


Abstract
Although interictal hypoperfusion and ictal hyperperfusion are established localizing findings in partial epilepsy, their relative value is disputed. After a meta analysis of several published articles on SPECT brain imaging in patients with epilepsy (with extractable data on at least 6 patients per article), institutions using SPECT for evaluation of epilepsy have been encouraged to perform ictal scanning or interictal and postictal SPECT studies. Methods: We compared the relative localizing values of hypoperfusion in video-electroencephalographically (EEG) monitored interictal SPECT (IISPECT) and hyperperfusion in immediate postictal or periictal SPECT (PISPECT) in nonlesional patients who underwent temporal lobectomies in our epilepsy center from 1995 to 1998. We also evaluated the usefulness of combined interpretation of IISPECT and PISPECT when available. Results: Our experience with continuous cerebral blood-flow monitoring, published elsewhere, and SPECT results indicate that these recommendations are valid, but obtaining ictal SPECT is often serendipitous. We found that (a) interictal hypoperfusion was easier to demonstrate by SPECT but was less often concordant with the EEG focus than hyperperfusion in PISPECT, but not significantly (P = 0.11) so; (b) the lower incidence of hyperperfusion in PISPECT in our series was due to the occurrence of hypoperfusion in PISPECT, which was seen in 34.5% of our patients; and (c) hypoperfusion in PISPECT did have localizing value when it occurred on the same side as the hypoperfusion noted in IISPECT. Conclusion: On the basis of our findings, we recommend the use of 3 distinct perfusion patterns that emerge from the combined interpretation of IISPECT and PISPECT we proposed earlier (patterns 1–3), for localization purposes when possible, rather than ictal SPECT, IISPECT, or PISPECT by itself.
The site of onset of ictal events provides the best means of localization of the seizure focus (1,2). Since propagation of the ictal electrical discharge from the epileptogenic zone to the symptomatic zone may not be appreciable in the scalp recording, intracranial elecrtrocorticography (ECoG) and depth recordings are presumably the most accurate methods of localization. Even such recordings have been shown to be associated with lack of improvement in seizure control (3). This led to the search for additional methods for the localization of the surgical focus in the last quarter of the 20th Century (4). MRI can detect almost 100% of the structural lesions that are associated with epilepsy and the structural correlates of mesial temporal sclerosis (5). Other widely used techniques include PET and SPECT, which can be positive even when MRI is negative. PET claims higher sensitivity and specificity but is more expensive and is not available except in selected epilepsy centers. SPECT, on the other hand, is less expensive and is more widely available than PET.
However, SPECT is also the most controversial and, according to some, possibly the least specific (6). The principle behind the technology is the perfusional abnormalities that accompany the metabolic changes in epileptogenic brain tissue in the interictal phase and the changes in the blood flow in the periictal phase. In the 1970s, regional cerebral blood flow measurements using the radioactive isotope of xenon (133Xe) documented the cerebral blood flow changes during seizures. Using this technique, investigators found increased blood flow in the ictal phase (7) and decreased blood flow in the interictal phase at the site of the electroencephalographically (EEG) demonstrated focus (8). Several studies that followed, using PET (9) and SPECT (10), confirmed these early findings of interictal hypoperfusion and ictal hyperperfusion in the epileptogenic region, thus adding another dimension to the localization of the epileptogenic focus in partial seizures. However, reports of interictal increase in perfusion by some authors (11,12) as well as ictal (13) and late ictal (14) hypoperfusion reported by others added to the controversy surrounding the usefulness of SPECT for surgical localization in epilepsy.
As a result of subsequent technologic advances in CT and more and more stable isotopes, SPECT, with its ability to demonstrate localized changes in cerebral blood flow (CBF) interictally, during ictus, and postictally became a valuable tool for the evaluation of epilepsy (10,15). Its major disadvantage has been the controversy surrounding its sensitivity and specificity. Although most reports favored interictal hypoperfusion and ictal hyperperfusion, departures from this principle were noted early on (11–14). Some claimed interictal studies to be as sensitive as PET (15,16), others considered ictal studies to be more reliable (17,18). and yet others doubted their usefulness (19,20). The reasons for the controversy are that the earlier perfusional studies—some done with 133Xe, others with 123I-isopropyliodoamphetamine, 99mTc-hexamethylpropyleneamine oxime (HMPAO), yet others with 18F-FDG PET, and a small number of centers using the more stable 99mTc-ethylcysteinate dimer (99mTc-ECD), using differing technologies, performed on varied cohorts—had little in common to justify comparisons. Attempts at making sense of the enormous data accumulated worldwide, under such circumstances, only added to the controversy.
Interictal hypometabolism and ictal hypermetabolism are the most common PET findings in the epileptogenic cortex in partial epilepsies (9,21,22). We also know that blood flow is coupled to epileptiform activity and metabolism. Penfield in 1933 (23), Penfield et al. in 1939 (24), and Plum et al. (25) had already demonstrated that there is increased CBF in the region of the epileptogenic focus during and immediately after partial seizures. PET studies in a few patients during focal status epilepticus (26) and during or after a single complex partial seizure have confirmed the presence of periictal hyperperfusion and hypermetabolism.
More recent evidence from long-term surface cortical CBF monitoring in temporal lobe epilepsy also has confirmed that the interictal epileptic foci are significantly hypoperfused relative to the nonepileptic cortex (27,28).
The range of positive interictal SPECT (IISPECT) studies varies from 57% to 95% (12,29). From a meta analysis of 30 published studies from a literature search with at least 6 patients in each study, Devous et al. (30) concluded that IISPECT, has a sensitivity of 0.75, which is similar to the results obtained with interictal PET, which shows interictal focal abnormalities in 70% of patients with complex partial seizures (9). But the relative validity of IISPECT and ictal SPECT has been the subject of a long controversy (6,31). Our own experience with SPECT has been that it is a valuable addition to MRI and video-EEG in reducing the need for invasive monitoring, with its consequent morbidity and expense, similar to the experience of Rowe et al. (32) and, hence, in reducing the cost of presurgical evaluation of seizures of temporal lobe origin. SPECT has thus become a routine procedure at epilepsy centers, and the Society of Nuclear Medicine has included presurgical localization of epilepsy as a standard indication for brain SPECT (33) in their Procedure Guidelines. However, not enough studies have compared the value of IISPECT, ictal SPECT, and immediate postictal SPECT (PISPECT) (34), and their relative merit is thus yet to be established.
In this study we compared the concordance of perfusional changes in video-EEG monitored, semiquantitative IISPECT and PISPECT studies in nonlesional patients with seizures of temporal lobe onset who underwent temporal lobectomies at the Comprehensive Oklahoma Program for Epilepsy from 1995 to 1998. We also attempted correlation of the previously described perfusional patterns we proposed earlier (patterns 1–3), resulting from combined analysis and interpretation of IISPECT and PISPECT studies.
MATERIALS AND METHODS
Forty-two patients underwent temporal lobectomies during the study period. Twenty-one patients were male and 21 were female (mean age ± SD, 32.14 ± 10.95 y old). All patients underwent continuous video-EEG monitoring, MRI, and scalp EEG for localization of the seizure focus. Seizure foci were localized by reviewing the edited video-EEG, of a minimum of 3 each, of each the patient’s typical seizures. In cases in which the scalp EEG was nonlocalizing or was in conflict with the MRI findings, video-EEG monitoring was repeated after implantation of subdural strip electrodes. IIPSPECT was performed after the patients had been seizure free, under video-EEG surveillance for at least 24 h, to reduce the effect of prior seizures (35,36) over the temporal lobe blood flow and, thereby, the SPECT results. A safety window of 24 h was set after the initial injection of the radioisotope before the second injection to allow for adequate decay of radioactivity produced by the first injection and to enhance radiation safety.
The radioisotope used was 99mTc-ECD. PISPECT was accomplished by injection of 99mTc-ECD with either the clinical or electrical onset of seizures in the epilepsy-monitoring unit under combined closed-circuit video and EEG surveillance of the patient by specially trained EEG-monitoring technologists. The doses were restocked twice a day at the bedside for easy availability and the patients had heparin-locks for immediate intravenous access during the seizure. The injection was performed by specially trained nurses. SPECT image acquisition was done as soon as it was practically feasible after the ictal injection, in most cases within 3 h of injection. Imaging data were acquired using a Siemens triple-head scanner with a high-intensity fanbeam collimator in a 128 × 128 matrix with a zoom factor of 1.23 (2.89 mm/pixel) with 120 stops or projections at 60,000 counts per stop, for both the IISPECT and PISPECT scans. This required that some patients had to stay longer in the scanner than others but ensured a measure of consistency in counts that was as standardized and as quantitative as possible.
We were able to obtain images of excellent quality because the brain distribution of 99mTc-ECD is stable over time (37) and the brain-to-background ratio is 17:1 for 5 h as opposed to 2:1 for HMPAO (38). The images were interpreted by a nuclear medicine physician who was unaware of the MRI and EEG results, and the studies were later reviewed and correlated with MRI and EEG, in conference with the electroencephalographer and the neuroradiologist. Studies were reported as normal or as showing evidence of hypoperfusion or hyperperfusion in the various brain regions in the interictal and the immediate postictal periods. The IISPECT and PISPECT were then compared to evaluate the preictal and immediate postictal perfusion patterns.
RESULTS
Of the 42 patients, who were included in the study, 40 had IISPECT scans. Two patients did not have IISPECT due to technical reasons. The relative concordance of the 2 studies to the EEG is shown in Table 1. Of the 40 patients who had IISPECT, 36 (90%) showed evidence of focal temporal hypoperfusion. Four (10%) were nonlocalizing, 2 because they were normal and 2 because they had evidence of bilateral temporal hypoperfusion. PISPECT was available for 29 of the 42 patients. Of the 29 who had PISPECT, 19 (65.5%) showed focal hyperperfusion. In 10 (34.5%) patients, there was accentuation of the focal hypoperfusion in PISPECT, on the same side as the interictal hypoperfusion. None had interictal hyperperfusion.
SPECT Findings
The mean injection time was 1.86 ± 0.88 min from onset of the seizure. In our experience, it took 15–20 s for the bolus of 99mTc-ECD to be administered. Since it takes 20 s for 95% brain extraction of the isotope (37), only the patients in whom the injection was started within 40 s of seizure onset would have had 95% extraction of the isotope within 60 s. The timing of the injection is extremely important if one is to obtain true ictal SPECT since the electrical activity, to which the initial rise in blood flow is coupled, lasts 60–140 s (39) only. Because our mean injection time was about 114 s in most cases, the brain extraction of the isotope occurred after the rhythmic electrical activity associated with the seizure had peaked or was on the decline when the injection was finished. Therefore, we considered that the term immediate postictal or periictal SPECT (PISPECT) was more appropriate than the term ictal SPECT, even though the injections in our patients were accomplished in a very short time to justify our use of the term “ictal SPECT” as it has been used in the literature (13) by other investigators.
In our series of 42 patients, we observed that IISPECT was easier to obtain, with the study being done in 40 of 42, or 95.2%, of patients. PISPECT was more difficult to obtain, with the study available in only 29 of the 42 patients (69%). This was because the other patients had all the required seizures before the next batch of isotope was stocked, because the second and third seizures occurred within the 24-h window when another injection was not permitted and the patient was discharged, or because the seizures occurred over the weekend when scanning was not available. In 2 cases, only PISPECT was available. This was done before IISPECT because the patients had the first seizure before an interictal study could be performed and they had to be discharged before IISPECT could be done. Interictal hypoperfusion was the most common finding seen in 36 of 40 (90%) patients, with 32 of the 36 (88.9%) being concordant with the EEG focus. None had interictal hyperperfusion. PISPECT was available in 29 patients. Immediate postictal hyperperfusion was seen in 19 of 29 (65.5%) patients and was less frequent than the occurrence of interictal hypoperfusion but 18 of 19 (94.7%) were concordant with the EEG focus. This was slightly better than the rate of concordance (88.9%) for interictal hypoperfusion but was not significantly better (P ≥ 0.5). Keeping this in mind, our data would indicate that PISPECT has a higher concordance rate (94.7%) with the EEG focus than IISPECT (88.9%). The lower incidence of hyperperfusion in the immediate postictal studies, (65.5%) as opposed to hypoperfusion in interictal studies (90%), was due to the occurrence of the phenomenon of accentuation of hypoperfusion in PISPECT, compared with their own interictal studies, in 10 of 29 (34.5%) patients. In 9 (90%) of these 10 patients who had ipsilateral accentuation of hypoperfusion in PISPECT, it was concordant with the EEG focus, whereas in 1 (10%) the accentuation of hypoperfusion was contralateral.
DISCUSSION
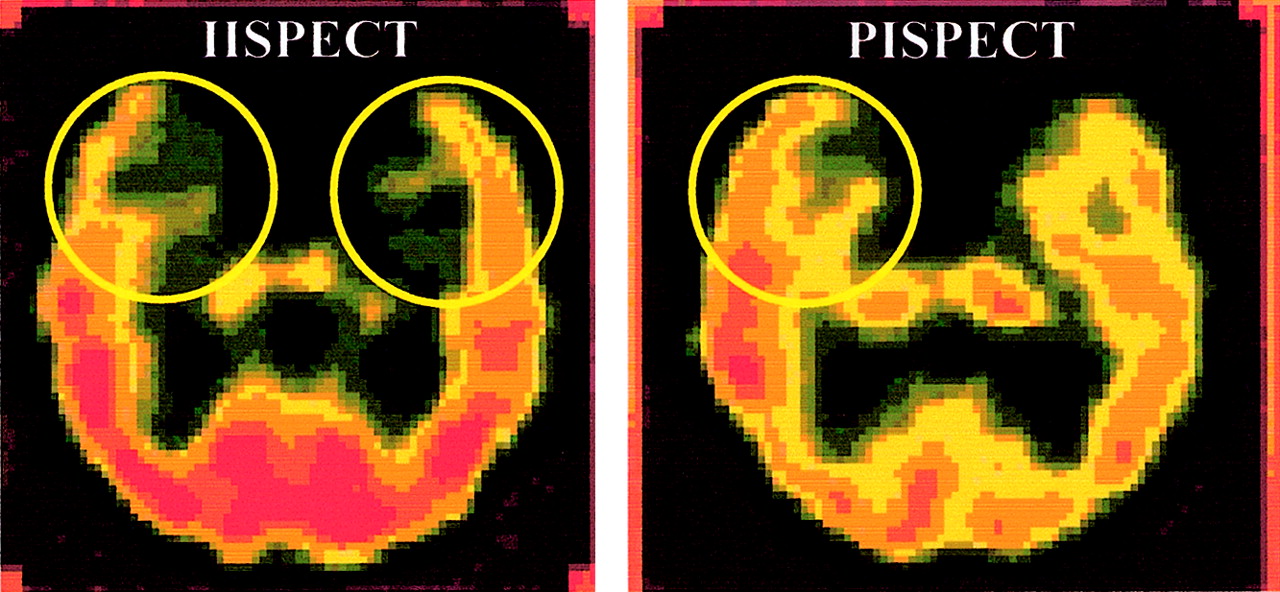
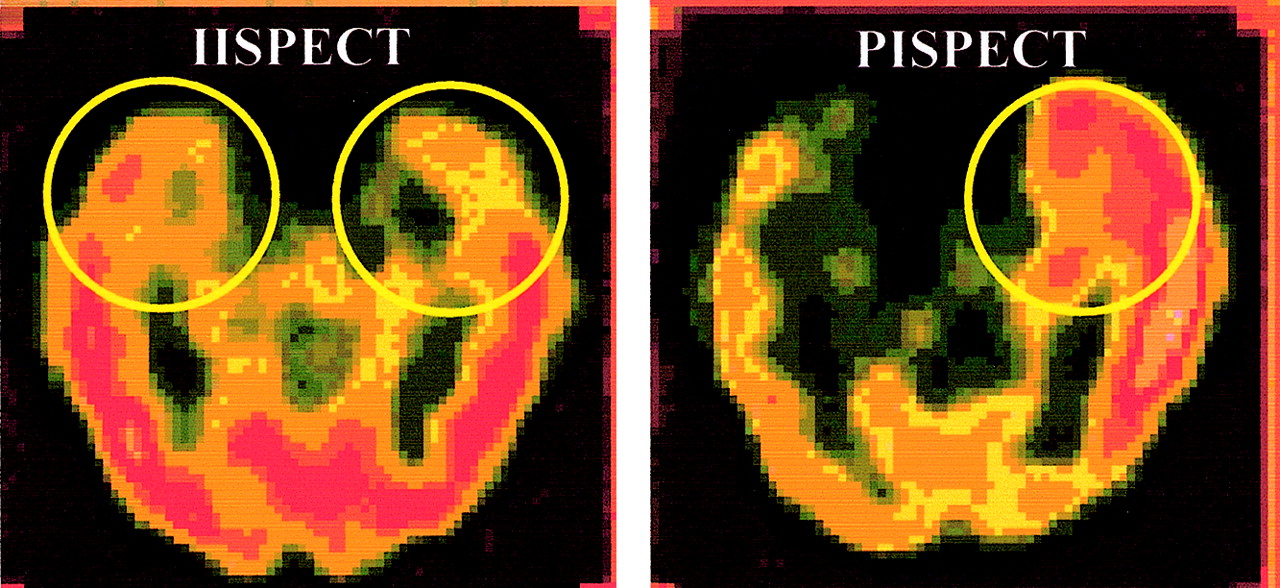
In 1993, Oommen et al., using long-term ECoG and cortical CBF monitoring with specially designed subdural strip electrodes capable of measuring CBF and ECoG at the same time, showed that the ictal hyperperfusion was coupled to the ictal spike train. It was also shown that that the rhythmic electrical discharge in the temporal lobe during the seizure is short-lived and that the CBF after the cessation of the rhythmic electrical activity or spike train may show 3 different phenomena: The blood flow may immediately revert to the preictal level, change to a hyperperfusional state, or change to a hypoperfusional state. These latter phenomena lasted up to 3 h in that particular study (39). Thus, the dynamic nature of blood flow in the periictal period systematically studied by Penfield (23) and Penfield et al. (24) during surgery, and later demonstrated by Plum et al. (25) experimentally, was confirmed by Oommen et al. by in vivo CBF monitoring in the human brain using this novel technology. This observation became the basis of their combined interpretation of IISPECT and immediate postictal SPECT studies published subsequently (40). As our experience evolved, we divided these into patterns 1–3. In pattern 1 (Fig. 1), there is hypoperfusion in IISPECT and hyperperfusion ipsilaterally in PISPECT. In pattern 2 (Fig. 2), the IISPECT is either normal with unilateral hyperperfusion in PISPECT or, if there is bilateral hypoperfusion in IISPECT, it is normalized unilaterally or is focally hyperperfused on one side in PISPECT. In pattern 3 (Fig. 3), there is focal or bilateral hypoperfusion in IISPECT and immediate postictal accentuation of the hypoperfusion in PISPECT.

Pattern 1: Focal interictal hypoperfusion (left) and immediate postictal hyperperfusion in same temporal lobe.
Pattern 2: Symmetric bilateral interictal hypoperfusion and asymmetric unilateral (right) immediate postictal hyperperfusion.

Pattern 3: Bilateral interictal hypoperfusion and unilateral (right) immediate postictal accentuation of hypoperfusion in temporal lobe.
In the combined analysis of the IISPECT and PISPECT data, pattern 1 was concordant with the EEG focus in 13 of 14 (92.9%) patients. When the accentuation of hypoperfusion occurred on the same side as the interictal hypoperfusion, (pattern 3), it also significantly (90% concordance) correlated with the EEG focus. Pattern 2 was noted in only 1 patient in the current series and had 100% correlation with the EEG focus (Table 2). Thus, bitemporal hypoperfusion, which usually does not help in localization, became useful in localization, when combined with the hyperperfusion in PISPECT. Many previous studies have noted focal hypoperfusion in the ictal studies, and others have looked at its usefulness in localization. Recognition of this phenomenon is critical in avoiding false localization, because an area of hypoperfusion in SPECT may result in the homologous area on the other side appearing to be hyperperfused, because of the inherent qualitative nature of most SPECT studies.
Relationship of Perfusion Patterns to EEG Localization
CONCLUSION
Interictal hypoperfusion in spontaneous seizures of temporal lobe origin can be demonstrated with SPECT and the pattern of periictal and postictal CBF is useful in predicting the seizure focus. True ictal hyperperfusion is practically difficult to obtain in epilepsy-monitoring units because of the transient nature of seizures and the dynamics of CBF during seizures. Except for very few instances in which injection of the isotope is made at the onset of seizures, using isotopes that are rapidly (within seconds) taken up by the brain tissue, most ictal studies reported in the literature have been periictal or, in some cases, postictal studies. This is one reason for the controversy regarding the usefulness of SPECT findings in the “so-called” ictal studies reported in the literature. The paradoxical increase in flow in interictal studies reported in the literature was in some cases due to the presence of unrecognized structural lesions and in others due to interictal epileptiform activity. We did not see this phenomenon in any of our patients, all of whom had a demonstrated seizure-free period of about 24 h before their IISPECT studies. SPECT studies should therefore be done under controlled circumstances with video-EEG monitoring to define the relationship of the scans to interictal EEG activity and seizures. When performed in this way, both IISPECT and PISPECT have their place in the localization of seizure foci and, when both are available, they should be interpreted keeping the dynamic nature of blood flow during seizures in mind. The recognition and use of patterns 1–3 using IISPECT and PISPECT will improve the value of SPECT in localization of epileptogenic foci, and the combined interpretation can improve the usefulness of the procedure, particularly in patients in whom the IISPECT is normal or shows bilateral hypoperfusion.
Footnotes
Received Mar. 17, 2004; revision accepted Jul. 15, 2004.
For correspondence or reprints contact: Kalarickal J. Oommen, MD, Department of Neurology, University of Oklahoma Health Sciences Center, 711 Stanton L. Young Blvd., Suite 215, Oklahoma City, Oklahoma, 73104.
E-mail: Kalarickal-oommen{at}ouhsc.edu
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.