


Abstract
To investigate changes in cerebral blood flow (CBF) and blood volume induced by acetazolamide (ACZ) in patients with a variable autoregulatory status responding to reduced perfusion pressure, PET measurements of hemodynamic parameters were performed on patients with cerebrovascular disease, and the relationships between the parameters were evaluated. Methods: Sixteen patients with unilateral major cerebral arterial occlusive disease underwent PET studies with 15O-gas and the steady-state method to obtain hemodynamic parameters in the brain. All patients and 8 healthy volunteers underwent H215O PET at baseline and 10 min after ACZ injection to calculate the CBF and arterial-to-capillary blood volume (V0) based on a 2-compartment model. Results: The regional CBF (rCBF) and V0 increased significantly after ACZ administration in volunteers and in the hemisphere contralateral to the ischemic side in patients. However, in a subgroup of patients with disease who showed a significant reduction in the rCBF increase in the ipsilateral hemisphere, the ACZ challenge caused a decrease in the rCBF even though the V0 showed a significant increase. The reduction in the rCBF increase was associated with an asymmetric increase in oxygen extraction fraction (OEF) but not with an absolute OEF increase. Conclusion: The increases in rCBF and V0 induced by ACZ administration, as well as absolute OEF value in the baseline condition, did not necessarily parallel each other in the ipsilateral hemispheres of patients. Thus, the increase in rCBF after ACZ challenge may not represent vasodilatory capacity in patients with cerebrovascular disease, especially in the regions with a reduced rCBF response.
The vasodilatory capacity of the cerebral circulation as measured by the cerebrovascular response to a vasodilatory stimulus has been evaluated using methods that measure cerebral blood flow (CBF) or blood velocity. The test for acetazolamide (ACZ), one of the vasodilatory stimuli, has been reported to be useful for evaluating and predicting the risk of cerebral ischemia in patients with major cerebral arterial occlusive diseases (1–3). Our previous study with healthy volunteers proved that changes in CBF were accompanied by changes in arterial-to-capillary blood volume (4), which was represented by a parameter of the vascular distribution volume (V0) (4,5). However, in the varying hemodynamic conditions observed in cerebrovascular disease, which shows a variable degree of cerebral autoregulatory vasodilatation in response to reduced perfusion pressure, it still remains unknown whether a similar parallel response to ACZ is observed in the 2 parameters. The relationship between arterial vasodilatation and an increase in regional CBF (rCBF) in the affected part of the brain in those patients seems more complicated than that observed in the normal brain. A comparison of changes in rCBF and V0 induced by a vasodilatory stimulus would provide information on the relationship between blood flow and vasodilatory capacity, as well as show whether a reduction in rCBF in the affected part of the brain, the so-called steal phenomenon, is caused by an unchanged arterial vascular volume.
The CBF response to ACZ may reflect the residual capacity for arteriolar resistance after a vasodilatory stimulus. In patients with major cerebral arterial occlusive disease, the CBF is often not increased after ACZ administration, presumably because autoregulation has already caused maximal vasodilatation in response to a reduced perfusion pressure. The steal phenomenon, a decrease in rCBF after ACZ administration instead of an increased or unchanged CBF (6,7), is presumed to be caused by the redistribution of blood to areas where vasodilatation can still occur, at the expense of the regions where vasodilatation is already at its maximum. However, the mechanism of the steal phenomenon after ACZ administration is not yet clear, and whether the reduction in rCBF is associated with no increase in blood volume or vasodilatory capacity has not been shown. The steal phenomenon may also result from changes in the relative distribution of arterial perfusion pressure caused by regional differences in vasodilatory capacity, if the regional blood volume increases after ACZ administration.
In the present study, PET was performed to investigate whether ACZ-induced changes in CBF and V0 in the impaired hemisphere of patients with cerebrovascular disease are different from those in normal circulation. The changes in rCBF and V0 were compared between the 2 hemispheres of patients and among subject groups. In addition, the relationship between the CBF response and other hemodynamic parameters in patients was studied. The ACZ test may be substituted for PET measurements of oxygen extraction fraction (OEF) and cerebral blood volume (CBV), which is considered to be a standard index for determining the degree of hemodynamic impairment (8,9). However, whether this test is valid for quantitative assessment of maximum cerebral autoregulatory vasodilatation is still controversial (10). The purpose of this study was to evaluate whether measurement of CBF in the ACZ test reflects the vasodilatory capacity and other hemodynamic parameters measured using PET.
MATERIALS AND METHODS
Subjects
Sixteen patients (12 men and 4 women) aged 54–74 y (mean ± SD, 65.1 ± 7.4 y) with unilateral major cerebral arterial occlusive disease underwent PET studies with the 15O-gas steady-state method and the H215O-bolus method. Only patients with an occlusion or 99% stenosis in the unilateral internal carotid artery (ICA) or in a middle cerebral artery (MCA) were included in the study. These findings should be appropriate to the accompanying symptoms of transient ischemic attacks (TIA) or a nondisabling stroke. The clinical information for the patients studied is summarized in Table 1. Because only half of the 16 volunteers recruited in the previous PET study had the CBF measured 10 min after the ACZ challenge, as done in this study (4), PET data of 8 healthy volunteers (4 men and 4 women; mean age ± SD, 26.0 ± 5.6 y) were used as the control. The study was approved by the Ethical Committee of the Shiga Medical Center, and written informed consent was obtained from each subject before the study.
Clinical Information for Patients with Occlusive Cerebrovascular Disease
PET Procedures
All subjects underwent PET scanning with an ADVANCE scanner (General Electric Medical Systems), which permits simultaneous acquisition of 35 image slices with interslice spacing of 4.25 mm. Performance tests showed the intrinsic resolution to be 4.6–5.7 and 4.0–5.3 mm in the transaxial and axial directions, respectively. A transmission scan was obtained using 68Ge/68Ga for attenuation correction before tracer administration, and the PET data were reconstructed using a Hanning filter (4,11).
The subjects were positioned on the scanner bed with their heads immobilized using a head holder. A small cannula was placed in the left brachial artery for blood sampling. The patients underwent PET scanning using the bolus method with H215O and dynamic data acquisition, followed by the 15O-gas steady-state method as described in detail elsewhere (11). An additional H215O-bolus scan was obtained 10 min after the ACZ injection. Healthy volunteers underwent PET studies with H215O, 15O2, and C15O using the bolus method (4). For the CBF measurement with bolus H215O injection, a 3-min dynamic PET scan was started at the time of tracer administration, with frame durations of 5 s × 12, 10 s × 6, and 20 s × 3, and radioactivity in the arterial blood was counted continuously using an automatic radioactivity counter (Pico-Count; Bioscan Inc.). The arterial blood was drawn using a Bio-minipump (AC-2120; Atto Co.) at a constant rate of 7 mL/min for the first 2 min, followed by manual sampling of arterial blood every 20 s during the rest of the scan time. Radioactivity counted by the automatic radioactivity counter was calibrated with that of the blood sampled manually, and delay and dispersion for the external tube were corrected (12). Decay of the radioactivity from PET and blood data was corrected to the starting point of each scan. CBF images were calculated from the dynamic PET data and arterial blood curves by means of the 3-weighted integral method (5,13). V0 images (mL/100 g) were calculated simultaneously from the bolus H215O PET data using the 3-weighted integral method (4,5,13).
In the steady-state method, the subjects inhaled C15O2 and 15O2 continuously for approximately 10 min, and static data were then acquired for 5 min to obtain images of the CBF (mL/min/100 g), OEF (%), and cerebral metabolic rate of oxygen (CMRO2; mL/min/100 g) (11,14). Each subject also inhaled a single dose of C15O to obtain a CBV image (mL/100 g) (11). Arterial blood was sampled during each procedure, and the radioactivity in the blood was immediately measured with a scintillation counter. During continuous inhalation of 15O2, the radioactivity of whole blood and plasma was counted from the sampled blood. For calculation of the CMRO2, the total arterial O2 content (tO2c), as well as the arterial tensions for CO2 (PaCO2) and O2 (PaO2), and pH were measured. The blood pressure of each subject was measured continuously through the arterial line and displayed on a monitor during the PET study. For the calculation of CBV from the C15O data, a cerebral–to–large-vessel hematocrit ratio of 0.85 was used (15,16). After the 15O-gas scans, ACZ (1.0 g) in 10 mL of saline was administered intravenously over 1 min. The changes in CBF and V0 were measured 10 min after the ACZ administration using the same procedure as for measurement of the baseline CBF with H215O.
Data Analysis
Regional values for each parametric image in the 16 patients were determined using multiple regions of interest (ROIs) drawn on the individual cortical territories of the right and left MCA. A total of 30 small circular ROIs (10 mm in diameter) were drawn in each hemisphere through several slice levels and were applied to all parametric images for each subject. In patients with infarction in the cerebral cortex, the ROIs corresponding to the infarct area were excluded from analysis by referring to MR images (9). The regional values thus obtained were averaged among all ROIs in each hemisphere for each parameter. Differences in rCBF and V0 between the baseline and after-ACZ-administration conditions for the 2 hemispheres were compared statistically using repeated-measures ANOVA. Each hemodynamic parameter was also compared statistically between the 2 hemispheres in the 16 patients using repeated-measures ANOVA. Differences in rCBF and V0 between patients and healthy volunteers for each condition were compared as hemispheric differences using 1-way ANOVA with a post hoc comparison using Fisher’s protected least significant difference. Because CMRO2 and OEF images in healthy volunteers were calculated using the different method (the bolus method) (4), these values were not compared between patients and volunteers. Any relationship between the 5 hemodynamic parameters measured in patients, and the percentage change in CBF and V0, were also examined using a linear regression analysis with an F test.
Patients were divided into 2 groups according to the percentage change in rCBF obtained from the ACZ challenge in healthy volunteers. The lower limit percentage in the rCBF increase was defined from the mean ± 2 SDs of the percentage increase in the 16 hemispheres of 8 volunteers, the interval that is expected to include 95% of the entire population of healthy subjects. Group A consisted of patients who showed less of an increase in rCBF than the threshold determined above, and the rest of the patients were defined as group B. The differences in rCBF and V0 between the 2 conditions, and the differences in each parameter between the 2 hemispheres, were compared for each group using repeated-measures ANOVA.
When a difference was detected by repeated-measures ANOVA, a post hoc comparison was performed using a paired t test. A probability value of less than 0.05 was considered to indicate a statistically significant difference. The Bonferroni method for multiple comparisons was applied to the threshold probability value of a paired t test to keep overall α equal to 0.05 when testing multiple null hypotheses.
RESULTS
The overall pattern of changes in the physiologic variables measured in the 16 patients at baseline and after ACZ administration was similar to that of the healthy volunteers studied for our previous report. Of the 6 physiologic parameters, tO2c (0.167 ± 0.020 [at baseline] and 0.173 ± 0.020 [after ACZ]) and PaO2 (76.7 ± 10.97 mm Hg [at baseline] and 90.2 ± 11.7 mm Hg [after ACZ]) were significantly different between the baseline and ACZ-challenge conditions (P < 0.001). Mean blood pressure and PaCO2, which may affect the CBF values, did not change during the study.
Figure 1 shows the changes in rCBF and V0 in the cortical territories of the right and left MCAs at baseline and after ACZ administration. Four of the 16 patients showed a reduction in rCBF in the ipsilateral hemisphere of the occlusive artery after the ACZ injection, although the V0 in all 4 patients increased on the same side. The hemispheres contralateral to the arterial occlusion showed regional values and changes in both rCBF and V0 similar to those in healthy volunteers. The mean regional values for each hemisphere in the patients and in the 16 hemispheres of the 8 healthy volunteers are given in Table 2. Both hemispheres in the patients showed a significant increase in rCBF and V0, although the percentage change in rCBF was significantly smaller in the ipsilateral hemisphere than in the contralateral hemisphere (P < 0.005) or in healthy volunteers (P < 0.001). The rCBF and V0 in patients were significantly different between the 2 hemispheres for both conditions (P < 0.001). The increase in V0 was significantly smaller in the ipsilateral hemisphere of patients than in the contralateral hemisphere (P < 0.001) or in healthy volunteers (P < 0.01).

Bilateral changes in rCBF and V0 in cortical territories of MCA before and after ACZ administration. Increase in rCBF and V0 for all patients was significant when before-ACZ administration was compared with after-ACZ administration, although 4 of 16 patients showed reduction in rCBF in ipsilateral hemisphere. V0 in all 4 patients increased on same side of hemisphere. Changes in patients of group A (•) are represented by dashed lines, and solid lines show changes in group B (×).
Regional Values of Each Parameter (Mean ± SD) in MCA Territories
Because the mean rCBF increase induced by ACZ in healthy volunteers was 37.5% ± 13.5%, 2 groups of patients were defined by the limit of a 10.5% (mean − 2 SDs) increase in rCBF in the ipsilateral hemisphere. Group A consisted of 8 patients who had a smaller increase in ipsilateral rCBF than the limit, and group B consisted of the other 8 patients. Mean values for each parameter and changes in rCBF and V0 for the 2 conditions are shown in Table 3. Absolute values of baseline rCBF and V0 were significantly different between the 2 hemispheres in both groups. The percentage change in rCBF did not differ between the 2 hemispheres in group B, and the difference between the 2 conditions was significant (P < 0.0001), whereas the rCBF in the ipsilateral hemisphere of group A was slightly decreased after ACZ administration, which provided an interhemispheric difference in rCBF change (P < 0.01). The percentage change in V0 showed a significant difference between the 2 hemispheres in both groups, although the absolute values were increased significantly in both hemispheres. Two representative images from group A are shown in Figure 2. The interhemispheric difference in rCBF and V0 was intensified in both cases, and the absolute rCBF values were decreased on the ipsilateral side, although the V0 was slightly increased in the same region. The corresponding OEF images for the 2 patients show an asymmetric increase in the ipsilateral hemisphere; however,one had an OEF in the normal range in the ipsilateral hemisphere, whereas another had a significantly greater OEF in the ipsilateral hemisphere. No relationship or tendency was observed between the time after onset and hemodynamic parameters measured by PET. All patients in group B had an event of stroke, whereas patients in group A tended to have a history of TIA (Table 1).

Representative images of patients with occlusion of right ICA in group A: patient with normal OEF values in bilateral hemispheres (A) and patient with significantly greater OEF in ipsilateral hemisphere (B). Interhemispheric difference in rCBF was intensified and absolute rCBF values decreased on ipsilateral side, although V0 was slightly increased in same region. Corresponding OEF images show asymmetric increase in ipsilateral hemisphere in both patients. Same color scale is used for same parametric images.
Comparison of CBF, V0, and Other Parametric Values (Mean ± SD) in the 2 Patient Groups
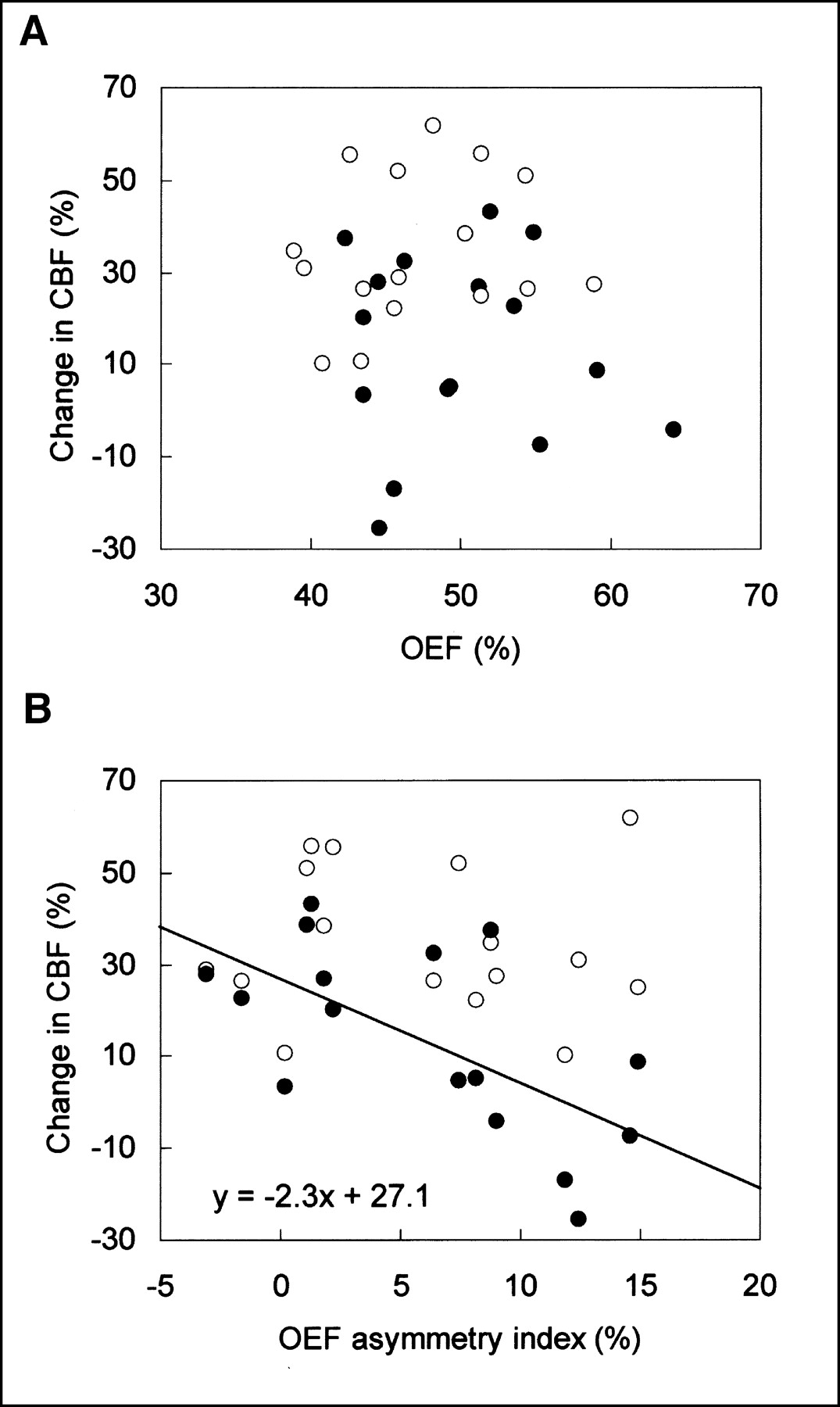
An asymmetric increase in the OEF in the ipsilateral hemisphere was observed in 9 patients (7 from group A and 2 from group B). However, only 3 showed a significant increase in absolute OEF greater than 52.9%, which is the upper limit of the normal range measured using the steady-state method on 7 healthy volunteers at our institute. One had a global OEF increase and showed a significant OEF increase in both hemispheres. Figure 3 shows the relationship between OEF and percentage changes in rCBF induced by ACZ administration. OEF in absolute values and the rCBF increase showed no relationship in either hemisphere; however, the asymmetry index for OEF ([ipsilateral − contralateral]/[contralateral] × 100%) was linearly correlated in the ipsilateral hemisphere (r = 0.64, F = 9.60 > F1,14 (0.95), P < 0.05). None of the other pairs of parameters measured in the current study showed any significant correlation in either hemisphere of the patients.
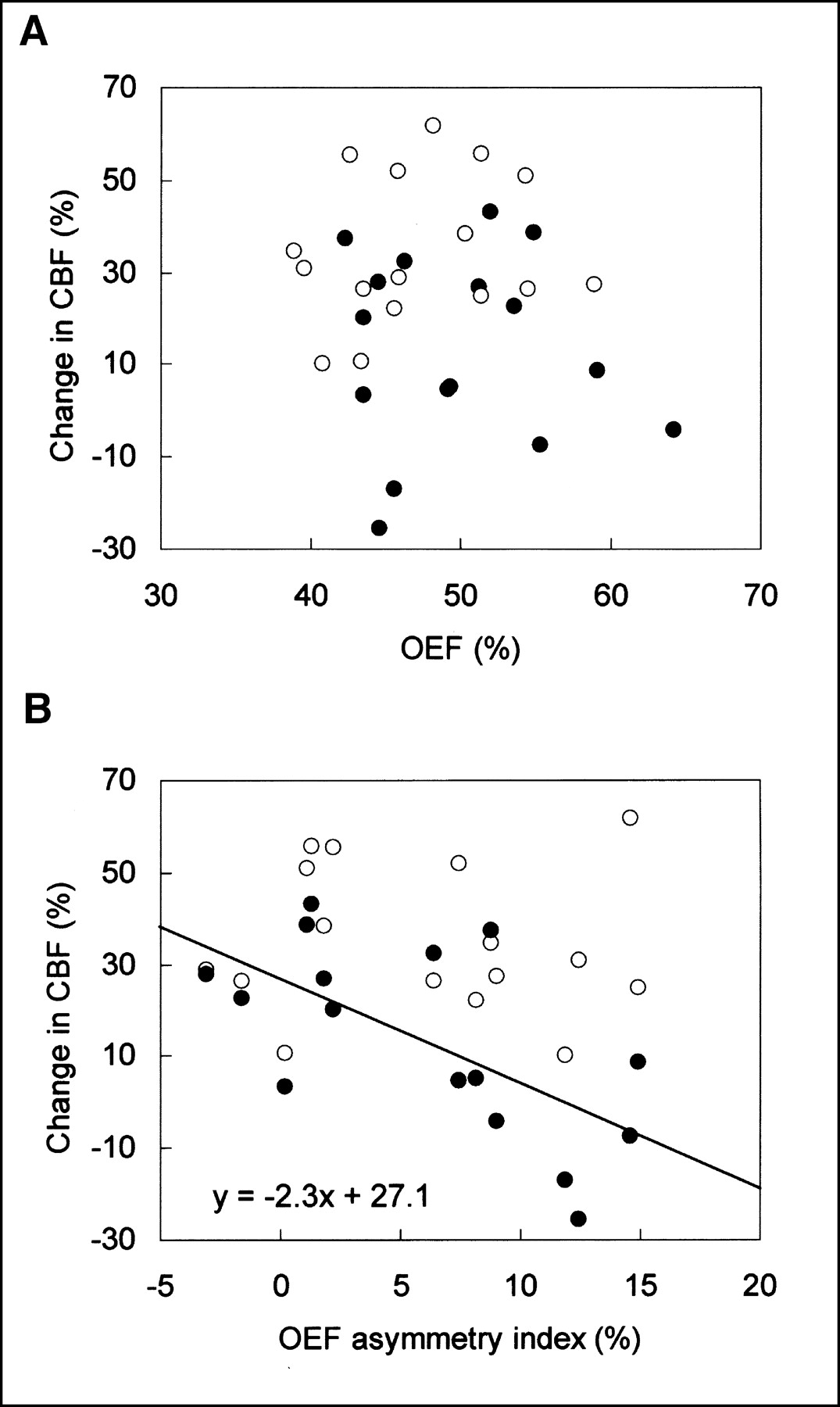
Relationship between OEF and percentage change in rCBF induced by ACZ administration. (A) Absolute OEF values and percentage change in rCBF showed no relationship in either ipsilateral (•) or contralateral (○) hemisphere. (B) Asymmetry index for OEF was linearly correlated only in ipsilateral hemisphere. Line is regression line for correlation in ipsilateral hemisphere (r = 0.64; P < 0.05).
DISCUSSION
The results of the current study on patients with unilateral major cerebral arterial occlusive disease demonstrated that the vasodilatory capacity, which is represented by an increase in V0, was not necessarily associated with the rCBF change in all patients, suggesting that the changes in rCBF induced by ACZ may not represent vasodilatation itself. Of the 16 patients involved in the present study, half showed a significantly smaller rCBF increase induced by ACZ in the ipsilateral hemisphere, compared with the contralateral hemisphere and the healthy volunteers. The definition of normal data is difficult, especially in aged subjects because they may have more or less sclerotic changes in the cerebral arteries. The control data obtained from younger healthy subjects who had no vascular lesions were presented as reference data to be compared with patients with impaired cerebral circulation. The contralateral hemisphere of patients showed rCBF and V0 similar to those of controls in both conditions, suggesting that sound cerebral circulation was preserved in this hemisphere. The patients were divided into 2 groups based on the ipsilateral rCBF response to ACZ, that is, a reduced-response group (group A) and a normal-response group (group B). The threshold for dividing the groups was determined by the data from younger healthy volunteers; that is, the groups were defined on the basis of normal cerebral circulation irrespective of the subjects’ age. Statistical errors are possible because of the difference in the mean age of the groups; however, the baseline rCBF and changes after ACZ challenge in the contralateral hemisphere were very close to those of healthy volunteers, suggesting that the threshold for group definition was appropriate. Furthermore, similar results for baseline rCBF and its ACZ-induced increase in middle-aged volunteers were reported in a recent study with PET (17).
The V0 in the ipsilateral hemisphere of group A increased significantly, although the mean rCBF in the same hemisphere was decreased to less than the baseline. The ACZ test is usually performed to evaluate cerebral vasodilatory capacity in patients with major cerebral arterial occlusive disease to determine whether neurosurgical treatment is indicated or to assess the effects of treatment (2,6,10). Our previous study with healthy volunteers proved that ACZ caused parallel increases in rCBF and V0 under normal hemodynamic conditions (4); however, as shown in the current study, the ACZ test with measurements of rCBF may not properly evaluate vasodilatory capacity in patients with cerebrovascular disease who have varied hemodynamic conditions.
The paradoxic reduction of rCBF—the so-called steal phenomenon—is presumed to be caused by a redistribution of blood from the areas where vasodilatation was already at its maximum. However, whether the steal phenomenon is associated with no change or a reduction in blood volume after ACZ administration has not been shown. This phenomenon may also result from a change in the relative distribution of arterial perfusion pressure caused by regional differences in vasodilatory capacity. A reduction in rCBF in the ipsilateral hemisphere after ACZ administration was observed in 4 patients, and the mean ipsilateral rCBF did not increase in group A. However, V0 increased in the right and left hemispheres of both patient groups as well as in the cortices of the 4 patients in whom the steal phenomenon was observed, indicating that in the cortices that showed significantly smaller increases or even reductions in rCBF, vasodilatory capacity remained. This result suggests that rCBF was reduced and redirected to the well-perfused areas or the contralateral hemisphere by the vasodilatory stimuli even in the cortices with preserved vasodilatory capacity. The percentage increase in V0 was significantly smaller in the ipsilateral hemisphere than on the contralateral side and may have caused the considerable difference in rCBF responses. A smaller interhemispheric difference in the V0 response to ACZ in group B than in group A did not yield a significant interhemispheric difference in the rCBF change. The remarkable interhemispheric contrast of rCBF images after ACZ injection tended to overestimate the reduction in vasodilatory capacity; thus, the intensified asymmetry of rCBF may not appropriately represent vasodilatory capacity. The ACZ test with qualitative images does not clarify these various hemodynamic changes and tends to overestimate the reduction in vasodilatory capacity. Thus, the test should be accompanied by quantitative measurements of rCBF in both conditions.
The baseline V0 values in the ipsilateral hemisphere of patients were significantly lower than those on the contralateral side and those of healthy volunteers, although the CBV in the same region was significantly greater than on the other side. A similar tendency was observed in our previous study of 7 patients with cerebrovascular disease, in which V0 in the ipsilateral hemisphere was slightly less than on the contralateral side (11). Arterioles in the affected cortices may not dilate sufficiently even after the reduction in perfusion pressure and may maintain the capacity for further dilation. The increase in V0 after ACZ administration in the ipsilateral hemisphere seems to support this speculation. The increase in baseline CBV despite the small change in V0 may largely be dependent on the passive venous dilatation due to a decrease in arteriolar resistance. The CBV increase in the ipsilateral hemisphere of cerebrovascular disease has been assumed to be caused by autoregulatory dilatation in arterioles to compensate for the reduction in perfusion pressure (8). However, the degree of increased blood volume seems too large if the change in CBV represents the increase in volume caused by dilation of the arterioles alone. Zaharchuk et al. estimated the increase in arteriole volume to be less than 3%–5% of the total CBV (18). In their report, a decrease of perfusion pressure caused an increase in total CBV, whereas the microvascular blood volume was significantly decreased. Although the hemodynamic conditions of their experimental hypotension would be different from those of the patients who had a chronic unilateral reduction in cerebral perfusion pressure, the results are consistent between the 2 studies.
Another explanation for the decrease in ipsilateral baseline V0 and the reduced vasodilatory capacity is that a metabolic impairment in the affected hemisphere may have provided insufficient vasodilatation and responsiveness against ACZ. The cause is considered to be neuronal impairment and a reduction in vascular density. Of the 4 patients who showed the steal phenomenon, 2 did not show an increase in OEF in the ipsilateral hemisphere, because the rCMRO2 in this area decreased. V0 was reduced in the baseline condition in such cortices, compared with the contralateral cortices. A possibility exists that the reduction in perfusion pressure in the ipsilateral cortices affected tracer kinetics and that, thus, the V0 value may have failed to reveal the precise part of the arteries that was dilated. However, time–radioactivity curves obtained from the right and left hemispheres did not show the time difference in tracer arrival (data not shown).
Several studies have investigated the relationship between OEF and rCBF in response to vasodilatory stimuli such as the ACZ test or CO2 inhalation (19–21), because the 15O-gas study is considered to be a reliable index for evaluation of cerebral hemodynamics, and the OEF values are closely related to the prognosis of those patients (9,22,23). In the present study, the percentage change in rCBF did not correlate with the absolute values of OEF, as is consistent with the previous report of Nariai et al. (24). However, the change correlated inversely with the asymmetry index of OEF, suggesting that the vasodilatory capacity is more closely related to the asymmetry in OEF than to an absolute increase in OEF. The ACZ test with measurement of rCBF and V0 may be able to detect vasodilatory capacity, and it might be dependent on the relative redistribution of arterial perfusion pressure caused by regional differences in vasodilatory capacity. The dissociation of changes in rCBF and V0 after ACZ administration in the ipsilateral hemisphere of group A indicates that the perfusion pressure decreased relatively in the ipsilateral compared with the contralateral hemisphere. This finding was presumably caused by deficient collateral circulation in group A, which may have caused the difference in clinical histories between the 2 patient groups. Compared with the patients in group B, the patients in group A tended to have a history of TIA. These differences in the results of the ACZ test do not necessarily represent absolute changes in hemodynamic parameters that indicate oxygen metabolism or the critical condition of viable cortices in the hypoperfused regions, suggesting that the ACZ test and OEF values reflect different aspects of hemodynamic impairment. Several studies have demonstrated that the cerebrovascular reactivity (CBF response) to vasodilatory stimuli is related to the long-term prognosis of patients with cerebrovascular disease (7,25,26), although Yokota et al. (27) reported that a reduced vasodilatory capacity did not predict recurrence of stroke. Further investigation will be needed to determine whether a reduced CBF response to vasodilatory stimuli can detect indications for surgical treatment and is a reliable index with which to estimate prognosis. Analysis of both rCBF and V0 obtained from the bolus method using H215O PET along with the ACZ test will provide further hemodynamic information on the brain of patients with varied cerebral circulation.
CONCLUSION
The current study demonstrates that the vasodilatory reaction in cerebral arteries induced by ACZ was not necessarily coupled with rCBF changes in patients with unilateral cerebral arterial occlusive disease, because the decrease in rCBF was accompanied by an increase in V0 in the region with the steal phenomenon. The remarkable contrast in CBF images after the ACZ injection, which may be dependent on the relative rather than the absolute vasodilative response, tended to overestimate the reduction in vasodilatory capacity. The percentage change in rCBF correlated only with the asymmetry in OEF, not with an increase in OEF. The discrepancy between the ACZ test and other hemodynamic parameters may be explained by the differences between the changes in rCBF and V0 caused by ACZ. The measurement of V0 coupled with the ACZ test would provide additional data for an evaluation of vasodilatory capacity and cerebral hemodynamics.
Acknowledgments
The authors thank Yoshihiko Kishibe, Hidekazu Matsugi, and other staff members of the PET Unit in the Research Institute for clinical and technical support. The authors also thank the staff of the Departments of Neurology and Neurosurgery, Shiga Medical Center, for clinical assistance. This study was supported in part by Grant-in-Aid 14207039 for Scientific Research from the Japan Society for the Promotion of Science.
Footnotes
Received Dec. 16, 2002; revision accepted May 1, 2003.
For correspondence or reprints contact: Hidehiko Okazawa, MD, PhD, Biomedical Imaging Research Center, Fukui Medical University, 23-3 Shimoaizuki, Matsuoka, Fukui, 910-1193, Japan.
E-mail: okazawa{at}fmsrsa.fukui-med.ac.jp
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- The Acetazolamide Challenge: Techniques and Applications in the Evaluation of Chronic Cerebral Ischemia
- Combination of a Mean Transit Time Measurement with an Acetazolamide Test Increases Predictive Power to Identify Elevated Oxygen Extraction Fraction in Occlusive Carotid Artery Diseases
- Mapping Cerebrovascular Reactivity Using Blood Oxygen Level-Dependent MRI in Patients With Arterial Steno-occlusive Disease: Comparison With Arterial Spin Labeling MRI
- Reduced Blood Flow and Preserved Vasoreactivity Characterize Oxygen Hypometabolism Due to Incomplete Infarction in Occlusive Carotid Artery Diseases