


Abstract
This study investigated the feasibility of PET with 18F-FDG to evaluate retrospectively early recurrence in patients with cervical cancer. Methods: From September 1997 to March 2000, 249 patients with no evidence of cervical cancer after treatment were investigated with 18F-FDG PET. 18F-FDG PET scanning, beginning 50 min after injection of 370–555 MBq 18F-FDG, was performed. 18F-FDG uptake other than physiologic uptake was evaluated with the standardized uptake value and was analyzed by 2 observers who were unaware of CT or MRI data. CT or MRI and needle biopsies were performed to evaluate the positive lesions on 18F-FDG PET, and all patients were monitored closely for 6 mo for recurrence. Results: Of the 249 patients, 80 patients (32.1%) showed positive lesions with 18F-FDG PET, and 28 patients (11.2%) were clinically or histologically confirmed as having recurrences. Eighty-two percent of recurrence was detected within 6–18 mo after diagnosis, and 89% of recurrence occurred in Fédération Internationale de Gynécologie et d’Obstétrique (FIGO) stage IIb and stage III patients. The sensitivity and specificity of 18F-FDG PET for detection of early recurrence were 90.3% and 76.1%, respectively. The sensitivity of 18F-FDG PET was high in mediastinal, hilar, and scalene lymph nodes, spine, and liver; however, the sensitivity was relatively low in lung, retrovesical lymph nodes, and paraaortic lymph nodes. Three false-negative cases were detected in lung, retrovesical lymph nodes, and paraaortic lymph nodes. Conclusion: 18F-FDG PET was effective in detecting early recurrences in cervical cancer patients with no evidence of disease. 18F-FDG PET may be a useful follow-up method for cervical cancer, thereby providing the patients with early opportunities for sophisticated treatments.
Cervical cancer is one of the most common gynecologic malignancies throughout the world. Although the overall mortality from cervical cancer has decreased because of early detection and treatment of preinvasive disease, it still remains one of the leading causes of cancer death (1). Despite of carefully planned and executed treatments, approximately 30% of cervical cancer is known to eventually recur after treatment (2). Conventional follow-up methods, such as physical examination, Papanicolaou smear (Pap smear), and tumor markers, and radiologic imaging methods, such as CT or MRI, have been used to detect early recurrence; however, it is very difficult to achieve an early diagnosis of pelvic recurrence of cervical cancer (3).
PET with 18F-FDG, which is preferentially trapped in tumor cells, reveals a functional image of high glucose metabolism (4,5). Recently, 18F-FDG PET has been widely used for detection of early recurrence that cannot be diagnosed with conventional radiologic imaging studies and is known to be more accurate than CT or MRI in detecting recurrent lymph node metastases in several human cancers (6). In lung cancer, 18F-FDG PET showed 81% accuracy on the involvement of mediastinal lymph nodes, whereas CT showed only 52% accuracy (7). Similar observations have also been reported in breast cancer, melanoma, and other cancers (8,9).
In cervical cancer, the role of 18F-FDG PET has not been well established. Recently, Sugawara et al. (10) reported that 18F-FDG PET could detect 100% of cancers and 86% of lymph node metastasis, whereas CT was positive in 57% of lymph node metastasis in 21 cervical cancers, suggesting a promising role of 18F-FDG PET in cervical cancer detection. In other studies, 18F-FDG PET is known to be very effective not only in detecting early recurrences but also in preoperative staging and evaluating the response of treatment (11–17). However, the feasibility of 18F-FDG PET in the early detection in cervical cancer recurrence is not well established.
The purpose of this study was to assess the feasibility of 18F-FDG PET in detecting early cancer recurrences in patients with no evidence of the ailment unmasked by conventional imaging methods.
MATERIALS AND METHODS
Patients
From September 1997 to March 2000, 249 patients with cervical cancer, showing no evidence of disease after treatment, underwent 18F-FDG PET as part of their investigations. The patients had histologically proven cervical cancers and were treated with surgery or radiation combined with or without chemotherapy according to the Fédération Internationale de Gynécologie et d’Obstétrique (FIGO) clinical stage. The detection rate of 18F-FDG PET for recurrences was analyzed retrospectively.
All patients were treated and monitored according to standard protocol. In brief, most of the patients with stage Ib and stage IIa were treated with radical hysterectomy and bilateral pelvic lymphadenectomy. Postoperative adjuvant radiation therapy was performed on patients with high-risk factors such as full-thickness involvement of the cervix, parametrial invasion, lymphatic invasion, and positive resection margin. Definitive radiation therapy without (before 1999) or with (after 1999) chemotherapy was performed on patients with stage IIb or higher, and chemotherapy was performed on patients with distant metastasis. The chemotherapy regimen was based mainly on cisplatin, such as 5-fluorouracil (500 mg/m2) + cisplatin (50 mg/m2) or cyclophosphamide (500 mg/m2) + cisplatin (50 mg/m2). After treatment, patients were monitored every 3 mo in the first 2 y and every 6 mo thereafter for 5 y with tumor markers, Pap smears, chest radiography, and annual pelvic CT or MRI.
In patients who had undergone surgery, no evidence of disease was defined as normal follow-up tests, including physical examination, chest radiography, tumor marker (squamous cell carcinoma antigen), Pap smear, and annual radiologic imaging studies. In patients who were treated with radiation, those who showed complete disappearance of the lesion on radiologic imaging studies performed at least after 6 mo of treatment and who showed normal follow-up tests (described above) were defined as having no evidence of disease.
18F-FDG PET was recommended as a part of the work-up on all patients with high risk factors for recurrence such as full-thickness involvement of the cervix, parametrial invasion, lymphatic invasion, and positive resection margin. Among them, 249 patients, who showed no evidence of disease on previous annual pelvic CT or MRI, physical examination, chest radiography, tumor marker, and Pap smear, were selected retrospectively for analysis.
PET
Patients were prepared with overnight fasting before 18F-FDG injection. 18F-FDG PET was performed on an Advance HR+ scanner (General Electric, Waukesha, WI), starting 50 min after injection of 370–555 MBq (10–15 mCi) 18F-FDG with the bladder emptied by Foley catheter insertion and injection of diuretics to reduce tracer activity in the bladder.
18F-FDG PET images were interpreted by using a dedicated system (ECAT EXACT 921; Siemens/CTI, Knoxville, TN) with a 10.8-cm transverse field of view and a 2-dimensional acquisition mode. Three- to 5-min transmission scans and 8-min emission scans were obtained. Five or 6 bed positions were used to cover the area from the orbitomeatal line to the midfemoral line. Images were reconstructed on transaxial, sagittal, and coronal planes by means of the ordered-subset expectation maximization algorithm and segmented photon absorption correction and were interpreted by 2 observers on both film and computer displays, who were unaware of the clinical information of previous treatment and of annual CT or MRI data. Any focal uptake of 18F-FDG, which is considered not be physiologic on PET images, was measured on the basis of the standardized uptake value, being the radioactive concentration in a hot spot divided by the injected dose and the patient’s body weight.
Diagnosis of Recurrence
Any positive lesion on 18F-FDG PET was evaluated with CT or MRI and was confirmed for recurrence histologically by fine-needle aspiration (FNA) as quickly as possible. For the lymph nodes in the mediastinum, hilum, paraaorta, and pelvis, lymph nodes of >1 cm in the short axis on CT were interpreted as positive for metastasis. Lymph nodes that had prominent uptake on 18F-FDG PET but were <1 cm in the short axis were reevaluated with CT 3 mo later. If there was no change in the size on the follow-up CT scan, the patients were recommended to follow-up every 3 mo for 1 y. All scalene lymph nodes with obvious 18F-FDG uptake were evaluated for recurrence with FNA or node dissection.
Any prominent lesion in the lung parenchyma on 18F-FDG PET was evaluated for recurrence with chest CT and histologically confirmed by FNA or lung biopsy. Small lung lesions of <0.5 cm, which were difficult to access with FNA, were evaluated with CT 3 mo later. If there was no change in the size on the follow-up CT scan, the patients were recommended to follow-up every 3 mo for 6 mo.
In other body regions such as the retrovesical area, liver, and chest wall, any lesion of >1 cm in size on CT was confirmed by FNA. A prominent uptake on 18F-FDG PET of <1 cm in the short axis was reevaluated with CT 3 mo later. If there was no change in size on the follow-up CT scan, the patients were recommended to follow-up every 3 mo for 6 mo.
CT or MRI images to confirm recurrences were analyzed by 2 separate observers, who were unaware of 18F-FDG PET data and clinical information. If there was no histologic evidence of recurrence, we decided there was no evidence of disease after close follow-up for 1 y.
RESULTS
The median age of the patients was 51 y (range, 31–78 y), and 59.7% of the patients were classified as FIGO stage Ib and stage IIa. Histologically, 90.7% of the cervical cancer was squamous cell carcinoma. The duration of no evidence of disease at the point of 18F-FDG PET was not statistically different in stages Ib, IIa, and IIb; however, 18F-FDG PET scans were obtained earlier in patients with stage III than in patients with other stages. The median interval from the last CT or MRI to 18F-FDG PET was 6 mo (Table 1).
Patient Characteristics
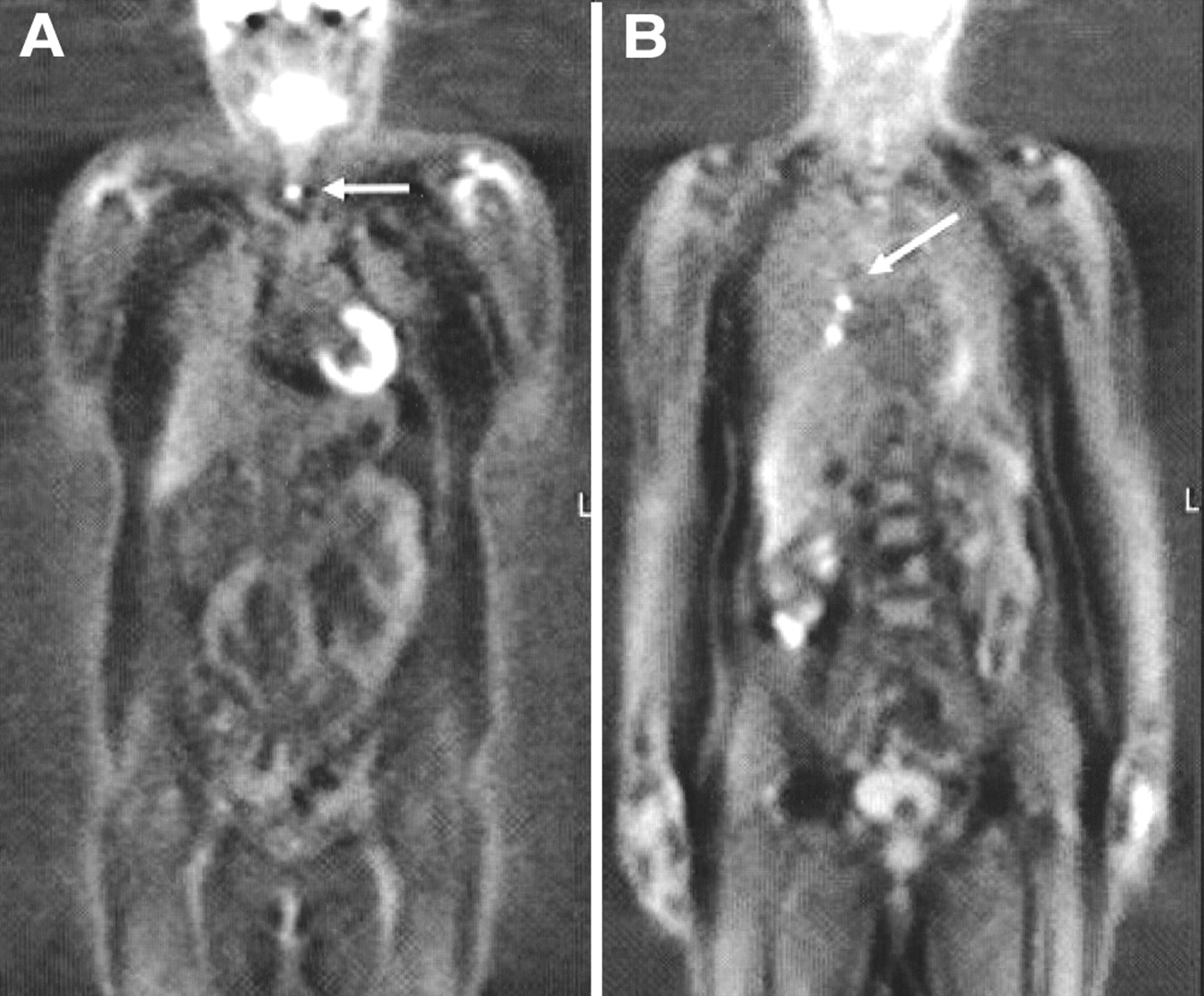
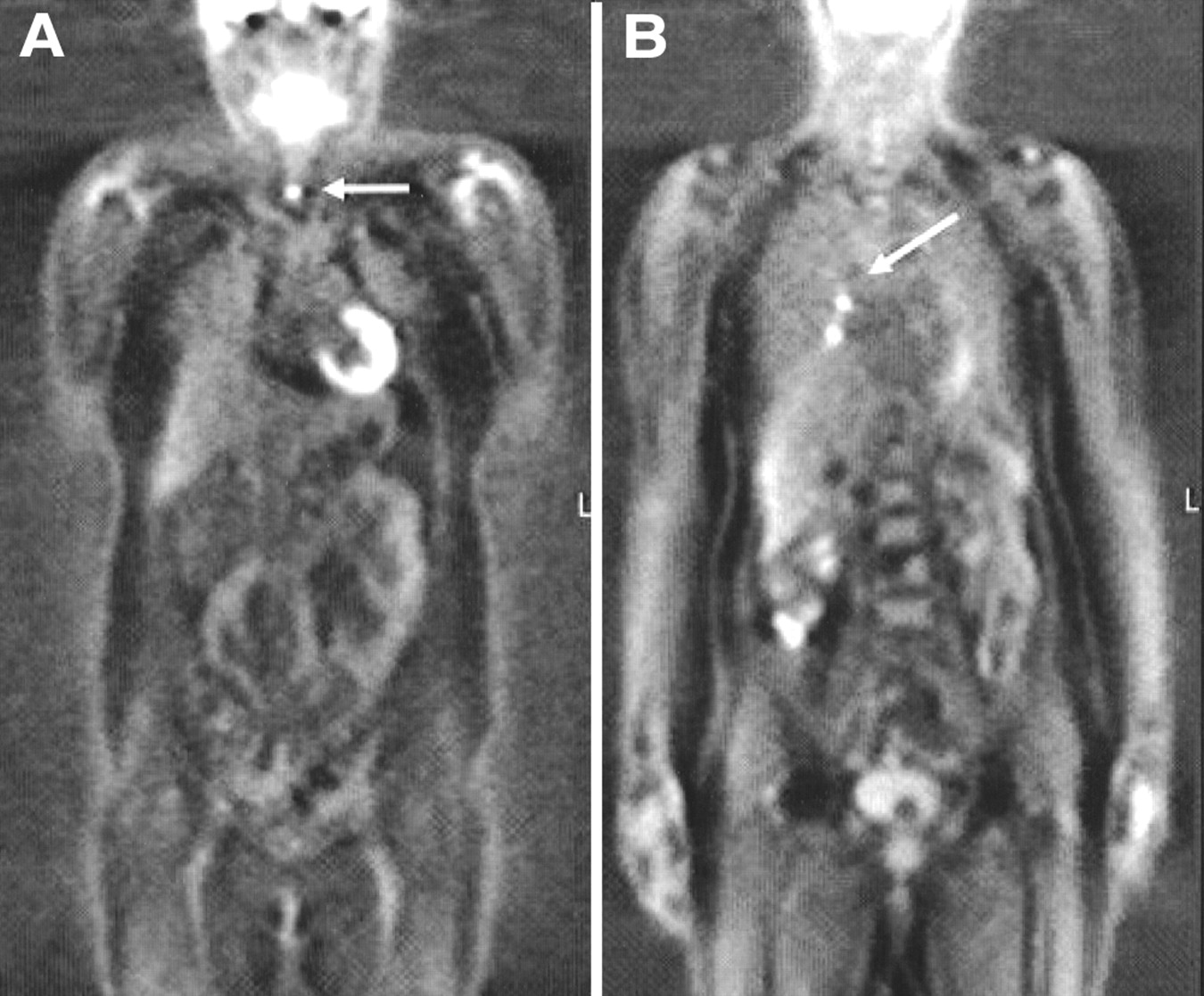
Of the 249 patients with cervical cancer who showed no evidence of disease after treatment, 80 patients (32.1%) showed positive lesions on 18F-FDG PET (Table 2). Among the 80 patients with positive 18F-FDG PET scans, 28 patients (11.2% [28/249 patients]) were clinically or histologically confirmed to have recurrent lesions (Fig. 1). The sensitivity and specificity of 18F-FDG PET in detecting recurrences of cervical cancer were 90.3% and 76.1%, respectively. Positive and negative predictive values of 18F-FDG PET in detecting recurrence of cervical cancers were 35% and 98.2%, respectively.

Detection of recurrences by 18F-FDG PET in patients with cervical cancer showing no evidence of disease. (A) Multiple recurrences in lung (↙). (B) Right scalene lymph node metastasis (←). (C) False-positive hilar lymph nodes (↘).
Detection of Early Recurrence with 18F-FDG PET in Cervical Cancer
Most recurrences were detected within 18 mo after diagnosis of the disease, and the peak period of detection was 9–12 mo after diagnosis (Fig. 2). The detection rate of 18F-FDG PET according to the stage was higher in FIGO stages IIb and III than in stages Ib and IIa (20.4% and 29.4% vs. 6% and 6.1%, respectively) (Fig. 3).

Detection of recurrences by 18F-FDG PET in patients with cervical cancer showing no evidence of disease (NED).

Detection of recurrences by 18F-FDG PET according to stage of patients with cervical cancer showing no evidence of disease.
The sensitivity of 18F-FDG PET was relatively high in lesions such as the mediastinum, hilum, chest wall, scarlene lymph node, iliac, spine, and liver; however, it was relatively low in lesions including the lung, retrovesical area, and paraaortic lymph node. The specificity of 18F-FDG PET was relatively low in lesions such as the lung, retrovesical lymph node, and paraaortic lymph node (Table 3). Incidentally, as shown in Figure 4, 18F-FDG PET detected 2 cases each of thyroid cancer and tuberculosis.
18F-FDG PET incidentally detected 2 cases each of thyroid cancer and tuberculosis in patients with cervical cancer who showed no evidence of disease after treatment. (A) Thyroid cancer (←). (B) Tuberculosis (↙).
Clinical Significance of 18F-FDG Uptake According to Location of Recurrence
DISCUSSION
This study showed that 18F-FDG PET is a useful method to detect early recurrences in patients with cervical cancer who showed no evidence of disease after treatment. Because all patients in the study showed no evidence of disease on physical examination, tumor markers, chest radiography, and annual pelvic CT or MRI, the 28 patients who were confirmed to have recurrence were detected only by 18F-FDG PET.
It is estimated that approximately 35% of patients with invasive cervical cancer will have recurrent or persistent disease after therapy (2). Conventional imaging modalities such as CT or MRI were performed to detect early recurrent lesions; however, the detection rate is low (18). Sugawara et al. (10) reported that 18F-FDG PET could detect lymph node metastasis more accurately than CT or MRI in patients with cervical cancer. 18F-FDG PET could detect recurrences in small lesions of <1 cm and in the retrovesical area, which are frequently obscured by postradiation fibrosis. In a retrospective study performed on 13 patients with cervical cancer, 18F-FDG PET could detect recurrences in 10 patients who had recurrences in the iliac lymph node, liver, lung, and paraaortic lymph node, suggesting a promising role of 18F-FDG PET in cervical cancer (16).
The higher feasibility of 18F-FDG PET over CT or MRI in detecting recurrences of cervical cancer may be explained by several factors. First, because 18F-FDG PET scans can provide functional information on the lesions rather than anatomic images, it can detect recurrent lesions independent of the size (7–9). Furthermore, as already well recognized in head and neck cancers (6,19), 18F-FDG PET provides more important images when anatomy has been distorted after surgery or radiation treatment. In our study, 18F-FDG PET could detect occult recurrent metastasis in lesions such as the vaginal cuff, retrovesical area, and pelvic sidewall, where it is difficult to differentiate between fibrosis and recurrence.
The other advantage of 18F-FDG PET is that it can show a whole-body image at one time. Approximately 70% of recurrences of cervical cancer are estimated to be distant or a combination of local and distant metastases (2). Most of the distant metastasis is detected in an already far-advanced state with clinical symptoms such as cough, hemoptysis, and pain. Because 18F-FDG PET can provide a whole-body image at one time, distant metastases, which are usually not evident on routine pelvic CT or MRI, can easily be detected by 18F-FDG PET. In this study, 18F-FDG PET was useful in detecting metastasis in lesions such as the scarlene lymph node, lung, and mediastinum, where it was difficult to detect recurrence with conventional imaging modalities. Two cases each of pulmonary tuberculosis and thyroid cancer, incidentally detected in this study, also benefited from the whole-body image of 18F-FDG PET.
Most recurrence in cervical cancer is known to occur within 2 y after therapy (2); however, the peak period of recurrence detected by 18F-FDG PET in this study was 9–12 mo after treatment. This finding suggested that 18F-FDG PET might detect recurrences earlier than historical data with conventional methods (2). Moreover, because the recurrence rate of cervical cancer is higher and distant metastasis is more common in advanced diseases, 18F-FDG PET is a more useful method to detect recurrence in patients with advanced stages of disease.
Our results showed that the false-positive rate of 18F-FDG PET was relatively high in lesions such as the hilum, neck, lung, inguinal area, and axillae. Three false-negative cases were illustrated in the paraaortic lymph node and the retrovesical area. Even though we usually correct the standardized uptake value according to the depth of the lesions by the transmission scan, it was highly likely that there were more false-positive lesions in the superficial area than in deep areas such as the paraaortic lymph node and the retrovesical area. More thoughtful consideration according to the depth of lesions may be necessary in interpreting the significance of 18F-FDG uptake. However, the most important step for detection of early recurrences is a suspicion of recurrence, which leads the physician to investigate for any early recurrence, indicating that the clinical feasibility of 18F-FDG PET is relatively high despite of the high false-positive rate. Although the positive predictive value is relatively low, the high negative predictive value of 18F-FDG PET in this study suggests that the clinical feasibility of 18F-FDG PET is a method to assure the patients who are anxious about a possible recurrence.
All patients in this study showed no evidence of disease on conventional methods after treatment and were monitored by the standard protocol. However, because all patients with no evidence of disease were not investigated by 18F-FDG PET, we could not exclude completely a selection bias. Despite a possible selection bias, because the patient characteristics and recurrence rate did not differ significantly from the historical data, we believe that the selection bias may not be significant (2). A further prospective study is needed.
For further evaluation of the clinical feasibility, the cost-effectiveness of 18F-FDG PET should be evaluated. The high negative predictive value in this study suggests that the indication for 18F-FDG PET should be given thoughtful consideration after proper evaluation of the cost-effectiveness. Even though we did not elucidate the cost-effectiveness of 18F-FDG PET, we suggest that evaluation for recurrence with 18F-FDG PET is beneficial in patients with risk factors for recurrence. Further investigation is necessary for the proper indication and cost-effectiveness of 18F-FDG PET in patients with cervical cancer.
CONCLUSION
In this study, we showed that 18F-FDG PET was a useful method to detect early recurrence in cervical cancer; however, we did not evaluate the cost–benefit effect or, more importantly, the survival impact of 18F-FDG PET on the treatment of cervical cancer. Nevertheless, we suggest that 18F-FDG PET at least 1 y after treatment in advanced stages might be useful to detect early recurrence in patients with cervical cancer, even if they showed no evidence of disease after therapy.
Footnotes
Received May 20, 2002; revision accepted Sep. 27, 2002.
For correspondence or reprints contact: Sang-Young Ryu, MD, Department of Obstetrics & Gynecology, Korea Cancer Center Hospital, 215-4, Kongneung-dong, Nowon-ku, Seoul, Korea.
E-mail: ryu{at}kcch.re.kr
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- PET/CT scan improves detection of metastatic disease compared with CT scan alone in women with high-grade neuroendocrine cervical cancer: a NeCTuR study
- Esophageal Stenosis: A Differential Diagnosis Between Esophageal Cancer and Metastasis from Other Neoplasia
- Clarifying the Diagnosis of Clinically Suspected Recurrence of Cervical Cancer: Impact of 18F-FDG PET
- PET in Cervical Cancer -- Implications for `Staging,' Treatment Planning, Assessment of Prognosis, and Prediction of Response
- Expanding Role of Positron Emission Tomography in Cancer of the Uterine Cervix
- Utilization of Diagnostic Studies in the Pretreatment Evaluation of Invasive Cervical Cancer in the United States: Results of Intergroup Protocol ACRIN 6651/GOG 183
- Progress and Promise of FDG-PET Imaging for Cancer Patient Management and Oncologic Drug Development
- 18F-FDG PET Imaging in Posttherapy Monitoring of Cervical Cancers: From Diagnosis to Prognosis
- Defining the Priority of Using 18F-FDG PET for Recurrent Cervical Cancer
- Posttherapy [18F] Fluorodeoxyglucose Positron Emission Tomography in Carcinoma of the Cervix: Response and Outcome