


Abstract
Experience in our and other institutions with PET/CT imaging of lung and head and neck cancers has shown that this new modality has higher specificity and sensitivity than PET alone and in certain settings even when compared to PET and CT viewed side by side. The largest experience exists with non-small cell lung cancer (NSCLC), in which it has been demonstrated that PET/CT is superior to PET and CT in T and in N staging. Superiority in M staging has yet to be demonstrated. CT contrast media enhancement is probably only necessary when a substantial mediastinal tumor component is present. In such cases, delineation of tumor from vascular structures is relevant. In ENT tumors, PET/CT also appears to be superior to PET, and probably also to PET and CT viewed side by side. Early information suggests that contrast media enhancement for staging may not be required, but the data available is still limited. In both settings, it is interesting to note that in a number of patients, second metachronous tumors are discovered with PET/CT, mainly localized in the GI tract.
We know already from the “old times” in medical imaging, that in diagnosing bone lesions, bone scanning provides sensitivity, while conventional x-rays provide specificity. The relation of PET and CT is similar to this in both imaging of the chest and the head and neck for tumor staging. 18F-FDG PET finds the lesions, and CT frequently helps to specify what is seen. For example, an unclear focus near the thoracic wall on PET can be identified readily as a rib fracture on CT. Precise identification and localization of a lesion are frequently decisive, and many patients undergo surgical treatment after PET and CT examinations. Therefore, the availability of coregistered images is useful and sometimes essential. As experience with integrated PET/CT increases, the prime question appears less and less to be: When do we need PET/CT? Instead, more frequently the question is: How much PET and how much CT do we need in a PET/CT examination? There is no question that we need a relatively high-resolution, high-sensitivity PET scanner for tumor imaging. But we are also learning that, for many situations, a low-dose unenhanced CT scan as part of a PET/CT examination is good enough to yield all the necessary information. FDG is indeed an excellent “x-ray” contrast agent! However, it is not clear as yet whether and in which settings of tumor imaging a full contrast-enhanced CT yields better results than an unenhanced CT examination.
In addition to the usefulness of PET/CT in clinical diagnosis, the obvious technical advantages of PET/CT have made this technology a resounding success. Among these advantages is CT-based attenuation correction, which leads to patient throughput increases of approximately 25%, thereby creating a substantially more efficient system.
LUNG CANCERS
Lung cancers are probably the best staging indication for PET, and important data on the use of PET/CT in lung cancers have been accumulated. In our experience, PET/CT offers several advantages in patients with lung cancer, some of which may also be advantages of PET/CT in imaging other cancers. Among the diagnostic advantages are: exact demarcation of the primary tumor, enabling diagnosis of tumor invasion into adjacent tissue; exact demarcation of tumor in atelectasis; precise localization of mediastinal lymph-node metastases <8 mm in size; and precise localization and classification of extrathoracic lesions, even when no morphologic changes are identified with CT.
PET/CT also offers advances in surgical management, including: the ability to guide surgical mediastinal biopsy to small lymph-node metastasis, thus improving the accuracy of surgical mediastinal staging; and the ability to guide biopsy of extrathoracic metastasis, thus reducing anatomic misses.
PET/CT offers a number of advantages in radiation therapy, including reduced risk of geographic misses; a minimized dose of ionizing radiation to nontarget organs; definition of radiation treatment field of tumor in atelectasis; and improved volume delineation as a result of a decrease in interobserver variability.
Economic and cost-saving advantages of PET/CT include: exclusion of unnecessary examinations for clarification of unclear findings; and the avoidance of ineffective surgery and radiation therapy.
Non–Small Cell Lung Cancer
The majority of PET imaging work has been performed in non–small cell lung cancer (NSCLC). It has been shown that 18F-FDG PET is highly accurate in classifying lung nodules as benign or malignant. Whole-body PET improves the rate of detection of mediastinal lymph-node metastases as well as extrathoracic metastases, when compared with conventional imaging methods such as CT, MR, ultrasound, or bone scan (1–2). Because commercial PET scanners provide nominal spatial resolution of 4.5–6 mm in the center of the axial field of view, even lesions <1 cm in size with an increased 18F-FDG uptake can be detected. This represents a critical advantage of PET over CT and MR. Integrated PET/CT enables the exact matching of focal abnormalities on PET to anatomic structures on CT (3–5).
T Staging
Without image fusion, the use of PET in T staging lung cancer is limited. Recently, we have shown that integrated PET/CT is superior to CT alone, PET alone, and visual correlation of PET and CT in T staging of patients with NSCLC (3). Because of the exact anatomic correlation of the extent of 18F-FDG uptake, the primary tumor can be precisely delineated (Fig. 1). Therefore, the assessment of chest-wall infiltration and mediastinal invasion by the tumor is improved. However, integrated PET/CT imaging is not perfect in the diagnosis of tumor invasion. It might be difficult to distinguish accurately contiguity of tumor from direct tumor invasion. However, in our series of patients, integrated PET/CT imaging was statistically superior to other imaging modalities (3). It has been shown that 18F-FDG PET is a useful tool for differentiation between tumor and peritumoral atelectasis. This is particularly important for radiotherapy planning in patients with lung cancer associated with atelectasis. The information provided by 18F-FDG PET results in a change in the radiation field in approximately 30%–40% of patients (6). With integrated PET/CT-based radiotherapy planning, the radiation field can be exactly defined. The dose of ionizing radiation to nontarget organs can be minimized, and the risk of geographic misses can be reduced. It has been shown that integrated PET/CT improves the volume delineation of the radiation field because of the increase in interobserver variability (7).

Lung carcinoma in upper right lung with ipsilateral mediastinal lymph-node metastasis. (A) Transverse PET. (B) Transverse CT. (C) Integrated transverse PET/CT image of upper thorax. Integrated PET/CT imaging ruled out tumor invasion of thoracic wall.
N Staging
PET has proven to be a very effective staging modality for mediastinal nodal staging. CT and MR imaging are limited in depicting small mediastinal lymph-node metastases, because they predominantly provide anatomic information. Several studies have demonstrated that 18F-FDG PET is significantly more accurate than CT in determining nodal status (1,8–10). Exact localization of focal abnormalities to specific lymph nodes by PET alone is difficult or even impossible because of the poor anatomic information provided (Fig. 2). The presence and site of lymph-node metastases should be recorded according to the revised American Thoracic Society lymph-node station-mapping system. In patients with bulky mediastinal disease or multilevel nodal involvement, the assessment of N stage is easy. The difficulty of conventional PET is in localization of small single nodes, particularly in a patient with a mediastinal shift as a result of atelectasis or anatomic variants. The exact localization of a single lymph-node metastasis in the hilus is difficult as well. Lymph nodes distal to the mediastinal pleural reflection and within the visceral pleura are classified as N1 nodes. Lymph nodes within the mediastinal pleural envelope are classified as N2 nodes. Exact differentiation between N1 and N2 stages in a single hilar metastasis changes the prognosis significantly. In our experience, integrated PET/CT imaging is becoming the new standard of radiologic mediastinal staging (3). Antoch et al. (5) have confirmed our results. In their study, specificity of regional lymph-node staging was 94% with PET/CT, 89% with PET alone, and 59% with CT alone. Surgical biopsy by mediastinoscopy remains the gold standard for mediastinal staging. However, mediastinoscopy is not perfect and is surgeon dependent. In our experience, integrated PET/CT guides surgical mediastinal biopsy to the small lymph-node metastasis, thus improving the accuracy of surgical mediastinal staging (3).

Lung carcinoma (not shown) in right lung with focal increased 18F-FDG accumulation in left lower neck. (A) Transverse PET. (B) Transverse CT. (C) Integrated transverse PET/CT image of lower neck. Integrated PET/CT imaging ruled out N3 stage. PET/CT revealed that increased 18F-FDG accumulation in neck was localized in the intrinsic laryngeal muscles. Finding was result of compensatory laryngeal muscle activation caused by contralateral recurrent laryngeal nerve palsy from direct nerve invasion by lung cancer.
M Staging
Whole-body 18F-FDG PET is an excellent method to use in screening for extrathoracic metastases. In the era of integrated PET/CT, current morphologic imaging methods are inaccurate for M staging of patients. It has been shown, that PET detects unexpected extrathoracic metastases in 10%–20% of patients with NSCLC, and changes therapeutic management in about 20% of these patients. FDG PET is more accurate than CT in the evaluation of adrenal metastases, more accurate than bone scintigraphy in the detection of bone metastases, and more accurate than CT in the diagnosis of liver metastases (10,11). Yet, the clinical significance of a single focal abnormality on PET remains unclear, especially when no morphologic alterations are seen on CT images. The advantage of integrated PET/CT imaging is the exact localization and classification of a focal 18F-FDG accumulation. This was the case in 20% of all patients with extrathoracic metastases in our study of the value of integrated PET/CT (3). In the study by Antoch et al. (5), 17 distant metastases in 4 patients were detected with PET/CT, 4 distant metastases in 2 patients were detected with PET alone, and 14 distant metastases were detected in 4 patients with CT alone. PET/CT resulted in a significant increase in the number of correctly staged patients. Integrated PET/CT assists in those patients who require histopathologic confirmation of an extrathoracic 18F-FDG accumulation. PET/CT minimizes the risk of an anatomic miss, especially when no morphologic changes are found in CT.
Effect on Patient Treatment
According to the results of various groups, integrated PET/CT imaging has a positive effect on treatment. In a study with 204 patients with different types of cancer, PET/CT had an impact on management in 28 patients (14%) compared to a separate analysis of the PET and the CT component of the imaging studies (4). In a study with 27 patients with NSCLC, PET/CT analysis correctly revealed the tumor to be of a higher stage in 1 patient (4%) and to be of a lower stage in 7 patients (26%). The more accurate staging of PET/CT imaging affected treatment recommendations for 5 patients (19%) (5).
Physiologic Uptake Mimicking Metastasis
It is well known that activated muscles accumulate 18F-FDG. In some patients with lung cancer, an intense focal 18F-FDG accumulation is seen in the lower anterior neck just lateral to the midline. Integrated PET/CT has revealed that the focal 18F-FDG uptake is localized in the internal laryngeal muscles (Fig. 2). This finding is a result of compensatory laryngeal muscle activation caused by contralateral recurrent laryngeal nerve palsy from direct nerve invasion by lung cancer of the left mediastinum or lung apices (12). Awareness of this finding is important in avoiding false-positive PET results.
Small Cell Lung Cancer
The staging procedures for small cell lung cancer (SCLC) do not differ from those for NSCLC. The primary role for imaging is to separate accurately limited disease from extended disease. Because SCLC spreads early and widely, a battery of imaging tests is performed, such as CT of the chest and abdomen, CT or MRI of the brain, and a bone scan. It has been shown that whole-body FDG PET is a useful tool for staging SCLC (13). FDG PET is superior to conventional staging in the detection of all involved sites, particularly in the assessment of mediastinal lymph-node metastases. Integrated PET/CT imaging in SCLC is a highly valuable tool for planning radiation treatment. It is useful for accurate target definition by reducing the probability of overlooking involved areas (7).
Malignant Pleural Mesothelioma
Just as in lung cancer, excellent FDG uptake has been observed in malignant pleural mesothelioma (MPM). The role of PET is to document the extent of pleural disease, to establish mediastinal lymph-node involvement, to evaluate tumor invasion, and to diagnose recurrence. It has been shown that PET scanning is more accurate than CT scanning in staging patients with malignant mesothelioma (14). In our experience, integrated PET/CT imaging is an excellent method for staging patients with MPM. With coregistration of anatomic and metabolic information, the extent of the tumor can be defined precisely. Small mediastinal lymph-node metastases can be detected and precisely localized. Integrated PET/CT imaging is helpful in identifying the optimal biopsy site and thereby increasing the diagnostic accuracy of the histologic examination (15).
HEAD-AND-NECK CANCERS
Assessment of the Primary Lesion
Patients with mucosal squamous cell carcinoma of the head and neck (HNSCC) most often have a histologic diagnosis before they are referred for PET examination. PET is mainly used as a staging method to define the patient’s N or M stage. In contrast, some patients suffer from an unknown primary that PET is able to localize in the head-and-neck region. However, the precise identification, localization, and delineation of size and anatomic extent of a primary lesion is very important to correctly plan surgical interventions and radiation treatment. Therefore, contrast-enhanced CT, sonography, and MRI are routinely used in such patients.
With image coregistration of PET with CT or MRI, researchers have reported an ability to better evaluate cancers of the head and neck (16,17). However, the coregistration of datasets obtained by different devices at different time points has major drawbacks (e.g., patient repositioning, intercurrent anatomic changes, such as swelling of the head-and-neck area, and patient scheduling). Such problems are overcome with an integrated PET/CT scanner. The “intrinsic hardware” coregistration of both image datasets and the relatively fast acquisition provide high-quality image coregistration. Such data have been shown to be helpful for staging and treatment planning (18,19).
Furthermore, PET/CT improves the confidence of image interpretation (20). For example, in a patient with neck-muscle uptake, it is still possible to reliably distinguish malignant lesions from physiologic 18F-FDG uptake (18). Other physiologic 18F-FDG accumulations, such as in brown adipose tissue, can easily be identified and discriminated from muscle uptake or a soft-tissue mass, because on the coregistered CT image, this uptake will be localized within normal-appearing fatty tissue (21). Therefore, the specificity is improved with the help of structural information provided by CT.
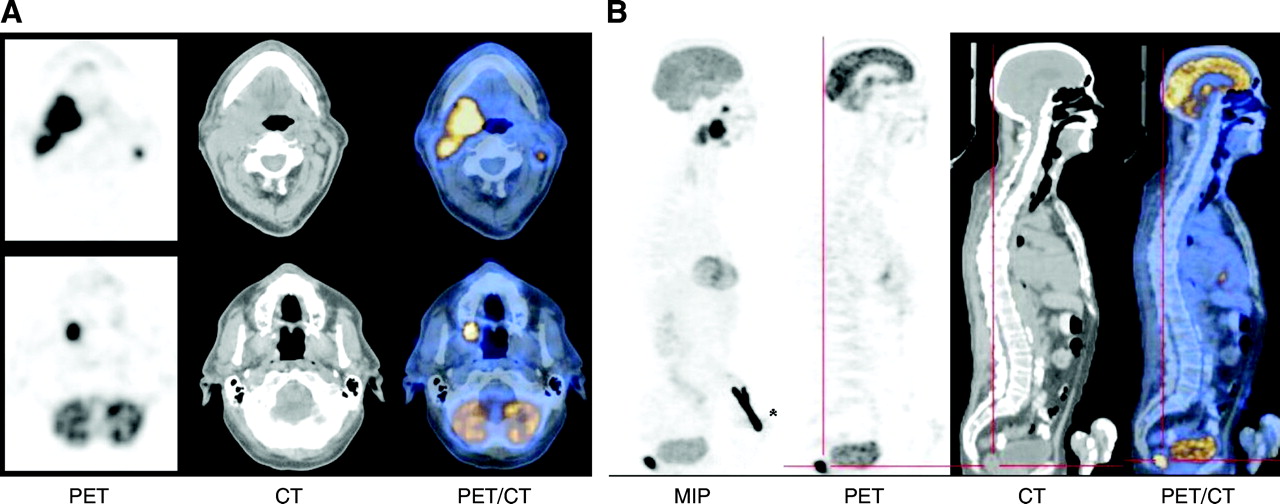
Small lesions can be missed on PET images. Also, small tumors can be overlooked with contrast-enhanced CT, and some tumors may remain undetectable when no intravenous contrast enhancement is administered. Intravenous contrast is important in evaluating extension of tumors adjacent to vessels and may be needed presurgically. Because PET alone is not able to reliably assess organ involvement and invasion of a tumor into adjacent structures, PET/CT images can help to better delineate such infiltrations. Based on our experience, the assessment of the extent of a lesion can be made more confidently with PET/CT than with PET and contrast-enhanced CT images read together side by side. Figure 3 is an example of a whole-body PET/CT image in a patient with two synchronous cancers in the oral cavity. The extent of the primary lesions and invasion into adjacent bony structures can only be assessed reliably together with the structural information of CT. However, studies are needed that compare noncontrast-enhanced PET/CT with contrast-enhanced PET/CT and contrast-enhanced CT read together with conventional PET side by side.

Transverse and sagittal PET, noncontrast-enhanced CT, and PET/CT images of 65-y-old patient who underwent staging for a squamous cell carcinoma of the tongue. (A) Primary extends from right lateral border of tongue inferiorly to floor of mouth, posteriorly to base of tongue, and laterally to pharyngeal wall. There were no signs of osteolysis at adjacent mandibula (bone window not shown), which was also confirmed in helical contrast-enhanced CT acquired with 3-mm slices (not shown). In addition, second primary with osseous maxillary infiltration at posterior alveolar part was found. Bilateral lymph-node involvement easily identified with PET, CT, and PET/CT. Note that FDG uptake in cerebellum is visible on consecutive CT slice and projects into bone as a result of partial-volume effect and leveling intensity of PET image. (B) In sagittal view, intense uptake of 18F-FDG is seen posteriorly to bladder on maximum intensity projection image (MIP) (* = injection site) and on sagittal slices of PET, CT, and PET/CT. This was a tubulovillous adenoma without histologic signs of cancer.
Early after treatment, edema of the neck can render the clinical evaluation of a patient difficult. PET is better than contrast-enhanced CT at discriminating scarring from residual cancer, especially in patients with altered anatomy (22). Combined PET/CT can help in such situations by localizing 18F-FDG uptake exactly to anatomic or pathologic structures and, therefore, facilitating patient management at restaging (e.g., by guiding biopsy) (23). It has been suggested that on early follow-up, false-positive PET findings as a result of an inflammation reaction will reduce the specificity of PET scanning (24). In our experience, in patients undergoing radiation treatment for advanced-stage HNSCC, a PET or PET/CT scan provides reliable information on the presence of residual cancer tissue if performed between 6 and 8 wk after the end of treatment (25).
Assessment of Lymph Nodes
Locoregional lymph-node metastases have an impact on survival, as patients with lymph-node involvement have a worse prognosis (approximately 30%) than patients without lymph node involvement (>50% 5-y survival) (26,27). For the assessment of lymph- node status, numerous publications have shown that PET has a higher sensitivity and specificity than contrast-enhanced CT or MRI (28–30). FDG PET also compares favorably with sonography for assessment of lymph-node metastases (31,32). In many cases we found that FDG uptake helps to detect lymph-node involvement either in nonenlarged lymph nodes or in lymph nodes that would have been missed on the contrast-enhanced CT scan.
Enlarged lymph nodes are often seen on contrast-enhanced CT without increased 18F-FDG uptake. The CT information facilitates the correct identification and localization of lymph nodes with an increased 18F-FDG uptake, and the anatomic level can be identified easily, helping in surgical and radiation treatment planning. Using PET/CT, the assessment of locoregional disease is performed much more easily and quickly.
For the locoregional management of HNSCC, PET/CT not only has the potential to improve diagnostic work-ups of patients, but the CT data also can be used for radiation treatment planning. Only a few reports have been published on the use of FDG PET and PET/CT to manage patients for radiation therapy (6,7,32). For the PET/CT-based planning of radiation treatment, the patient must be positioned in exactly the same way as for radiation treatment and the CT scan must be acquired with a high enough dose to reliably calculate the target volume. A low-dose CT scan (140kV, 40mAs), as used in our institution for routine diagnostic PET/CT, is not suitable for such dose calculations.
Based on our experience, a match of PET and CT datasets in the head and neck is possible to within only a few millimeters, which is better than the spatial resolution of a PET scanner, even in patients undergoing scanning without a face mask. This quality of image coregistration is precise enough for presurgical and preradiotherapeutical diagnostic evaluation of patients. However, the use of external markers can facilitate the correct positioning of the patient’s head when PET/CT is performed for the radiation treatment planning.
To date, the question of how the target volume definition would be affected if treatment planning were based only on the area of increased FDG uptake remains to be addressed. Furthermore, it is not known whether such a change of radiation planning would improve local cancer control and outcome for patients. There is a need for future studies evaluating how the accuracy of simulation will be affected by PET information and whether PET-based adaptations of radiation fields will translate into relevant clinical improvements.
Assessment of Distant Metastases
In head-and-neck cancer patients, it is important to evaluate for distant metastases, because this has great impact on survival (34). For the assessment of distant tumor involvement, imaging with contrast-enhanced CT of the thorax, ultrasound of the liver, and bone scanning do not improve patient management in a high enough proportion of patients to be routinely used for staging (35–37). Therefore, there are no common recommendations on how to evaluate distant metastases and secondary tumors in HNSCC patients. The advantage of PET with regard to this question is the ability to provide whole-body scanning in the same imaging session. It has been shown that imaging from the head to the pelvic floor influences clinical management of patients by detection of distant metastases or secondary tumors (38,39). Because most secondary cancers observed in HNSCC patients, such as bronchogenic cancer and squamous cell carcinoma of the esophagus, show a high 18F-FDG uptake, whole-body PET is ideal to identify these secondary malignancies.
Because it has been noted that >20% of patients with a HNSCC develop a secondary synchronous or metachronous cancer within 5 y (40), the most important question at restaging is whether a patient can still be treated (e.g., with salvage surgery for a locoregional problem) or if the disease has spread systemically. Therefore, we recommend the routine use of whole-body PET/CT not only for staging examinations but also for restaging.
HNSCC can grow very quickly in some patients, and the primary lesion may grow between the first diagnosis and the start of treatment. It is therefore very important to work quickly and to schedule the different tests for staging one after the other. In very busy centers, patients often have to wait between a contrast-enhanced CT and a PET scan. The use of PET/CT clearly shortens this work-up time.
CONCLUSION
PET-CT in lung and head and neck cancers may become the one-stop-shop oncological staging and follow-up examination in the near future. All available data point in this direction. The combination of PET information and anatomic information is often indispensable. PET/CT offers many advantages: it facilitates the interpretation of PET information and can offer adequate anatomic information to plan surgical interventions and radiation treatment. At restaging, PET/CT helps to better delineate the site and extent of a recurrence in patients with sometimes complex anatomical situations. For the assessment of lesion extension, PET/CT appears to be more reliable than PET with contrast enhanced CT and image interpretation is done more confidently and faster. Whole body imaging can detect distant metastases and secondary tumors and, thus, influence patient management. There is an important role of PET/CT for radiation treatment planning, but improved outcome and cost-effectiveness have to be assessed. The combination of molecular and anatomic information appears to be highly synergistic, and the studies evaluating PET/CT point to increased sensitivity, specificity and diagnostic accuracy. Still, PET/CT is in its infancy, and as a dual modality system it provides many options for different imaging protocols. While the basic approach to imaging with PET/CT has been worked out, the fine tuning of protocols requires many further studies. As the technology disseminates rapidly, these protocols will undoubtedly develop quickly.
Footnotes
Received Oct. 7, 2003; revision accepted Nov. 21, 2003.
For correspondence or reprints contact: Gustav K. von Schulthess, MD, PhD, Nuclear Medicine, University Hospital Zurich, Rämistrasse 100, CH-8091 Zurich, Switzerland.
E-mail: gustav.vonschulthess{at}usz.ch
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- PET/MR Imaging: A Critical Appraisal
- MRI-Based Attenuation Correction for Hybrid PET/MRI Systems: A 4-Class Tissue Segmentation Technique Using a Combined Ultrashort-Echo-Time/Dixon MRI Sequence
- 18F-FDG PET Can Replace Conventional Work-up in Primary M Staging of Nonkeratinizing Nasopharyngeal Carcinoma
- Value of contrast-enhanced multiphase CT in combined PET/CT protocols for oncological imaging
- Introduction