


Abstract
The rate of treatment failure in acute exacerbation of ulcerative colitis (UC) still reaches 20%–30%. Early identification of nonresponders to therapy is important, since intensified or other medical treatment or, ultimately, colectomy should be considered to reduce morbidity. Because 99mTc-hexamethylpropyleneamine oxime (99mTc-HMPAO) white blood cell (WBC) scintigraphy is accurate in determination of the severity and extent of UC lesions, the aim of this study was to assess whether WBC scintigraphy can predict early treatment failure in patients with an acute attack of UC. Methods: We included 20 consecutive patients (7 women, 13 men; mean age ± SEM, 36.8 ± 10.9 y) with a history of UC who were hospitalized with severe exacerbations. All patients underwent endoscopy and scintigraphy within 24 h of admission and 1 wk after beginning treatment. WBCs were labeled with 200 MBq 99mTc-HMPAO. SPECT of the abdomen was performed 60 min after WBC reinjection. Maximum tracer uptake in the different colon segments was defined and expressed as a ratio of lumbar bone marrow uptake. The scintigraphic activity score (SAS) was expressed as the sum of segmental colon uptake ratios. Scintigraphic evolution was considered favorable when the SAS decreased by ≥50% and SPECT uptake ratios after therapy were ≤1.5 per segment. Rectosigmoidoscopy with biopsy was performed within 24 h after scintigraphy. Results: Outcome analysis after 3 mo showed 6 of 20 patients in clinical and endoscopic or histologic (rectosigmoid) remission, without alteration of treatment (responders). Of the other patients (nonresponders), 5 of 14 received a colectomy, 5 of 14 received prolonged or intensified treatment, and 4 of 14 received other treatment. In the responders group, the SAS (determined 1 wk after beginning therapy) significantly decreased in all patients. In the group of nonresponders, 10 patients had an increase of >10% in the SAS, 2 patients had an unchanged SAS, and 2 patients had a decreased SAS of >10% but had a residual mean segmental WBC uptake ratio of >1.5. There was a statistically significant difference between the responders and nonresponders (P < 0.01). Conclusion: Repeated 99mTc-HMPAO scintigraphy seems to be able to predict therapy resistance in UC within 1 wk after beginning treatment.
- inflammatory bowel disease
- ulcerative colitis
- radionuclide imaging
- 99mTc-HMPAO white blood cell scintigraphy
- treatment response
Ulcerative colitis (UC) is a chronic inflammatory bowel disease (IBD) characterized by periods of acute attacks and remission (1). Treatment is mainly based on corticosteroids, administered orally, parenterally, or rectally (2). A rapid and sustained response is usually seen within a few days after initiation of treatment. However, the overall rate of steroid treatment failure in acute exacerbations of UC remains high, and 20%–30% of patients ultimately require surgery (3,4). The introduction of cyclosporine as a potent immunosuppressive drug for treatment of corticosteroid-refractory UC benefits the short-term management in 60%–80% of patients (5,6).
Early identification of the patients with a severe exacerbation of UC who will respond to therapy remains difficult. However, it is of great clinical importance to be able to predict a need for step-up medical treatment or, ultimately, colectomy at an early stage of the acute attack to reduce morbidity (3,7).
Multiple clinical and laboratory parameters have been suggested as valuable predictors of outcome with respect to colectomy for assessment of glucocorticoid response. Recent trials identified persistent high stool frequency, bloody diarrhea, continued C-reactive protein (CRP) elevation, and sustained elevation of body temperature as strongly predictive parameters of clinical steroid resistance in acute attacks of UC, with a high probability of the ultimate need for colectomy (3,7). Clinical and laboratory indices, however, seem relatively inaccurate in assessment of disease severity at the tissue level (8).
White blood cell (WBC) scintigraphy has been shown to be a reliable and accurate determinant of the extent and intensity of UC lesions, combining imaging of the affected colon with a semiquantitative scoring of disease activity (9,10). WBC scintigraphy has been shown to be superior to the activity index and the gastroenterologist’s clinical opinion for diagnosing active inflammation in patients with IBD (11).
An influx of neutrophils and other acute inflammatory cells in inflamed intestinal mucosa is a prominent feature in acute attacks of UC (12). Neutrophils are the predominant effector cell within the active lesions of UC and probably mediate most of the tissue damage (13). Therapeutic action is based on reduction of inappropriate gut inflammation, by means of glucocorticoids, immunomodulators such as cyclosporine, or biologic therapeutic intervention in mucosal homing (14,15). Because scintigraphy and histology correlate very well in this particular field, WBC scintigraphy could become a reliable, noninvasive prognostic tool in prediction of the therapeutic response and the follow-up of treatment for UC.
The aim of this study was to determine whether WBC scintigraphy can predict early treatment failure in patients with acute attacks of UC.
MATERIALS AND METHODS
Subjects
We included 20 consecutive patients (13 men, 7 women; mean age ± SEM, 36.8 ± 10.9 y) with a history of UC who were hospitalized with severe exacerbations. A severe episode was defined as an acute attack of UC with an activity score of ≥10 (6). Exclusion criteria were toxic megacolon or perforation evident on plain abdominal radiographs, infectious disease, and use of intravenous steroids for >12 h before admission. Patients with a history of bowel surgery were not included. All patients gave written informed consent to participate in the study, which was approved by the medical ethics committee of the Leuven University Hospital.
The clinical activity score was determined on admission and daily after initiation of therapy (6). For this study, only the activity scores on admission and 1 wk after initiation of therapy were recorded. A rectosigmoidoscopy with biopsy was performed within 24 h of inclusion. The macroscopic appearance of the mucosa was classified using a 4-grade scoring system (16). Mucosal biopsy specimens obtained in the most severely affected areas were also graded on a 4-point scale (8). All patients underwent scintigraphy within 24 h after endoscopy. Rectosigmoidoscopy with biopsy and scintigraphy were repeated 1 wk after initiation of therapy. All scores (endoscopic, histologic, and scintigraphic) were interpreted as grade 0, meaning normal bowel mucosa, and grades 1–3, meaning mild, moderate, and severe disease, respectively.
Scintigraphic Test Procedure
The technique of labeling granulocytes in a mixed leukocyte suspension using 99mTc-hexamethylpropyleneamine oxime (99mTc-HMPAO) has been performed according to the consensus protocol for leukocyte labeling (17). An average of 200 ± 10 MBq of 99mTc-labeled granulocytes was reinjected into the patient.
Planar anterior and posterior 3-min images of the abdomen and pelvis were obtained at 45 min after reinjection using a large-field-of-view γ-camera fitted with a low-energy, general-purpose collimator. Just before scintigraphy, the patient was asked to void. The 45-min image was used for localization and determination of the extent of bowel activity.
At 60 min after reinjection, SPECT was performed. A 360° circular orbit was used acquiring 90 views of 40 s in a 30-min-duration study. An image matrix of 64 × 64 pixels was used. After data acquisition, images were processed on a Trionix workstation using filtered backprojection using a ramp reconstruction filter with a Hamming window. Correction for attenuation was made using the Chang technique with an attenuation coefficient of 0.12 cm−1 (18). Transaxial abdominal slices of 8.4-mm thickness were reconstructed. After reconstruction, a 9-point smoothing was applied.
Scintigraphic Data Analysis
The planar scintigrams were evaluated by 2 physicians without knowledge of the endoscopic, histologic, or clinical findings. On SPECT images, the colon was divided into 5 segments: ascending colon, transverse colon, descending colon, sigmoid, and rectum. Tracer uptake was determined as described by Weldon (19) and Weldon et al. (20). Therefore, the maximum counts per pixel in each segment was measured using region-of-interest analysis of serial transaxial slices to obtain the maximum value for each colon segment. The SPECT segment uptake ratio was expressed as a fraction of bone marrow activity, obtained by averaging the maximum counts in 5 transaxial slices of lumbar spine. All processing was performed by the same observer.
The SPECT segment uptake ratio was converted into a segmental SPECT severity score: grade 0, no uptake; grade 1, uptake ratio = 0.326 ± 0.19 (mean ± SD); grade 2, uptake ratio = 1.11 ± 0.36; and grade 3, uptake ratio = 3.33 ± 1.84 (19,20). This severity score was used for comparison of scintigraphy and histology. For comparison of total colon uptake before and after therapy, the pathologic segmental uptake ratios were summed and expressed as the scintigraphic activity score (SAS). The difference in the SAS before and 1 wk after beginning treatment (ΔSAS) was expressed as the percentage change in the SAS after therapy compared with the baseline scintigraphy.
Dosimetry
The radiation doses received by target organs—spleen, liver, and bone marrow—were 0.21, 0.025, and 0.023 mGy/MBq, respectively (21). The effective dose equivalent was 0.011 mSv/MBq.
Management
Patients were double-blind randomized as part of another pharmacotherapeutic trial and treated with either intravenous corticosteroids, 40 mg/d continuous infusion, or intravenous cyclosporine, 4 mg/kg body weight. Cyclosporine was administered by continuous infusion adjusted to blood levels between 200 and 300 ng/mL by a physician not taking part in the direct patient management. Treatment was continued for 8 d and subsequently adjusted if necessary. Patients who had a clinical response in the cyclosporine group were switched to oral cyclosporine, started at a dose of 8 mg/kg in 2 equally divided doses per day and adjusted to serum levels between 200 and 350 ng/mL. Patients in the corticosteroid group who had a clinical response were switched to oral methylprednisolone, 32 mg/d for the first 3 wk and tapered by 4 mg/wk until discontinuation.
Outcome
After 7 d of treatment, patients were classified according to the clinical activity score (6). Immediate clinical response to intensive medical therapy was defined as improvement of the clinical activity score to a score of <10 with a drop of at least 3 points, with the ability to discharge the patient. Immediate scintigraphic response was defined as a decrease in the SAS of >50% and a residual mean segmental WBC uptake ratio of <1.5. The scintigraphic response was not used for immediate patient management decisions. After 3 mo, all patients were reviewed. For this study, patients were considered responders when the initial treatment strategy led to remission without alteration or intensification of the regimen. Patients were considered nonresponders when the initial treatment strategy needed to be intensified or changed to yield remission or when patients required a colectomy.
Statistical Analysis
All results are expressed as mean ± SEM values. The paired samples t test was used to compare differences between activity scores. Spearman rank correlation was used for statistical analysis of results. All statistical tests were 2-tailed and differences were evaluated at the 5% level of significance.
RESULTS
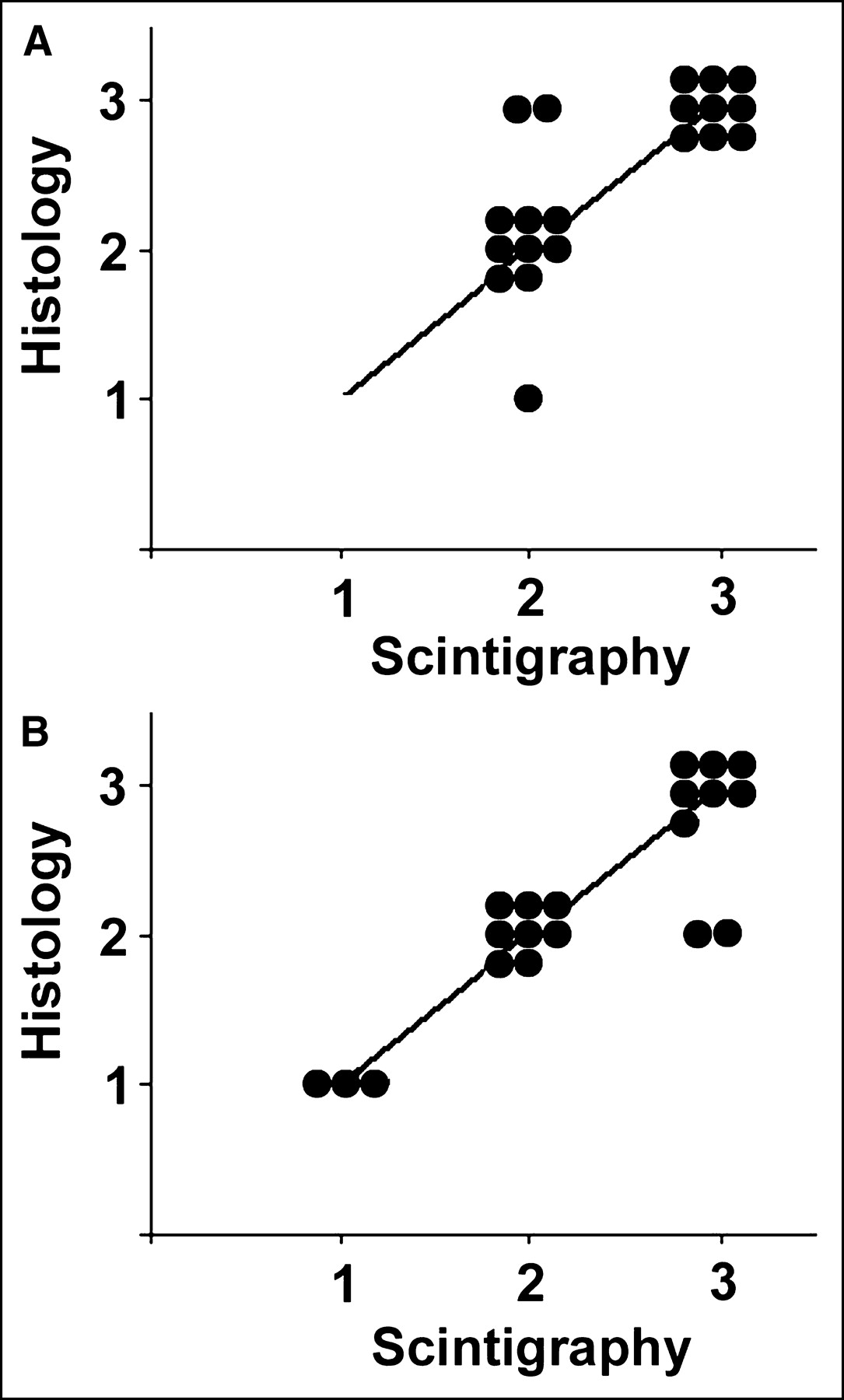
Patient data are illustrated in Tables 1 and 2. Before treatment, 10 patients had left-sided colitis and 10 patients had pancolitis. The mean inflammatory activity determined clinically using the numeric symptom score was 12.85 ± 0.68 (mean ± SEM). Upon inclusion, there was a significant correlation between planar scintigraphic (data not shown) and histologic indices of disease intensity of the rectosigmoid (r = 0.64, P < 0.01) before treatment. There was an even better correlation between SPECT-derived scintigraphic and histologic indices of disease intensity of the rectosigmoid (r = 0.80, P < 0.01). One week after therapy, there was an excellent correlation between SPECT-derived scintigraphic and histologic indices of disease intensity of the rectosigmoid (r = 0.88, P < 0.01; Fig. 1).
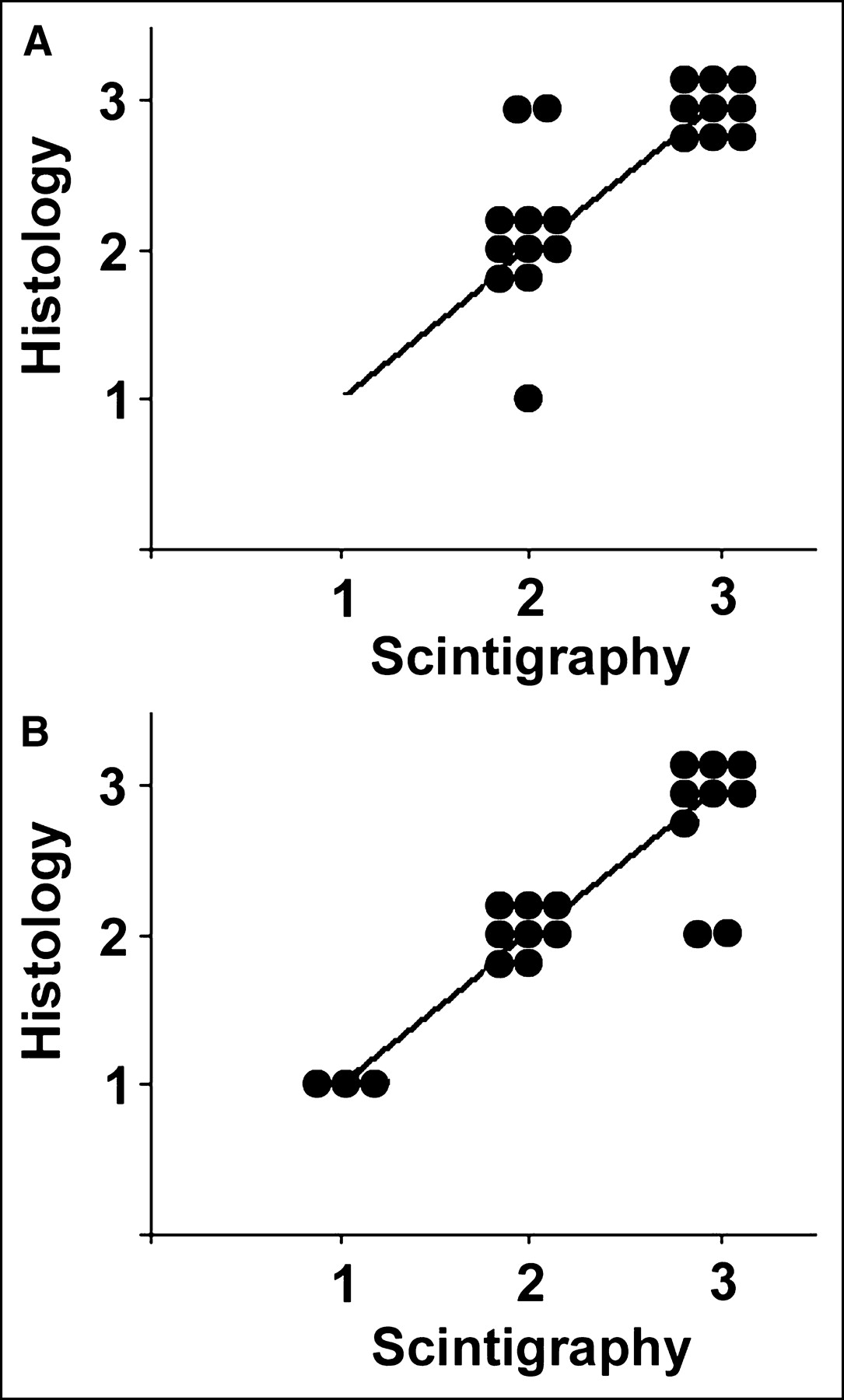
Correlation of activity score assessment by histologic analysis and SPECT of rectosigmoid on inclusion (A) and 1 wk after beginning treatment (B). Good correlation of scintigraphic and histologic assessment of disease activity before and after therapy is evident (r = 0.80, P < 0.01 vs. r = 0.88, P < 0.01, respectively).
Patient Characteristics
Cyclosporine and Methylprednisolone Therapy: Correlation of Various Parameters
After 3 mo, 6 of 20 patients (30%) were responders and achieved a complete response without changing the therapeutic strategy (R). Fourteen of 20 patients (70%) were nonresponders to initial therapy. In this group, 9 of 14 patients finally achieved a complete response but required a change of therapeutic strategy (RA), and 5 of 14 patients were treatment failures and required colectomy (FC).
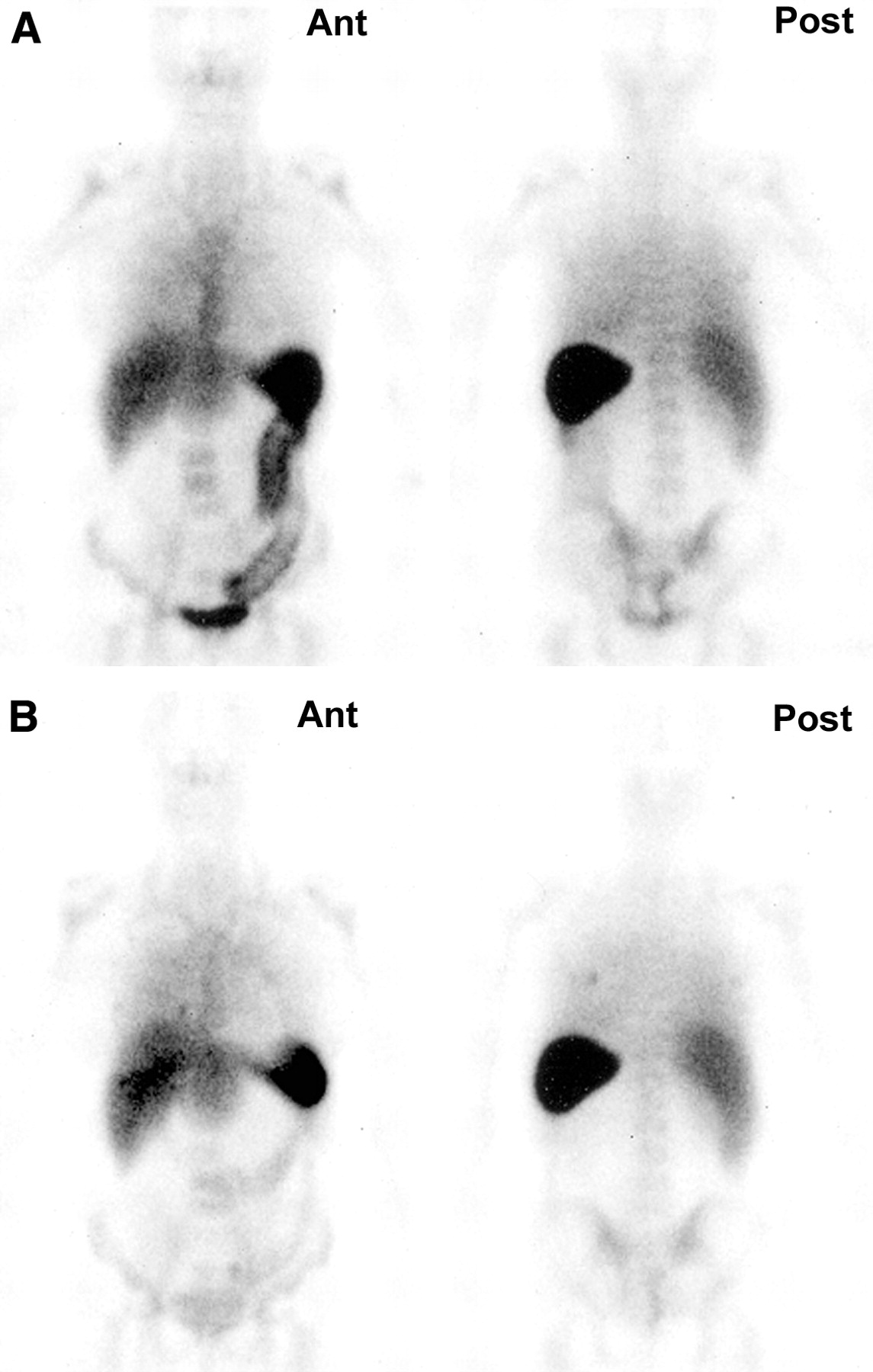
In the group of responders, all patients had a decrease in the SAS of ≥50% and had a residual mean segmental WBC SPECT uptake ratio of <1.5 (Figs. 2 and 3). The mean decrease in the SAS in this group was significant (P < 0.05). The mean percentage decrease (ΔSAS) in this group was 70% (range, 53%–84%).
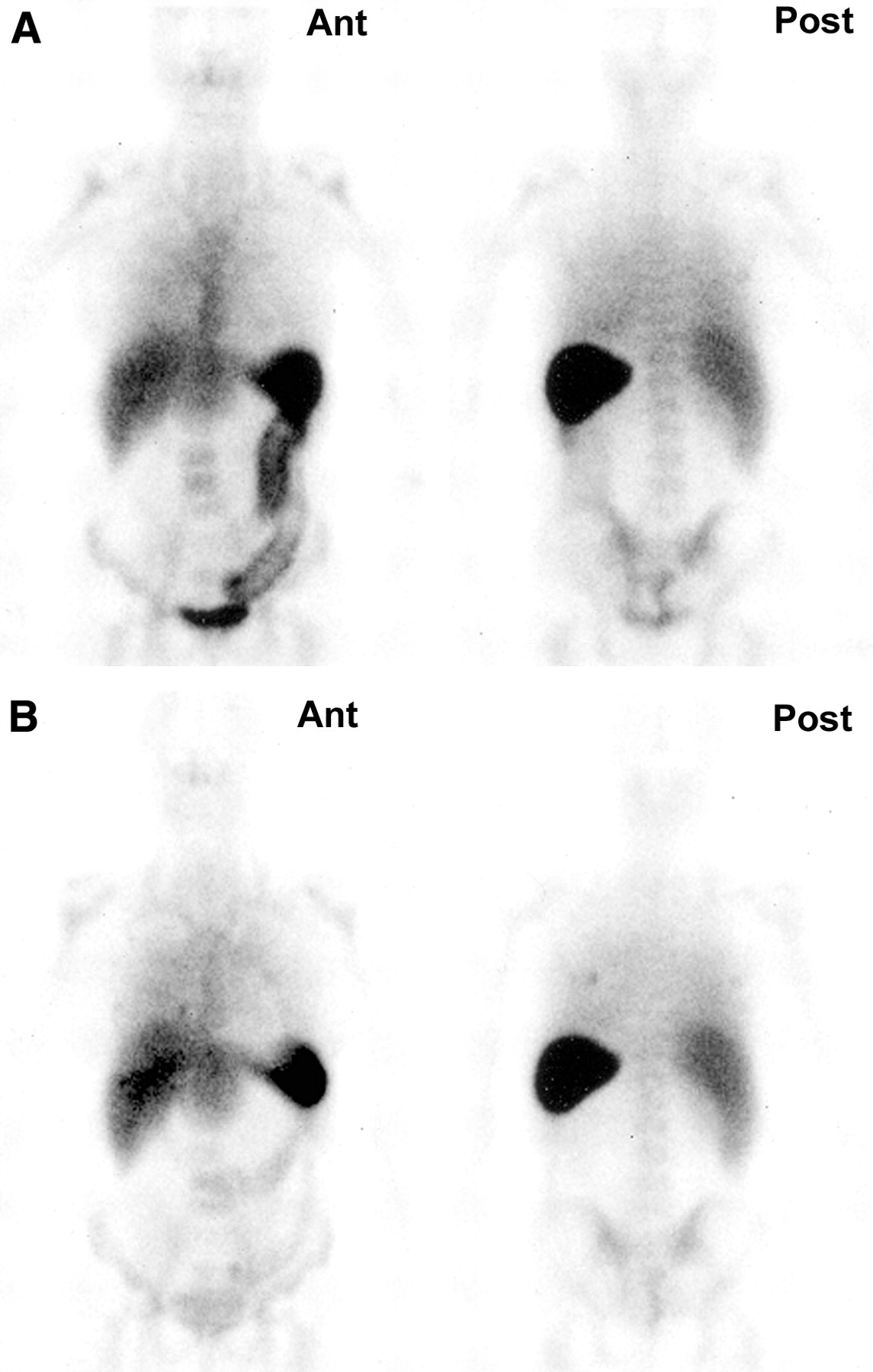
99mTc-HMPAO WBC whole-body scintigraphy (patient 6) in anterior (Ant) and posterior (Post) views before therapy (A) and 1 wk after beginning therapy (B). Scintigraphy before treatment shows severe colitis in 4 segments. Scintigraphy 1 wk after treatment shows markedly decreased uptake with mild-to-moderate colitis in 4 segments.
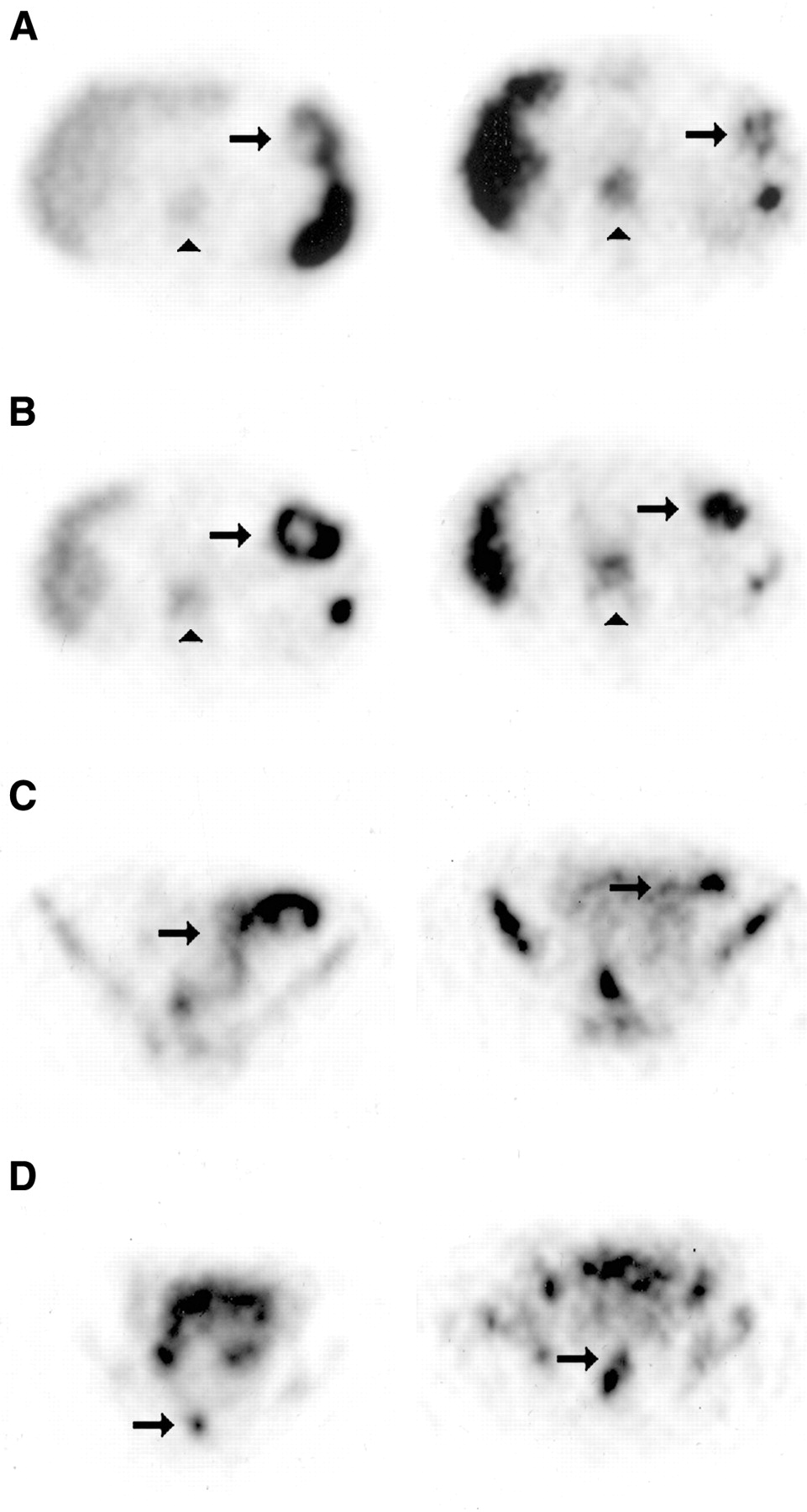
99mTc-HMPAO WBC SPECT (patient 6). Transaxial slices at different levels in abdomen from cranial to caudal (A–D) before therapy (left) and corresponding slices 1 wk after beginning therapy (right). Colon activity before therapy (arrow) is manifestly increased (SAS = 7.33) in transverse colon (A), descending colon (B), sigmoid (C), and rectum (D) compared with bone marrow (▴). Colon activity 1 wk after beginning therapy decreased (SAS = 3.01).
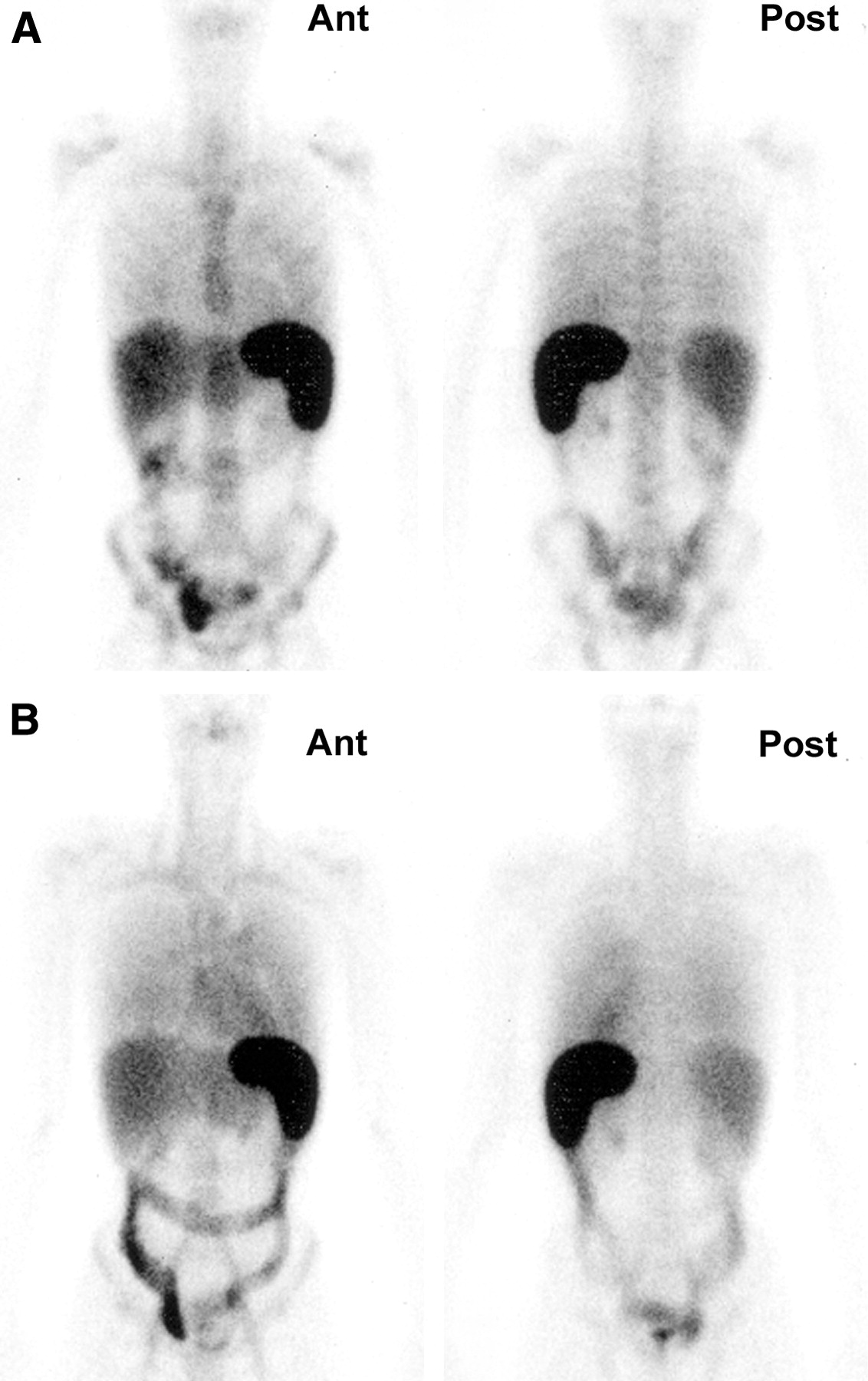
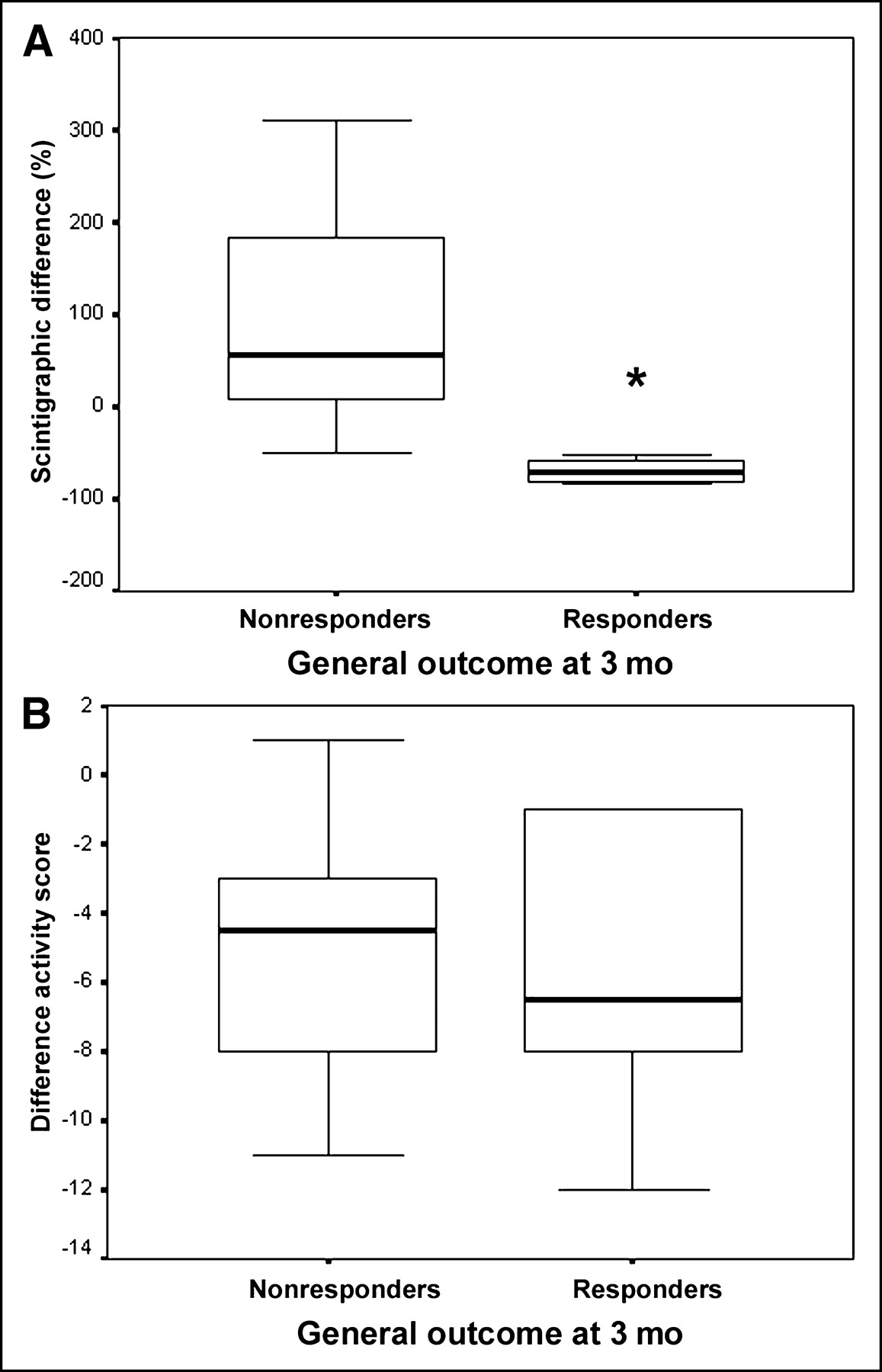
In the group of nonresponders, 10 patients had an increase in the SAS of >10%, 2 patients had an unchanged SAS, and 2 patients had a decreased SAS of >10% (Fig. 4) but had a residual mean segmental WBC SPECT uptake ratio of >1.5. The difference in ΔSAS between responders and nonresponders was statistically significant (P < 0.01; Fig. 5A). There was no significant difference in ΔSAS between nonresponders requiring altered management or colectomy (data not shown). There was no significant difference in response between treatment groups.
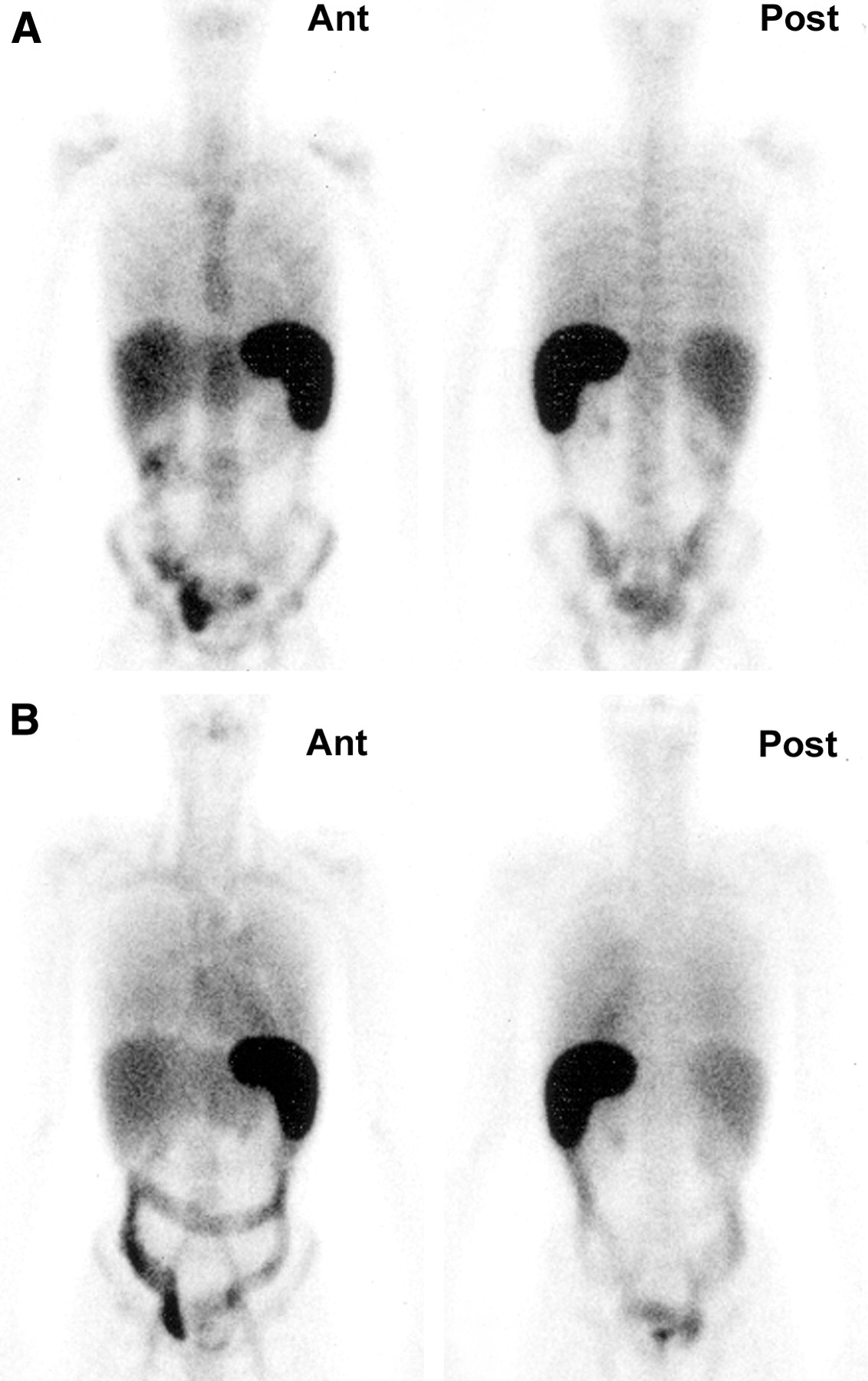
99mTc-HMPAO WBC whole-body scintigraphy (patient 14) in anterior (Ant) and posterior (Post) views before therapy (A) and 1 wk after beginning therapy (B). Scintigraphy before treatment shows mild-to-severe colitis in 5 segments. Scintigraphy 1 wk after treatment shows markedly increased uptake with severe colitis in 5 segments.

(A) Box plots (median and interquartile range) of percentual difference between SAS before and 1 wk after beginning therapy (ΔSAS). Difference in ΔSAS between responders and nonresponders is significant (*P < 0.01). (B) Box plots of difference between clinical activity score before and 1 wk after beginning therapy. Difference in clinical score evolution between responders and nonresponders is not significant.
For clinical assessment by means of the clinical activity score, the difference between responders and nonresponders was not significant (Fig. 5B; clinical activity score [mean ± SEM], −5.83 ± 1.78 and −4.71 ± 0.93, respectively).
DISCUSSION
WBC scintigraphy has been used for several decades as a diagnostic tool for IBD (22–24). 111In-Labeled granulocytes have been replaced by 99mTc-HMPAO-labeled granulocytes to yield a rapid, simple, nontraumatic, and effective technique with an acceptable radiation dose (10,25–27). It has been shown that 99mTc-HMPAO WBC scintigraphy is superior to the activity index of van Hees and the gastroenterologist’s clinical opinion for diagnosing active inflammation in patients with IBD (11). The sensitivity and specificity of 99mTc-HMPAO WBC scintigraphy are very high (94%–100%) for active disease (11,28,29). Furthermore, it was recently reported that disease severity can be determined adequately by planar scintigraphy in patients with a severe attack of UC and that WBC scintigraphy is able to assess disease activity and extent without the need for colonoscopy (10). Unlike 99mTc-HMPAO WBC scintigraphy, 99mTc-LeucoScan (Immuno-medics) lacks sensitivity and has no place in the assessment of gastrointestinal inflammation in IBD (30,31).
Where planar 99mTc-HMPAO WBC scintigraphy has proven to be reliable to assess disease extent when compared with histologic findings (32,33), we have recently shown that the disease activity in the rectum can also be assessed with accuracy by scintigraphy (10). However, planar scintigraphy has inherent inaccuracies due to variable depth and overlapping activities. SPECT has the advantage to overcome these problems and the use of 99mTc-HMPAO SPECT for detection and quantification of acute bowel inflammation has been extensively described by Weldon (19). The determination of maximum segmental bowel uptake and calculation of an uptake ratio to bone marrow yield a noninvasive, objective, and accurate approach to the assessment of disease activity.
We used histologic findings from biopsy specimens obtained in the most severely affected areas in the rectosigmoid before and 1 wk after therapy as the gold standard for disease activity. The sensitivity of WBC scintigraphy for identifying rectosigmoid involvement of UC in this series of selected patients was 100%, which is in accordance with our previous observations (10). However, the study population is a selected one with severe colitis and it is known that WBC scintigraphy can be false-negative in patients with only slight macroscopic changes (34,35). No controls were included in this study to assess the sensitivity of WBC scintigraphy in the full spectrum of clinical activity of IBD. There was a good correlation between disease activity in the rectosigmoid determined on histology and planar scintigraphy. There was an even better correlation for disease activity determined on SPECT.
Several attempts have been made to predict responsiveness of UC exacerbations to initial therapy (3,7,36). These techniques are based on clinical and laboratory observations to identify patients likely to require intensified or altered therapy or, ultimately, colectomy. The correlation of a clinical index with other variables—such as CRP; the erythrocyte sedimentation rate (ESR); or endoscopic, histologic, or scintigraphic scores—for the extent and severity of disease is not always reported as significant (37). Clinical indices have an inherent subjectivity, resulting in a less reliable activity score (28). Laboratory parameters such as CRP and ESR reflect inflammation in general, and conflicting results concerning the predictive value have been reported (38).
Scintigraphic assessment of disease activity correlates very well with histologic disease activity assessment (10,19). This was reconfirmed in this study, both before and after treatment. The summed SAS represents the maximum inflammatory activity detected in each segment of the entire colon reflecting histologic assessment, which is based on biopsies obtained from the most macroscopically severely affected areas of each segment (19). Because the correlation between histologic and scintigraphic disease activity assessment is that good, it seems appropriate to use scintigraphy for disease activity assessment.
The difference between the SAS before and 1 wk after treatment was predictive for remission up to 3 mo after beginning therapy without change of therapy. This would not have been possible with the clinical activity score alone. In our series, a decrease in the SAS of >50% of the initial value and a SPECT uptake ratio of ≤1.5 per segment (representing not more than moderate disease) (19) are predictive of remission without the need for altering therapeutic management. In our series, nonresponders have a 36% probability of colectomy in the following weeks, which does not differ from other observations (3).
CONCLUSION
Repeated 99mTc-HMPAO SPECT seems able to predict therapy resistance in UC within 1 wk after beginning treatment. This technique provides a noninvasive and reliable tool to monitor therapy in UC and depict nonresponders in an early stage, where intensifying therapy or changing management or, ultimately, colectomy is possible without losing valuable time and increasing risk of dangerous complications.
Footnotes
Received Nov. 20, 2003; revision accepted Apr. 12, 2004.
For correspondence contact: Roelof J. Bennink, MD, PhD, Department of Nuclear Medicine, Academic Medical Center, P.O. Box 22700, 1100 DE Amsterdam, The Netherlands.
E-mail: r.bennink{at}amc.uva.nl
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Imaging of Inflammation by PET, Conventional Scintigraphy, and Other Imaging Techniques
- Imaging of Inflammation by PET, Conventional Scintigraphy, and Other Imaging Techniques
- Role of Modern Imaging Techniques for Diagnosis of Infection in the Era of 18F-Fluorodeoxyglucose Positron Emission Tomography
- Dedicated Pinhole SPECT of Intestinal Neutrophil Recruitment in a Mouse Model of Dextran Sulfate Sodium-Induced Colitis