


Abstract
(E)-N-(3-iodoprop-2-enyl)-2β-carbomethoxy-3β-(4′-methyl-phenyl) nortropane (PE2I), a cocaine analog, is a new, highly specific tracer for imaging dopamine transporter labeled with 123I for in vivo SPECT. Its reversible binding on dopamine transporter and its rapid kinetics allow quantification of its binding potential according to a 3-compartment model. For quantification of distribution volume of reversible tracer, Logan developed a noninvasive and graphical method that allows accurate estimation of binding potential. In this study, we performed 123I-PE2I SPECT on healthy volunteers and patients with Parkinson’s disease (PD) to validate the Logan graphical method for quantification of 123I-PE2I binding and to analyze the relationship between 123I-PE2I SPECT and clinical features of this frequent degenerative disease. Methods: Eight PD patients (3 women, 5 men; mean age, 64 ± 7.9 y; disease duration range, 1–8 y, Hoehn and Yahr stage range, 1–2.5) and 8 age-matched healthy volunteers (4 women, 4 men; mean age, 61.5 ± 9.5 y) were included in 2 centers and studied with SPECT. Four sequential SPECT imaging sessions of 15-min duration were performed from 5 to 65 min after bolus injection of 140 ± 30 MBq of 123I-PE2I. Results: The kinetics of PE2I in healthy volunteers and PD patients were rapid, and the Logan graphical method allowed quantification of distribution volume ratio (DVR) in the caudate nucleus and putamen. 123I-PE2I striatal specific binding was significantly reduced in PD patients, compared with healthy volunteers, in the caudate and putamen. The decrease of DVR in the putamen was significantly and inversely correlated to disease duration and Hoehn and Yahr stage. In asymmetric PD patients, 123I-PE2I uptake was significantly more reduced in the putamen contralateral to the side with predominant clinical symptoms. However, 123I-PE2I uptake was also significantly reduced in the ipsilateral putamen, compared with that in healthy volunteers, suggesting that 123I-PE2I SPECT can detect nigrostriatal degeneration before the appearance of clinical symptoms. Conclusion: Our data indicate that the Logan graphical method is accurate for noninvasive quantification of PE2I and that 123I-PE2I SPECT is a useful quantitative method for accurate estimation of nigrostriatal dopaminergic nerve terminal degeneration. The close relationships between SPECT findings and clinical data suggest that this method is useful for objectively following the progression of PD and for assessing the effect of potential neuroprotective treatments. Finally, our findings suggest that 123I-PE2I SPECT can be used for preclinical and early diagnosis of PD.
Parkinson’s disease (PD) is a progressive disabling neurodegenerative disorder observed in 1% of the population older than 55 y, the mean age at which the disease is first diagnosed (1). PD consists of a syndrome including tremor, rigidity, bradykinesia, and postural abnormalities. The 2 principal anatomopathologic characteristics of PD are the progressive loss of pigmented melanistic neurons of mesencephalon, particularly loss of dopaminergic neurons in the substantia nigra pars compacta (2), and a ventrocaudal gradient of degenerative lesion (3). In the past 2 decades, the strategy of symptomatic treatments has been improved and deep stimulation surgery has become an effective alternative for motor fluctuations and dyskinesia due to medical treatment (4). The issue for our new century will be the development of neuroprotective therapeutics aimed at slowing or stopping the degenerative process. This aim stresses the need for very early diagnosis of PD (5,6).
In recent years, PET and SPECT exploration of the dopamine system using specific ligands has evolved, thus showing the usefulness of pre- and postsynaptic transporters or receptors as objective markers of the integrity of this system (7,8). SPECT is widely available and offers an in vivo noninvasive diagnostic method to detect nigrostriatal nerve terminal lesions with specific ligands of the dopamine transporter (DAT) (9–11). A new high-affinity and selective ligand for imaging the DAT has recently been developed: (E)-N-(3-iodoprop-2-enyl)-2β-carbomethoxy-3β-(4′-methylphenyl) nortropane (PE2I) (12). In vitro studies have demonstrated that 125I-PE2I has high affinity for DAT (dissociation constant [Kd] = 4 nmol/L) and very high selectivity for DAT versus serotonin (5HT) and noradrenaline transporters (12,13). PE2I has been labeled with 123I and 11C for in vivo SPECT and PET studies, which have shown a reversible and specific in vivo binding to the DAT (14,15). According to a 3-compartment model, 2 methods have been proposed to quantify in vivo binding of reversible tracer, that is, the specific (striatum)-to-nonspecific (occipital lobe or cerebellum) uptake ratio at pseudoequilibrium to determine binding potential (16), and the Logan graphical method to obtain distribution volume ratio (DVR) (17). Initially, quantification of PE2I was proposed using measurement of the striatum-to-cerebellum ratio (18), but Logan analysis was recently shown to be a more accurate method for quantification of striatal 123I-PE2I binding because of the rapid kinetics of the tracer (19). Pinborg et al. (19) demonstrated that, compared with compartment kinetics analysis, the Logan graphical method was accurate for quantification of PE2I.
The aim of this study was therefore to demonstrate that quantification of 123I-PE2I DVR with the Logan graphical method without blood sampling allowed early diagnosis and follow-up of PD.
MATERIALS AND METHODS
Patients
Eight patients with idiopathic PD (3 women, 5 men; mean age, 64 ± 7.9 y) and 8 healthy volunteers (4 women, 4 men; mean age, 61.5 ± 9.5 y) were recruited at, respectively, the Department of Neurology, Bretonneau Hospital, Tours, France, and the Clinic Investigation Center, Purpan Hospital, Toulouse, France. The study was performed according to the standard ethical guidelines of the Hospital and University of Tours and was approved by the local ethical committee on April 27, 1998. All patients and healthy volunteers gave informed and written consent.
Seven of 8 patients had asymmetric disease and 1 had bilateral symmetric disease, all with bradykinesia and at least 1 of the other cardinal features of the disease: rigidity, rest tremor, or impaired postural reflexes. The diagnosis of PD was assessed according to the United Kingdom Parkinson’s Disease Society Brain Bank criteria (20). None of the 8 patients had features suggestive of atypical parkinsonism or responded to the Quinn criteria for multiple-system atrophy (21) or the criteria for progressive supranuclear palsy of the National Institute of Neurological Disorders and Stroke and the Society for Progressive Supranuclear Palsy (22). No patient had relevant abnormalities on brain MRI or CT. No patient had mental deterioration or depression according to the criteria in the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (23) or according to the Mini-Mental State score (>25) (24). The clinical handicap state was determined by the modified version of the Hoehn and Yahr scale (1). Patients were asked to stop dopaminergic treatment 8 d before the SPECT scan if they were taking anticholinergic molecules and dopamine agonists or 12 h before the SPECT scan if they were taking l-dopa. The 8 healthy volunteers had no relevant medical history, no hypertension, no diabetes, no cardiac disorders, and no history of cranial trauma or serious infectious disease. They were not receiving any medication. No healthy volunteer had relevant abnormalities found on brain MRI. They were recruited in the same age range as the parkinsonian patients. The characteristics of the 2 groups are presented in Table 1.
Clinical Characteristics of Subjects at Time of 123I-PE2I SPECT
Radioiodine uptake by the thyroid gland was prevented by oral ingestion of 400 mg of potassium perchlorate 15 min before intravenous injection of ligand. A catheter was inserted into an antebrachial vein, and an isotonic glucose solution was infused. A bolus of 140 ± 30 MBq 123I-PE2I was injected through the catheter.
Preparation of PE2I
123I-PE2I was prepared by iododestannylation of the tributyl tin precursor. To a vial containing 50 μg of the stannic precursor were added 50 μL of EtOH, 50 μL of HCl (0.1N), 740 MBq of 123I-NaI (in 100 μL of NaOH, 0.1N, with a specific activity > 185 TBq/mmol; Cis Bio International), and 50 μL of 10 mg/mL chloramine T. The reaction was allowed to stand at room temperature for 30 min, quenched with 100 μL of Na2S2O5 (300 mg/mL), basified with saturated NaHCO3, and extracted with ethyl acetate (3 × 1 mL). The combined ethyl acetate extracts were evaporated under a nitrogen stream, and the residue was dissolved in 200 μL of the high-performance liquid chromatography (HPLC) mobile phase. The radioiodinated solution was purified by HPLC using a reverse-phase C-18 column and a mixture of MeOH:H2O:Et3N (80:20:0.1) as the mobile phase (flow rate, 1 mL/min). The fraction eluted at the retention time of PE2I was collected and passed through a Sep-Pak C-18 column (Waters). The radioiodinated product was then eluted with 2 × 1 mL of EtOH and evaporated under a nitrogen stream. Structural identification and radiochemical purity were checked by HPLC using cold PE2I as a reference under the same conditions.
SPECT Protocol
SPECT data acquisition started 5 min after the intravenous injection. A double-head camera equipped with parallel collimators (Cardial Elscint; General Electric Medical Systems) was used for healthy volunteers, and a multislice brain-dedicated camera (Ceraspect; Digital Scintigraphics) was used for PD patients. Resolution was 8–9 mm and 7–8 mm in full width at half maximum for, respectively, the double-head and brain-dedicated cameras. In the healthy volunteers, four 15-min sequential acquisitions were obtained, followed by two 15-min acquisitions at 180 and 200 min after injection. In the patients, 4 sequential 15-min acquisitions using a 120 × 3° step rotation were obtained. Images were reconstructed from photopeak counts (159 ± 16 keV) using a filtered backprojection algorithm with a Butterworth filter (cutoff, 0.754 cm; order, 4; size, 7) for the double-head camera and a 2-dimensional Hanning filter (order, 0.5) for the Ceraspect camera. Images were displayed as a 128 × 128 matrix (pixel size, 1.67 mm2). SPECT data were reoriented according to a line passing through the inferior part of the frontal and occipital lobes parallel to the anterior–posterior commissure. We made no correction for the partial-volume effect or attenuation resulting in systematic errors; these were assumed to have a similar effect on data from both cameras. Cross calibration of the 2 cameras with phantoms showed that the use of 2 different cameras did not significantly affect the counting ratio measurement between the striatum and occipital regions. The 5 slices corresponding to the highest striatal uptake were digitally summed, yielding a final transverse slice 8.5 mm thick. Geometric standardized circular (caudate nucleus and occipital lobe) or elliptic (putamen) regions of interest (ROIs) were drawn on the striatum (S, specific binding) and the occipital cortex (O, free and nonspecific binding). The sizes of the ROIs were 74 mm2 for the caudate nucleus (C), 140 mm2 for the putamen (P), and 314 mm2 for the occipital region. The mean activity was counted in the 6 different ROIs in counts per second per pixel; that is, C(T), P(T), S(T), and O(T), where T is time T.
Graphical Analysis
Average regional counts were used in calculations. Time-activity curves for each ROI were determined from 5 to 65 min after injection and were corrected for radioactivity decay of 123I. Time-activity data were analyzed by the noninvasive linear graphical method developed by Logan et al. (17) for reversible ligands. This method assumed that the distribution volume of nondisplaceable tracer is the same in reference (occipital lobes) and striatal regions and that delivery of the tracer is similar for both regions. The integrated striatal ROI activity from time zero to T normalized to striatal activity at time T ([int (0–T) S(t)dt]/S(T)) was plotted against integrated occipital ROI activity from zero to T also normalized to striatal activity at time T ([int (0–T) O(t)dt]/S(T)).
 with
with
 where Str = striatum, Occ = occipital lobe, and ct = constant.
where Str = striatum, Occ = occipital lobe, and ct = constant.
The Logan plot becomes linear when pseudoequilibrium is reached, that is, when the ratio Occ(T)/Str(T) becomes constant. The asymptotic slope equals DVR. DVR is defined as the ratio between distribution volume of specific binding of 123I-PE2I to DAT (striatum) and distribution volume of nonspecific binding of the ligand in regions devoid of DAT (occipital lobes). DVR is related to the binding potential (DVR = binding potential − 1) (17), and binding potential is assimilated to the density of DAT (16). In a previous study with SPECT PE2I in a nonhuman primate, we demonstrated that 4 SPECT acquisitions done 5 min after injection during 1 h were sufficient to determine the Logan plot and DVR (25).
Statistical Analysis
Differences between patients and healthy volunteers for the DVR of the caudate, putamen, and striatum were assessed with a nonparametric Wilcoxon test. Associations between clinical parameters, that is, age, Hoehn and Yahr score, and evolution of the disease, were assessed with Spearman correlation coefficients. Differences between contralateral and ipsilateral putamen in hemiparkinsonism were assessed with a Wilcoxon matched pairs test.
RESULTS
Table 1 summarizes demographic and clinical data of the 8 healthy volunteers and the 8 parkinsonian patients. Age range was similar between both populations. The sex distribution in PD was not significantly different from that in healthy volunteers. Four PD patients had a disease duration of less than 2 y, and 4 patients had more than 3 y of symptomatic clinical evolution. Four PD patients had a Hoehn and Yahr score of 1 or 1.5, reflecting unilateral extrapyramidal syndrome with or without impaired posture reflexes. Four PD had bilateral symptoms, 3 with asymmetric severity; the Hoehn and Yahr score was 2 or 2.5.
123I-PE2I SPECT in Parkinsonian Patients Versus Healthy Volunteers
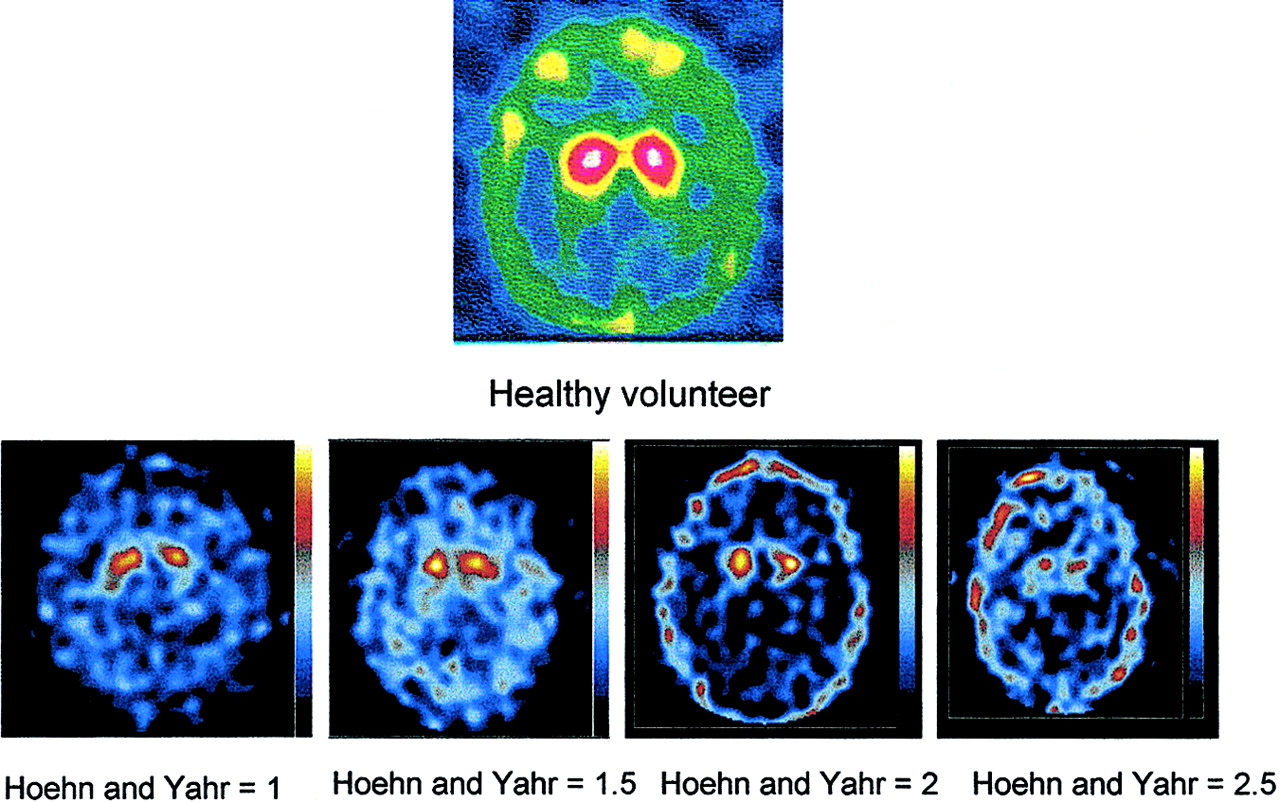
By visual analysis was observed a very high contrast between specific striatal uptake and nonspecific cortical binding in healthy volunteers and in PD patients. These data indicated a high concentration of the radiopharmaceutical in the striatum and minimal accumulation in other brain areas, in particular in the thalamus, hypothalamus, and midbrain, regions rich in 5HT and noradrenaline transporters. Figure 1 shows 123I-PE2I uptake (summation of data acquired from 20 to 35 min after injection) in striatum in 1 healthy volunteer and 4 parkinsonian patients for each Hoehn and Yahr score. In unilateral or asymmetric PD, binding of 123I-PE2I was markedly affected in contralateral putamen to the more affected side of the body but ipsilateral putamen was also affected. In addition, uptake of PE2I decreased when Hoehn and Yahr stage increased.

123I-PE2I SPECT (acquisition between 35 and 50 min after injection) of healthy volunteer and 4 PD patients according to 4 stages of Hoehn and Yahr clinical score. All PD patients are characterized by progressive reductions in dopamine nigrostriatal terminal density, first in putamen and then in caudate nucleus.
Figure 2 shows representative PE2I time–activity curves for the striatum and the occipital cortex of healthy volunteers and PD patients. These curves show rapid cerebral uptake and washout of PE2I. Striatal accumulation of PE2I after intravenous injection was rapid, reached a maximum at 15–20 min in healthy volunteers and at 10–15 min in PD patients, and then decreased. In PD patients, striatal binding decreased more rapidly than in healthy volunteers, reaching nearly background level by 1 h. This type of kinetic is consistent with reversible binding.

Kinetics of 123I-PE2I in striatum (caudate nucleus and putamen) and occipital lobe in healthy volunteer (A) and parkinsonian patient (B) according to 4 sequential SPECT acquisitions. (C) Quantification of distribution volume of 123I-PE2I in striatum according to slope of Logan plot in healthy volunteers and parkinsonian patients.
Kinetic analysis by the Logan graphical method is illustrated in Figure 2 in a healthy volunteer and a patient with severe PD. The curves became linear soon after PE2I injection. The application of the Logan graphical method resulted in a linear relationship between integral O(t)dt/S(T) and integral S(t)dt/S(T), with a least squares correlation coefficient equal to 0.9995 ± 0.0005 in the healthy volunteers and 0.9953 ± 0.0066 in the patients. PE2I DVR values in the whole striatum, right and left striata, caudate, and putamen are shown in Table 2 for healthy volunteers and patients. A nonsignificant correlation was observed between striatal DVR and age in the healthy volunteers (r = −0.461, 95% confidence interval = (−0.88; 0.36)). No correlation between age and DVR was found for PD patients. The slopes of Logan plots were significantly less in parkinsonian patients than in healthy volunteers. In all regions, the DVR values were significantly lower in patients than in healthy volunteers (P < 0.001) (Fig. 3). When we compared all parkinsonian patients with healthy volunteers, mean DVR decreases were 48%, 44%, and 41% for caudate, putamen, and striatum, respectively. In the 4 patients with a Hoehn and Yahr score lower than 2, mean reductions of DVR in caudate nuclei, putamen, and striatum were 39%, 41%, and 38%, respectively. In the 4 patients with a Hoehn and Yahr score of up to 2, mean decreases of DVR in caudate, putamen, and striatum were 57%, 48%, and 44%, respectively.

Distribution volume of 123I-PE2I in caudate nucleus, putamen, right striatum (rS), left striatum (lS), and striatum in 8 healthy volunteers (♦) and 8 parkinsonian patients (○).
123I-PE2I Striatal DVRs
Correlation Between DAT Density and Clinical Impairment
In the 7 parkinsonian patients with lateralization of symptoms, DVR was significantly more decreased in the contralateral putamen than in the ipsilateral putamen (P = 0.016) (Table 3).
123I-PE2I DVRs in Putamen Contralateral and Ipsilateral to Side with Predominant Extrapyramidal Clinical Signs: Data for 7 Parkinsonian Patients
Correlation was significant between putamen DVR and Hoehn and Yahr score (r = −0.73, P = 0.04) but not between striatum and caudate DVR. DVR in the putamen was 2.24 ± 0.49 for patients with a Hoehn and Yahr score of 1 or 1.5 and 1.98 ± 0.32 for patients with a Hoehn and Yahr score of 2 or 2.5. The difference was not significant (P = 0.148) because of the small sample size.
In PD patients, DVR values in striatum, caudate, and putamen were significantly correlated with disease duration (r = −0.84, P = 0.08; r = −0.70, P = 0.054; r = −0.65, P = 0.083, respectively). The DVR values in the putamen, caudate, and striatum of patients with a disease duration of less than 2 y were 2.60 ± 0.55, 3.84 ± 0.58, and 2.83 ± 0.34, respectively, and were significantly different from those of PD patients with a disease duration of 3–8 y (1.82 ± 0.36, P = 0.028; 2.57 ± 0.93, P = 0.06; and 2.08 ± 0.53, P = 0.057, respectively).
DISCUSSION
Brain images after PE2I injection showed a high contrast between the background, that is, cortex and thalamus, and the striatum in healthy volunteers but also in parkinsonian patients. These data agree with previous 125I-PE2I studies of postmortem human brain that documented intense binding in caudate and putamen and low binding in 5HT and noradrenaline-rich structures and in the cortex (26). These data are also concordant with PET studies using 11C-PE2I (15). Our results showed rapid kinetics for PE2I, because it reached a striatal peak of uptake between 10 and 20 min and had rapid washout in healthy volunteers and in PD patients. Kinetics were even more rapid with evolution of nigrostriatal neuronal loss in PD.
Experience with SPECT imaging of DATs in healthy volunteers and in parkinsonian patients is steadily increasing. In recent years, a series of cocaine-derivative 123I-labeled tracers have been developed that could be classified into 1 of 3 types according to their properties and kinetics. The first is the well-known 123I-β-carbomethoxy-3-β-(4-iodophenyltropane) (123I-βCIT), which binds with high affinity to DAT (Kd = 0.2 nmol/L; inhibitory concentration of 50% [IC50] = 1.6 nmol/L) but also to 5HT transporter (IC50 = 3.78 nmol/L) (27). Its kinetics are slow, as shown by a striatal time–activity curve indicating a 12- to 18-h interval to highest uptake and a slow washout of less than 0.5% per hour (28). SPECT imaging must therefore be done 18–27 h after injection, when activity in brain compartments closely approximated equilibrium binding at the DAT. The binding potential of 123I-βCIT can be simply quantified using the ratio between specific (striatum, caudate, putamen) and nonspecific (occipital lobe or cerebellum) activity during the plateau phase of tracer uptake (28). However, the prolonged wait for highest striatal uptake before SPECT can be performed is not easy to apply in clinical practice. Another difference between this tracer and PE2I is its high affinity for 5HT transporter in structures near the striatum, which can also be affected in PD, but it seemed that the kinetics of 123I-βCIT in 5HT-rich regions are more rapid (9,29). The second type of DAT tracer is 123I-FPCIT, a fluoroalkyl derivative of 123I-βCIT. Compared with 123I-βCIT, it binds with lower affinity to DAT (inhibition constant = 3.5 nmol/L) but with higher selectivity toward 5HT transporter (DAT/5HT = 2.8/1) (30). Sequential 123I-FPCIT SPECT imaging of healthy volunteers and PD patients by Booij et al. showed that the time to peak striatal uptake after injection was 3 h and that washout rates were relatively slow (31). These findings suggested that binding potential could be quantified at steady-state binding, that is, 3–6 h after injection, using a simple ratio of specific activity to background activity (31). However, a recent study showed that significant washout occurred in striatum and occipital lobes 3–6 h after injection and resulted in a transient equilibrium state, which suggests that 123I-FPCIT SPECT may not accurately quantify DAT density with the striatum–to–occipital lobe ratio (32). Finally, the third type of presynaptic tracers have a high affinity for DAT, a low affinity for 5HT and noradrenaline transporters, and rapid kinetics. Among them, 2 tracers are similar: 123I-PE2I (Kd = 4 nmol/L, DAT/5HT = 29.4/1) (13) and 123I-2β-carbomethoxy-3β-(4-fluorophenyl)-n-(1-iodoprop-1-en-3-yl) nortropane (IACFT) (Kd = 4.96 nmol/L, DAT/5HT = 25/1) (33). The high selectivity of 123I-PE2I for DAT is an important characteristic for future in vitro and in vivo studies of potential and selective neuroprotective or neurotrophic drugs on nigrostriatal neurons. Faster kinetics allow SPECT imaging within the first 2 h after injection, an interval that is convenient for clinical practice. The striatal time–activity curve showed a time to peak striatal uptake of less than 20 min, no plateau period, and rapid striatal washout after occipital washout. Logan (17) described a graphical method with or without blood sampling for quantification of the distribution volume of reversible tracer. Pinborg et al. (19) demonstrated recently that this method without blood sampling could accurately quantify the DVR of 123I-PE2I for striatum, that is, the striatal 123I-PE2I binding potential on DAT. Our data confirm that the Logan graphical method is appropriate for quantification of 123I-PE2I in healthy volunteers and in PD patients, since Logan plots always became linear even with only 4 sequential SPECT imaging sessions from 5 to 65 min after injection. The slope of the Logan plot decreased according to the severity of nigrostriatal nerve terminal degeneration. In addition, Bonad et al. (34) compared 4 methods for quantification of 123I-IACFT and validated the Logan graphical method as more appropriate for estimation of the binding potential of this tracer, which is similar to 123I-PE2I. Moreover, in a previous study in a progressive model of PD induced with 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine (MPTP) in a nonhuman primate, we showed that 123I-PE2I binding to DAT decreased even before clinical extrapyramidal signs were evident (25). Logan analysis is then confirmed as a useful method for accurate quantification of binding potential of reversible tracers, such as 123I-PE2I. According to the Logan method, DVR is derived from the kinetics of 123I-PE2I and the ratios of activity between 2 cerebral regions. This calculation reduces the variations due to counting yield differences between the 2 different cameras. Because multimodality imaging with an anatomic device was not available, we chose to define fixed geometric ROIs that demonstrated little inter- and intraindividual variability (35,36). Our data showed that 123I-PE2I is definitely an attractive tracer because of higher affinity to DAT; higher selectivity to DAT/5HT transporter, compared with that of 123I-FPCIT; rapid kinetics, resulting in a shorter SPECT acquisition protocol; and easier quantification without blood sampling with the Logan graphical method.
Moreover, our findings confirmed that 123I-PE2I is a useful tracer for studying DATs in patients with PD and thus identifying nigrostriatal degeneration. Our data demonstrated a significant decrease of PE2I binding in putamen but also in caudate nucleus in PD, whatever the clinical duration or clinical severity. In comparison, 18F-F-dopa PET imaging showed an approximately 50%–60% decrease in putamen and 20%–30% decrease in caudate in parkinsonian patients (8,10). Differences between findings could be explained by the fact that PE2I and F-dopa measure different aspects of presynaptic dopaminergic neurons, which are differently affected in PD patients. 18F-F-dopa uptake is dependent on dopamine metabolism of nigrostriatal nerve terminals, whereas 123I-PE2I binding reflects nerve terminal integrity. In our 5 patients with a disease duration of less than 2 y, the mean decrease in DVR was 40%, 32%, and 34% for caudate, putamen, and striatum, respectively. These data agree with other SPECT studies of de novo patients with unilateral or asymmetric PD (37). In asymmetric PD, uptake of the tracer was significantly more reduced in the putamen contralateral to the side of the body showing initial and more severe extrapyramidal syndrome. In patients with unilateral extrapyramidal syndrome, the interval between the diagnosis of PD and the development of bilateral symptoms is often several years. Our data show that in those patients, PE2I binding was already decreased in the ipsilateral striatum. SPECT PE2I can therefore identify PD at its early onset but also in its presymptomatic period. A study demonstrated that SPECT imaging of DAT could identify preclinical PD in at-risk family members (38). We also recently demonstrated, in a progressive MPTP nonhuman primate model of PD, that 123I-PE2I SPECT could identify lesions of dopaminergic nerve terminals before the development of extrapyramidal signs (25). These in vivo SPECT data are of prime importance because they demonstrate that SPECT can diagnose PD in the presymptomatic period. The implications of this concept are substantial, because it defines a period in which dopamine depletion progresses without symptoms. This presymptomatic period provides an opportunity for presymptomatic diagnosis and therapeutic intervention, ideally the administration of neuroprotective compounds. Our data demonstrate that putamen DVR is related to the severity of clinical symptoms and disease duration, a finding that corroborates previous SPECT studies of the DAT with other tracers such as 123I-βCIT (9,29) and 123I-FPCIT (7,31). The decrease in DVR, compared with Hoehn and Yahr score, was more important in caudate than in putamen, as agrees with other SPECT studies showing that the putamen-to-caudate ratio decreases with increasing Hoehn and Yahr stage (39). Our data demonstrate that 123I-PE2I SPECT is sensitive for longitudinal studies after progression of dopaminergic degeneration in PD. SPECT provides an opportunity for better understanding the pathophysiology of PD.
CONCLUSION
Our findings indicated that 123I-PE2I SPECT with the Logan graphical method is useful for estimating nigrostriatal neuronal loss in patients with PD. One main advantage of 123I-PE2I is its rapid kinetics, allowing SPECT acquisition 1 h after injection. We also observed a correlation between striatal 123I-PE2I binding and disease duration and clinical features, suggesting that SPECT can be used to follow progression of the disease. One promising use of SPECT with 123I-PE2I is the diagnosis of nigrostriatal degeneration in the presymptomatic period. This preclinical SPECT diagnosis of PD offers an opportunity for future early administration of neuroprotective therapeutics. Our findings suggest that quantitative PE2I SPECT can be a useful method to determine the neuroprotective potential of drugs.
Acknowledgments
This study was supported by the EUREKA Program (Dopimag) and by a grant from Tours University Hospital.
Footnotes
Received Aug. 2, 2002; revision accepted Jan. 13, 2003.
For correspondence or reprints contact: Caroline Prunier, MD, Service de Médecine Nucléaire, CHRU Hôpital Bretonneau, 2bis boulevard Tonnellé, 37044 Tours Cedex, France.
E-mail: c.prunier{at}chu-tours.fr




{kind=link}
{kind=link}
{kind=link}