


Abstract
Dynamic cholescintigraphy (DCG) is a valid technique for evaluating gallbladder emptying. Cholecystokinin (CCK) as a slow infusion is recommended as a contraction stimulus. The normal ejection fraction (EF) has been shown to be reproducible, although the reproducibility of abnormal results has not been investigated. The aims of the present study were to standardize the CCK administration method (phase 1), obtain EF normality values (phase 2), and evaluate the reproducibility of abnormal results in patients with clinically suspected gallbladder dysfunction (phase 3). Methods: Phase 1 included 40 healthy volunteers divided into 4 groups (n = 10) and subjected to intravenous CCK infusion according to 4 different regimens (0.25, 0.30, 0.40, and 0.60 Ivy dog units [IDU]/kg). Phase 2 comprised 33 healthy volunteers for determining DCG normality values, and phase 3 evaluated the reproducibility of abnormal results in 44 patients having clinical manifestations compatible with gallbladder dysfunction and showing an abnormal EF in a previous study. Results: The most effective CCK infusion regimen was 0.40 IDU/kg (3.07 ng/kg) over 20 min, because it afforded the least variability and a high EF. When this regimen was applied to the healthy population, the EF was found to be 74.2% ± 17.1% (mean ± SD); the inferior normality limit was estimated to be 40%. Abnormal results were recorded in 77% (95% confidence interval, 62%–89%) of the patients. When the 2 DCG studies of phase 3 were compared, the EF correlation coefficient between them was 0.439 (P = 0.003). Conclusion: Slow CCK infusion is the best regimen for stimulating gallbladder contraction; an EF of less than 40% is estimated to represent abnormality. The abnormal results for the EF in patients with clinically suspected gallbladder dysfunction proved to be reproducible.
Dynamic cholescintigraphy (DCG) has been shown to be a valid technique for evaluating gallbladder emptying. In 1981, Krishnamurthy et al. (1) described the technique. Several methodologic modifications have since been incorporated, and much information has been gathered on the role of DCG in diagnosing patients with clinically suspected gallbladder dysfunction (2). Although other techniques are available, DCG is generally considered the gold standard. Nevertheless, some authors disagree with this opinion (3).
The usual stimulus for inducing gallbladder contraction is cholecystokinin (CCK) in its different molecular forms—fundamentally CCK-33 (4) and the octapeptide (CCK-8) (5)—although there are no uniform criteria for dose and method of administration. In any event, CCK infusion for a prolonged period appears to afford a more physiologic gallbladder response than rapid bolus administration (6). Good reproducibility of normal results in healthy controls has been observed (7). Although the reproducibility of abnormal results associated with gallbladder dysfunction has not been investigated, such results justify treatment with cholecystectomy, which has been found to be effective (7).
The aims of the present study were to standardize the DCG method for evaluating gallbladder function and to assess the reproducibility of abnormal results in patients with clinical manifestations compatible with gallbladder dysfunction.
MATERIALS AND METHODS
The study design included 3 consecutive phases. In phase 1, the technique was standardized, establishing the most appropriate CCK dose and infusion time. In phase 2, the normality values in our setting were calculated. Finally, in phase 3, the reproducibility of pathologic results in patients with clinically suspected gallbladder dysfunction was evaluated.
Subjects
Standardization of the Technique.
A total of 40 healthy volunteers were included (21 women and 19 men; mean age, 37 y [range, 18–66 y]) after informed consent was obtained. The absence of disease was based on the anamnesis, physical examination, and results of basic laboratory tests (including complete blood count and blood biochemical analyses). An abdominal ultrasound study was also performed. None of the volunteers was receiving pharmacologic treatment capable of interfering with digestive function in general or with biliary motility in particular. Women were not using oral contraceptives and were neither pregnant nor lactating.
Four groups (n = 10) were established to analyze the effects of 4 different CCK administration regimens (Table 1).
Characteristics of 4 Groups for Analyzing Effects of CCK Doses on Gallbladder Dynamics, LP, EP, and EF
Calculation of Normality Values.
Thirty-three healthy volunteers were included (18 women and 15 men; mean age, 40 y [range, 19–67 y]) on the basis of the same criteria as in the preceding phase. Only 3 volunteers (2 men and 1 woman) were more than 20% above ideal body weight.
Reproducibility of Abnormal Results.
Forty-four patients (41 women and 3 men; mean age, 45 y [range, 25–71 y]) who had a clinical syndrome compatible with gallbladder dysfunction, on the basis of the Rome diagnostic criteria (2), and who had an abnormal ejection fraction (EF) at an initial DCG evaluation underwent another DCG study within 15 d. The Rome criteria are episodes of severe steady pain located in the epigastrium and right upper quadrant and all of the following: symptom episodes that have lasted 30 min or more, with pain-free intervals; symptoms that have occurred on one or more occasions in the preceding 12 mo; pain that is steady and interrupts daily activities or requires consultation with a physician; no evidence of structural abnormalities to explain the symptoms; and abnormal gallbladder functioning with regard to emptying.
Technique and Data Acquisition
Abdominal isotopic activity was continuously recorded during the study with a digital gamma camera (Orbiter, Digitrac 37; Siemens, Gammasonics Inc., Des Plaines, IL) connected to a pinhole-type collimator. A computer was used to program the recording, acquiring, and storing of serial 64 × 64 matrix images at a rate of 1 image per minute for later analysis.
The studies were carried out with the patients under fasting conditions for at least 8 h. After receiving an explanation of the characteristics of the test, the patients were placed in the dorsal decubitus position on a stretcher positioned to allow focusing of the collimator over the study zone. The patients were instructed to avoid large respiratory movements and to minimize all other types of movement. To avoid superposition of activity in different areas of the biliary tract and duodenum, the gamma camera collimator was oriented 30° to the left and 10° caudal, as close as possible to the patient, and placed so that the liver zone (the first area visualized) was located approximately in the upper left quadrant of the screen to ensure good recordings of the extrahepatic biliary tract and gallbladder activity.
The radioactive drug, 111 MBq (3 mCi) of 99mTc-disofenin, was administered as a slow intravenous injection with physiologic saline perfusion in a vein of the forearm while the cannula was maintained in place. Once the gallbladder was visible as a result of filling with radioactively labeled bile (generally 30–45 min after administration of the isotope), the recording of gallbladder isotopic activity was started (time 0). After 5 min, CCK-33 (KabiVitrum, Stockholm, Sweden) administration was started via the intravenous route with an infusion pump. After the completion of CCK-33 perfusion, the recording of gallbladder isotopic activity was continued for another 20 min.
All of the recorded studies were analyzed on the computer. An area of interest corresponding to the gallbladder was defined on an image resulting from summation of all study images. An activity curve was plotted (counts per minute over time) for the area of interest, with correction for the background activity and physical decay of the isotope.
Three parameters were evaluated: gallbladder EF, the latency period (LP), and the ejection period (EP). Gallbladder emptying was considered to exist when a decrease in counts to at least 5% was recorded. The LP was in turn defined as the time (in minutes) elapsed between the start of CCK infusion and the start of gallbladder emptying; the EP was defined as the duration (in minutes) of gallbladder emptying. The EF reflected (in percentage form) the amount of bile ejected from the gallbladder as a function of the change in isotopic activity. The value was calculated from the following equation: [(counts before contraction − counts at end of contraction)/counts before contraction] × 100.
CCK-33 Dose
Four CCK-33 administration regimens were tested to standardize the technique (Table 1). The selection of the most effective dose was based on the variation coefficient estimated from the EF values obtained for the 4 study groups to identify the regimen with the least variability. CCK-33 was administered in the study groups for which the normality values and reproducibility of abnormal EF results were investigated (phases 2 and 3) by use of the regimen with the least variability in phase 1 (standardization of the technique).
Statistical Analysis
Quantitative variables are given as mean, SD, and maximum and minimum values. Qualitative variables are given as percentages. The formula SD/mean was used to calculate the variation coefficient. The 95% confidence intervals were calculated by means of an exact method (CIA, version 1.1). The paired or unpaired Student t test was used for the comparison of means, and the Pearson correlation coefficient was used to determine the correlation between variables.
Ethical Considerations
As a requirement before the studies were conducted, all subjects gave their oral consent to participate after receiving a detailed explanation of the method and aims of the study. They were also duly informed of the remote possibility of side effects resulting from CCK-33 administration and the limited radiation exposure involved.
RESULTS
Phase 1: Standardization of the Technique
The gallbladder was clearly visualized in all of the studies 30–45 min after administration of the isotope. No patient experienced side effects as a result of CCK-33 administration. The results obtained for the 4 study groups are shown in Table 1. EF values gradually increased at higher doses and with more prolonged CCK-33 infusion, with statistically significant differences between group I (short infusion lasting 3 min) and groups III and IV, involving longer infusion times (20 and 30 min, respectively). However, statistical significance was not reached for comparisons of the differences between groups I and II and among groups II, III, and IV.
The LP was identical in all groups. Significant differences were recorded for the EP between infusion for 3 min (group I) and the longer perfusions as well as between infusion for 15 min (group II) and infusion for 30 min (group IV).
The variation coefficients for the EF were 0.45 in group I, 0.44 in group II, 0.26 in group III, and 0.32 in group IV. The regimen corresponding to group III (0.40 Ivy dog units [IDU]/kg or 3.07 ng/kg over 20 min) was regarded as the most effective regimen, because it afforded the least variability and a high EF, with no significant differences from group IV.
Phase 2: Calculation of Normality Values
The studies were carried out by administering CCK-33 as a gallbladder contraction stimulus by use of the regimen selected in phase 1 (0.40 IDU/kg or 3.07 ng/kg over 20 min). In all of the studies, CCK-33 infusion induced gallbladder emptying, with an EF of between 38% and 96%. Table 2 shows the values corresponding to gallbladder dynamics. There were no differences on the basis of sex, and no correlation was observed between patient age and the EF.
LP, EP, and EF in Groups Studied in Phase 2 (n = 33)
When the values obtained in phase 2 were compared with those recorded in phase 1 for 10 individuals subjected to the same cholecystokinetic stimulus (group III), the LP values were found to be identical (4 ± 2 min) and the EP values were found to be similar (28 ± 6 min vs. 30 ± 5 min). Although the EF values were somewhat higher (74.2% ± 17.1% vs. 68.3% ± 18.1%), statistical significance was not reached. The EF values were similar with or without inclusion of overweight subjects.
The EF inferior normality limit was established to be 40%. This value was calculated by subtracting 2 SDs from the mean. When this EF was used as a cutoff value, results for 2.5% of the studied subjects were found to be below the normality limit; this percentage agreed with that determined by the method used to identify the normality limit (population mean minus 2 SDs).
Phase 3: Reproducibility of Abnormal Results
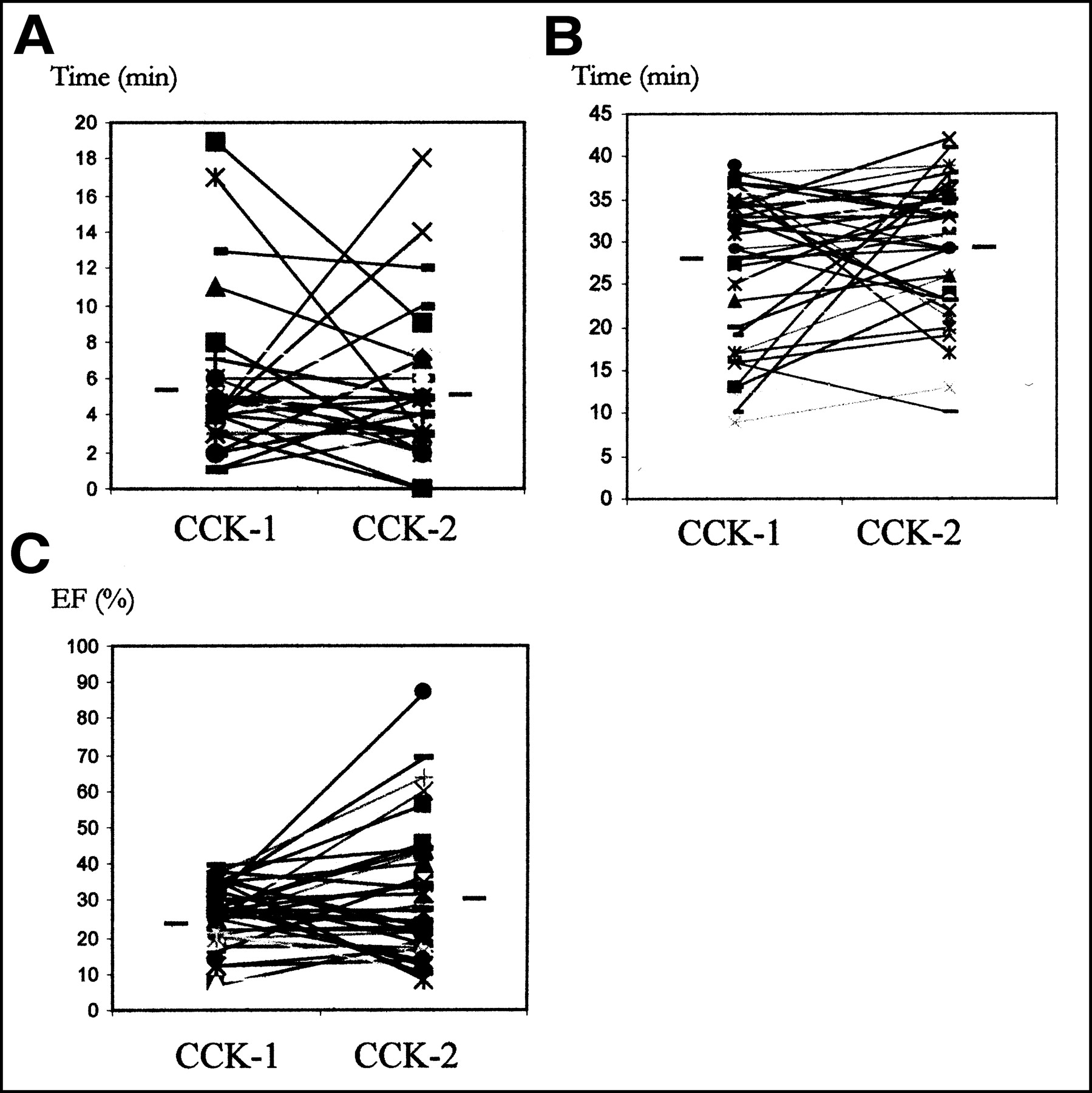
No statistically significant differences were observed for any of the parameters corresponding to gallbladder dynamics when the results of both studies in phase 3 (CCK-1 and CCK-2 doses) were compared (Table 3). The correlation coefficient between the EF values in the 2 studies was 0.439 (P = 0.003). For 10 of the 44 tested patients, the second study showed a normal EF; consequently, abnormal results were recorded in 77% (95% confidence interval, 62%–89%) of the patients. For all patients with an EF of less than 23% in the first study, abnormal results were also recorded in the second study. Figure 1 shows the individual EP, LP, and EF values for both studies.

Graphic representation of LP (A), EP (B), and EF (C) for CCK-1 and CCK-2 doses. Only the data corresponding to those for patients with an abnormal EF (≤40%) in the first study are shown. Horizontal bars represent mean values.
LP, EP, and EF in 2 Studies of Phase 3 (CCK-1 and CCK-2 doses) for 44 Patients Each
In 6 patients, CCK infusion was followed by pain similar to that seen in the clinical syndrome, although only 1 patient also experienced such pain in the first study.
DISCUSSION
DCG is a useful technique for studying gallbladder function (8). In this context, DCG quantifies gallbladder emptying according to the decrease in gallbladder isotopic activity resulting from the stimulation of gallbladder contraction. Laboratory studies simulating in vivo conditions (1,9) have shown the existence of a relationship between the decrease in isotopic activity and volume reduction. At present, scintigraphic techniques are considered to be the best option for investigating gallbladder dynamics in both the interdigestive (9) and the digestive (1,5,7,10–15) periods.
The octapeptide of CCK (sincalide, or CCK-8), which was the first molecular form available for clinical use in the United States, has been the stimulus used in many studies. In early publications, the dose ranged from 5 to 40 ng/kg, administered as a bolus or as a rapid infusion (1–3 min) (1,5,11–13). This method yielded a variable EF of between 20% and 60%. The general recommendation was the administration of a dose of 5–10 ng/kg as an infusion over approximately 3 min (3.3 ng/kg/min). With this method, the EF was considered to be pathologic when it was less than 35% (13). The administration of larger doses increased the incidence of side effects (particularly abdominal pain and nausea), without improved cholecystokinetic results. According to in vitro studies (16), a dose of 5–10 ng/kg is equivalent to 0.65–1.30 IDU of CCK-33 per kg. In the present study, we perfused a much lower dose over 3 min (0.25 IDU/kg) and obtained EF values similar to those reported in studies with CCK-8 at higher doses, with values ranging between 32% and 68% (1,11–13).
Rapid CCK infusion has been suggested to be nonphysiologic, inducing ineffective contraction in some subjects (6). Pauletzki et al. (17) found that high CCK doses do not overcome gallbladder emptying defects; on the contrary, they actually reduce the EF via an unclear mechanism. These observations suggest the administration of low CCK doses over relatively long periods to be the best approach for attempting to reproduce postprandial gallbladder emptying as precisely as possible.
Starting in 1985, studies in which CCK-8 administration was performed over longer periods began to appear. The most widely used dose was 20 ng/kg, administered over 20–45 min (7,10,12,14); this regimen was equivalent to a CCK-33 dose of between 0.04 and 0.08 IDU/kg/min. These values were higher than those used in other studies (4), including our own. Ziessman et al. (12) compared 3 infusion regimens: 20 ng/kg over 3 min (6.6 ng/kg/min), 20 ng/kg over 30 min (0.6 ng/kg/min), and 10 ng/kg over 30 min (0.03 ng/kg/min). In this context, the administration of CCK-8 over 30 min afforded a higher EF value and less variability than rapid infusion over 1–3 min as well as no side effects. Studies involving CCK-33 have generally used low doses as a prolonged infusion (15–30 min and even 60 min) and have reported more physiologic results (6). With a dose of 0.02 IDU/kg/min for 30 min, Pomeranz and Shaffer (4) obtained an EF value of 81.5%. This dose was chosen for our study, but with different infusion times (15, 20, and 30 min). The resulting EF values (higher than those afforded by a short, 3-min perfusion) were similar to the values reported in studies with CCK-8 (12,14) and coincided with the findings of earlier studies that revealed a direct relationship between gallbladder contraction and plasma CCK concentration (18). Of the 4 dosing regimens used, the 20-min infusion regimen had the lowest variation coefficient, with an EF not significantly different from that obtained with infusion over 30 min. This regimen was chosen for the subsequent study phases. When this regimen was used for the control group, the results obtained were nearly analogous to those reported in other series (7).
EF normality values are not the same in all studies, with the establishment of a lower limit of between 35% (19–21) and 50% (22). For all of the subjects in our study, CCK-33 infusion induced gallbladder emptying with an EF of between 38% and 96%; the inferior normality limit was calculated to be 40%. This value was obtained by subtracting 2 SDs (17.1%) from the mean (74.2%). As a result, we were able to discriminate subjects with abnormal responses with a high degree of reliability, because only 2.5% of healthy subjects would have values below that estimated. Although the EF values in this group were higher than those in the 10 phase 1 patients who received the same stimulus (74.2% ± 17.1% vs. 68.3% ± 18.1%), they failed to reach statistical significance—an observation that offers indirect proof of the reproducibility of normal results, as already reported elsewhere (7,23,24).
The diagnosis of gallbladder dysfunction requires the demonstration of altered emptying (2). The evaluation of gallbladder emptying is therefore important both for establishing a diagnosis and for deciding the management approach. It is therefore essential for the results obtained to be reliable. In this context, DCG offers demonstrated reproducibility for healthy controls (7,23,24), although to our knowledge there have been no evaluations to date of the reproducibility of pathologic results, which in our series reached 77% of all patients (100% when the EF was found to be less than 23% in the first study).
In addition to its known effects on the biliary tract, CCK exerts actions at other levels. It may thus be expected to produce side effects when administered at high doses, particularly over short infusion times (12). In our study, no side effects were recorded with any of the dosing regimens used. For the group of patients with clinically suspected gallbladder dysfunction, postadministration pain similar to the pain seen in the clinical syndrome was reported by 6 patients.
CONCLUSION
Our results confirm the advisability of administering CCK at low doses and over prolonged infusion times to stimulate gallbladder contraction; the optimum CCK-33 dosing regimen in our series was 0.40 IDU/kg (3.07 ng/kg) over 20 min. This approach allowed the estimation of an EF of 40% as the inferior normality limit. Good reproducibility was observed for abnormal results in patients with clinically suspected gallbladder dysfunction.
Footnotes
Received Jul. 1, 2002; revision accepted Oct. 8, 2002.
For correspondence or reprints contact: Julio Ponce, MD, Servicio de Medicina Digestiva, Hospital Universitario La Fe, Avda. Campanar 21, 46009 Valencia, Spain.
E-mail: jponce{at}doymanet.es




{kind=link}