


Abstract
We investigated the value of supranormal function and renogram patterns on 99mTc-mercaptoacetyltriglycine (99mTc-MAG3) scintigraphy in relation to the extent of hydronephrosis for predicting ureteropelvic junction (UPJ) obstruction in the newborn. Methods: We studied 48 patients with prenatally diagnosed unilateral hydronephrosis that was confirmed on postnatal ultrasonography. The anteroposterior pelvic diameter (APPD) and the Society for Fetal Urology (SFU) grade were measured on 1-mo ultrasonography to assess the extent of hydronephrosis. Neonates with an APPD of ≤10 mm or a differential renal function of ≤40% were excluded. Supranormal function (≥55%) and renogram grades (1, not obstructive; 2, indeterminate; 3, obstructive; and 4, prolonged parenchymal transit) were determined on 1-mo 99mTc-MAG3 renography. Multivariate logistic regression analysis was performed to predict the presence of obstruction. Results: Of the 48 kidneys with hydronephrosis, 19 were diagnosed as having UPJ obstruction. Twenty-nine kidneys were classified as having nonobstructive hydronephrosis. The APPD of the 19 kidneys with obstruction (24.3 ± 9.2 mm) was significantly larger than that of the 29 kidneys without obstruction (17.5 ± 11.2 mm; P < 0.05). The SFU grades of UPJ obstruction (2 with grade 3, 17 with grade 4) were also significantly higher than those without UPJ obstruction (grades 1–4 in 1, 6, 10, and 12 kidneys, respectively; P < 0.01). Supranormal function was present in 4 kidneys with UPJ obstruction but in none without obstruction (P < 0.001). 99mTc-MAG3 renography of the 19 obstructions showed grades 2, 3, and 4 renograms in 4, 8, and 7 patients, respectively. The 29 without obstruction revealed significantly lower grades (grades 1–4 in 10, 13, 5, and 1 patient, respectively; P < 0.001). Multivariate logistic regression analysis revealed that the addition of supranormal function or renogram grade in the model significantly increased the likelihood ratio in comparison with that of the SFU grade only (χ2 = 7.73 and 9.99, respectively; P < 0.01). Of the 29 neonates with SFU grade 4, supranormal function or renogram ≥ grade 4 had a positive predictive value of 90% (9/10). Conclusion: 99mTc-MAG3 renography at 1 mo after birth has a significant additive value in relation to the degree of hydronephrosis in predicting UPJ obstruction in patients with prenatally diagnosed unilateral hydronephrosis with normal function.
- 99mTc-mercaptoacetyltriglycine renography
- ureteropelvic junction obstruction
- neonates
- supranormal function
The management of ureteropelvic junction (UPJ) obstruction in infants is difficult because the diagnosis of a significant obstruction cannot always be established with certainty without a waiting period for the development of measurable progressive renal injury (1,2). There are 2 different approaches to the management of neonatal hydronephrosis with preserved renal function. Proponents of the noninvasive approach advocate that neonatal hydronephrosis is a benign disease and that serial measurement of renal function and pelvic size will permit a conclusive diagnosis of obstruction with minimal delay (2–4). Some centers, however, prefer to operate before there is loss of function, even at the risk of operating on a few infants who might have remained stable. The proponents of this approach claim that the earlier surgery will result in improving renal function of obstructive kidneys (5,6) and that repetitive imaging studies may be more invasive than pyeloplasty (7).
Ultrasonography provides essential information regarding renal thickness and degree of dilatation of the pelvocalyceal system. The degree of hydronephrosis—either the anteroposterior pelvic diameter (APPD) or the Society for Fetal Urology (SFU) grading system—is related to the presence of obstruction (2–4,8–11). Similarly, the renogram pattern is related to the degree of obstruction (12). However, studies on the natural history of neonatal hydronephrosis have shown conflicting results of the value of diuretic renography in the selection of hydronephrotic kidneys that would benefit from pyeloplasty (2–4,8,13–16). These conflicting reports are probably due to the functionally immature kidneys of neonates, use of 99mTc-diethylenetriaminepentaacetic acid, and no bladder catheterization (17,18). Another parameter of renography is the supranormal function of the hydronephrotic kidney. Varied with definitions of supranormal function, 9%–22% of all congenital unilateral hydronephrosis have supranormal function (19,20). Although the management of hydronephrosis with supranormal function has not been clearly established to date (21–23), a recent study has shown that supranormal function is real and may be related to obstructive hydronephrosis (24).
Because ultrasonography is usually the first study to be performed, for radionuclide renography to be useful for diagnosing UPJ obstruction it needs to provide additional information. In previous studies that have demonstrated the usefulness of 99mTc-mercaptoacetyltriglycine (99mTc-MAG3) diuretic renography in evaluating hydronephrosis during the neonatal period (13–16), the value of 99mTc-MAG3 renography in relation to the degree of hydronephrosis was not confirmed. We presumed that a combination of noninvasive predictors would provide a better means of identifying UPJ obstruction and may guide surgical decision making without an observation period or close monitoring of neonates at higher risk for renal deterioration. We performed a prospective study to investigate the value of 99mTc-MAG3 renography in relation to the degree of hydronephrosis measured by 1-mo ultrasonography in patients with prenatally diagnosed hydronephrosis with preserved renal function.
MATERIALS AND METHODS
Between April 1996 and June 2000, we prospectively studied neonates with prenatal hydronephrosis ≥5 mm (APPD) that was confirmed by postnatal ultrasonography 2 d after birth. The neonates underwent ultrasonography and 99mTc-MAG3 diuretic renography at 1 mo after birth. Inclusion criteria for the study were unilateral hydronephrosis of an APPD ≥10 mm on 1-mo ultrasonography and preserved differential renal function (≥40%) of the hydronephrotic kidney on 99mTc-MAG3 renography. Neonates with hydroureter, vesicoureteral reflux, or other congenital anomalies were excluded.
Follow-up renal ultrasonography and 99mTc-MAG3 diuretic renography were performed at 3, 6, and 12 mo after birth. Pyeloplasty was indicated if the initial studies revealed an APPD of ≥30 mm with prolonged clearance half-time (t1/2) on a diuretic scan (>20 min). Pyeloplasty was also performed when a urinary infection developed, renal function deteriorated (≥10%) on follow-up 99mTc-MAG3, or the extent of hydronephrosis increased on follow-up ultrasonography.
Sixty-three neonates with hydronephrosis were enrolled. Of these, 15 patients who did not adhere to the follow-up protocol were excluded. Finally, 48 neonates (41 boys, 7 girls) with unilateral hydronephrosis were evaluated (Table 1). The date of the initial 99mTc-MAG3 diuretic scans ranged from 3 to 82 d after birth (mean, 39.1 ± 15.2 d).
Baseline Clinical, Ultrasonographic, and 99mTc-MAG3 Diuretic Renographic Results in Patients with Unilateral Hydronephrosis and Normal Differential Renal Function
The APPD and the SFU grades were determined on 1-mo ultrasonography to assess the extent of hydronephrosis (10). Initially, the APPD of the hydronephrotic kidney was measured by practicing radiologists. Later, 2 experienced radiologists, who were unaware of the clinical data, determined the grade of the SFU system and confirmed the APPD data. Any discrepancies in the SFU grades were resolved by consensus. The weighted κ-value for grading the SFU system was 0.63.
99mTc-MAG3 diuretic renography was performed following the standardized protocol (25). Bladder catheterization was not performed. Before the injection of 99mTc-MAG3, patients were hydrated intravenously at a rate of 10 mL/kg of normal saline over 30 min. We administered 3.7 MBq/kg 99mTc-MAG3 (minimum dose, 37 MBq) intravenously. One experienced technologist calculated differential renal functions and generated renograms. For the measurement of differential renal function, regions of interest were drawn over the entire kidney and background on each side. The kidney background was manually drawn on 1- to 2-min images in a crescent shape over the outer aspect of the kidney to exclude the collecting systems. The perirenal background region of interest was 2 pixels wide and 1 pixel outside the kidney. Differential renal function was calculated as the percentage of relative activity of the hydronephrotic kidney over the sum of background-corrected total renal activity at 1–2 min after injection. Supranormal function of the hydronephrotic kidney was defined as a differential renal function of ≥55%. Intraobserver variability for differential renal function was 0.8% ± 0.6%.
For the diuretic renogram, furosemide (1 mg/kg) was injected 20 min after the injection of a radiopharmaceutical. The diuretic t1/2 was defined as the time when the half of the activity was washed out of the collecting system after injection of furosemide. The basal and diuretic renograms were categorized according to the well-tempered diuretic renogram (14,15). 99mTc-MAG3 diuretic renograms obtained at about 1 mo were graded as follows: grade 0 = normal renogram; grade 1 = obstructive basal and nonobstructive diuretic renogram; grade 2 = obstructive basal and indeterminate diuretic renogram; grade 3 = both obstructive renograms; and grade 4 = both obstructive renograms with delayed parenchymal transit time. An indeterminate renogram indicated a delayed t1/2 of >15 min with some activity excretion. The radiotracer appearance time on the collecting system was measured visually in both hydronephrotic and contralateral normal kidneys. Delayed parenchymal transit time was considered to be present when there was prolonged retention of activity in the renal parenchyma and >10 min of delayed pelvocalyceal appearance time compared with that of a normal contralateral kidney.
The final diagnosis of UPJ obstruction was made using the following criteria: (a) further impairment of renal function (>10%) or hydronephrosis on follow-up 99mTc-MAG3 or ultrasonography or (b) improved postoperative drainage (t1/2 < 15 min) and hydronephrosis (or both criteria). Diagnosis of nonobstructive hydronephrosis was made when there was no change in differential renal function and t1/2 on follow-up 99mTc-MAG3 diuretic renography and stationary or improved hydronephrosis on ultrasonography at 12 mo. In patients with presumed nonobstructive hydronephrosis, clinical or ultrasonographic follow-up was performed for at least 1 y.
Numeric data are expressed as mean ± SD if not specified. Correlation between variables was assessed by the Spearman rank correlation coefficient. The variables used to examine an association with UPJ obstruction were sex, site of obstruction, degree of hydronephrosis (APPD or SFU grade), supranormal differential function, and grades of the diuretic renogram. The Fisher exact test or Kolmogrov-Smirnov test was used for categoric variables and the Student t test was used for continuous variables. Enhanced prediction of UPJ obstruction with the combined use of 99mTc-MAG3 renography and ultrasonographic variables compared with that of the degree of hydronephrosis only was assessed by multivariate logistic regression analysis.
RESULTS
Diagnosis of UPJ Obstruction
Baseline clinical, ultrasonographic, and 99mTc-MAG3 diuretic renographic results are summarized in Table 1. Of the 48 kidneys with hydronephrosis, 19 were diagnosed as having UPJ obstruction and the patients underwent pyeloplasty. Four patients needed pyeloplasty because of urinary tract infection and were diagnosed as having UPJ obstruction based on increasing extent of hydronephrosis (n = 2) or improved hydronephrosis and drainage after pyeloplasty (n = 2). Eleven patients underwent pyeloplasty because of worsening hydronephrosis. Among these, 2 neonates showed increasing extent of hydronephrosis and worsened differential renal function (>30%). Unfortunately, their differential renal function did not return to normal values after pyeloplasty. These patients had a grade 4 renogram on the initial 1-mo 99mTc-MAG3 renogram. The other 9 neonates who underwent pyeloplasty because of worsening hydronephrosis had improved hydronephrosis and drainage postoperatively. The remaining 4 patients underwent pyeloplasty because of severe hydronephrosis (APPD > 30 mm) with obstructive renogram, and all showed postoperative improvement of hydronephrosis and drainage on follow-up ultrasonography and 99mTc-MAG3 renography, which made the diagnosis of UPJ obstruction.
Twenty-nine kidneys were classified as having nonobstructive hydronephrosis. Of the 29 without UPJ obstruction, 8 had complete resolution of hydronephrosis. Fourteen kidneys showed reduction in the extent of hydronephrosis. The remaining 7 continued to remain stable in terms of renal function and the degree of hydronephrosis on follow-up ultrasonography and 99mTc-MAG3 diuretic renography.
Prediction of UPJ Obstruction: Univariate Analysis
Results of univariate analysis of the variables that predict UPJ obstruction are summarized in Table 2. Sex or the side of the hydronephrotic kidney was not associated with UPJ obstruction.
Univariate Analysis of Variables that Predict UPJ Obstruction in Neonates with Unilateral Hydronephrosis
The extent of hydronephrosis assessed by ultrasonography (APPD or SFU grade) was significantly higher in neonates with UPJ obstruction (Table 2). In the UPJ obstruction group (n = 19), all kidneys showed SFU grade 3 (n = 2) or grade 4 (n = 17). The SFU grades of neonates with nonobstructive hydronephrosis ranged from grade 1 to grade 4. However, all neonates with SFU grade 1 or grade 2 had nonobstructive hydronephrosis. When SFU grade 4 was considered to be suggestive of UPJ obstruction, the diagnostic sensitivity and specificity of ultrasonography were 89% (17/19) and 59% (17/29), respectively.
There was no significant difference in differential renal function between neonates with obstructive and nonobstructive hydronephrosis (Table 2). Supranormal function was present in 4 kidneys (1 right and 3 left: 56%, 57%, 61%, and 62%) with obstructive hydronephrosis, whereas there were no supranormal kidneys with nonobstructive hydronephrosis (P < 0.001). Renogram grades were also associated with UPJ obstruction (P < 0.001; Table 2), although patterns of renogram grades overlapped between the 2 groups. All neonates with a renogram with grade 1 (n = 10) had nonobstructive hydronephrosis, whereas 7 of 8 neonates with grade 4 had UPJ obstruction (Fig. 1). With a cutoff value of grade 3 or higher for diagnosing UPJ obstruction, the diagnostic sensitivity of 99mTc-MAG3 renography was 79% (15/19) and specificity was 79% (23/29).

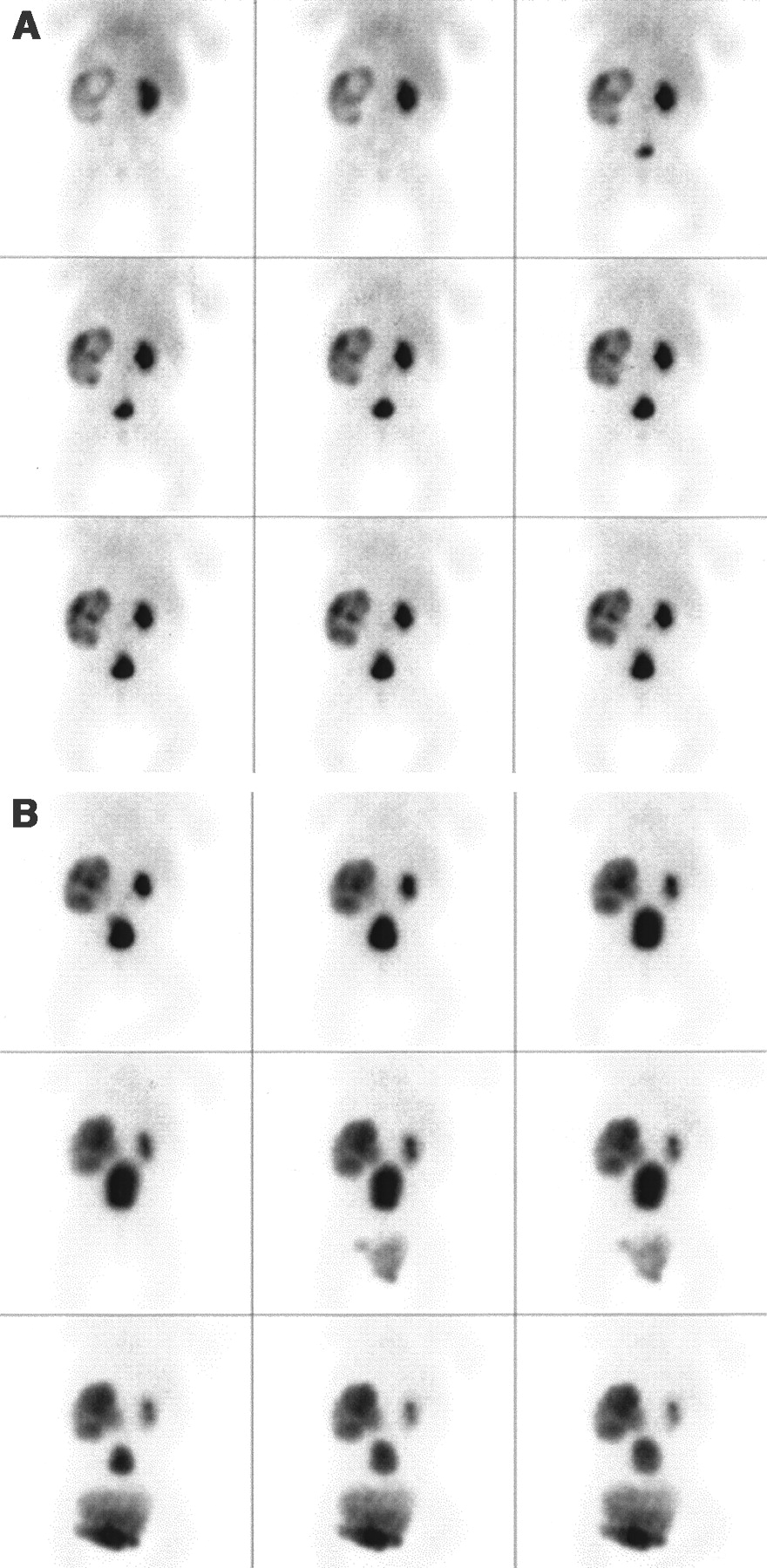
Posterior 2-min-interval images of 99mTc-MAG3 scan are displayed. (A) Basal renal scan (38 d after birth) of boy with SFU grade 4 hydronephrosis of left kidney demonstrates evidence of delayed parenchymal transit (persistent renal parenchymal activity and delayed appearance of pelvocalyceal radiotracer). Differential renal function of left kidney was 43%. (B) Diuretic scan shows deterioration of clearance from left renal pelvis (t1/2 > 20 min). Postoperatively, improved hydronephrosis and drainage (t1/2 = 8 min) were observed on ultrasonography and diuretic 99mTc-MAG3 scan at 6 mo.
The renogram grade was positively correlated with the SFU grade (ρ = 0.583; P < 0.001) or the APPD (ρ = 0.443; P < 0.001). There was no significant correlation between the other variables.
The radiotracer appearance time in the renal pelvis ranged from 5 to >20 min after injection of 99mTc-MAG3 in kidneys with UPJ obstruction and from 2 to 14 min in kidneys without UPJ obstruction. The time difference between hydronephrotic and nonhydronephrotic contralateral kidneys ranged from 0 to 6 min in nonobstructive hydronephrosis or UPJ obstruction without delayed parenchymal transit. All patients with delayed parenchymal transit showed a >12-min time difference.
Prediction of UPJ Obstruction by Ultrasonograhy and 99mTc-MAG3 Scintigraphy: Multivariate Analysis
Simple logistic regression analysis revealed that the APPD and the SFU grade were significant predictors of UPJ obstruction (Table 3). On multivariate logistic regression analysis, addition of supranormal function and renogram grade in the model significantly increased the likelihood ratio in comparison with that of the SFU grade only (Table 3). The χ2 value of all 3 variables in the model was also significantly higher than that of the SFU grade with supranormal function in the model (χ2 = 14.352 − 7.728 = 6.624 with 1 degree of freedom; P < 0.01) or that of the SFU grade with renogram grade (χ2 = 14.352 − 9.989 = 4.363 with 1 degree of freedom; P < 0.05).
Multivariate Logistic Regression Analysis Showing Increased Likelihood Ratio for Prediction of UPJ Obstruction by Addition of 99mTc-MAG3 Variables
A summary of the SFU grade, function of ≥55%, and 99mTc-MAG3 renogram findings in relation to the presence of UPJ obstruction in neonates with unilateral hydronephrosis and normal function is shown in Table 4. All neonates with either SFU grade 1 or grade 2 or renogram grade 1 had nonobstructive hydronephrosis. In neonates with SFU grade 3 or grade 4, the renogram grade or the presence of supranormal function contributed significantly in the differentiation of UPJ obstruction from nonobstructive hydronephrosis. Of the 29 neonates with SFU grade 4, supranormal function or renogram grade 4 or higher had a positive predictive value of 90% (9/10; Table 4).
Summary of SFU Grade, Supranormal Function, and 99mTc-MAG3 Renogram Findings in Neonates with Unilateral Hydronephrosis
DISCUSSION
This study demonstrates that 99mTc-MAG3 renography at 1 mo after birth has significant additive diagnostic value in relation to the degree of hydronephrosis measured by 1-mo ultrasonography in patients with prenatally diagnosed hydronephrosis with preserved renal function. Renogram grades and supranormal function were helpful in identifying obstructive hydronephrosis in neonates with a high degree of hydronephrosis. Combined ultrasonographic and renographic information may guide correct surgical decision making without an observation period or close monitoring of neonates at higher risk for renal functional deterioration or aggravation of hydronephrosis.
In this study, the APPD and the SFU grading system were correlated with the final diagnosis of obstruction. The more significant correlation of the SFU grades than the APPD may be related to the importance of calyceal dilatation as a manifestation of significant obstruction (10,26). In this study, all neonates with SFU grade 1 or grade 2 had nonobstructive hydronephrosis, confirming the value of SFU grading. However, in neonates with SFU grade 3 or grade 4, renogram findings were helpful in predicting UPJ obstruction.
Supranormal function was shown to be useful in predicting UPJ obstruction in this study. Many factors, including background subtraction methods and the reservoir effect of hydronephrosis, affect measurement of differential renal function (19,23,24). To avoid potential overestimation, we adopted perirenal background correction (24,27), measuring differential function at 1–2 min after injection (13,24), and a more stringent criterion of ≥55% (21,24). We had only 4 kidneys (4/19; 21% of obstructive hydronephrosis) with supranormal function. However, the presence of supranormal function identified a subgroup of neonates at higher risk of developing UPJ obstruction.
There were no obstructive kidneys with a grade 1 renogram. Close observation may not be necessary in this group. However, it has been reported that some patients with initial nonobstructive hydronephrosis later developed obstruction (8,16,28–30). A longer follow-up period of >1 y may be required to exclude the possibility of future progression to obstructive hydronephrosis.
All patients with UPJ obstruction had inadequate drainage of grades 2–4. The percentage of UPJ obstruction increased with increasing grade of renogram drainage. The results of this study confirm the results of an earlier study that reported the shape of the washout curve on the first postnatal nuclear scan was informative for predicting outcome, such that cases with an initial obstructive pattern were less likely to normalize (31). In the earlier study, however, patients with poor renal function were included, and the value of nuclear renography in relation to ultrasonography for predicting UPJ obstruction was not demonstrated (31).
False-positive results of obstructive 99mTc-MAG3 renograms in our study again confirm that an obstructive diuretic renogram on a 99mTc-MAG3 diuretic scan in the neonatal period does not always indicate the presence of UPJ obstruction, as was shown in previous studies using 99mTc-diethylenetriaminepentaacetic acid diuretic scintigraphy (2,4,8). Immature renal function or lack of bladder catheterization may explain a false-positive result. Interpretation of an obstructive diuretic renogram requires careful considerations of technical aspects of diuretic renography and the anatomic status of hydronephrosis before making the clinical decision of early surgery or close follow-up evaluation.
It is noteworthy that 8 kidneys showed delayed parenchymal transit in this study. UPJ obstruction was confirmed in 7 patients. Delayed parenchymal transit is a well-known indicator of obstruction (32,33). Parenchymal transit and the appearance of tracer in the collecting system are relatively proportional to the severity of the obstruction (12). Although we did not measure parenchymal transit time by deconvolutional analysis, the simple approach to estimate transit time is to evaluate the appearance time of activity in the renal pelvis or prolonged retention of activity in the parenchyma (34). The definition of delayed appearance time in the renal pelvis was based on the time difference in patients without UPJ obstruction. On the basis of our results, it appears that a scintigraphic finding of delayed parenchymal transit is a specific finding of UPJ obstruction. Two patients with delayed parenchymal transit on the initial 99mTc-MAG3 renography underwent pyeloplasty because of aggravated renal function and hydronephrosis without postoperative improvement of differential renal function. Postoperative functional improvement remains a subject of debate (2–4,18,30,35,36). However, our results correspond with those of other investigators (18,30,36), suggesting that it is important to establish the diagnosis of UPJ obstruction in the neonatal period before the deterioration of renal function. The presence of delayed parenchymal transit in patients with UPJ obstruction may indicate that there is a subgroup of patients who need early pyeloplasty without an observation period to prevent functional loss. Neonatal kidneys with delayed parenchymal transit on 99mTc-MAG3 renography need closer follow-up study or early surgery.
In this study, 19 of the 48 kidneys (40%) with unilateral hydronephrosis (APPD ≥ 10 mm) had pyeloplasty. Several reports have indicated that most newborns (>80%) with preserved differential function did not require surgery (2–4,9). The higher number of hydronephrosis requiring pyeloplasty in our study may be attributed to the exclusion of mild hydronephrosis of an APPD ≤10 mm. In contrast, a recent randomized control study evaluating surgery versus observation in unilateral hydronephrosis with preserved function and obstructive renogram concluded that children younger than 6 mo old with unilateral hydronephrosis with good function and obstructive renogram are better served by pyeloplasty than observation (26). The difference in study designs, follow-up periods, and patient population likely contributed to the different numbers of patients with obstruction between studies. In our study, the natural history of 4 patients who underwent pyeloplasty because of severe hydronephrosis with obstructive renogram was not observed. However, the diagnosis of UPJ obstruction was established by postoperative improvement of hydronephrosis and drainage.
This study has some limitations. 99mTc-MAG3 diuretic renography was performed without bladder catheterization or postgravity-assisted drainage (16). We might have had better results using those techniques. Second, a follow-up period of 1 y may not be long enough to assess the final diagnosis and outcome. Finally, the number of study patients may be small for multivariate analysis. In particular, we studied only 4 neonates with supranormal function. However, we obtained statistically significant results in respect to the additive value of 99mTc-MAG3 renography.
CONCLUSION
Supranormal function and obstructive renogram on 99mTc-MAG3 renography are valuable parameters in relation to the degree of hydronephrosis for the prediction of UPJ obstruction in patients with prenatally diagnosed unilateral hydronephrosis and preserved renal function. Ultrasonographic and renographic information may guide correct surgical decision making without an observation period or close monitoring of neonates at higher risk for deterioration. Combined information may also obviate the need for repeated imaging studies in neonates with low risk of developing UPJ obstruction.
Footnotes
Received Jul. 22, 2002; revision accepted Nov. 27, 2002.
For correspondence or reprints contact: Dae Hyuk Moon, MD, Department of Nuclear Medicine, Asan Medical Center, University of Ulsan College of Medicine, 388-1 Pungnap-2dong, Songpa-gu, Seoul 138-736, Korea.
E-mail: dhmoon{at}amc.seoul.kr
REFERENCES
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.