


Abstract
The high sensitivity of the thyroid gland to the carcinogenic effects of radiation during childhood contrasts with the absence of demonstrable carcinogenic effects of radiation in adults. To better understand these age-related variations, we studied follicular morphometry, functional status, and proliferative activity in 31 thyroid glands removed from relatives of medullary thyroid carcinoma patients, with ages ranging from 3 to 39 y. Methods: The mean follicular diameter (MFD) was estimated, and immunohistochemistry was performed with antibodies directed to molecules involved in iodide transport (Na+/I− symporter [NIS], pendrin, and apical iodide transporter), in organification (thyroperoxidase [TPO] and Duox), in cell cycle and growth (Ki-67, cyclin A and D1, and galectin-3), and in angiogenesis (vascular endothelial growth factor and nitric oxide synthase III [NOSIII]). Results: Compared with older patients, patients who were ≤12 y old had a smaller MFD (P < 0.001) and more frequently positive NIS, pendrin, and Duox (P < 0.01). Proliferation rate as indicated by cyclin A expression was also higher in patients < 12 y (P < 0.01) but peaked at the time of puberty. Staining for NIS, pendrin, TPO, Duox, and NOSIII was stronger in thyroid glands with a smaller MFD (P < 0.001). On multiple tests adjusted for age and thyroid mass, TPO, Duox, and NOSIII remained significantly correlated to MFD (P < 0.001), whereas staining for NIS and pendrin did not. This finding suggests that NIS and pendrin expression is related mainly to the age of the patient. Conclusion: Smaller follicles with a higher expression of proteins involved in iodide metabolism were found in younger children. In cases of radioiodine contamination in children, the result will be a higher radioactive concentration and, hence, higher radiation doses. This event may induce the development of thyroid cancer under conditions of accelerated proliferation, as evidenced at puberty.
A strong relationship has long been shown between exposure to external radiation during childhood and the risk of thyroid tumors (1,2). More recently, the increase in cancer incidence caused by the nuclear accident at Chernobyl has been restricted to the thyroid (3). This finding is related to the enormous amounts of iodine radioisotopes released from the nuclear reactor and the great efficacy of the thyroid gland in concentrating iodine (4), resulting in high radiation doses to the thyroid.
The risk of thyroid carcinoma is restricted to patients exposed during childhood to either external or internal radiation: The risk is maximal during the first years of life, decreases with increasing age at exposure, and is not significant in adults. This great change in sensitivity with age at radiation exposure is not yet fully explained (3,5).
In cases of exposure to radioiodine, the mean radiation dose to the thyroid is related to the radioactive concentration in the thyroid, that is, the ratio between total thyroid uptake and thyroid mass. The total thyroid uptake is similar in children and in adults, but the normal thyroid mass is 1 g at 1 y old, 5 g at 5 y old, and 15–20 g in adulthood (6). Thus, contamination leads to a much higher radioactive concentration and, hence, radiation dose in children than in adults, explaining in part the higher risk of thyroid cancer in children. The absence of an association between medical 131I exposure and the risk of thyroid cancer may be related to the low numbers of young children evaluated. Such low numbers do not permit any conclusions to be made about radiation exposure at a young age (7,8).
The influence of age was also observed after exposure to external radiation, confirming that age at exposure by itself has paramount importance in the sensitivity of the thyroid to the carcinogenic effects of radiation (9). This observation was attributed to cell proliferation, which favors the accumulation of genetic defects. Indeed, thyroid cell proliferation is active during childhood but is reduced in adulthood (10).
A marked morphologic and functional heterogeneity in the thyroid gland has been found by autoradiography techniques (11) and secondary ion mass spectrometry (12–13). These techniques have found active areas with a high iodine concentration, characterized by a predominance of smaller follicles with tall thyrocytes, and hypofunctioning areas with a low iodine concentration, characterized by larger follicles and flattened thyrocytes. These observations parallel the results of immunohistochemical studies showing a stronger expression of proteins belonging to the thyroid iodine pathway in small follicles (14–20).
Whether the morphologic and functional status of the thyroid changes with age remains to be documented. The present study was performed to investigate the follicular morphology, functional status, and growth pattern of normal human thyroid tissue obtained at various ages.
Because functional heterogeneity may be responsible for a heterogeneous dose distribution among follicles, with higher radiation doses to more active follicles, a second part of the study (to be reported in a separate publication) used these data for dosimetry estimates.
MATERIALS AND METHODS
Patients
Thirty-one patients, 17 male and 14 female, who belonged to families with hereditary medullary thyroid carcinoma and underwent a prophylactic thyroidectomy at the Institut Gustave Roussy between 1983 and 2001 were selected for the study. At surgery, 3 patients were less than 5 y old, 6 were 5–9 y old, 4 were 10–12 y old, 4 were 13–16 y old, 4 were 17–20 y old, 5 were 21–30 y old, and 5 were 31–39 y old. The median mass of the thyroid gland was 7 g (range, 1–12 g).
Germinal RET gene mutation was evidenced in 25 patients belonging to 24 families, including a 634 codon mutation in 14 patients, a 618 mutation in 3, a 918 mutation in 3, a 620 mutation in 2, and a 611, 638, or 790 mutation in 1 patient each. In the remaining 6 patients, a pentagastrin stimulation test disclosed stimulated calcitonin levels > 100 ng/L that led to prophylactic thyroidectomy. Sequencing of exons 10, 11, 13, 14, 15, and 16 was negative in 2 patients and was not performed for the other 4 patients, who underwent surgery before 1988. The histologic examination disclosed medullary thyroid carcinoma in 22 patients. According to the TNM classification (21), 15 tumors were stage I (T1, N0), 4 were stage II (T2, N0), and 3 were stage III (T1, N1; T2, N1; and T3, N1, respectively). Only C-cell hyperplasia was found in the other 9 patients. At the time of surgery, all patients had a normal serum thyroid-stimulating hormone level, none was treated with thyroid hormone, and all lived in an iodine-sufficient area. By light microscopy observation, 3 Duboscq-Brasil–fixed, paraffin-embedded tissue sections were selected for each thyroid sample, on the basis of absence of medullary thyroid carcinoma foci. Indeed, the follicular thyroid tissue selected had a normal appearance on light microscopy. This study was performed in accordance with protocols previously approved by the local human studies committee.
Morphometric Analysis
For estimating the follicular diameter and its variations within the thyroid gland, follicles were considered spheric and both thyroid lobes were considered similar.
For each patient, 2 microscopic pictures (magnification, ×142) were printed for each of 3 sections. The main diagonal line was drawn from the bottom left corner to the upper right corner of the picture (Fig. 1). Then, the major axis of all follicles crossed by or tangent to the main diagonal line was measured.

Paraffin-embedded human thyroid tissue stained with hematoxylin–eosin–safranin (original magnification, ×142): morphologic aspect. The major axis of each follicle crossed by or tangent to the diagonal was measured.
In total, 2,661 follicular diameters were measured. For each patient, 58–130 diameters were measured. Because we did not know where the follicles were cut by the sampling, the method underestimated some follicular diameters, but comparisons between thyroid samples were still possible because of the large number of measurements.
Immunohistochemistry
Tissue sections of 4 μm were initially freed of paraffin by serial passages through xylene and alcohol. Endogenous peroxidase activity was quenched by incubation in 0.03% hydrogen peroxide and in 0.1 mol/L Tris-HCl buffer 1X (pH 7.6) for 5 min. Subsequently, microwave/pressure cooker pretreatment (3 cycles of 5 min each) was performed in 1 mmol/L ethylenediaminetetraacetic acid buffer (pH 8). Sections were then incubated for 30 min at room temperature with anti–Na+/I− symporter (NIS) (1:25 dilution, polyclonal antibody (15)), antipendrin (1:50 dilution, polyclonal antibody (17)), anti–apical iodide transporter (AIT) (1:25 dilution, polyclonal antibody (19)), antithyroperoxidase (TPO) (1:4 dilution, monoclonal antibody; Biocytex), anti-Duox (1:50 dilution, polyclonal antibody (18)), antigalectin-3 (1:50 dilution, monoclonal antibody; Novocastra), anti–Ki-67 (1:75 dilution, monoclonal antibody MIB-1; Dako Corp.), anticyclin D1 (1:50 dilution, monoclonal antibody; Novocastra), anticyclin A (1:25 dilution, monoclonal antibody; Novocastra), anti–vascular endothelial growth factor (VEGF) (1:25 dilution, polyclonal antibody; Santa Cruz Biotechnology, Inc.), and anti–nitric oxide synthase III (NOSIII) (1:75 dilution, polyclonal antibody; Transduction Laboratories) antiserum. They were washed 3 times in Tris-HCl 1X buffer for 5 min each time and incubated with a peroxidase-conjugated antibody for 15 min (peroxidase antimouse/rabbit En Vision System; Dako Corp.). After 3 additional washes, peroxidase staining was revealed in diaminobenzidine tetrahydrochloride (Polysciences Inc.) with 0.1% hydrogen peroxide, in Tris buffer, 0.01 mol/L (pH 7.2). Sections were counterstained with hematoxylin, dehydrated, mounted, and examined under a microscope. For negative controls, incubation with the primary antibody was omitted.
Immunohistochemical Evaluation
The immunohistochemical results were scored semiquantitatively by light microscopy. The intensity of staining was scored as no staining (−), weak staining (+), moderate staining (++), or strong staining (+++). The percentage of stained thyroid cells was scored as no stained cells (−), staining in less than 25% of cells (+), staining in 25%–50% of cells (++), staining in 50%–75% of cells (+++), or staining in more than 75% of cells (++++). Proliferation rate was determined by counting positive thyrocyte nuclei in 10 high-power fields using either the anti–Ki-67, anticyclin D1, or anticyclin A antibody. Staining for galectin-3 was also quantified.
Statistical Analysis
Statistical analysis was performed using SAS software (2000 update; SAS Institute Inc.). Continuous data were described using median and range. Mean follicular diameter (MFD) was estimated for each patient using least-squares means of measured follicular diameters, in a mixed model for repeated measurements. Explanatory factors were age, sex, and thyroid mass at surgery. Age was entered in the model as a categoric factor. Differences between least-squares means were tested using the Tukey adjustment for multiple tests. Immunohistochemical data were described using median and range, and the association with age was tested using the χ2 test or Fisher exact test. The association between immunohistochemical data and MFD was evaluated in a mixed model for repeated measurements. The Spearman rank coefficient was computed to correlate proliferation rate with age and MFD.
RESULTS
Morphometric Analysis
Follicular diameters ranged from 30 to 840 μm, with a median value of 130 μm. Smaller follicles (diameter < 100 μm) were prevalent in patients ≤ 12 y old, and larger follicles (diameter > 200 μm), in older patients (P < 0.001) (Fig. 2).

Distribution of follicular diameters according to age at surgery. Smaller follicles (<100 μm in diameter) are prevalent in patients ≤ 12 y old, and larger follicles (>200 μm in diameter), in older patients.
MFD was smaller in patients ≤ 12 y old than in older patients and in male patients than in female patients (Table 1). As expected, MFD significantly correlated with thyroid mass (P < 0.001). The association between smaller MFD and younger age remained significant after adjustment for sex and thyroid mass (Table 1). Among patients ≤ 12 y old, MFD was smaller in the 3 who were less than 5 y old (P < 0.01).
Statistical Models for Morphometric Measurements
Immunohistochemical Analysis of Proteins Involved in the Iodine Pathway
As expected, NIS localized in the basolateral membrane of the thyrocytes, and pendrin, AIT, Duox, and TPO localized in the apical membrane. There was also a cytoplasmic staining for TPO.
NIS, pendrin, TPO, and Duox were preferentially expressed in small follicles and tall thyrocytes, resulting in a significant correlation with small MFD (P < 0.001). In positively staining cells, the staining intensity for NIS and pendrin was strong in all thyroid specimens, whereas the staining intensity for TPO and Duox varied among samples and significantly correlated with small MFD (P < 0.01). AIT staining was moderate and similar in both tall and flattened cells.
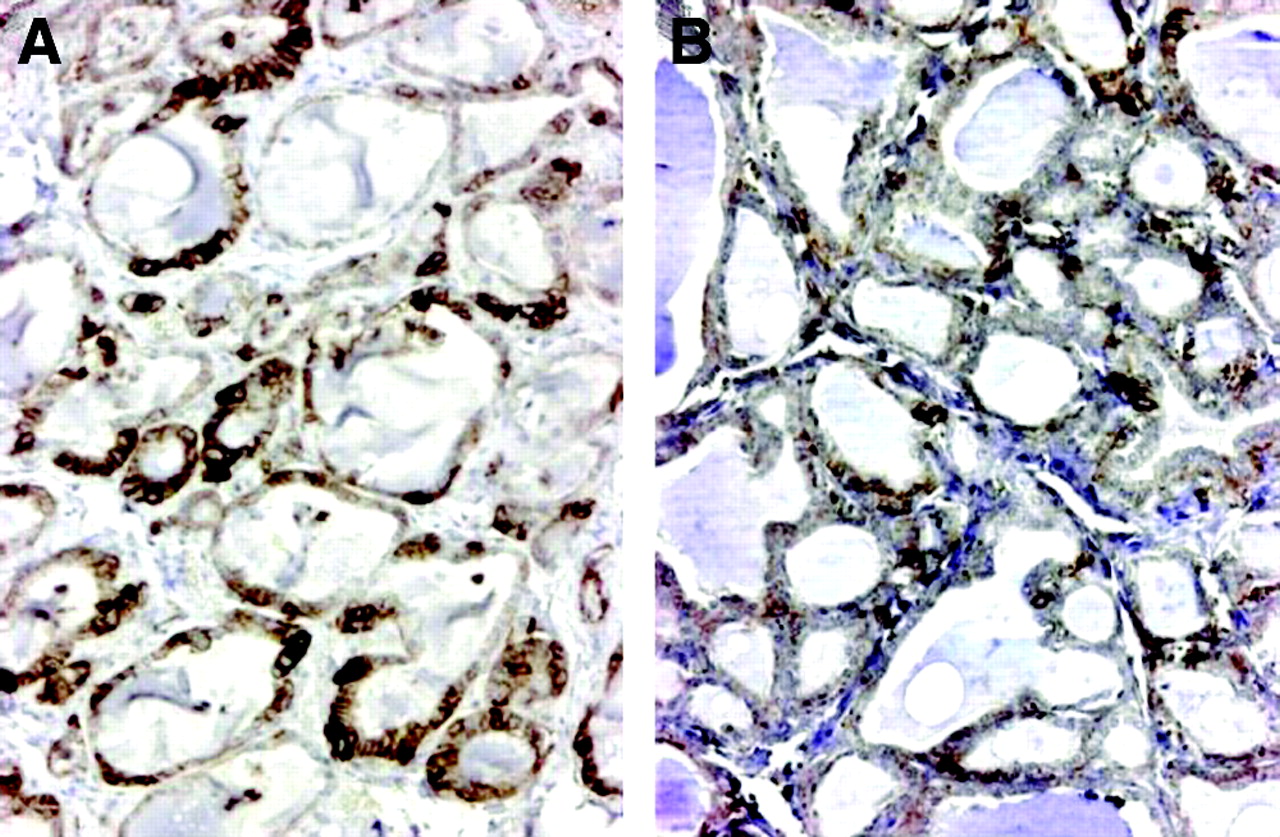
From one patient to another, the percentage of cells staining for NIS ranged from <25% to >75%, whereas staining was less heterogeneous for the other functional proteins (Table 2). The proportion of thyroid cells and follicles staining for NIS (Fig. 3), pendrin, and Duox was higher in patients ≤ 12 y old than in older patients, whereas staining for AIT and TPO did not significantly vary with age (Table 2).
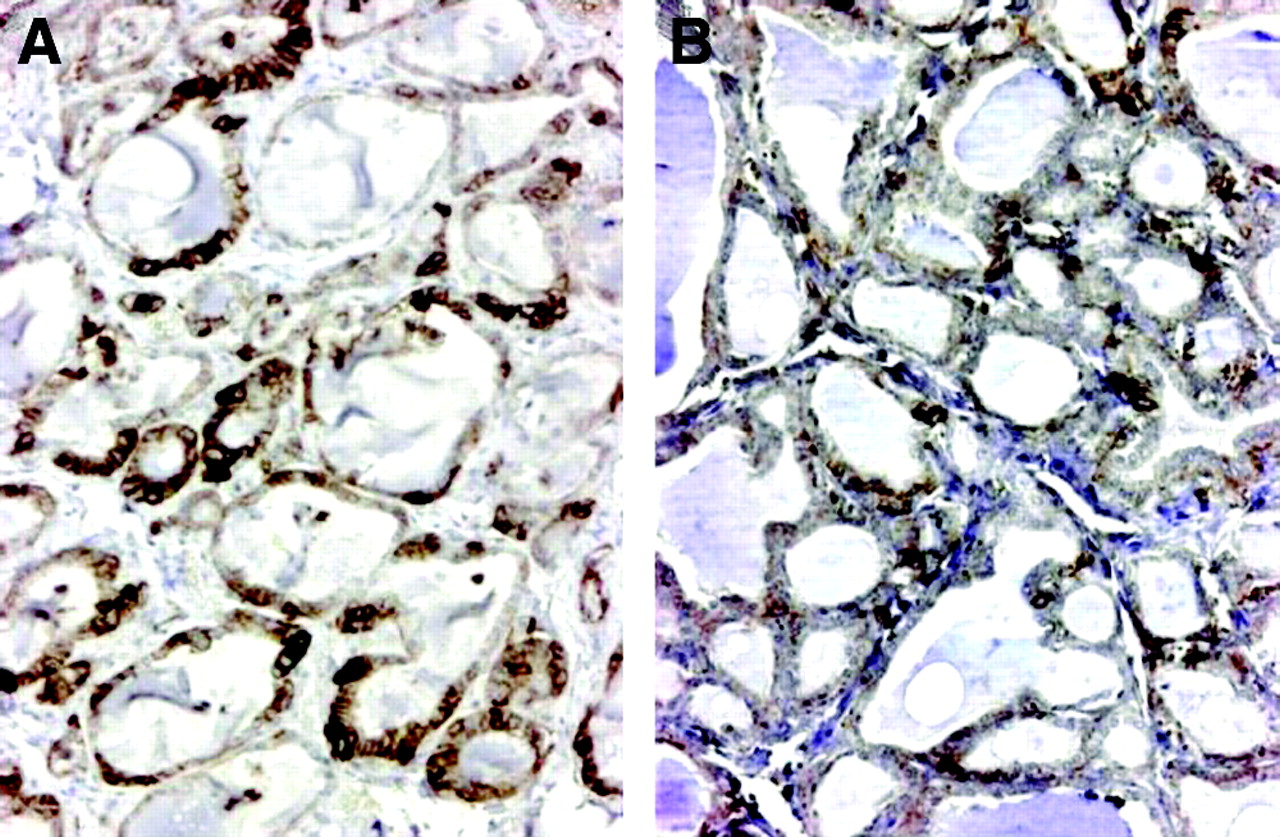
Immunohistochemical expression of NIS in thyroid tissues according to age at surgery (original magnification, ×100). (A) Strong staining is seen in the majority of follicles of an 8-y-old patient. In some smaller follicles, all thyrocytes are stained. (B) Strong staining is seen in a few small follicles of a 17-y-old patient; in positive follicles, only single or a few thyrocytes are stained.
Immunohistochemical Data According to Age at Surgery
Immunohistochemical Analysis of Proteins Involved in Cell Growth
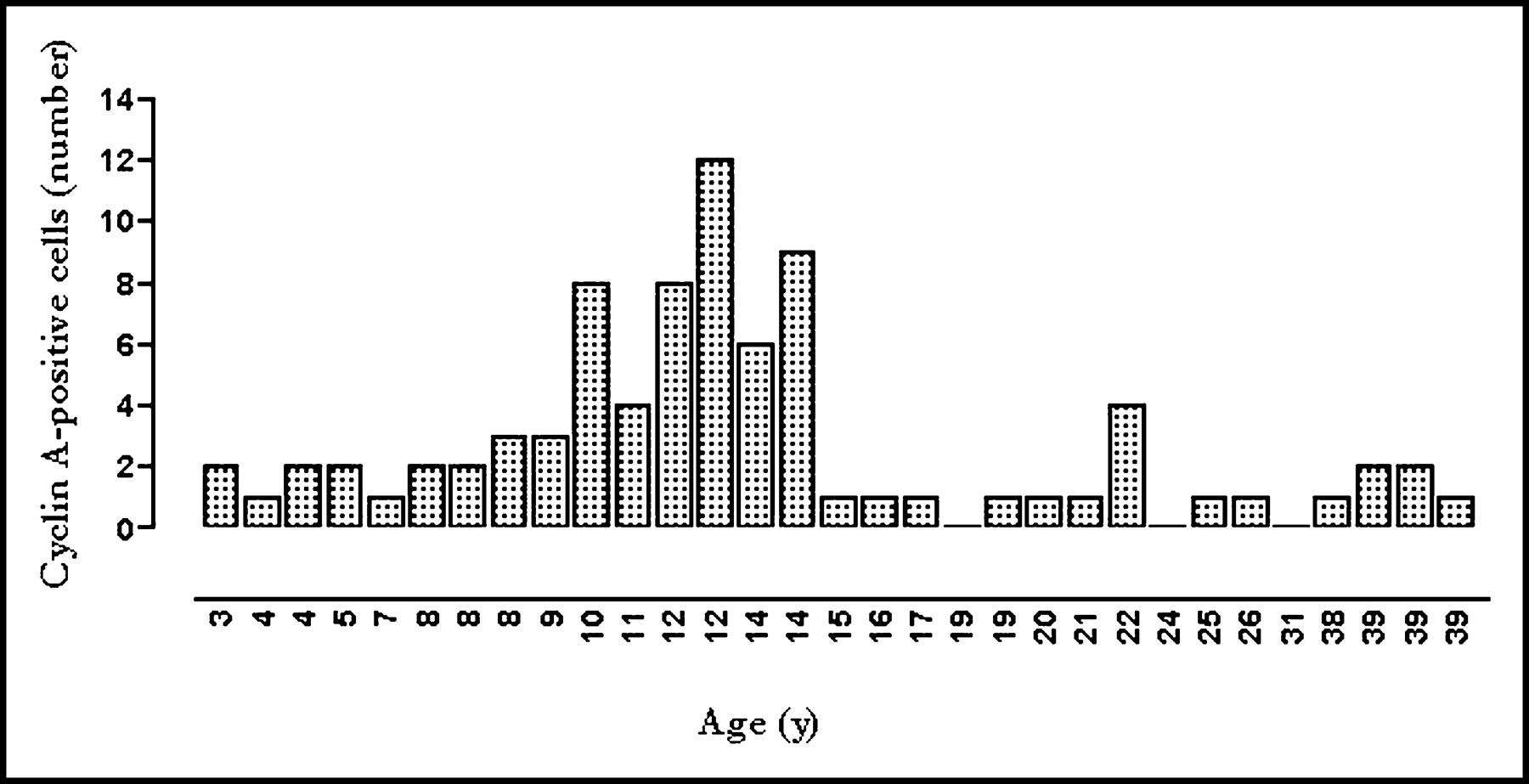
The proliferation rate, as indicated by the number of cyclin A–positive thyrocytes per 10 high-power fields, was significantly higher in patients ≤ 12 y old (P < 0.01) and peaked in patients between 10 and 14 y old (Fig. 4). No significant staining was found for Ki-67 and cyclin D1 in normal thyrocytes. Similarly, no galectin-3 staining was found in normal thyrocytes.
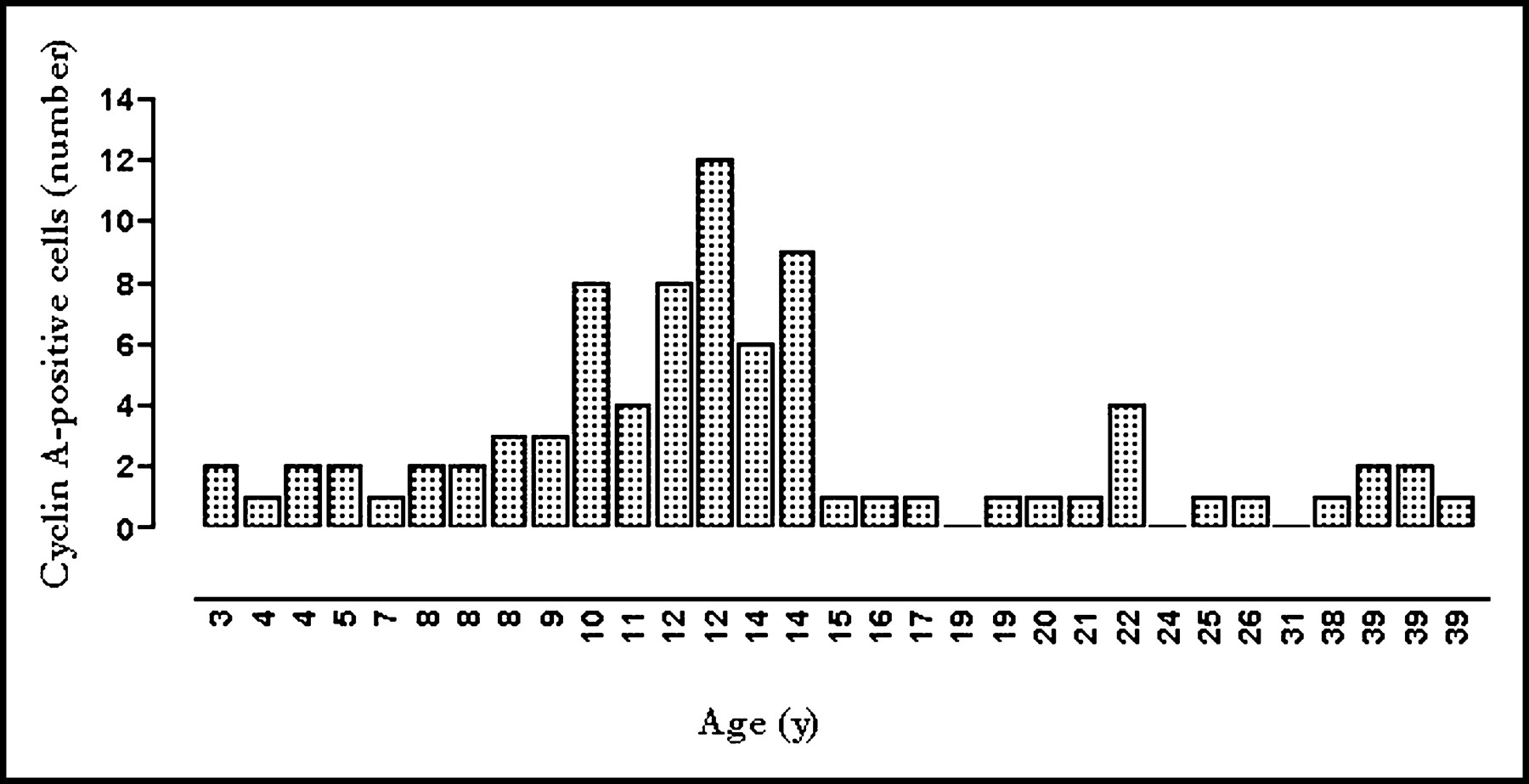
Age distribution of thyroid cell proliferation rate, as estimated by the number of cyclin A–positive thyrocytes per 10 high-power fields.
Some macrophages, fibroblasts, and endothelial and smooth muscle cells of vessels were stained for cyclin A and galectin-3.
Immunohistochemical Analysis of Angiogenic and Vasoactive Factors
A weak VEGF immunostaining was observed in almost all thyrocytes and follicles, regardless of their functional status. VEGF staining was diffuse in the cytoplasm. NOSIII staining was localized in the cytoplasm at the perinuclear level, displaying a granular pattern of distribution. NOSIII stained preferentially and more strongly small follicles with tall thyrocytes, and NOSIII staining correlated with small MFD (P < 0.01). No age-related difference was found for either VEGF or NOSIII expression.
VEGF staining was also detected in smooth-muscle cells of vessels, whereas endothelial cells were negative for both VEGF and NOSIII.
Relationships Between Morphometric and Immunohistochemical Studies
Because staining was related to both MFD and the age of the patient, the Tukey adjustment for multiple tests was performed. After adjustment for age and thyroid mass, the correlation between smaller MFD and higher proportion of thyrocytes expressing Duox, TPO, and NOSIII remained significant (P < 0.001). In contrast, the correlation between MFD and staining for NIS and pendrin did not remain significant, indicating that NIS and pendrin expression is principally related to the age of the patient. Neither MFD nor expression of iodide transporters was correlated with proliferation activity.
DISCUSSION
The present study shows that thyroid tissue is morphologically more active in childhood than in adulthood and overexpresses functional proteins. The follicular epithelium of thyroid tissues used in this study was considered normal, because to our knowledge, no effect of familial C-cell disease on thyrocytes has ever been reported. Also, patients were euthyroid as shown by a normal thyroid-stimulating hormone level at surgery, they were not treated with thyroid hormone, they lived in an iodine-sufficient area, and thyroid tissue appeared normal on light microscopy.
Autoradiography techniques, secondary ion mass spectrometry, and immunohistochemical studies have demonstrated an important morphologic and functional heterogeneity among follicles and among thyrocytes inside a given follicle (11–20). The current study clarifies that smaller follicles, lined by tall thyrocytes and considered active, strongly express proteins involved in the iodine pathway, and larger follicles, lined by flattened cells and considered hypofunctioning, exhibit absence of or weak staining for these proteins.
In children, follicles were smaller on average, with a higher proportion of small follicles (30–100 μm in diameter) and intermediate follicles (100–200 μm in diameter). This finding indicates that thyroid activity inversely correlates with age, as follicles smaller than 100 μm are considered active and those larger than 200 μm are considered hypofunctioning. In line with this observation was our finding that NIS, pendrin, TPO, and Duox staining was positive in the majority of thyrocytes of small follicles. NIS and pendrin expression was independently associated with younger age, regardless of other factors such as follicular size or thyroid volume. This may indicate that iodide transport mechanisms are more active in the thyroids of younger patients. On the other hand, the relationship between Duox and MFD remained significant, even after adjustment for age, indicating that Duox expression is related to the functional status of the follicle. Finally, TPO and AIT expression was not related to age at surgery.
The possible relationship between the expression of some angiogenic factors and age was also studied. VEGF expression appeared weakly but diffusely distributed in all follicles and was not related to their functional status. The increased NOSIII expression in small active follicles, in line with previous reports (20), suggests that this vasoactive factor, responsible for nitric oxide synthesis, participates in the local regulation of follicular activity by modulating blood flow.
The age-related changes in thyroid tissue may be the biologic basis of the greater thyroid activity during childhood than in adulthood that results in a similar thyroid uptake in a much smaller gland and, consequently, in a higher mean radioactive concentration and, finally, in a higher mean radiation dose. Indeed, NIS and Duox are the 2 proteins controlling the main limiting steps of iodine metabolism, NIS being responsible for the active iodide uptake from blood into the thyrocyte and Duox for the generation of H2O2, the limiting factor for iodide organification (15,16,18). Furthermore, the dose distribution at the follicular level may be related to the functional activity of the follicle and to its size and hence may be different between children and adults. The present biologic data will be used to test this hypothesis in mathematic models.
Thyroid cell proliferation, by exposing cells in active replication to mutational events, may be an important factor in the sensitivity of the thyroid to the carcinogenic effects of radiation. Thyrocytes have been estimated to undergo a total of 6–7 mitoses during a life span (6), explaining the scarce proliferation rates detected in the current study. The higher rate of cyclin A–positive thyrocyte nuclei observed in children than in adults appears to be an age-related factor not influenced by follicular activity. However, the age distribution in childhood showed the highest rates of cyclin A–positive thyroid cells at the time of puberty. This finding may be related to the hormonal changes of puberty but contrasts with the age-related sensitivity to radiation, which is maximal in children who are ≤5 y old at the time of radiation exposure (1,2,3,5). One possibility is that the increased growth rate at puberty facilitates the occurrence of a thyroid tumor in previously irradiated cells carrying the radiation-produced lesions, such as a RET/PTC rearrangement (rearranged in transformation/papillary thyroid carcinomas) (22). This may explain why the incidence of thyroid cancer is extremely low before the age of 10 y, even in children exposed to radiation, and why the incidence increases gradually after the age of 10 y. This hypothesis is in agreement with the model of radiation-induced thyroid carcinogenesis in rats, in which mutational lesions acquired by radiation are clinically silent and result in thyroid carcinoma development only under proliferative conditions (23).
CONCLUSION
To our knowledge, this study was the first to find an age-related variability in the morphofunctional status of the thyroid gland, with smaller follicular size and higher expression of the proteins involved in iodine transport in younger children. This study also evidenced a higher proliferation rate at peripubertal age. The accelerated proliferation may explain the increasing occurrence of thyroid cancer in pubertal children who were previously irradiated. The morphofunctional ability of the thyroid of children to concentrate iodine may, by increasing the radiation dose to the thyroid, favor carcinogenic processes. The possibility of accurately measuring the follicular activity of a given thyroid will be helpful in elaborating models to calculate the dose delivered by radioactive iodine isotopes at the follicular level.
Acknowledgments
This study was supported by grants RB 2001-08 and RB 2002-15 from Electricité de France and by a grant from the Italian Society of Paediatric Endocrinology and Diabetology.
Footnotes
Received Jul. 28, 2003; revision accepted Oct. 8, 2003.
For correspondence or reprints contact: Martin Schlumberger, MD, Nuclear Medicine Department, Institut Gustave-Roussy, 39 rue C. Demoulins, 94805 Villejuif Cedex, France.
E-mail: schlumbg{at}igr.fr
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Initial Management and Follow-up of Differentiated Thyroid Cancer in Children
- Understanding the Relationship Between Age and Thyroid Cancer
- Total Thyroidectomy and Adjuvant Radioiodine Treatment Independently Decrease Locoregional Recurrence Risk in Childhood and Adolescent Differentiated Thyroid Cancer
- Juvenile differentiated thyroid carcinoma and the role of radioiodine in its treatment: a qualitative review