


Abstract
This study assessed the radiation dosimetry of 99mTc-labeled ethylene dicysteine (EC) C225 (EC-C225), a promising radioligand for functional tumor imaging. Methods: Whole-body scanning was performed on 6 patients with head and neck squamous cell carcinoma up to 24 h after administration of 99mTc-EC-C225. Alternate patients who had been randomized to receive C225 in a phase III trial received 99mTc-EC-C225 before their 20-mg test dose or after their 400 mg/m2 loading dose of unlabeled C225 (patients 1/3/5 and 2/4/6, respectively). Radiation dosimetry was assessed using the MIRD method. Results: The critical organ was the kidney, with an average radiation-absorbed dose for all 6 patients of 0.0274 mGy/MBq. The average total-body absorbed dose was 0.0022 mGy/MBq (0.243 cGy/1,110 MBq). Conclusion: The new radiopharmaceutical 99mTc-EC-C225 appears to have reasonable dosimetric properties for a diagnostic nuclear medicine agent. Correlation of the imaging results with clinical findings is the next step.
One factor indicating a poor prognosis in patients with squamous cell carcinoma of the head and neck is upregulation of the epidermal growth factor receptor (EGFR) (1–8). Antibody therapy, in a single modality or in combination with radiation or chemotherapy, directed against EGFR-expressing tumors (e.g., C225) is under investigation in the laboratory and clinic (9–23). Proper selection of patients for such therapy would likely improve the therapeutic ratio. Unfortunately, squamous cell carcinoma of the head and neck can grow quite large, and biopsy of a single portion of a tumor may not be representative.
Our goal was to develop a noninvasive imaging procedure that could detect tumors that express EGFR. For this purpose, 99mTc-labeled C225 was synthesized at our institution with an ethylene dicysteine (EC)-based chelation technique (EC-C225) (24). Technetium was chosen because of its low energy, short half-life (6 h), and low cost and because tumor does not take up free 99mTc, unlike another candidate radionuclide, 111In. EC is a relatively small molecule (molecular weight, 260), which conjugates to C225 (molecular weight, >30,000). The chelation procedure does not affect the affinity of C225 for tumor or the cytotoxicity profile of C225 (24). The labeling procedure is easy and inexpensive, and the necessary γ-camera is commonly available.
Six patients already scheduled to receive concomitant treatment with radiation therapy and C225 (IMCL CP02-9815; ImClone Systems, Inc.) consented to undergo the experimental imaging with 99mTc-EC-C225. Based on the recommendation of the Food and Drug Administration, half the patients were given their loading dose of unlabeled C225 before the administration of 99mTc-EC-C225. Clinical radiation dosimetry data are reported below.
MATERIALS AND METHODS
Radiosynthesis of 99mTc-EC-C225
The linker EC was prepared in a 2-step synthesis according to methods described by Blondeau et al. (25) and Ratner et al. (26). Briefly, cysteine-HCl (41.52 g) was dissolved in water (106 mL). To this, formaldehyde was added (26.1 mL), and the reaction mixture was stirred overnight at room temperature. Pyridine (26.6 mL) was then added and the precipitate formed. The crystals were separated and washed with ethanol (54 mL) for 25 min at room temperature, then filtered with a Buchner funnel. The crystals were triturated with petroleum ether (150 mL), again filtered, and then lyophilized for 3 d. The precursor, l-thiazolidine-4-carboxylic acid (melting point, 195°C; reported, 196°C–197°C), was used for synthesis of EC. The precursor (22 g) was dissolved in liquid ammonia (200 mL) and refluxed. Sodium metal was added until a persistent blue color appeared. Ammonium chloride was added to the blue solution, and then the solvents were evaporated to dryness. The residue was dissolved in water (200 mL), and the pH was adjusted to 2 by adding concentrated hydrochloric acid. A precipitate was formed as a result of pH adjustment to 2. The solid was filtered and washed with water (500 mL). The solid, EC (melting point, 247°C; reported, 251°C–253°C), was dried in a calcium chloride desiccator. The structure was confirmed by 1H nuclear magnetic resonance and fast-atom-bombardment mass spectroscopy (mass-to-charge ratio, 268; molecule parent ion, 100).
Clinical grade anti-EGFR mAb C225 (IMC-C225) was obtained from ImClone Systems, Inc. C225 (20 mg) was stirred with EC (28.8 mg, 0.11 mmol in 1.4 mL of 1N NaHCO3), N-hydroxysulfosuccinimide (23.3 mg, 0.11 mmol), and 1-ethyl-3-(3-dimethylaminopropyl)carbodiimide-HCl (16.6 mg, 0.09 mmol). After dialysis, 17 mg of EC-C225 were obtained. Na99mTcO4 (3,700 MBq) was added to a vial containing 1 mg of EC-C225 and 100 μg of SnCl2, and the product was purified with a G-25 column and eluted with phosphate-buffered saline, yielding 2,960 MBq of 99mTc-EC-C225. Radiochemical purity was assessed by high-performance liquid chromatography (HPLC), using a sodium iodide detector and ultraviolet detector (254 nm). HPLC was performed on a gel permeation column (Biosep SEC-S3000, 7.8 × 300 mm; Phenomenex) eluted with 0.1% LiBr in pH 7.4 phosphate-buffered saline (10 mmol/L) at a flow rate of 1.0 mL/min. The retention time for 99mTc-EC-C225 was 10.2–10.6 min. In some samples, there was a second small peak (<10%) at 7.5 min, which might have been a lower-molecular-weight antibody. Radiochemical purity for 99mTc-EC-C225 was 90%–100%. Specific activity was 74 GBq/μmol.
An immunoassay (Western blot and immunoprecipitation) and cell proliferation assays were used to examine the integrity of EC-C225. Western blot analysis was also performed on A431 (high EGFR expression, positive control), MDA231 (medium EGFR expression), and MDA453 (poor EGFR expression, negative control) cell lines. DiFi cells are known to undergo apoptosis when exposed to C225 in culture; thus, they were used for cell viability assays. Cell viability was determined by measuring the optical absorbance of cell lysate at a wavelength of 595 nm and normalizing the value with the corresponding untreated cells. Our previous studies showed no marked changes in EGFR affinity and potency between EC-C225 and C225. Cellular uptake differed markedly between A431 and MDA231 cell lines. A431, a known EGFR expression cell line, showed higher uptake than did MDA231 (24).
Patient Eligibility
Patients with locally advanced squamous cell carcinomas of the head and neck who had been enrolled in a phase III trial (IMCL CP02-9815) and randomized to receive radiation therapy with concomitant C225 were eligible for this pilot study. This study (RO00-311) opened for patient accrual on January 16, 2001, and closed on April 5, 2002, after completion of the M.D. Anderson Cancer Center patient accrual goal for the phase III trial. During that interval, 8 patients were eligible for enrollment in RO00-311 but 2 declined participation.
Treatment Plan
99mTc-EC-C225 was administered during the morning of the day on which the 400 mg/m2 loading dose of C225 was scheduled (every other patient entered on this protocol starting with patient 1 = arm 1) or immediately after the loading dose of C225 (every other patient entered on this protocol starting with patient 2 = arm 2). Just before injection of the 99mTc-EC-C225, a whole-body transmission scan using a 57Co sheet source was obtained for every patient in arm 1, for attenuation correction of the 99mTc scans. To avoid delay between administration of the loading dose of C225 and administration of radiolabeled C225, patients in arm 2 underwent transmission scanning before administration of cold C225. At time 0, a mean of 925 MBq (range, 814–1,073 MBq) of 99mTc-EC-C225 was administered intravenously, immediately followed by the time 0 whole-body scan. With the exception of 1 patient (patient 5) who missed his 2-h scan because the camera was not available for research purposes, further whole-body scans were obtained at 2, 4, and 6 h after injection. To better assess renal dosimetry, the last 3 patients underwent whole-body imaging the morning after their injection of 99mTc-labeled C225. All patients voided immediately before the transmission scan and immediately before the scans obtained at 2, 4, 6, and 24 h after the time 0 injection.
The whole-body scans were obtained with a dual-detector γ-camera (e.cam; Siemens Medical Solutions USA, Inc.) over a scan length of 200 cm in approximately 20 min (10 cm/min), and the images were acquired into a 1,024 × 256 digital matrix. A board-certified attending nuclear medicine physician then read the images.
Radiation Dosimetry
The whole-body images were analyzed using the Nuclidose program (Northwestern University) to define regions of interest, construct time-activity curves, and estimate source organ residence times (27,28). For patient convenience, neither blood nor urine nor feces were collected in this phase I pilot study. Source organ fractions of injected activity versus time were computed from the serial anterior and posterior whole-body images using the geometric mean quantification method (29,30). First, attenuation correction factors were estimated from the ratio of organ region counts in a scan of the 57Co sheet source without the patient to organ region counts in the transmission scan. The square root of this ratio was raised to the power μ140/μ122 to convert to 99mTc attenuation, where μ140 and μ122 are the mass attenuation coefficients for 99mTc and 57Co, respectively. The camera sensitivity was measured by including a 10-mL vial containing a calibrated reference source of activity within the field of view of each patient’s whole-body scan. This sensitivity was then used to scale the 99mTc-emission organ region counts to convert them to absolute activity. Finally, for the fraction of injected activity in each source organ, the time-activity curve was fit to either a monoexponential or biexponential function, and the function was integrated analytically to calculate residence time. Estimates of the radiation-absorbed doses to the standard MIRD target organs were then computed using the MIRDOSE3 algorithms (31,32). In addition to absorbed dose estimates to the standard MIRD target organs, effective dose equivalent and effective dose were calculated. Source-organ residence times were estimated for the kidneys, liver, lungs, spleen, and remainder of the body. All other organs were considered targets of radiation only.
RESULTS
Labeling
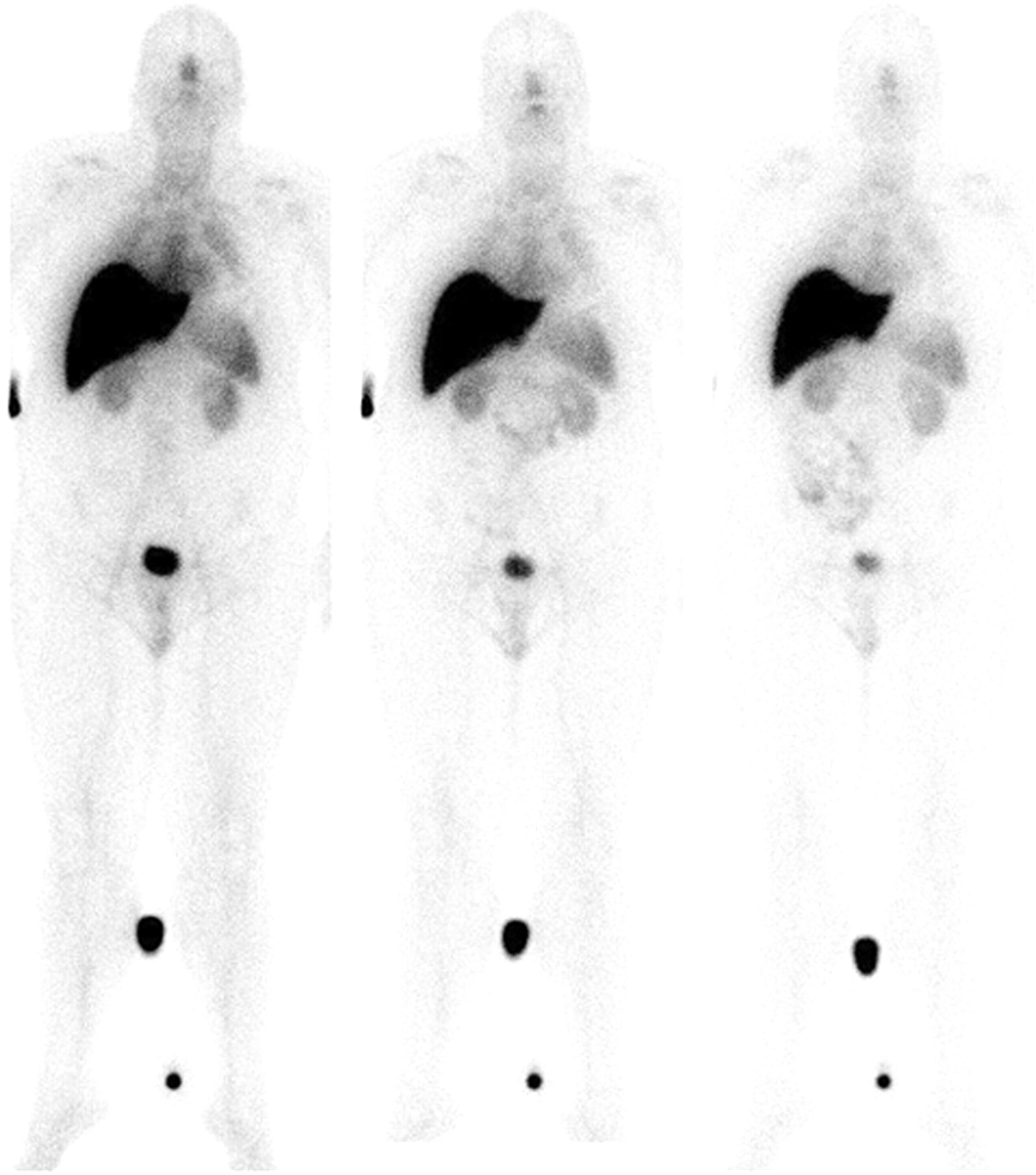
The labeling was excellent at first but appeared to decline over the course of the study. For the first 2 patients, there was no significant visualization of the thyroid, stomach, salivary glands, or saliva (Fig. 1). For the third patient, there was no significant visualization of the stomach, salivary glands, or saliva; however, the thyroid, which was not significantly visible at 2 h, became slightly visible at 4 h and more so at 6 h. For the fourth patient, there was no significant visualization of the stomach or saliva; however, there was mild visualization of the thyroid and salivary glands, suggesting the presence of some unlabeled free technetium or unstable labeled C225. For the fifth patient, there was no significant visualization of the thyroid or stomach, but there was some visualization of the salivary glands and saliva. The sixth patient’s scan was suboptimal overall, with significant visualization of the thyroid, stomach, salivary glands, and saliva.
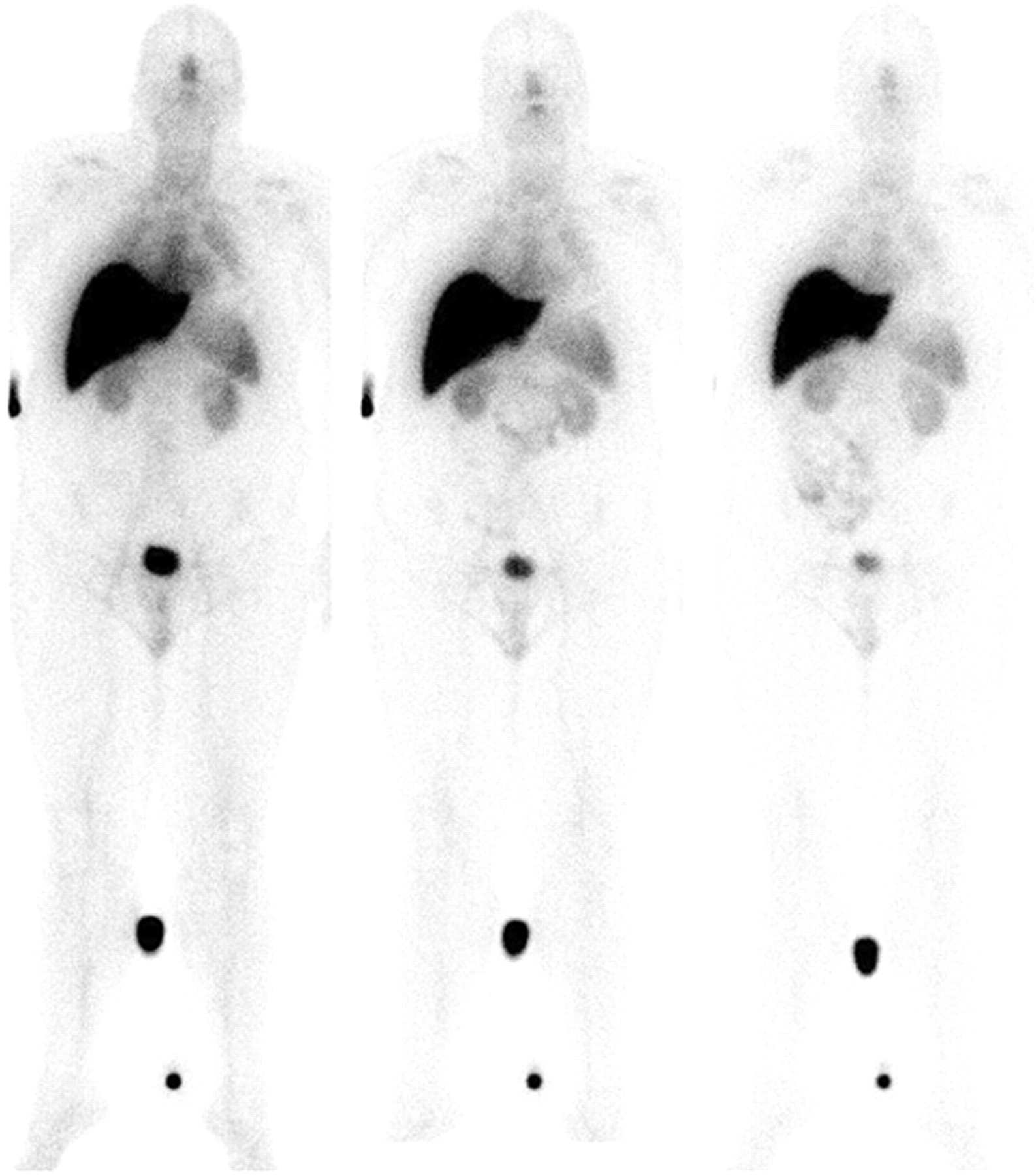
Whole-body coronal images obtained 2, 4, and 6 h (from left to right) after administration of 851 MBq of 99mTc-EC-C225 to a patient with squamous cell carcinoma of the head and neck—the first patient scanned with this compound.
As an aside, the first patient’s nasopharynx and fifth patient’s gallbladder were well visualized. Delayed visualization of the nasopharynx and gastrointestinal system, after 4 h, was noted for patients 5 and 6.
Target-Organ Dosimetry
The critical organ was the kidney, with an average absorbed dose for all 6 patients of 0.1014 cGy/mCi (0.0274 mGy/MBq) ± 22.9%. The average total-body absorbed dose was 0.0081 cGy/mCi (0.0022 mGy/MBq; 0.243 cGy/1,110 MBq) ± 19.2%. Table 1 shows the average absorbed dose for all 6 patients; for the 3 patients in arm 1 (without cold loading), that is, patients 1, 3, and 5; for the 3 patients in arm 2 (with cold loading), that is, patients 2, 4, and 6; and for the patients in arm 2 excluding patient 6. In Table 2, residence times are provided for the kidneys, liver, lungs, spleen, and remainder of the body.
Radiation Dosimetry: Mean Radiation Absorbed Dose for Each Target Organ ± SD (as % of Mean)
Radiation Dosimetry: Residence Times ± SD (as % of Mean)
Effective Dose Equivalent and Effective Dose
The mean effective dose equivalent for all 6 patients was 0.0222 cSv/mCi (0.006 mSv/MBq; 0.666 cSv/1,110 MBq) ± 24.3%. The mean effective dose for all 6 patients was 0.0138 cSv/mCi (0.004 mSv/MBq; 0.414 cSv/1,110 MBq) ± 15.5%. Table 3 shows the average effective dose equivalent and average effective dose for all 6 patients; for the 3 patients in arm 1 (without cold loading), that is, patients 1, 3, and 5; for the 3 patients in arm 2 (with cold loading), that is, patients 2, 4, and 6; and for the patients in arm 2 excluding patient 6.
Radiation Dosimetry: Effective Dose Equivalent and Effective Dose ± SD (as % of Mean)
DISCUSSION
Labeling was excellent overall, and at 90%–100%, radiochemical purity for 99mTc-EC-C225 was reasonable. Nine months transpired between administration of 99mTc-EC-C225 to the first patient and administration to the last patient. The seeming decline in labeling over that time may have been related to the second small peak (<10%) seen on HPLC at 7.5 min, consistent with the presence of a lower-molecular-weight antibody. The suboptimal study of the last patient was due to the accumulation of a significant amount of free 99mTc in the saliva and salivary glands; the presence of free 99mTc was corroborated by significant visualization of this patient’s thyroid and stomach on a whole-body scan.
The dosimetric estimates and especially average absorbed dose to the critical organ (0.0274 mGy/MBq) and to the whole body (0.0022 mGy/MBq [0.243 cGy/1,110 MBq]) indicate that the new radiopharmaceutical 99mTc-EC-C225 has reasonable dosimetric properties for a diagnostic nuclear medicine agent.
We do not have sufficient patient numbers to make a strong recommendation on whether cold loading should be used. Residence time in the liver appeared to be longer in patients with cold loading than in those without. One explanation could be that the liver does not have C225 binding sites but simply extracts whatever is not taken up elsewhere in the body. If the cold loading saturates many potential binding sites elsewhere in the body—leaving fewer nonliver binding sites to be labeled with 99mTc-EC-C225—the result would be more activity in the liver. If this is true, one may hypothesize that cold loading would be disadvantageous for the imaging of tumors.
CONCLUSION
The new radiopharmaceutical 99mTc-EC-C225 appears to have dosimetric properties that are reasonable for a diagnostic nuclear medicine agent. For best results, we recommend the fresh synthesis of EC-C225 before radiolabeling and scanning. Because C225 therapy is directed against tumors, which express EGFR, the imaging of patients with 99mTc-EC-C225 could potentially select good candidates for C225 therapy trials.
Acknowledgments
We are grateful for the dedicated efforts of our research nurse, Beth de Gracia; research assistant, Kristen Reynolds; and administrative assistants, Sylvia Kolojaco, Marie Turner, and Eloise Daigle. This work was supported by a grant from ImClone Systems Inc.
Footnotes
Received Mar. 19, 2004; revision accepted Jun. 2, 2004.
For correspondence or reprints contact: Naomi Schechter, MD, Department of Radiation Oncology, University of Texas M.D. Anderson Cancer Center, 1515 Holcombe Blvd., Box 97, Houston, TX 77030.
E-mail: nschecht{at}mdanderson.org
REFERENCES
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- Targeting Aberrant DNA Double-Strand Break Repair in Triple-Negative Breast Cancer with Alpha-Particle Emitter Radiolabeled Anti-EGFR Antibody
- Preparation, Biological Evaluation, and Pharmacokinetics of the Human Anti-HER1 Monoclonal Antibody Panitumumab Labeled with 86Y for Quantitative PET of Carcinoma
- Molecular imaging of Bcr-Abl phosphokinase in a xenograft model
- Disparity Between In Vivo EGFR Expression and 89Zr-Labeled Cetuximab Uptake Assessed with PET
- Preparation and Evaluation of 68Ga-DOTA-hEGF for Visualization of EGFR Expression in Malignant Tumors