


Abstract
A myocardial remodeling in dilated cardiomyopathy (DCM) after partial left ventriculectomy (PLV) has been previously discussed. The aim of this study was to investigate the functional changes in the follow-up of patients with DCM undergoing PLV using electrocardiographically triggered perfusion SPECT (gated SPECT). Methods: Twelve DCM patients (10 men, 2 women; 56 ± 9 y [mean ± SD]), after successful PLV and mitral valve repair (PLV–MVR), were monitored by gated SPECT and echocardiography. Gated SPECT quantified end-diastolic volumes (EDV), end-systolic volumes (ESV), myocardial and scar volumes, as well as ejection fraction (EF) preoperatively, early (38 ± 28 d), and late (296 ± 130 d) after PLV–MVR. Results: EDV and ESV showed an immediate reduction after PLV–MVR (EDV from 542 ± 90 mL to 350 ± 81 mL, P < 0.001; ESV from 452 ± 91 mL to 254 ± 79 mL, P < 0.001) with no significant change in the late follow-up (EDV late, 316 ± 63 mL; ESV late, 207 ± 63 mL; both P = not significant vs. early follow-up). PLV–MVR immediately improved EF (preoperative, 16.8% ± 5.5%; early, 28.8% ± 7.6%; P = 0.003) with no significant change in the late follow-up (36.0% ± 9.4%; P = not significant vs. early follow-up). Conclusion: In this highly selected DCM patient group, gated perfusion SPECT assessed early responses in volumes and EF after PLV–MVR. However, although statistically nonsignificant in the small patient group, ESV and EDV were further decreased, whereas EF improved toward 1 y, coinciding with the improvement of clinical symptoms (New York Heart Association), potentially indicating a functional remodeling after PLV–MVR. Further studies in larger patient cohorts and longer follow-up are warranted.
The prevalence of end-stage heart failure has increased in the past and is expected to increase worldwide even more in the future (1). In cases of refractory congestive heart failure, where even optimal medical treatment is not sufficient, the only definite therapeutic option is a heart transplantation, which is severely limited by donor availability (2).
As surgical alternatives to cardiac allografts, techniques such as mechanical left ventricular assist devices, xenografts, cardiomyoplasty, and, more recently, partial left ventriculectomy (PLV)—the so-called Batista procedure—have been developed. The latter was originally developed by Batista et al. (3,4) and modified by others (5) for surgical treatment of patients with end-stage dilated cardiomyopathy (DCM). Within PLV, a large portion of the left ventricular wall (usually the free wall) is resected to reduce the diameter of the left ventricle, often in combination with mitral valve repair (MVR) or replacement (6).
Several clinical studies have described the functional and clinical outcome of patients after PLV using 2-dimensional echocardiographic measurements of the left ventricular end-diastolic/end-systolic diameters (LVEDD/LVESD) and of ejection fraction (EF) (3,5,7,8).
However, these parameters are primarily modified by the reduction of the left ventricular diameter itself and therefore cannot assess cardiac function with respect to functional recovery of the left ventricular myocardium. It has been suggested that improvement of cardiac function after PLV should be defined by absolute indices of cardiac volumes, such as end-diastolic volume (EDV) and end-systolic volume (ESV) and stroke volumes, or of cardiac performance, such as exercise capacity (9).
The aim of this study was to investigate cardiac function and morphology in a highly selected group of patients with dilative cardiomyopathy undergoing PLV and MVR (PLV–MVR). For this purpose, this study used noninvasive electrocardiographically (ECG)-triggered myocardial perfusion scintigraphy (gated SPECT), uniquely able to assess myocardial perfusion, cardiac function, and parameters of cardiac morphology (myocardial volume, scar volume) in a single scan.
MATERIALS AND METHODS
Patients
Inclusion Criteria.
Patients were enrolled in this study on the following inclusion criteria: idiopathic DCM; severe heart failure, New York Heart Association (NYHA) functional class III or class IV refractory to maximal medical therapy; mitral insufficiency ≥ grade 2; left ventricular end-diastolic diameter > 7 cm; cardiac index < 2.5 L/min/m2; and maximal O2 consumption (VO2max) < 14 mL/kg/min.
Exclusion Criteria.
Routine coronary angiography was used to exclude coronary artery disease as the cause of the cardiomyopathy. Patients were excluded from the study if they did not fulfill all of the inclusion criteria.
Patients who were found to be candidates for cardiac transplantation and for PLV–MVR were given both options. All patients were offered the option of continuing with medical therapy while being listed for heart transplantation. Patients were advised that mechanical circulatory support and heart transplantation would be made available if PLV–MVR proved ineffective either acutely or chronically. If heart failure improved constantly in the postoperative course and criteria for heart transplantation were no longer fulfilled, patients were removed from the waiting list.
Based on these criteria, 12 patients (10 men, 2 women; age, 56 ± 9 y [mean ± SD]; range, 38–70 y; median, 57 y) were chosen from the referrals to our heart failure and transplant center over a period of 2 y to undergo PLV–MVR.
All patients gave informed consent and were approved by the local Interdisciplinary Heart Failure and Transplant Committee consisting of cardiologists, heart surgeons, and psychologists. Preoperative clinical characteristics of all study patients are summarized in Table 1.
Preoperative Clinical Characteristics
PLV–MVR
The operative technique used a modification of the original Batista procedures published earlier (3–5). Briefly, after a median sternotomy and initiation of a cardiopulmonary bypass, ventriculectomy was performed, typically removing a myocardial segment of the lateral wall between the anterior and posterior papillary muscles of the left ventricle.
For mitral valve reconstruction, intraoperative transesophageal echocardiography was performed to select the appropriate procedure. Annuloplasty using a Cosgrove–Edwards ring (10) (Baxter Healthcare Corp.) was performed in 2 patients, an Alfieri procedure (11) was performed in 5 patients, and a combination of both was performed in 5 patients.
Postoperatively, individual heart failure medication (maximal therapy including digitalis, nitrates, diuretics including spironolactone, angiotensin-converting enzyme inhibitors, and β-blockers) was resumed.
Noninvasive Cardiac Imaging in Follow-Up of PLV–MVR
Noninvasive investigations of morphologic parameters using echocardiography before as well as 3 mo (early) and 12 mo (late) after PLV–MVR were performed as part of the routine follow-up protocol in all patients. Moreover, the protocol included gated perfusion SPECT preoperatively, early (38 ± 28 d), and late (296 ± 130 d) after PLV–MVR. Although the study protocol aimed for SPECT at all time points, this could not be achieved for all patients due to logistics and patient compliance. Furthermore, 2 patients died in the follow-up. Therefore, a total of 7 patients did have all SPECT examinations preoperatively as well as in the follow-up of PLV–MVR.
Echocardiography
Echocardiographic measurements were performed according to the recommendations of the ACC/AHA Guidelines for the Clinical Application of Echocardiography (12).
M-mode data were acquired in the parasternal long-axis view shortly before surgery, 3 mo (early) and 12 mo (late) after surgery, following the leading edge–to–leading edge rule. Measured data were analyzed using algorithms of the standard software package of the ultrasound machine (Sonos 5500, Software Package B1; Phillips).
Gated Perfusion SPECT
ECG-triggered attenuation-corrected myocardial SPECT started 1 h after intravenous injection of 400 MBq 99mTc-tetrofosmine (Myoview; Amersham Buchler GmbH & Co. KG) under resting conditions (2 heads, 24 projections, 64 × 64 matrix, 180° orbit, 50 s per step, 8 gates, zoom factor = 1.45; butterworth filter: cutoff = 0.6, order = 5; E.Cam, Siemens Gammasonics). To correct for potential photon attenuation occurring in the massively enlarged hearts of the patients with severe heart failure enrolled in this study, all images were acquired with attenuation correction using the E.Cam profile attenuation system. All patients received their standard daily medication before the application of the radiopharmaceutical.
Perfusion was visually analyzed by 2 experienced nuclear medicine physicians who were unaware of the patient’s history. For analysis of cardiac contractile function as well as left ventricular volumes, the endocardial/epicardial contours of the left ventricle (elastic membrane surface model) of the ECG-triggered acquisition were derived using an automated contour-finding algorithm, described recently (13,14). EF, EDV, and ESV were calculated from the dynamic volumes encompassed by the endocardial surface of the left ventricle. In addition, the volume of the left ventricular myocardium was measured as the volume difference between the epicardial and endocardial surfaces of the left ventricle. This volume was finally divided into viable myocardium (myocardial volume, regional perfusion ≥ 50% of maximal left ventricular perfusion) and scar tissue after PLV–MVR (<50% of maximal left ventricular perfusion).
Statistics
For statistical analysis, Student unpaired t tests for equal/unequal variances (Levene test) were used (SPSS 10.0; SPSS Inc.). P < 0.05 was considered significant.
RESULTS
Echocardiography was performed preoperatively in all 12 patients, whereas 9 of these were investigated early and 8 of these late after PLV–MVR. A total of 8 patients had a complete serial echocardiographic follow-up. Gated SPECT was done in 8 patients before PLV–MVR, 8 patients early and 8 patients late after PLV–MVR. A total of 7 patients had a complete serial scintigraphic follow-up. Data and statistics in the Results are based on all patients measured at each time point with echocardiography and gated SPECT.
All 12 patients enrolled showed significant improvement of symptoms early (3 mo) after PLV–MVR with further improvement until 12 mo (NYHA class: preoperatively 3.2 ± 0.3, 2.6 ± 0.2 at 3-mo follow-up, P = 0.002 vs. preoperative; 2.1 ± 0.2 at 12-mo follow-up, P = 0.003 vs. 3 mo).
One-year survival in the group studied was 83.3% (10/12) with no immediate death during or close to surgery. One patient died of multiorgan failure 2 wk after PLV–MVR. Another patient died at home 10 mo postoperatively of a sudden cardiac death of unknown origin.
Echocardiography
The degree of mitral insufficiency was reduced from 2.3 ± 0.5 preoperatively to 1.1 ± 0.7 early after PLV–MVR (P = 0.002) and remained steady until the end of the first postoperative year (0.9 ± 0.6, P = not significant [ns]). The improvement in mitral valve function was not correlated with the technique used for MVR. LVEDD showed a significant reduction from 8.2 ± 0.8 cm preoperatively to 6.8 ± 0.6 cm early after PLV–MVR (P = 0.001) with no significant change thereafter (late: 6.6 ± 0.3 cm, P = ns). LVESD was reduced from 6.7 ± 0.9 cm preoperatively to 5.9 ± 0.4 cm at early follow-up (P = 0.027) with no significant change toward late follow-up (5.5 ± 0.6, P = ns vs. early follow-up).
The thickness of the interventricular septum and the posterior wall as well as the fractional shortening did not change from preoperatively to early and late follow-up. Echocardiographic data are displayed in Figure 1.

LVEDD (A) and LVESD (B) diameters before, early (3 mo), and late (12 mo) after PLV–MVR measured by echocardiography. Numbers in bars represent number of patients investigated for each time point (8 patients were measured serially). *P < 0.05; **P < 0.01; ***P < 0.001; ns equals P = not significant.
Gated Perfusion SPECT
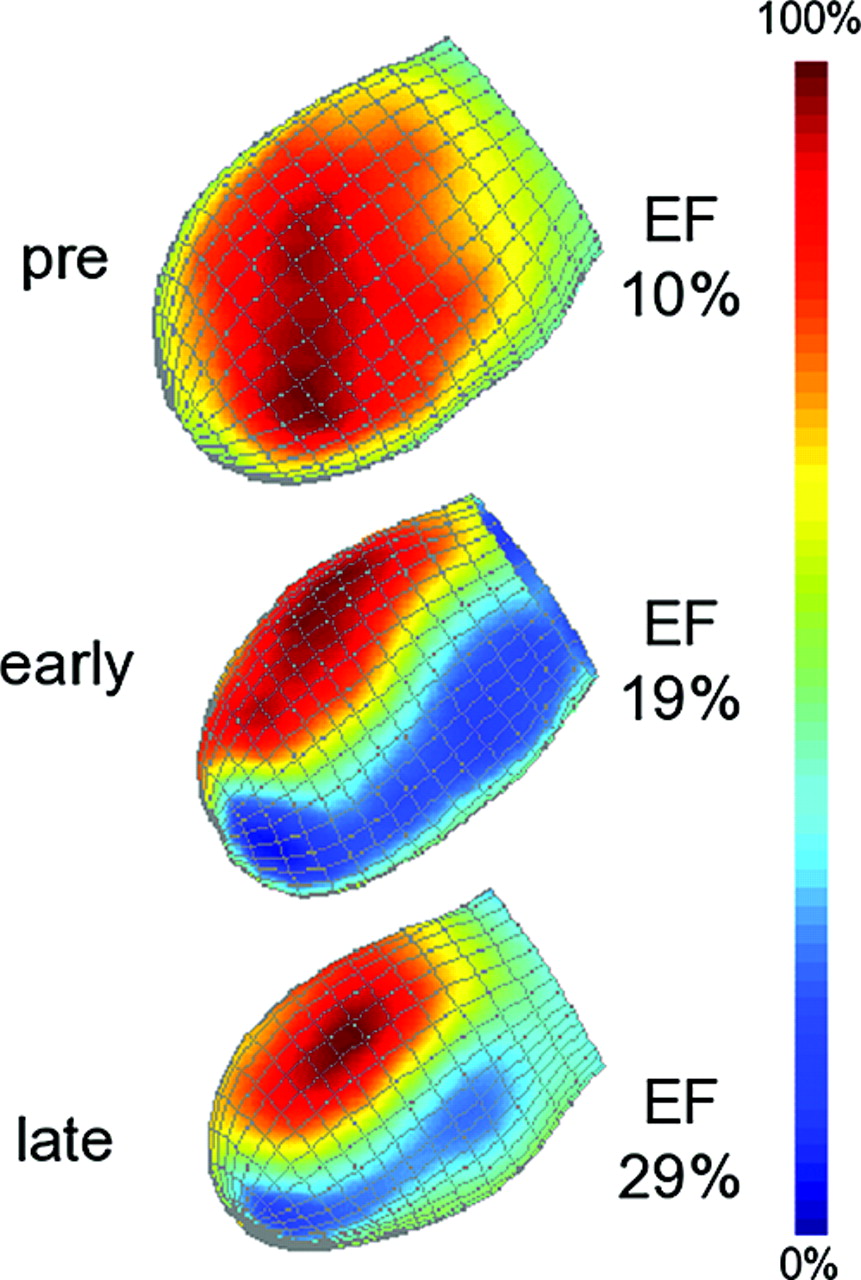
Because the selected patients had end-stage heart failure, logistic problems and patient compliance occasionally hampered and prevented the realization of the gated perfusion SPECT. However, gated perfusion SPECT was performed in 8 patients preoperatively (17 ± 23 d before surgery), 8 patients early (38 ± 28 d after surgery), and 8 patients late (296 ± 130 d after surgery) after PLV–MVR. Of these, only 7 had a complete serial scintigraphic follow-up. In all patients, preoperative gated perfusion SPECT showed no sign of local myocardial scarring or impaired resting perfusion. A typical example of a preoperative and follow-up myocardial scintigram is given in Figure 2.
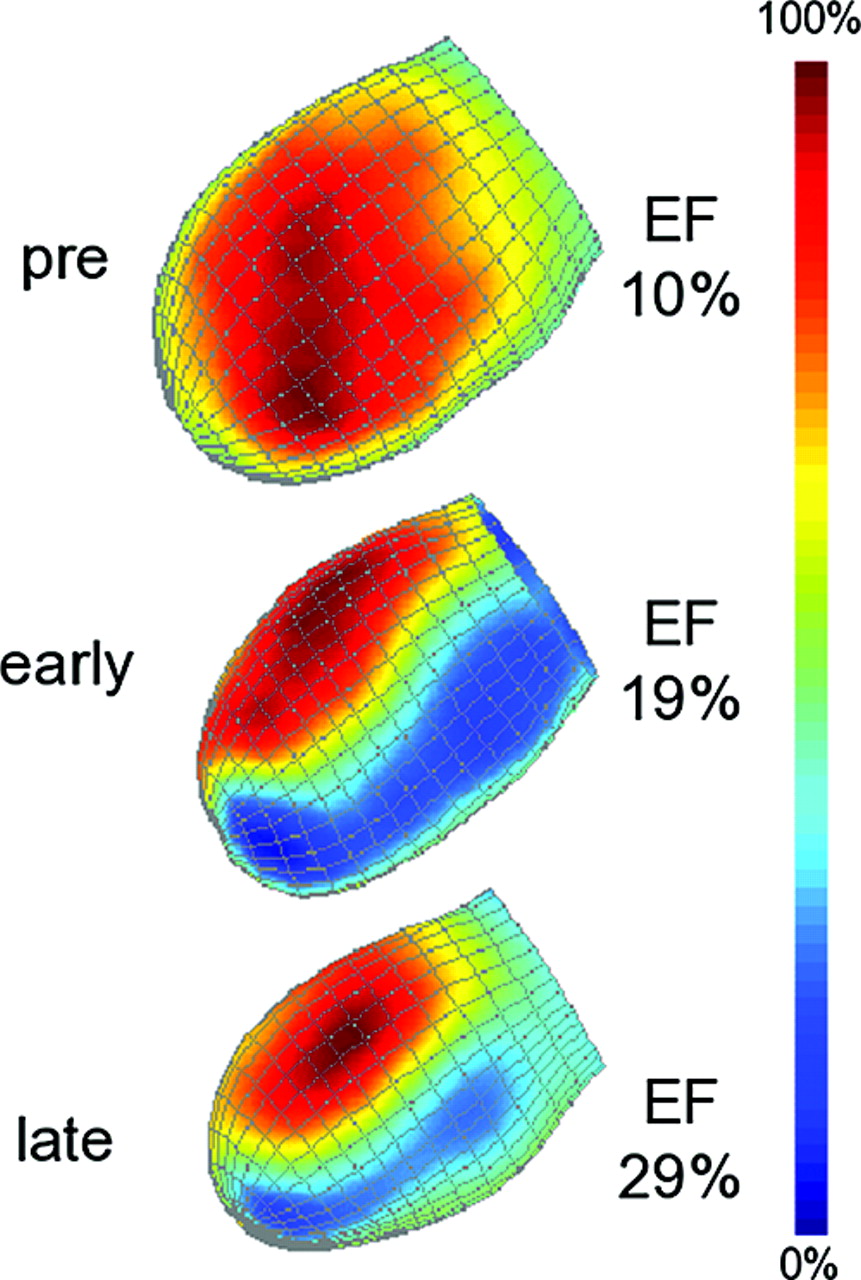
Three-dimensional left ventricular reconstruction (lateral view, end-diastolic image) projecting regional myocardial perfusion measured by gated SPECT preoperatively (pre) as well as 1 mo (early) and 12 mo (late) after PLV–MVR. Note that posterolateral scar in area of surgical suture after surgery seems to shrink in time interval from 1 to 12 mo.
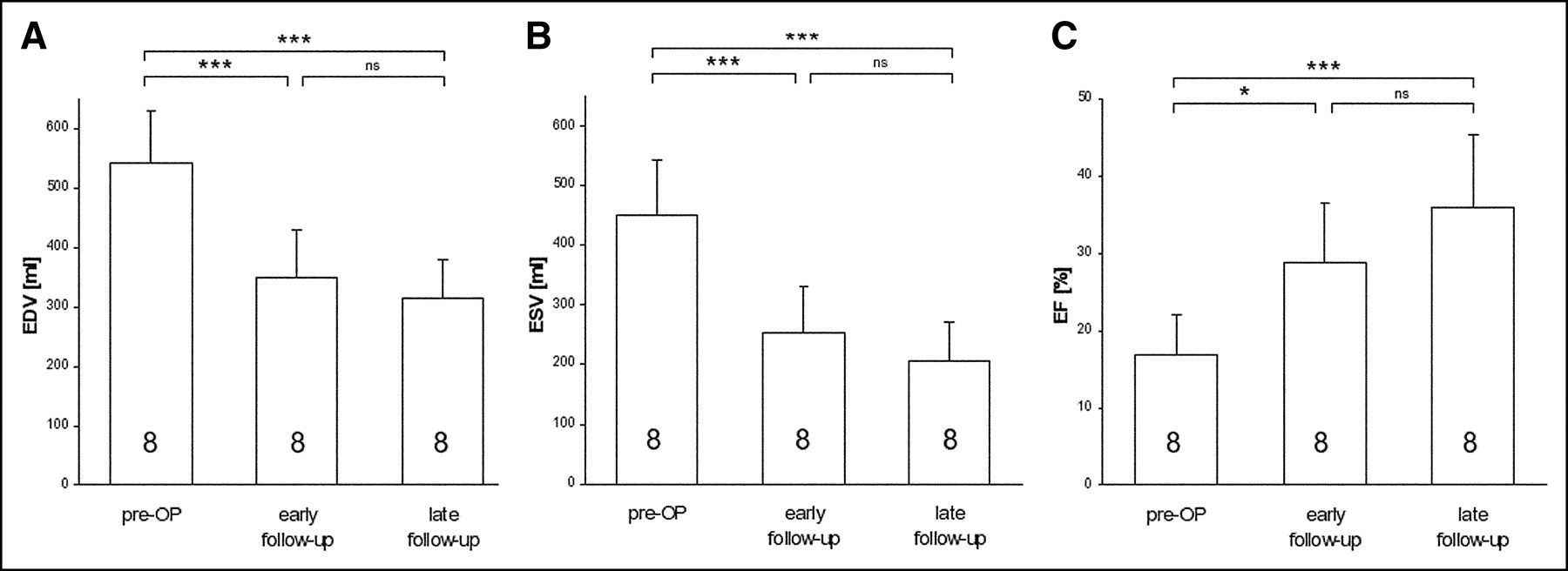
EDV and ESV showed a significant reduction from preoperative to early follow-up (EDV, 542 ± 90 mL vs. 350 ± 81 mL, P < 0.001; ESV, 452 ± 91 mL vs. 254 ± 79 mL, P < 0.001). There was no significant change in EDV and ESV from early to late follow-up (EDV late, 316 ± 63 mL; ESV late, 207 ± 63 mL, P = ns vs. early for both) (Figs. 3A and 3B).
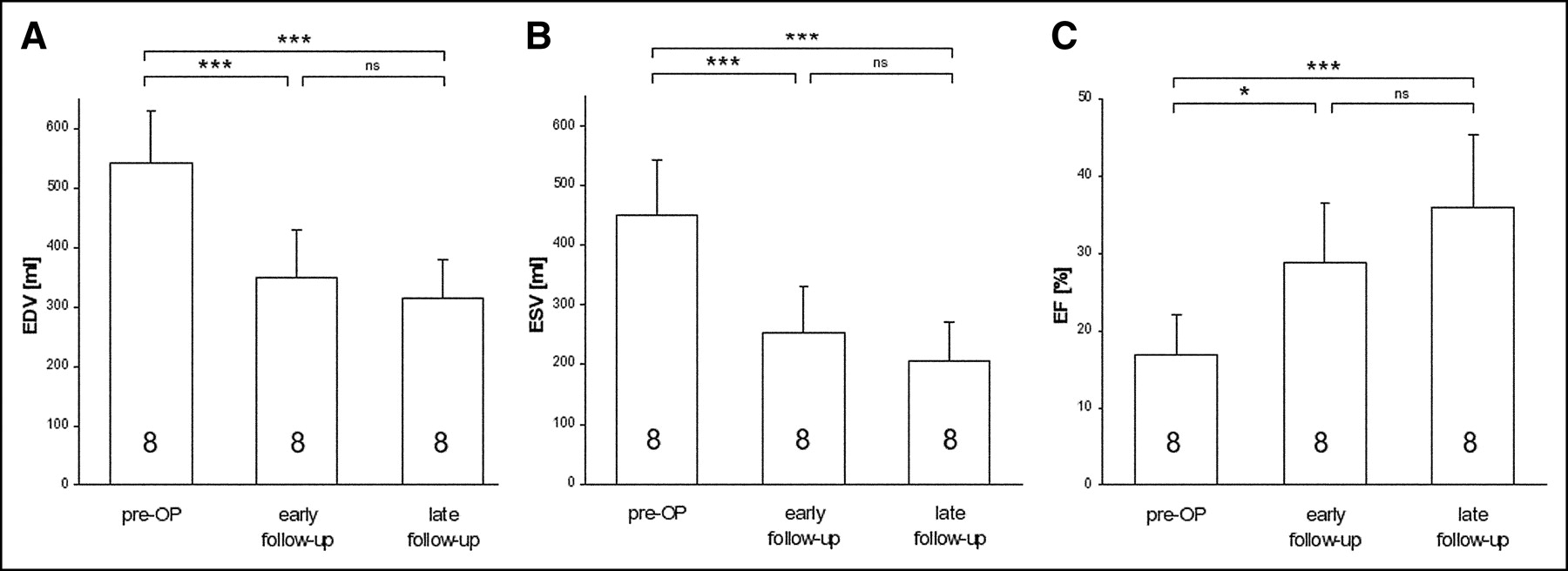
Results of gated perfusion SPECT before (17 ± 23 d) as well as early (38 ± 28 d) and late (296 ± 130 d) after PLV–MVR. End-diastolic (EDV, A) and end-systolic (ESV, B) left ventricular volumes and EF (C) are displayed. Numbers in bars represent number of patients investigated for each time point (7 patients were measured serially). *P < 0.05; ***P < 0.001; ns equals P = not significant.
PLV–MVR immediately improved EF (16.8% ± 5.5% preoperatively vs. 28.8% ± 7.6% at early follow-up, P = 0.003) with no change toward late follow-up (36.0% ± 9.4%, P = ns vs. early) (Fig. 3C).
The left ventricular myocardial volume was immediately reduced by PLV–MVR (430 ± 61 mL preoperatively vs. 194 ± 57 mL at early follow-up, P < 0.001) and remained stable until the late follow-up (late follow-up, 189 ± 44 mL; P = ns vs. early follow-up) (Fig. 4A). Regional scar volumes were not present in all patients before surgery, which is in line with the fact that these patients did not suffer from ischemic heart disease but all had idiopathic DCM. Scar volume due to scar tissue forming in response to the surgical resection of the free wall of the left ventricle in the area of the surgical suture, defined by perfusion <50%, was 111 ± 30 mL early after PLV–MVR and did not change significantly toward late follow-up (90 ± 41 mL, P = ns vs. early follow-up) (Fig. 4B).
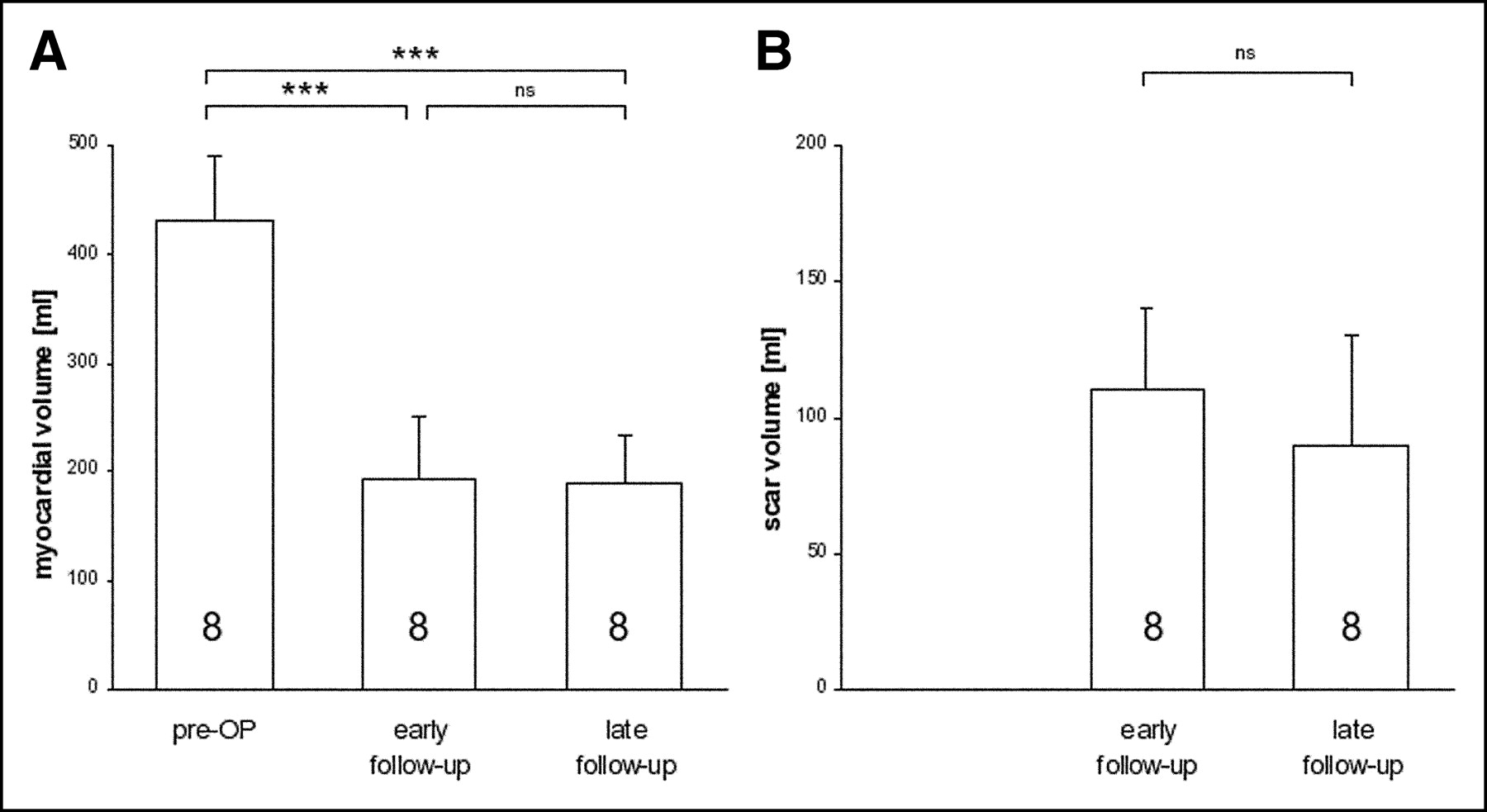
Results of gated perfusion SPECT before (17 ± 23 d) as well as early (38 ± 28 d) and late (296 ± 130 d) after PLV–MVR. Myocardial volume (A) and scar volumes (B) are displayed. Numbers in bars represent number of patients investigated for each time point (7 patients were measured serially). ***P < 0.001; ns equals P = not significant.
DISCUSSION
PLV is a surgical technique by which a section of the left ventricular muscle of dilated cardiomyopathic hearts in end-stage heart failure is resected (3). This procedure reduces the left ventricular muscle mass, which leads to an immediate decrease of left ventricular diameters. According to the law of Laplace, this reduction in size acutely results in a significant decrease in wall tension, which was predicted in a mathematic simulation model of PLV (9) as well as shown in patients using pressure–volume loops (15).
PLV is known to improve symptoms in about 60% of all patients with typical improvement from NYHA stages III–IV preoperatively to class I or class II postoperatively in early and midterm follow-up (5,7,16).
The clinical improvement seems to correlate with patient selection (7,17). Furthermore, it was hypothetized that a concomitant MVR should improve the outcome after PLV. However, Bocchi et al. (6) and Kawaguchi et al. (18) investigated the effect of concomitant MVR on the outcome after PLV comparing results in patients with and without MVR. They concluded that MVR does not have a beneficial effect on the functional outcome after PLV. Thus, the beneficial effects of PLV seem to be related to volume reduction rather than abolished mitral insufficiency. In the present study, all patients underwent PLV in combination with MVR. Although the technique of MVR was different in subgroups of patients, this should therefore not influence the results.
Based on the proposed criteria, this study enrolled a small, but highly selected, patient group (idiopathic DCM, no coronary artery disease, no myocardial scarring, elective operation, and so forth) assumed to result in the best outcome after PLV–MVR (16). In line with previous findings, the NYHA class improved early after PLV–MVR. However, in contrast to other studies, the NYHA class further improved in the selected group of patients investigated here toward 1 y after PLV–MVR. The successful selection is furthermore reflected by the excellent survival (10/12; 83%) in the first postoperative year, which is consistent with the best results reached in previously published studies (7,19) as well as the typical survival after heart transplantation (20,21).
Multiple studies have aimed to measure the effects of PLV–MVR on morphologic and functional parameters early or late after surgery; however, only a few measured these parameters serially in the follow-up. Furthermore, in the majority of studies either morphologic or functional parameters were assessed in the follow-up without combining both. Therefore, significant questions remain concerning a potential remodeling of the left ventricle induced by PLV–MVR.
PLV is assumed to immediately reduce LVEDD/LVESD by 10%–20% early after surgery with no further change in the follow-up (8,17,19). In this study, LVEDD was reduced by ∼16% and LVESD was reduced by ∼12% early after PLV, which matches values measured in other studies.
Data on the changes in left ventricular volumes after PLV are most often based on 2-dimensional techniques and have rarely been published. McCarthy et al. (19) found a reduction of EDV from 327 ± 124 cm3 preoperatively to 179 ± 73 cm3 1 y after PLV, and Schreuder et al. (15) found an acute reduction from 141 ± 27 mL/m2 preoperatively to 68 ± 16 mL/m2 2 d and to 65 ± 6 mL/m2 5 d after PLV. In parallel, ESV was reported to be decreased early (8) (127 mL/m2 preoperatively to 60 mL/m2 14 d after PLV) and late (17) (162.6 ± 41.6 mL/m2 preoperatively to 88.5 ± 45.8 mL/m2 1 y after PLV) after PLV.
Gated perfusion SPECT, which is uniquely able to noninvasively measure functional parameters as well as regional perfusion in a single scan (22), was used in the follow-up of PLV–MVR. This technique overcomes drawbacks of other techniques working 3-dimensionally, largely user independent and semiautomatically analyzable.
Comparable to previous studies and in line with the echocardiographic measurements of left ventricular diameters in this study, EDV and ESV were immediately decreased by ∼40% early after PLV–MVR. However, although not statistically significant, there was a trend toward lower EDV (−10% vs. early) and ESV (−19% vs. early) from early to late follow-up after PLV–MVR in this highly selected patient cohort. These trends in EDV and ESV most interestingly match the improvement in NYHA stages from early to late time points observed here but were much more pronounced than trends in echocardiographic measurements of LVEDD (−3% vs. early) and LVESD (−7% vs. early).
As expected from other studies in humans and animal models of PLV (4,5,7,23), PLV in combination with MVR resulted in an immediate increase of EF. Again, EF showed a nonsignificant upward trend (+25%) from early to late follow-up, matching the improvement in NYHA class.
However, NYHA assessment was available in 10 patients after 1 y, whereas only 8 patients were measured by gated SPECT at the late follow-up, which could explain the lack of significance of the trends in cardiac volumes and EF.
Left ventricular myocardial volume, introduced here as a measure of myocardial muscle mass, was immediately reduced by PLV–MVR with no further change in the follow-up until 1 y, consistent with previous findings (24). Furthermore, echocardiographic measures of the septal and posterior wall thickness did not change in the 1-y follow-up in this study. A previously discussed remodeling of the left ventricular myocardium with respect to changes in myocardial muscle mass is therefore not supported by the findings of this study.
Regional scar volumes were not present in all patients before surgery, which is in line with the fact that these patients did not suffer from ischemic heart disease but all had idiopathic DCM. However, scars were detected in the follow-up after PLV–MVR due to scar tissue forming in response to the surgical resection of the left ventricular free wall in the area of the surgical suture (Fig. 2). The volume of these scars (although not significant in the small group) seems to decrease from early to late follow-up, potentially indicating shrinking of the scar after PLV–MVR. This might explain, in part, the trend toward lower EDV and ESV from early to late follow-up measurements.
In summary, gated perfusion SPECT, applied here in patients undergoing PLV–MVR, measured an immediate reduction of EDV and ESV with a concomitant increase in EF. In contrast to previous studies, we investigated functional and morphologic effects in a highly selected patient group with idiopathic DCM. In this group, we measured downward trends of EDV and ESV as well as an upward trend of EF toward the 1-y follow-up, in line with a significant clinical improvement as assessed by NYHA class. This might indicate a further improvement of cardiac function in the first postoperative year. Studies with longer follow-up and larger patient cohorts are warranted.
This study investigated a small number of patients undergoing PLV–MVR. However, these patients were carefully selected and were closely followed by echocardiography and gated perfusion SPECT, which were not used in previous studies.
Although the follow-up protocol aimed for gated perfusion SPECT in all patients, gated perfusion SPECT was performed at baseline or follow-up after PLV–MVR in only a subgroup of patients (7 patients with all time points) due to several limitations (death, logistics, patient compliance, and so forth). This might explain why trends in functional parameters, such as EDV/ESV and EF from early to late follow-up, did not reach statistical significance.
Gated perfusion SPECT is a elegant technique by which left ventricular perfusion and volumes can be measured. This technique is limited by the relatively low spatial resolution of the imaging system, potentially leading to a partially incorrect measurement of absolute volumes compared with a 3-dimensional morphologic, high-resolution approach such as magnetic resonance tomography. Overall, a good correlation of EDV and ESV measured by gated SPECT with results from magnetic resonance tomography was shown (25). However, on an individual basis, values can be heavily influenced by the patient characteristics (25). On the other hand, gated perfusion SPECT overcomes drawbacks of other imaging techniques, working completely 3-dimensionally and widely user independent.
In the present study, a group of patients was monitored and investigated serially by gated SPECT. In this setup, serial intraindividual functional changes in individuals are of importance, which are usually not influenced to the same extent by a patient-dependent over- or underestimation of the imaging technique as in interindividual studies.
The measure of myocardial volume was introduced here and is not yet validated against magnetic resonance tomography or echocardiography. Therefore, this measure must be discussed with caution. However, because this measure relies on the endocardial and epicardial contour detection validated for calculation of ESV and EDV, it should in principle be reliable. A validation against magnetic resonance tomography should follow in the future.
CONCLUSION
In patients with idiopathic DCM undergoing PLV–MVR, a significant reduction of ESV and EDV as well as an increase of EF were found early after surgery, as assessed by gated SPECT. However, in this highly selected patient group, a trend—though not statistically significant probably due to sample size—toward decreased EDV and ESV and increased EF matching significant improvement of clinical symptoms (NYHA) in the late follow-up of 1 y was present. This may be indicative of a midterm improvement of the cardiac function after PLV–MVR and warrants further gated perfusion SPECT investigations with longer follow-up intervals and larger patient cohorts.
Acknowledgments
We are most grateful to Christine Bätza for analyzing the gated myocardial perfusion SPECT data. Michael Schäfers, MD, and Jörg Stypmann, MD, contributed equally to this study. This study was supported in part by the Herzzentrum Münster e.V., Münster, Germany, and the Interdisziplinäres Zentrum für Klinische Forschung Münster, Germany (IZKF, BMBF-01KS 9604, project grant B10).
Footnotes
Received Jan. 15, 2004; revision accepted Apr. 12, 2004.
For correspondence or reprints contact: Michael Schäfers, MD, Department of Nuclear Medicine, Hospital of the Westfälische Wilhelms-University, D-48129 Münster, Germany.
E-mail: schafmi{at}uni-muenster.de
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.