


Abstract
Many studies have demonstrated that reduced left ventricular (LV) diastolic distensibility plays a key role in the pathophysiology of hypertrophic cardiomyopathy (HCM). However, the relationship between myocardial ischemia and reduced LV distensibility in HCM remains unclear. We aimed to clarify the relationship between exercise-induced ischemia and reduced LV distensibility in patients with HCM. Methods: Twenty patients with HCM and 5 age-matched control subjects underwent stress-redistribution 201Tl myocardial scintigraphy and biventricular cardiac catheterization and echocardiography at rest and during exercise. Scintigraphic defect analysis was interpreted using Berman’s 20-segment model. The summed stress score (SSS) was calculated as the sum of scores of the 20 LV segments and the summed difference score (SDS) was calculated as the sum of differences between each of the 20 LV segments on stress and rest images. Results: Patients were divided into 2 groups according to the 201Tl defect as follows: 9 patients with an SSS on 201Tl of ≥10 and an SDS on 201Tl of ≥5 (ischemic group) and 11 patients with an SSS of <10 or an SDS of <5 (nonischemic group). The absolute increases from rest to peak exercise in LV end-diastolic pressure (LVEDP) and pulmonary artery wedge pressure were significantly greater (15.5 ± 5.2 vs. 7.6 ± 5.5 mm Hg and 17.3 ± 5.0 vs. 8.9 ± 5.0 mm Hg, P < 0.01, respectively), and the percentage changes from rest to peak exercise in the maximum first derivative of LV pressure and LV pressure half-time were significantly smaller in the ischemic HCM group compared with the nonischemic HCM group (70% ± 24% vs. 123% ± 43% and −32% ± 6.4% vs. −44% ± 9.4%, P < 0.01, respectively). However, the end-diastolic dimensions did not differ between the 2 HCM groups. One of the 9 patients in the ischemic group, as revealed by fill-in on 201Tl scintigraphy, showed increased 18F-FDG uptake in the anteroseptal wall. Conclusion: Some HCM patients show a significant increase in LVEDP without chamber dilatation, indicating reduced LV diastolic distensibility. Myocardial ischemia may at least in part contribute to this condition.
Hypertrophic cardiomyopathy (HCM) is a cardiac disease with a variety of clinical and morphologic features. This disease is characterized by myocardial hypertrophy and hypercontractility with impaired diastolic function (1–3). Many studies have demonstrated that HCM shows reduced left ventricular (LV) diastolic distensibility, as characterized by a raised LV end-diastolic pressure (LVEDP) and limited ventricular filling (2,4–9).
Previous studies have shown that myocardial ischemia plays an important role in the pathophysiology and natural history of HCM, although patients with HCM angiographically have no significant coronary artery stenosis (10–15). This concept is supported by the occurrence of the symptoms of angina pectoris (15), of an abnormal lactate metabolism during pacing (16), and of a reduced coronary flow reserve (13,17).
Stress 201Tl myocardial scintigraphy is a noninvasive method to identify myocardial ischemia in various heart diseases. Previous studies reported that some HCM patients showed reversible perfusion abnormalities on exercise-redistribution 201Tl scintigraphy or that coronary vasodilators prevented myocardial ischemia in patients with HCM, indicating the presence of silent ischemia in HCM (8,11, 13,18). Abnormal findings on 201Tl may be related to microcirculation abnormalities caused by interstitial fibrosis, myocyte degeneration, or intramural coronary artery “small vessel” disease (10,19,20).
Two previous reports showed that some HCM patients exhibit an impairment in not only LV isovolumic contraction but also LV isovolumic relaxation from rest to peak exercise, suggesting that reduced LV distensibility seems to be more emphasized during exercise than at rest in such patients (21,22).
No study has been attempted to determine the relationship between myocardial ischemia and reduced LV distensibility during exercise, although many studies have mentioned reduced LV distensibility in HCM at rest. To our knowledge, this study is the first to compare the findings of stress-redistribution 201Tl myocardial scintigraphy with hemodynamic changes in response to exercise by biventricular cardiac catheterization and echocardiography at rest and during exercise. We clarified the relationship between exercise-induced ischemia and reduced LV distensibility in patients with nonobstructive HCM.
MATERIALS AND METHODS
Patient Population
Twenty patients (19 men, 1 woman; mean age; 51 ± 7 y; mean LV ejection fraction [LVEF], 71% ± 6%) with nonobstructive HCM were enrolled in this study. HCM was diagnosed on the basis of the clinical and electrocardiographic findings and on an echocardiographic demonstration of a hypertrophied LV in the absence of any other cardiac or systemic disease that itself might produce LV hypertrophy, in accordance with recently proposed diagnostic criteria (23,24). Patients were excluded if they had any of the following: prior evidence of myocardial infarction or coronary artery diseases with a significant stenosis of ≥50% in the major coronary artery on coronary angiography; primary valvular diseases; congestive heart failure; essential hypertension; and orthopedic problems that would preclude taking exercise tests. Asymmetric septal hypertrophy was considered to be present if the end-diastolic thickness of the LV septum was at least 13 mm and its ratio to the thickness of the LV posterior wall was >1.3. Nineteen patients showed asymmetric septal hypertrophy and 1 patient showed concentric hypertrophy without obstruction in the LV outflow on 2-dimensional (2D) echocardiography. All patients underwent stress-redistribution 201Tl myocardial scintigraphy, biventricular cardiac catheterization, and echocardiography at rest and during exercise. One of the HCM patients also underwent 18F-FDG PET under fasting. All examinations were performed within 1 wk of each other.
An age-matched control group of 5 healthy subjects (5 men; mean age, 57 ± 8 y; mean LVEF, 67% ± 5%) also underwent stress-redistribution 201Tl myocardial scintigraphy, biventricular cardiac catheterization, and echocardiography at rest and during exercise. All control subjects who had been hospitalized for suspected angina pectoris had low-risk profiles with normal cardiovascular examination results, including echocardiography, coronary angiography, and left ventriculography. No control subject was on drug treatment for cardiac disease or had a cardiac disease possibly affecting myocardial perfusion.
We explained the aim of this study to all patients and obtained their informed consent in writing.
Exercise 201Tl Myocardial Scintigraphy
All patients underwent stress-redistribution 201Tl myocardial scintigraphy after they fasted overnight. β-Blockers and calcium-channel blockers were withdrawn at least 24 h before testing. Exercise tests were performed while patients were seated on a bicycle ergometer at an initial workload of 25 W/min for 3 min under electrocardiographic monitoring. The workload was increased by 25 W every 3 min until symptom limited or achievement of at least 85% of the maximum predicted heart rate. 201Tl (111 MBq) was injected intravenously 1 min before the exercise was stopped. Stress imaging was initiated 10 min after exercise, and redistribution imaging was conducted 3 h later. 201Tl SPECT images were obtained with a rotating 2-head γ-camera (E.CAM; Toshiba Inc.) equipped with a low-energy, high-resolution, parallel-hole collimator. Images were collected over a 180° arc from 45° left posterior oblique to 45° right anterior oblique with an acquisition time of 30 s per image at 6° intervals. Energy discrimination was provided by a 20% window centered at 70 keV, and SPECT images were transferred to a computer using a 64 × 64 matrix size. Projection images were processed using a Butterworth filter with a cutoff frequency of 0.32 cycle per pixel and an order of 8. No attenuation or scatter correction was applied. Tomographic slices (6-mm thick) were reconstructed relative to the anatomic axis of the left ventricle, and then vertical long-axis, horizontal long-axis, and short-axis slices were generated.
Simultaneous Echocardiography and Biventricular Cardiac Catheterization
Biventricular catheterization was performed using a brachial approach in fasting patients. A 20-gauge catheter was placed in the left brachial artery to measure arterial pressure. A 6-French sheath was placed in the right brachial artery, and an externally balanced and calibrated 6-French pigtail angiographic micromanometer-tipped catheter (model SPC-464D; Millar Instruments) was positioned in the LV cavity through the sheath to measure LV pressure. The signal from the micromanometer was adjusted to match that of the catheter. A 7-French triple-lumen Swan-Ganz thermodilution catheter (Baxter Healthcare) was positioned in the right pulmonary artery through the right brachial vein to measure pulmonary artery wedge pressure (PAWP) and cardiac index (CI). All parameters were recorded at rest and during exercise.
Echocardiography was performed with a Hewlett-Packard Sonos 2500 ultrasound system equipped with a 2.5-MHz transducer at rest and during exercise.
After baseline data were obtained, patients underwent a symptom-limited supine bicycle ergometer exercise test, and the initial and maximum workloads were similar to those of the stress scintigraphic study.
Analysis of 201Tl Scintigraphy
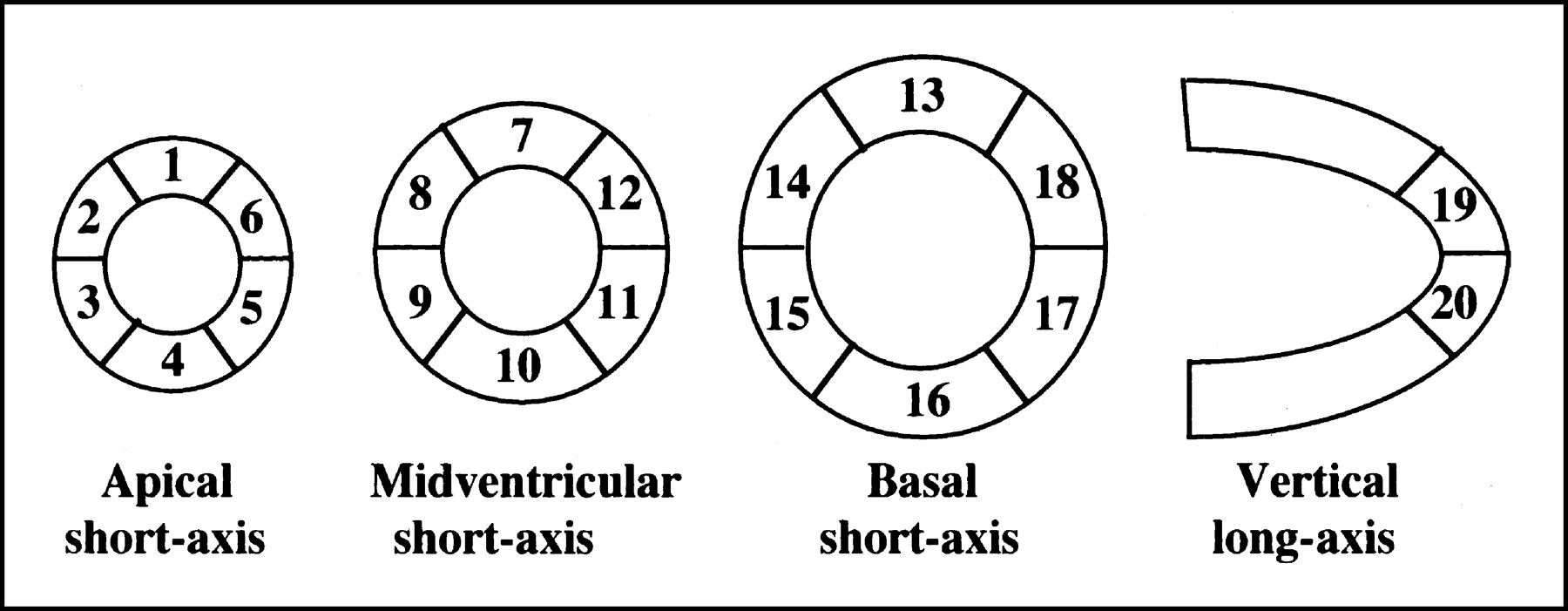
201Tl SPECT images were analyzed by 3 independent observers who were unaware of the clinical, hemodynamic, and echocardiographic data. Discrepancies were resolved by consensus. Perfusion was semiquantitatively assessed based on apical, middle, and basal short-axis and vertical long-axis tomograms. The LV myocardium was divided into 20 segments (18 on short-axis slices and 2 on vertical long-axis slices) as Berman et al. previously described (25) (Fig. 1). The defect score was visually defined using a 5-point scale (0 = normal tracer uptake, 1 = equivocal, 2 = mildly reduced, 3 = severely reduced, 4 = absent). The summed stress score (SSS) and summed rest score (SRS) were calculated as the summation of scores of the 20 segments in the stress (early) and rest (delayed) images. The summation of differences between each of the 20 segments on stress and rest images was defined as the summed difference score (SDS), representing ischemia. A normal perfusion scan was defined by an SSS of <4 (25,26).

Schema of LV 20-segment model as described by Berman et al (25). We defined 7 myocardial segments as follows: segment numbers 1, 7, and 13 as anterior wall; segment numbers 2, 8, and 14 as anteroseptal wall; segment numbers 3, 9, and 15 as inferoseptal wall; segment numbers 4, 10, and 16 as inferior wall; segment numbers 5, 11, and 17 as posterolateral wall; segment numbers 6, 12, and 18 as anterolateral wall; and segment numbers 19 and 20 as apical wall.
A reversible defect on 201Tl was considered present when the segmental score on delayed images improved by ≥1 point compared with early images. A fixed defect was defined as the same defect score between early and delayed images. To evaluate the location of myocardial 201Tl defects, we divided the myocardium into 7 segments as follows: anterior (segment numbers 1, 7, 13), anteroseptal (segment numbers 2, 8, 14), inferoseptal (segment numbers 3, 9, 15), inferior (segment numbers 4, 10, 16), posterolateral (segment numbers 5, 11, 17), anterolateral (segment numbers 6, 12, 18), and apical (segment numbers 19, 20) (Fig. 1).
LV Functional Analyses
In a hemodynamic study, LV pressure signals were digitized at 3-ms intervals and analyzed with software developed in our laboratory using a 32-bit microcomputer system (PC-9821-ST-20; NEC Corp.). Hemodynamic data were analyzed by 2 independent observers who were unaware of the clinical, echocardiographic, and scintigraphic data. LVEDP, the maximum first derivative of LV pressure (LV dP/dtmax) as an index of contractility, and LV pressure half-time (T1/2) to evaluate LV isovolumic relaxation were measured at baseline and peak exercise as previously described (21). In right heart catheterization, PAWP and CI were also measured. In 2D echocardiography, data were analyzed by 2 independent observers who were unaware of the clinical, hemodynamic, and scintigraphic data. LV end-diastolic dimension (LVEDD), LV end-systolic dimension (LVESD), interventricular septal thickness (IVST), posterior wall thickness (PWT), and LVEF were measured on the M-mode of the long-axis image according to standard criteria (27).
18F-FDG PET
The PET study was performed using a PET scanner (HEADTOME IV; Shimadzu Inc.) after one of the HCM patients fasted overnight. The scanner has 7 imaging planes; in-plane resolution is 4.5 mm at full width at half maximum (FWHM) and the z-axial resolution is 9.5 mm at FWHM. Effective in-plane resolution was 8 mm after using a smoothing filter. The sensitivity of the HEADTOME IV scanner is 14- and 24-kilocounts per second for direct and cross planes, respectively. Before obtaining emission images using PET, a transmission scan was obtained using a 68Ga ring source to correct for photon attenuation. Ten minutes after injection of 18F-FDG (285 MBq), dynamic data acquisition was performed for 1 h. Five regions of interest (5 × 5 pixels) were defined within the basal septum, apical septum, and anteroapical, apical lateral, and basal lateral walls in the transaxial slice. Patlak graphical analysis was used to calculate the regional metabolic rate of glucose (28).
Statistical Analysis
Values are expressed as the mean ± SD. A comparison between the 2 groups was done by unpaired t test and among the 3 groups by ANOVA. Comparison of proportion was done by χ2 analysis. A threshold value for ischemia on 201Tl SPECT was defined using receiver-operating-characteristic (ROC) analysis. P values < 0.05 were considered statistically significant.
RESULTS
No complication occurred during either exercise study. In the HCM patients, 400 myocardial segments were analyzed, among which fixed and reversible defects on 201Tl were shown in 71 segments (18%) and 14 segments (4%), respectively. Sixteen patients with HCM showed scintigraphic abnormalities (fixed or reversible defect) in the inferoseptal wall, 13 patients in the anteroseptal wall, 6 patients in the inferior wall, 6 patients in the posterolateral wall, and 4 patients in the apical wall. No control subjects showed significant scintigraphic abnormalities. IVST, left atrium dimension, and LVEDP were significantly greater, and T1/2 was significantly longer in the HCM patients compared with the control subjects. However, no significant differences in age, PWT, LVEDD, LVESD, LVEF, CI, PAWP, or maximum workloads were observed between the control subjects and the HCM patients. Baseline characteristics in the control group and HCM patients are listed in Table 1.
Comparison of Baseline Characteristics Between Control Subjects and HCM Patients
In a recent study, Takeichi et al. (22) suggested that the HCM patients showing a progressive increase to a maximum value in LVEDP had a stronger ischemic burden than those showing a biphasic pattern of LVEDP. At the threshold value of an SSS on 201Tl of ≥10 and an SDS on 201Tl of ≥5 using ROC analysis, we obtained the highest accuracy for detecting those patients showing a progressive increase in LVEDP. Accordingly, when patients with HCM showed an SSS on 201Tl of ≥10 and an SDS on 201Tl of ≥5, we defined them as HCM patients with ischemia. Therefore, our HCM patients were divided into 2 groups according to the 201Tl scintigraphic defect as follows: ischemic group (9 patients), an SSS on 201Tl of ≥10 and an SDS on 201Tl of ≥5; and nonischemic group (11 patients), an SSS of <10 or an SDS of <5.
Comparison of Maximum Workloads and Rate-Pressure Products at Peak Exercise
The maximum workloads did not differ significantly between scintigraphic and hemodynamic studies in any group (scintigraphic study: control, 87 ± 24 W; ischemic group, 79 ± 34 W; nonischemic group, 86 ± 34 W; and hemodynamic study: control, 77 ± 29 W; ischemic group, 75 ± 34 W; nonischemic group, 80 ± 28 W; P = not significant). The rate-pressure products at peak exercise did not differ significantly between the 2 studies in any group (scintigraphic study: control, 25,139 ± 1,994 mm Hg·bpm; ischemic group, 24,555 ± 2,164 mm Hg·bpm; nonischemic group, 24,335 ± 2,394 mm Hg·bpm; P = not significant; and hemodynamic study: control, 23,139 ± 2,274 mm Hg ·bpm; ischemic group, 24,009 ± 2,576 mm Hg·bpm; nonischemic group, 23,959 ± 2,458 mm Hg·bpm; P = not significant). The percentage changes in heart rate and rate-pressure product did not differ significantly between the scintigraphic and hemodynamic studies in any group.
Comparison of Parameters Among Control Subjects and HCM Patients With and Without Ischemia
In scintigraphic findings, SSS, SDS, and SRS were significantly greater in the ischemic and nonischemic HCM groups compared with the control subjects. SSS and SDS were significantly greater in the ischemic group compared with the nonischemic group (14.7 ± 2.1 vs. 6.9 ± 3.1, P < 0.0001; 9.0 ± 3.0 vs. 2.2 ± 1.8, P < 0.001). However, SRS did not differ significantly between the ischemic and nonischemic HCM groups (5.3 ± 3.4 vs. 2.9 ± 2.7, P = not significant).
In the echocardiographic study, IVST was significantly greater in the ischemic and nonischemic HCM groups compared with the control subjects. PWT was significantly greater in the ischemic group compared with the control subjects. However, neither other echocardiographic parameters at both rest and peak exercise nor absolute changes in LVEDD, LVESD, and LVEF differed significantly in any group. In particular, the absolute change in LVEDD did not differ significantly between the 2 HCM groups (Table 2).
Comparison of Echocardiographic Parameters Among 3 Groups
In the hemodynamic study, the LVEDP at rest was significantly higher in the ischemic and nonischemic HCM groups compared with the control subjects (13.1 ± 5.5 vs. 7.0 ± 4.0 mm Hg, P < 0.01; 12.0 ± 3.9 vs. 7.0 ± 4.0 mm Hg, P < 0.01). The T1/2 at rest was significantly longer in the ischemic and nonischemic HCM groups compared with the control subjects (41 ± 3.5 vs. 34 ± 4.0 ms, P < 0.05; 39 ± 5.1 vs. 34 ± 4.0 ms, P < 0.05). LV dP/dtmax, CI, and PAWP at rest did not differ significantly in any group. LVEDP and PAWP at peak exercise were significantly greater in the ischemic group compared with the nonischemic group and the control subjects (LVEDP: 29.5 ± 5.2 vs. 19.9 ± 6.2 mm Hg, P < 0.001; 29.5 ± 5.2 vs. 15.0 ± 5.1 mm Hg, P < 0.0001; PAWP: 25.3 ± 7.2 vs. 16.9 ± 6.1 mm Hg, P < 0.05; 25.3 ± 7.2 vs. 16.0 ± 4.1 mm Hg, P < 0.05). LV dP/dtmax at peak exercise was significantly smaller in the ischemic group compared with the nonischemic group (3,255 ± 610 vs. 4,664 ± 1,348 mm Hg/s, P < 0.01). T1/2 and CI at peak exercise did not differ significantly in any group (Table 3).
Comparison of Hemodynamic Parameters Derived from Cardiac Catheterization Among 3 Groups
In evaluating the changes in each parameter from rest to exercise, the absolute increases in LVEDP and PAWP were significantly greater in the ischemic group than in the nonischemic group and the control subjects (LVEDP: 15.5 ± 5.2 vs. 7.6 ± 5.5 mm Hg, P < 0.005; 15.5 ± 5.2 vs. 8.0 ± 4.1 mm Hg, P < 0.005; PAWP: 17.3 ± 5.0 vs. 8.9 ± 5.0 mm Hg, P < 0.01; 17.3 ± 5.0 vs. 10.0 ± 2.9 mm Hg, P < 0.05), and the percentage change in LV dP/dtmax was significantly smaller in the ischemic group than in the nonischemic group (70% ± 24% vs. 123% ± 43%, P < 0.005). The percentage change in T1/2 was also significantly smaller in the ischemic group than in the nonischemic group (−32% ± 6.4% vs. −44% ± 9.4%, P < 0.01) (Table 3).
Case Presentation
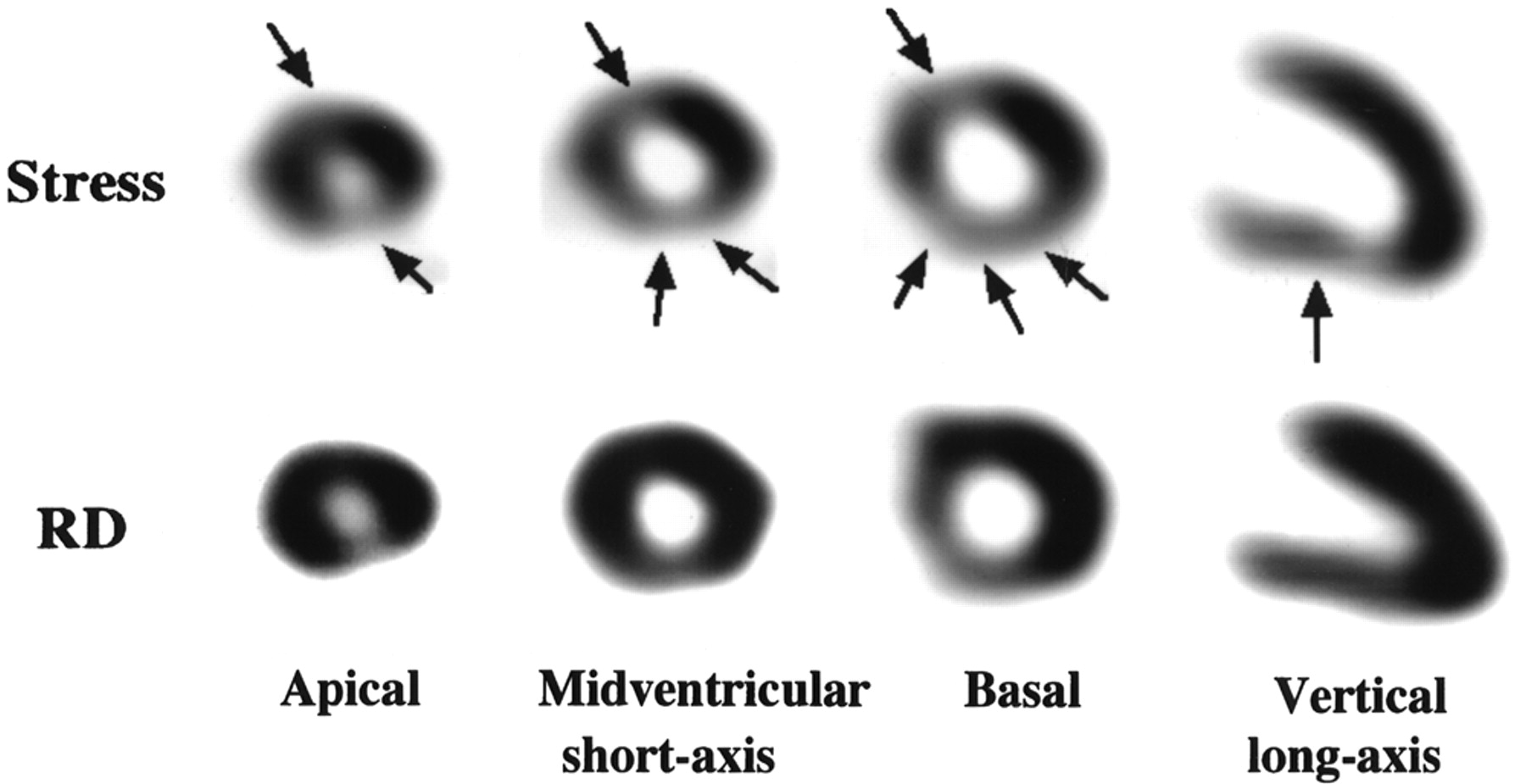
A typical patient who showed redistribution on 201Tl in the anteroseptal, inferoseptal, inferior, and posterolateral walls is presented in Figure 2.
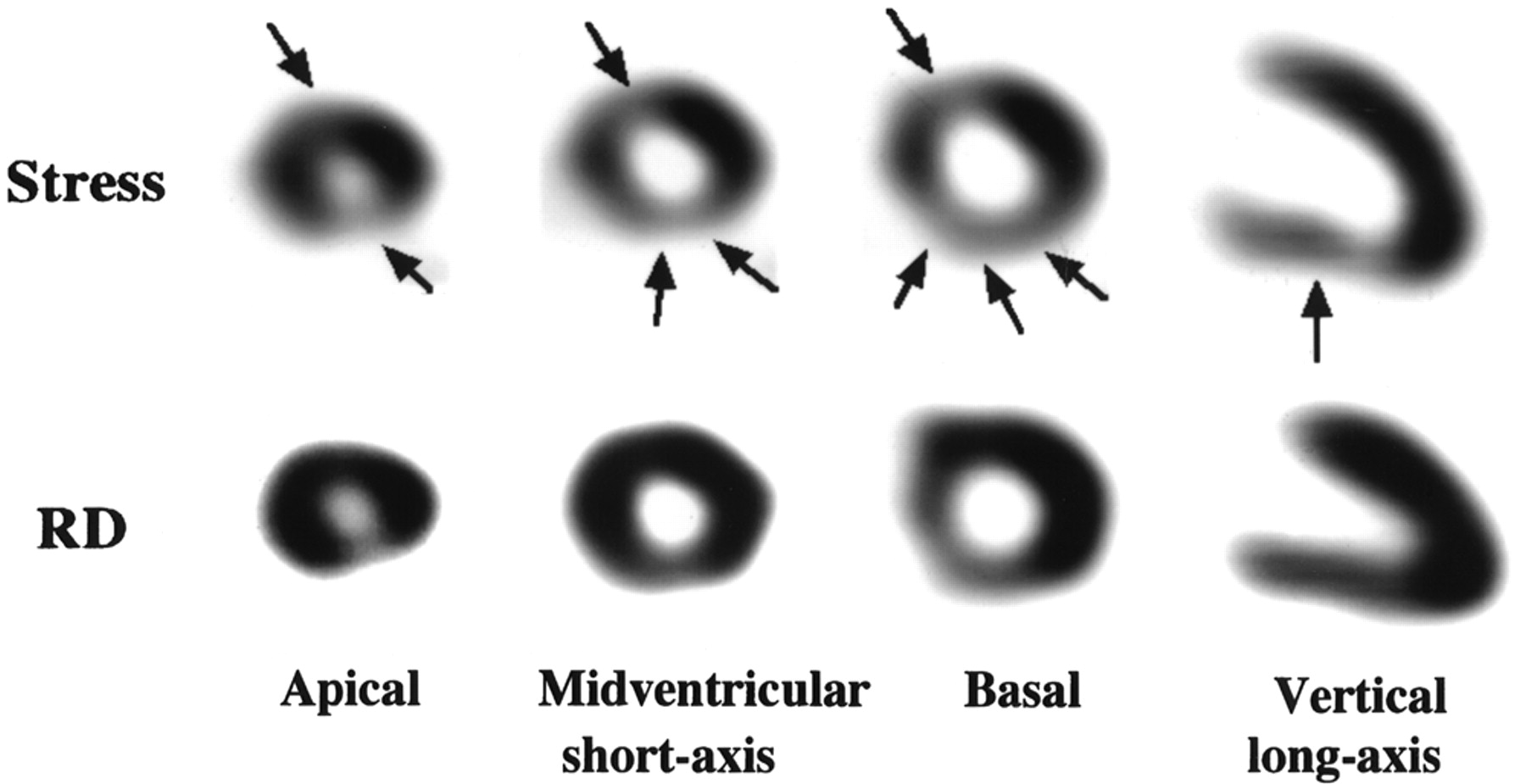
Stress-redistribution 201Tl SPECT of 45-y-old man from ischemic group. Redistribution (RD) was observed in anteroseptal, inferoseptal, inferior, and posterolateral walls on short-axis and vertical long-axis images (arrows).
18F-FDG PET was performed in 1 of the 9 patients from the ischemic group (Fig. 3). In a visual comparison of 201Tl with 18F-FDG, preserved 18F-FDG uptake on the transaxial image with redistribution on the horizontal long-axis image of 201Tl was observed in the anteroseptal wall. In quantitative Patlak graphical analysis, regional 18F-FDG uptake in the septal wall was increased more than that in the lateral wall (1.17 vs. 0.65 μmol/min/g), suggesting the presence of myocardial ischemia in the septal wall.
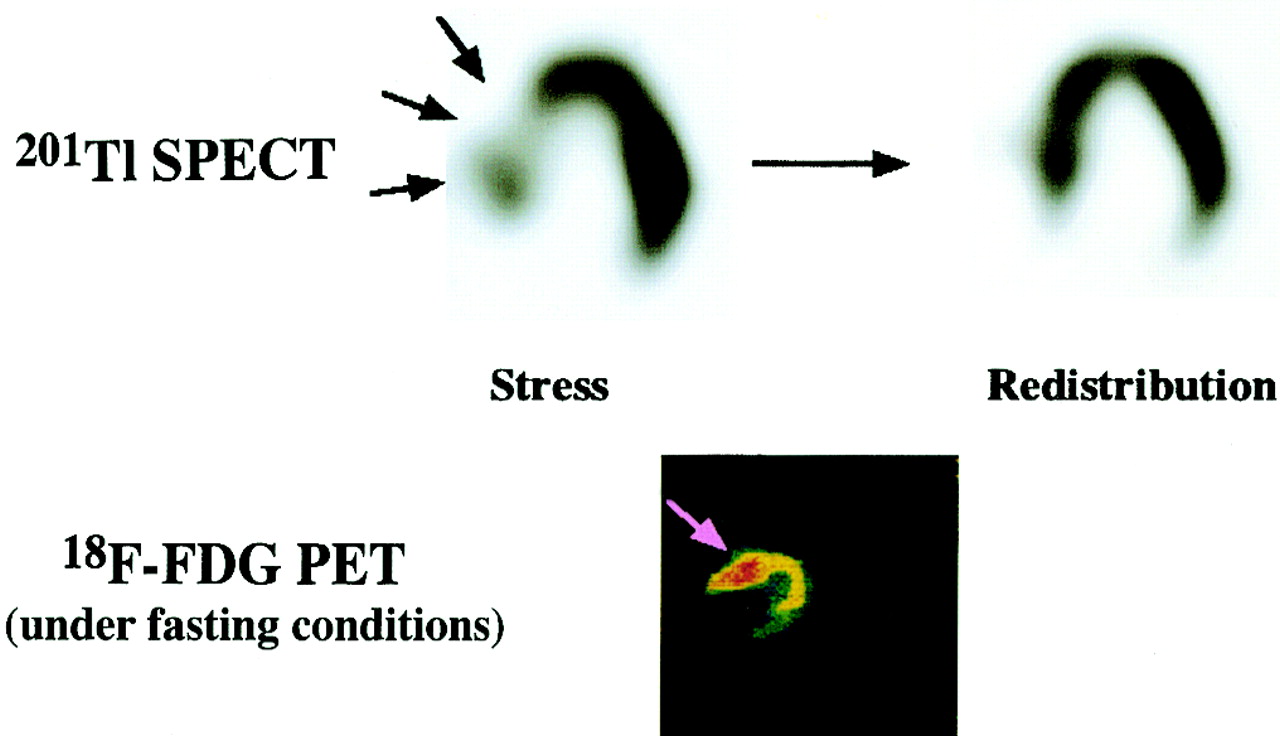
Stress-redistribution 201Tl SPECT and 18F-FDG PET in 1 ischemic group patient. Anteroseptal wall with redistribution on 201Tl SPECT (black arrows) showed increased uptake on 18F-FDG PET (pink arrow).
DISCUSSION
Some HCM patients showed ischemic change during exercise as revealed by stress-redistribution 201Tl myocardial perfusion scintigraphy. An LV preload, as shown by LVEDP and PAWP during exercise, was significantly greater in the ischemic group than in the nonischemic group. An acceleration of contractility (LV dP/dtmax) and a shortening of relaxation (T1/2) by exercise were more depressed in the ischemic group than in the nonischemic group. However, changes in LV cavity size from rest to peak exercise did not differ significantly between the 2 HCM groups. These results suggested that HCM patients with ischemia show abnormalities in hemodynamic changes during exercise without chamber dilatation, indicating that reduced LV diastolic distensibility may be enhanced by myocardial ischemia. We elucidated the relationship between a progressive impairment of LV diastolic distensibility during exercise and exercise-induced myocardial ischemia in patients with HCM.
This study showed that HCM patients with exercise-induced ischemia exhibited a more impaired response to relaxation during exercise than those without ischemia. In addition, patients with ischemia showed a larger absolute change in LVEDP from rest to peak exercise than those without it. In general, HCM is characterized by an impaired LV diastolic function, although LV systolic function demonstrates normal or supernormal values. In particular, the demonstration of elevated LVEDP in patients with HCM, despite a normal or reduced end-diastolic volume, suggests that an impaired LV diastolic function may contribute to the clinical manifestations of this disease. Such an impairment has been identified by the abnormal diastolic filling, abnormal relaxation, and reduced LV diastolic distensibility (29–33). Several studies presented evidence of reduced LV diastolic distensibility in patients with HCM even at rest (2,4–9). Our findings, in which LVEDP was shown to be higher and a shortening of relaxation was more prolonged in patients with HCM compared with healthy subjects (despite a similar LV dimension between HCM patients and healthy subjects), may indicate the presence of reduced LV diastolic distensibility at rest in HCM. Two recent invasive studies demonstrated that some HCM patients showed a progressive impairment in isovolumic relaxation during that time, probably indicating the progressive impairment of LV distensibility during exercise (21,22). In our study, some HCM patients with ischemia on 201Tl SPECT while exercising showed a significant increase in LVEDP without significant chamber enlargement, indicating the progressive impairment of LV diastolic distensibility caused by myocardial ischemia during exercise. With respect to the possible mechanisms by which myocardial ischemia during exercise induces reduced LV diastolic distensibility, a previous study indicated that it induces the Ca2+ overload and Ca2+ deposition caused by impaired Ca2+ sequestration by the sarcoplasmic reticulum (21). The Ca2+ overload then leads to the impairment of relaxation, resulting in reduced LV diastolic distensibility. On the other hand, patients with ischemia also showed an impaired LV systolic performance when exercising, as shown by a decrease in the percentage change in LV dP/dtmax from rest to peak exercise despite an increased LV preload, probably resulting from decreased myocardial contractility caused by exercise-induced ischemia.
In our study, some HCM patients showed reversible perfusion abnormalities on stress-redistribution 201Tl SPECT, which was in agreement with the results of previous studies (11–14). The causative mechanisms of myocardial ischemia in HCM have been demonstrated to be an intramural flow reduction because of structural abnormalities in intramural small coronary arteries caused by hyperplasia, medial hypertrophy or distribution of fibrosis, and hypertrophied tissue formation in the LV myocardium (10,19, 20); limitation of coronary flow reserve caused by an increased diastolic filling pressure due to myocardial hypertrophy or asynchrony of LV motion (10,13); and impaired coronary vasodilator response despite increased myocardial oxygen demand during exercise (13, 34). These histologic and hemodynamic abnormalities could potentially induce an inadequacy of myocardial blood flow even though myocardial oxygen demand increases during exercise, resulting in exercise-induced myocardial ischemia. One of the 9 patients in the ischemic group who underwent 18F-FDG PET in addition to 201Tl SPECT showed an increased 18F-FDG accumulation in the septal wall. This finding indicates that myocardial ischemia plays a key role in the pathophysiology of HCM. The PET finding may strongly support the presence of silent myocardial ischemia even at rest and, subsequently, the redistribution phenomenon on the exercise 201Tl study indicated that this ischemia was promoted by exercise. In addition, this PET finding may indicate that reduced LV distensibility induces the impairment of the myocardial energy metabolism.
In this study, perfusion abnormalities on 201Tl SPECT were often observed in the anteroseptal and inferoseptal walls. Previous studies demonstrated that perfusion or metabolic abnormalities on scintigraphy appeared to be in the area of junction, which often extended to the adjacent portion of the ventricular septum and LV free wall (35,36). Histologically, such areas are characterized by the presence of marked fascicular disarray, tissue clefts, and massive fibrosis, with fiber disarray extending to the adjacent portions of the septum and free walls (37). Therefore, scintigraphic abnormalities may be associated with the histologic abnormalities. Our result showing that 201Tl abnormalities were often observed in the area of junction was in agreement with the results of those previous studies. Because abnormal hemodynamic adaptations to exercise were related to the scintigraphic abnormalities as shown by our results, the contractility and relaxation responses to exercise may be affected by the extent or severity of the histologic abnormalities.
It is well known that sudden death occurs during physical exercise in some patients with HCM. Previous studies documented that the risk of sudden cardiac death is significantly higher in patients with HCM who show positive results on an exercise test (38), exercise-induced abnormality in the response of blood pressure (39), and a small increase in systolic blood pressure during exercise (40). Therefore, abnormal cardiac performance during exercise may play an important role in sudden cardiac death. In this study, the degree of impairment of both an exercise-induced acceleration in contractility and a shortening of relaxation by exercise was significantly greater in HCM patients with ischemia than in those without it. The positive results on the exercise test or hemodynamic maladaptations to exercise of patients with HCM seem to be related to sudden death, as shown by previous studies (38–40). Moreover, Dilsizian et al. (12) demonstrated that myocardial ischemia is a major risk factor for sudden cardiac death. Therefore, our result may indicate not only the degree of such severity in HCM but also one of the potential mechanisms of sudden cardiac death in those patients. Abnormalities on stress-redistribution 201Tl myocardial scintigraphy were related to abnormal hemodynamic adaptations to exercise in our results, probably affecting the clinical outcome of HCM patients. Systolic dysfunction caused by exercise-induced ischemia may be one of the potential mechanisms of sudden death. Reduced LV diastolic distensibility, as shown by abnormal diastolic performance by exercise-induced ischemia, may also trigger acute pulmonary edema or ventricular arrhythmias, leading to sudden death during exercise. However, these relations warrant further studies that include an evaluation of the long-term follow-up of patients.
Our analysis of regional perfusion defects based solely on a visual scoring of the SPECT images is a potential limitation of this study. Partial-volume effects, related to physical imaging characteristics in the acquisition of SPECT imaging when the ventricular walls vary in thickness in those same patients, may result in reduced counts in thinner myocardial areas compared with more hypertrophied areas. Despite a visual assessment of 201Tl SPECT, there was a significant concordance between the magnitude of perfusion abnormalities and abnormal hemodynamic adaptations to exercise. The impact on our hemodynamic data of progressive mitral regurgitation from rest to peak exercise or chance occurrence during exercise cannot be excluded. However, our patients showed mild mitral regurgitation at rest, even if it presented. Moreover, no patient showed a significant progression or chance occurrence during exercise. Therefore, we believe that the impact of mitral regurgitation on our data is insignificant.
CONCLUSION
Some HCM patients show a significant increase in LVEDP without chamber dilatation during exercise, representing reduced LV diastolic distensibility. Myocardial ischemia may contribute to this condition. The progressive impairment of LV distensibility due to myocardial ischemia may be related to sudden death during exercise in patients with HCM. However, this relation warrants further studies, including prognostic evaluations.
Acknowledgments
We thank Shinji Abe, Kazuo Toyama, and Masatsugu Nishino, radiologist of Nagoya University Hospital, for their technical assistance in the PET and SPECT studies. We are also indebted to Kohzo Nagata, MD, PhD, Fiji Somura, MD, PhD, Taisei Kawamura, MD, Hisashi Umeda, MD, Akihiro Hirashiki, MD, and Akiko Noda, PhD, for their cooperation and to Norio Honda and Koji Obata for their valuable technical and statistical advice in the hemodynamic studies.
Footnotes
Received Mar. 14, 2003; revision accepted Jul. 10, 2003.
For correspondence or reprints contact: Satoshi Isobe, MD, PhD, Department of Cardiology, Nagoya University Graduate School of Medicine, 65 Tsurumai-cho, Showa-ku, Nagoya, Aichi 466-8550, Japan.
E-mail: sisobe{at}med.nagoya-u.ac.jp
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.