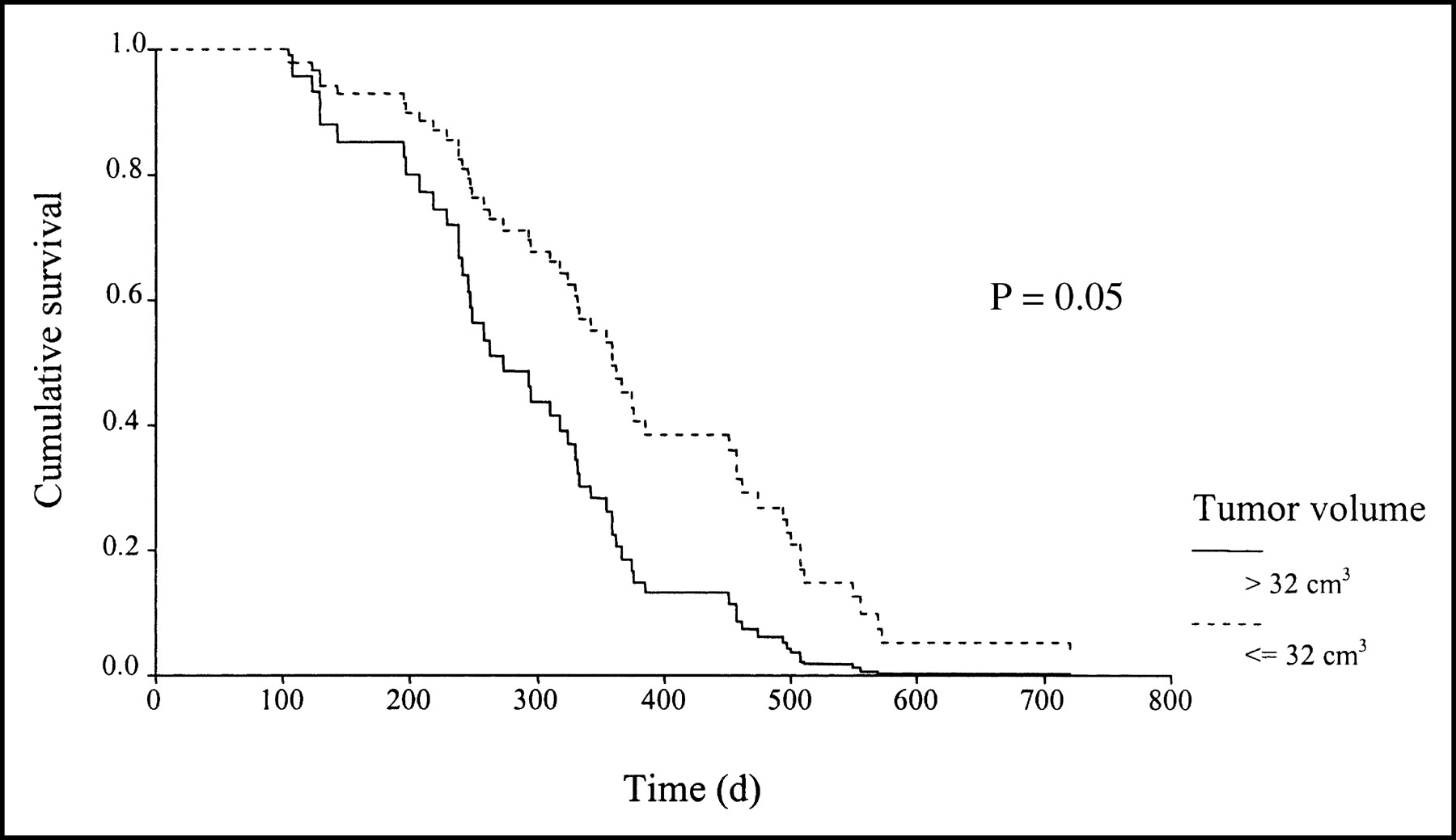
Cumulative survival according to tumor volume at the end of radiotherapy. The graph represents the cumulative MST (according to tumor volume) of the population at the end of radiotherapy. Patients with a tumor volume < 32 cm3 had an MST of 358 d, vs. 238 d in patients with a tumor volume ≥ 32 cm3.
Univariate and Multivariate Analyses of the Effect of Prognostic Factors on Survival
When a multivariate analysis was performed using the Cox proportional hazards model, age, complete tumor resection, KPS score, and MTV were found to be strongly predictive of survival (P = 0.002, 0.03, 0.001, and 0.02, respectively) (Table 2). The potential interactive effect between the type of surgery and the MTV was also analyzed and was not found to be statistically significant (P = 0.49). An MTV superior or equal to 32 cm3 significantly reduced a patient’s survival when adjusted for age, KPS score, and complete tumor resection. Approximately 50% of CT scans obtained within the first 10 d after radiation therapy were classified as showing doubtful or suggestive findings. As a consequence, no useful information was provided by this test for the management of these patients after a complete course of radiation therapy.
DISCUSSION
Treatment efficacy in malignant glioma studies is evaluated by neuroimaging. Conventional MRI and CT assess morphologic parameters such as changes in tumor size and contrast enhancement. However, changes in size and alterations in blood–brain barrier properties (after therapy) not only reflect therapeutic efficacy but also can represent nonspecific inflammatory reactions due to irradiation, tumor necrosis, or postoperative enhancement along the resection margins (12–15). Functional imaging methods have been proposed for the evaluation of treatment efficacy and are claimed to be more specific than are conventional radiologic investigations (16). SPECT or PET assesses tumor viability by specific intracellular uptake by the cells in malignantly transformed populations (17–21). 201Tl SPECT has an accuracy similar to that of 18F-FDG PET, which is also used to distinguish between brain tumor recurrences and radiation necrosis (5,22). 99mTc-MIBI is used as an alternative to 201Tl for the study of myocardial perfusion and has also been proposed as an imaging agent for tumors in breast, lung, and brain cancer and in melanoma and lymphoma (4,6,7,19,22). In these cases, MIBI brain SPECT has shown more specificity and sensitivity than has 201Tl brain SPECT (8). 99mTc-MIBI concentrates in mitochondria by active diffusion because of an increased negative transmembrane potential (18)—an advantage over 18F-FDG, which can be found in the inflamed area. Because there is no reason for MIBI uptake in nonvital tissues, 99mTc-MIBI brain SPECT can be used to evaluate tumor viability and therapeutic response in malignant glioma patients (7).
Malignant glioma is difficult to cure and leaves few long-term survivors (1–3). Early detection of treatment failure would benefit the patient; for example, a new aggressive therapy (reoperation, radiosurgery, brachytherapy, or chemotherapy) could be used in patients with the worst prognosis. Alternatively, therapeutic abstention or palliative treatment could also be considered. Neuroimaging evaluation during treatment is warranted to identify the causes of clinical deterioration such as true tumor progression, development of hydrocephalus, or other mass effects (16). Clearly, functional neuroimaging gives relevant information for efficacious clinical decisions. To the best of our knowledge, ours was the first demonstration that this functional imaging, 99mTc-MIBI brain SPECT, at the end of radiotherapy can predict survival of malignant glioma patients. To evaluate malignant glioma treatment, MRI is more sensitive than CT (many CT findings are negative or doubtful, and when they are positive, survival time is short). However, MRI may be difficult to interpret because of artifacts resulting from previous treatments and does not offer a better window on tumor viability. Hence, at the end of radiation therapy we were able to show that 99mTc-MIBI brain SPECT could help to establish patient prognosis early, while taking into account the other recognized prognostic factors: patient age, KPS score, and complete tumor resection (1–3). The initial question was to determine whether tumor volume could predict survival after radiotherapy. Our study showed that for the higher volumes (>32 cm3), survival time is significantly poor. We assessed other groups, but for lower volume there was not a linear relationship between tumor volume and survival time. Our results confirmed that the conventional radiologic tool (CT) does not allow the diagnosis of tumor progression, nor does it help neurooncologists in establishing patient survival. Of the 8 patients with negative CT findings, only 2 had negative findings when studied with 99mTc-MIBI brain SPECT. Of the 26 patients with doubtful or suggestive CT findings, tomography findings were negative in 1 and positive in the remaining 25. For these 34 patients, tumor resections were performed; 24 had complete tumor resections and 10 had incomplete tumor resections. These patients are usually considered to be good responders to therapies and are likely to have prolonged survival. An early and reliable assessment of individual prognosis, especially for patients who undergo tumor resection, is essential and warranted. These therapeutic strategies could be adapted for each patient to improve survival and quality of life. No previous studies have looked for a correlation between survival time and findings on brain SPECT using 99mTc-MIBI as the radiotracer. Other studies have used 201Tl brain SPECT and have assessed the utility of this tomoscintigraphy for predicting survival after treatment of brain tumor patients. Vertosick et al. and Kosuda et al. showed an inverse relationship between 201Tl uptake at reoperation and survival time (23,24). Schwartz et al. investigated the utility of dual-isotope brain SPECT in the identification of tumor recurrence and found a correlation between radioisotope uptake and the histologic characteristics of the tumor at reoperation (25). In another study, Schwartz et al. showed that in patients treated for malignant gliomas, uptake ratios for 201Tl/99mTc-hexamethylpropyleneamine oxime brain SPECT were more strongly associated with survival at 1 y than was tumor histologic type at reoperation or time from the initial surgery to recurrence (26). The purpose of our study was different; however, our results confirm the interest in and utility of using 99mTc-MIBI brain SPECT for following up malignant glioma patients.
CONCLUSION
99mTc-MIBI brain SPECT may help in determining the survival of glioma patients at the end of radiation therapy. Consequently, the management of patients can be adapted.
Footnotes
Received May 27, 2003; revision accepted Oct. 23, 2003.
For correspondence or reprints contact: Patrick Beauchesne, MD, PhD, Neuro-Oncologie, Neurologie, CHU de Nancy, Hôpital Central, CO no. 34, 54035 Nancy Cedex, France.
E-mail: beauchesneP{at}wanadoo.fr





{kind=link}