


Abstract
Much evidence suggests endothelial dysfunction to be present in non-insulin-dependent diabetes mellitus (NIDDM) and to be important for the development of myocardial ischemia. Endothelial function in the coronary vessels may be studied in various ways. We compared the effect of cold pressor testing (CPT) with that of dipyridamole, a pharmacologic vasodilator, on coronary blood flow (CBF) measured by PET in NIDDM patients and healthy volunteers. In addition, we studied the effect of acute angiotensin-converting enzyme (ACE) inhibition on the flow response. Methods: Ten NIDDM patients and 10 control subjects participated. Myocardial perfusion was determined at baseline, during CPT, and after dipyridamole infusion by PET using intravenous 13N-ammonia. Results: Resting CBF was similar in NIDDM patients and in control subjects. CPT increased CBF by 20% in the control group, whereas no increase was observed in the patients. After dipyridamole infusion, CBF increased 2- to 3-fold in patients and 3- to 4-fold in control subjects. The increase and maximal CBF were significantly higher in control subjects than in patients. During ACE-inhibitor infusion, which had no influence on resting CBF in patients or control subjects (n = 5), CPT increased CBF by 14% in the NIDDM group. After dipyridamole, CBF increased 3- to 4-fold in both groups. The increase in CBF and maximal CBF in the 2 groups were not different during ACE-inhibitor infusion. Conclusion: In these NIDDM patients without evidence of epicardial coronary disease, endothelial dysfunction is strongly suggested by an impaired increase in CBF both to dipyridamole and to CPT. This dysfunction was reversed by infusion of an ACE inhibitor. Although ACE inhibition during CPT did induce significant increases in CBF in the patients, the changes during ACE inhibition were small compared with the dipyridamole response, and the absence of CBF increase during CPT in 3 of the 10 control subjects further limits the value of CPT for the study of coronary endothelial dysfunction.
Evidence of endothelial dysfunction has frequently been found in diseases such as hypertension, hypercholesterolemia, and diabetes. The clinical importance of endothelial dysfunction in the development of coronary artery disease is probably related to impaired endothelium-dependent vasodilation in both coronary conductance and coronary resistance vessels. This impairment leads to an inadequate increase in coronary blood flow (CBF) in response to increased metabolic demand causing ischemia. Endothelial dysfunction may be demonstrated as a decreased vasodilatation response to an intracoronary infusion of acetylcholine and methacholine. The endothelium-dependent vasodilatation may also be demonstrated by intracoronary administration of an NO synthesis inhibitor, for example, NG-monomethyl-l-arginine (l-NMMA), that blocks endothelium-dependent vasodilatation, for example, flow-mediated coronary artery dilatation. In patients with non-insulin-dependent diabetes mellitus (NIDDM), endothelial dysfunction has been demonstrated using acetylcholine (1,2), methacholine (3,4), and l-NMMA (2).
A correlation between changes in blood flow during intravascular acetylcholine infusion and during cold pressor testing (CPT) (5) has supported the use of CPT as a noninvasive way to study coronary endothelial function with PET. The principle of CPT is nociception-induced activation of the sympathoadrenomedullary system. This, in turn, is supposed to lead to an increased oxygen demand of the myocardium and a secondary increased CBF in the normal heart, largely because of endothelium-dependent flow-mediated vasodilation. However, in patients with endothelial dysfunction, the loss of vasodilatory mechanisms leads to an absence of or insufficient increase in CBF. Dipyridamole is used as a pharmacologic stressor to measure maximal coronary flow, which is highly dependent on the function of the endothelium. The utility of PET in combination with pharmacologic stressors to measure flow reserve has previously been described (6,7).
To establish the clinical value of CPT in the evaluation of coronary endothelial function, we studied CBF by PET in NIDDM patients and in healthy volunteers during CPT and pharmacologic stress by dipyridamole both in a baseline situation and during angiotensin-converting enzyme (ACE) inhibition, which is known to improve endothelial dysfunction in peripheral vessels.
MATERIALS AND METHODS
Study Population
Ten patients with NIDDM and 10 healthy volunteers, as control subjects, were included. All patients were normoalbuminuric and normotensive, had normal cholesterol levels, and had normal results from exercise testing. They were recruited from the Steno Diabetes Center, Gentofte, Denmark, and the control group was recruited from the Naestved Population Study (Naestved, Denmark). The study was approved by the local scientific ethical committee, and all participants gave their written informed consent. Details on the study groups are shown in Table 1.
Epidemiology of Study Groups
General Protocol
Myocardial perfusion was determined by PET using intravenous 13N-ammonia as a tracer. For each subject, serial PET images were acquired at rest (baseline), during CPT, and after pharmacologic stress using dipyridamole. The whole series was performed twice: once during placebo infusion and once during infusion of the ACE inhibitor perindoprilat. The 2 studies were performed in random order within 2 wk. The PET studies were performed after an overnight fast. All participants refrained from intake of caffeine-containing food or beverages for at least 18 h before the PET study. Each subject lay supine in the PET scanner. A catheter was inserted in the antecubital vein of each arm for the infusion of tracer, dipyridamole, perindoprilat, or placebo (saline). CPT was performed by lowering the subject’s left foot and ankle into a tub filled with ice water. Thirty seconds later, 13N-ammonia was infused intravenously. The foot was kept for an additional 2 min in ice water to ensure that the stimulus lasted for the first 2 min of the dynamic image acquisition. Pharmacologic stress was induced by an intravenous dipyridamole infusion of 0.56 mg/kg over 4 min. Three minutes later, 13N-ammonia was infused. Perindoprilat, which in a pilot study had been “titrated” in 3 healthy volunteers to produce marked increases in the plasma concentrations of renin and angiotensin without causing hypotension, was infused as a bolus of 1.25 mg 15 min before the start of the scans, followed by a continuous infusion of 0.5 mg/h during the rest of the study. Heart rate, blood pressure, and electrocardiography findings were monitored throughout the study.
PET
Image Acquisition.
The study was performed on a whole-body tomograph (Advance; General Electric Medical Systems, Milwaukee, WI) with 18 crystal rings forming 35 two-dimensional imaging planes spaced by 4.25 mm, and an intrinsic spatial resolution of 4–6 mm in full width at half maximum. The gantry width has a diameter of 55 cm, and the axial field of view is 15.2 cm. Two pin sources with 68Ge were used for the blank and transmission scan acquisitions. Corrections for dead time, attenuation, scatter, and decay were applied, and the images were reconstructed to an effective in-plane resolution of 7 mm in full width at half maximum using a Hanning filter.
Initially, a 2-min transmission scan was acquired for optimal positioning, which was then checked during the study by a cross-shaped low-power laser beam and pen markers on the skin. Movement was minimized by fastening a hook-and-loop strap across the subject’s chest. The 3 image acquisitions, at rest, during CPT, and after dipyridamole, were performed in an identical matter separated by 50–60 min to allow for physical decay of 13N-ammonia activity. After a slow, intravenous bolus injection of 700 MBq 13N-ammonia over 30 s using an infusion pump (Harvard Apparatus, Inc., Holliston, MA), serial images were acquired for 20 min (24 frames: 13 × 6 s, 3 × 12 s, 3 × 20 s, 4 × 30 s, and 1 × 900 s).
Because patient discomfort during CPT and the long scanning protocol increased the risk of motion artifacts, the 3 dynamic image acquisitions were interpolated by 2 transmission scans to ensure optimal correction for motion artifacts. Immediately after the dynamic acquisition sequence, a 5-min correction frame was applied, based on the assumption that the distribution of 13N-ammonia activity remained constant for the remaining 20–45 min. The 5-min frame was used to correct the residual 13N-ammonia and background activity of the subsequent transmission scan. Transmission data were acquired for 20 min. The first set of transmission data was subsequently used to generate attenuation correction factors for the baseline study. The second set of transmission data was used to generate attenuation correction factors for CPT and the dipyridamole study.
Image Analysis.
For each frame of the serially acquired data, sets of 35 transaxial images were reconstructed. Each of these image datasets were resampled on a workstation (General Electric Medical Systems) into 12 contiguous short-axis cross-sections of the left ventricle.
For generation of time-activity curves, 6 serially acquired short-axis cross-sections (2 basal, 2 midventricular, and 2 apical) were selected for each subject, leaving out the 4 most apical and 2 most basal planes. Regions of interest (ROIs) were assigned to the last serial image (900 s) and copied to the first 16 serially acquired 13N-ammonia images (i.e., the initial 120 s of data after tracer injection) to obtain regional time-activity curves. Rectangular myocardial ROIs with an area of 64 mm2 were placed to correspond to the anterior, lateral, and inferior walls of the left ventricle using a standardized template. The junction of the anterior right ventricular wall with the anterior interventricular septum was used to ensure a standardized anatomic location for the template. The septal ROI was omitted in our analysis to reduce the error introduced by dual spillover. These time-activity curves from 3 corresponding sectors in 6 planes were then averaged. A circular ROI with an area of approximately 50 mm2 was situated over the center of the left ventricular blood pool to derive the arterial concentration curve used as an input function averaging the input time-activity curves from the 3 most basal planes. We corrected for partial-volume effects, with a recovery coefficient estimated from values obtained by echocardiographic measurement of the individual left ventricular free-wall thickness. The corrected time-activity curves were then fitted with a previously validated 2-compartment tracer kinetic model (8).
Statistical Evaluation
Differences within groups were tested by paired t tests, and differences between groups were tested by unpaired t tests. P < 0.05 was considered significant.
RESULTS
CBF
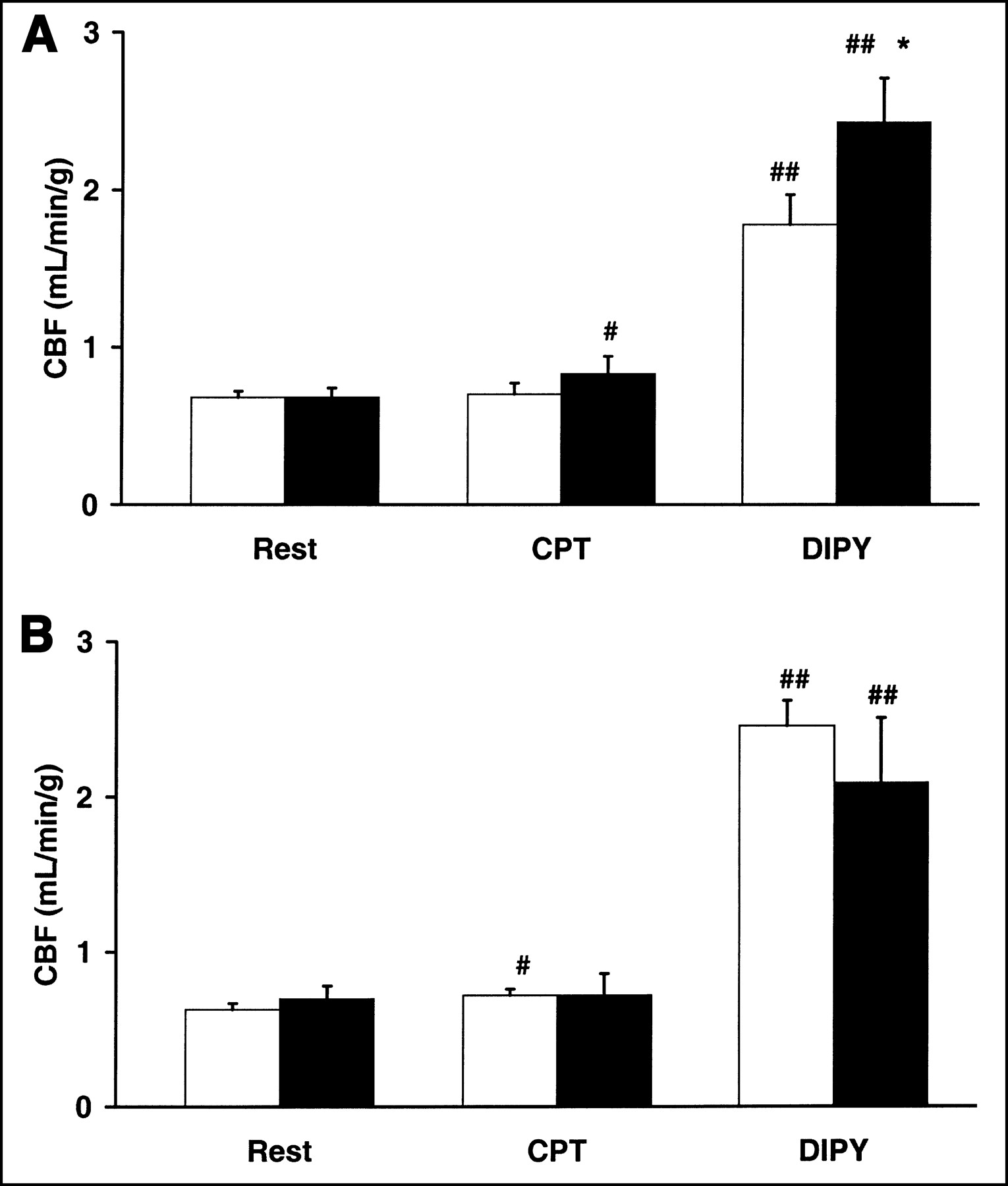
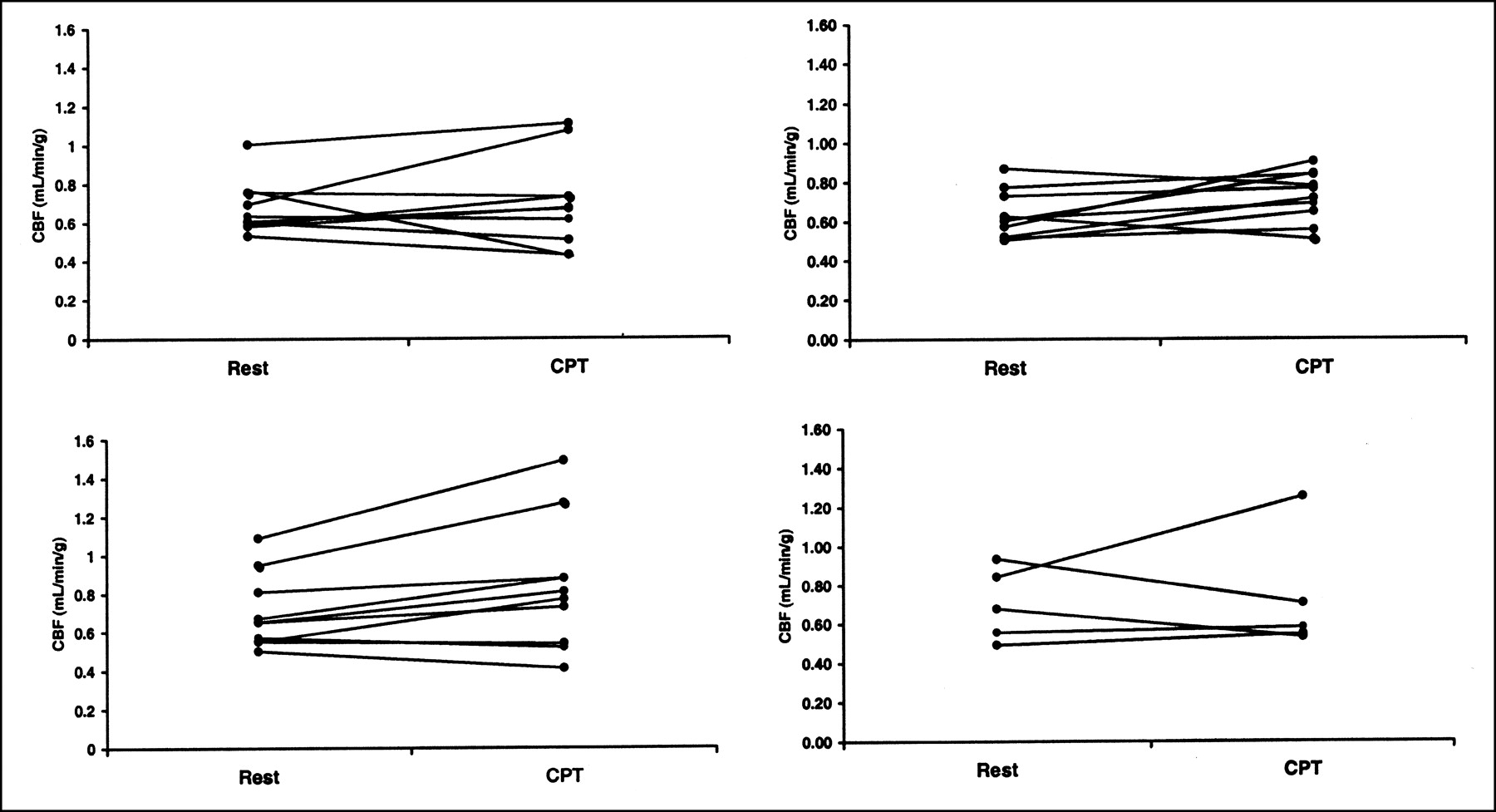
During placebo infusion, resting CBF was similar in NIDDM patients and control subjects (Fig. 1A). CPT increased CBF by 20% in the control group (P < 0.05), whereas no increase was observed in the NIDDM group. After dipyridamole infusion, CBF increased 2- to 3-fold in NIDDM patients (P < 0.01) and 3- to 4-fold in control subjects (P < 0.01). The increase and the maximal CBF were significantly higher in control subjects than in patients (P < 0.05). During ACE-inhibitor infusion, resting CBF was similar in NIDDM patients and control subjects (Fig. 1B). CPT increased CBF by 14% in the NIDDM group (P < 0.05), whereas no increase was observed in the 5 subjects of the control group who received perindoprilat. After dipyridamole infusion, CBF increased 3- to 4-fold in both groups (P < 0.01). The increase and maximal CBFs in the patients were statistically not different from those in the 5 control subjects receiving perindoprilat or from those in the 10 control subjects during saline infusion. The individual flow responses to CPT are shown in Figure 2.
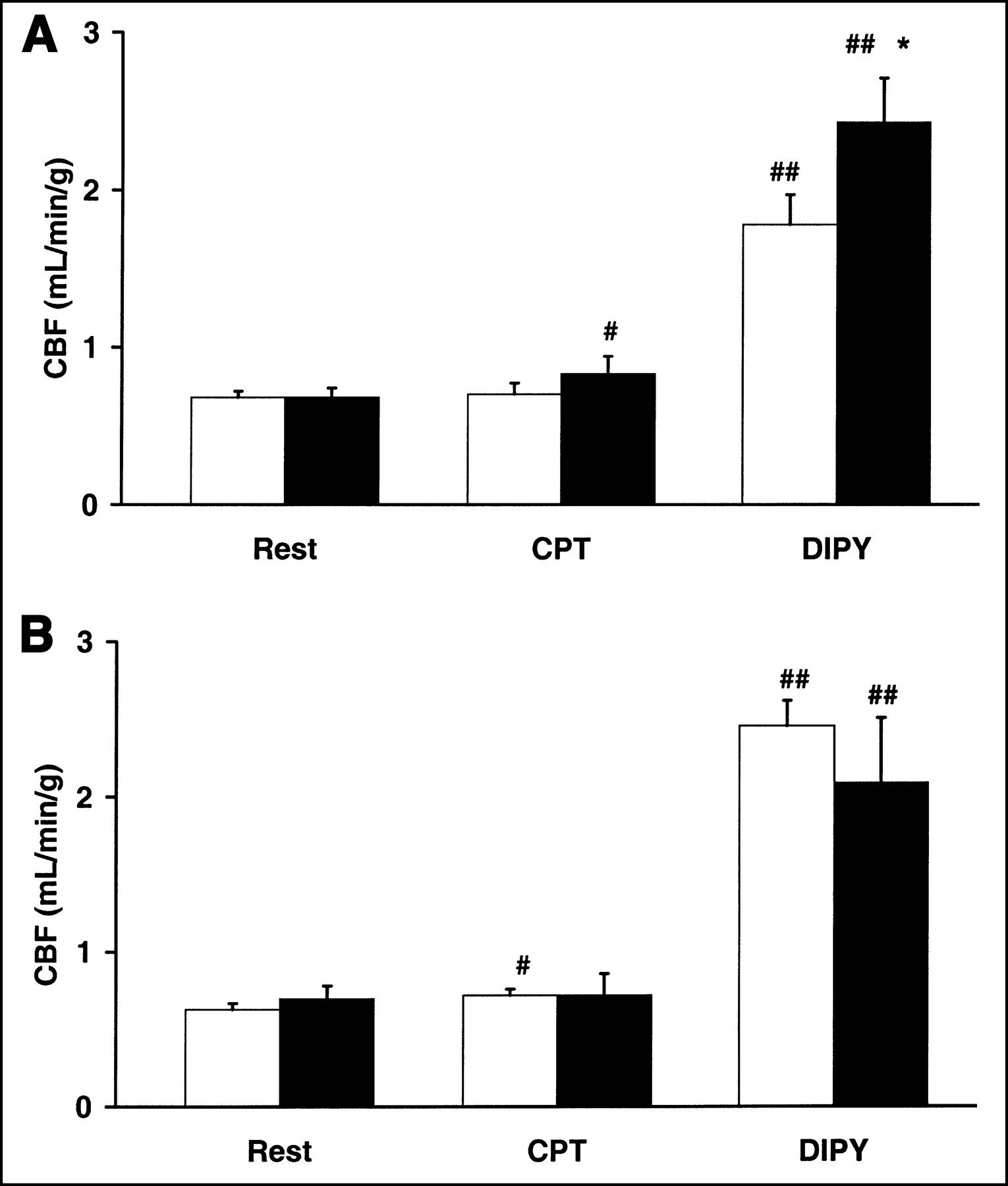
CBF values at rest, during CPT, and after dipyridamole (DIPY) during saline infusion (A) or perindoprilat (ACE inhibitor) infusion (B). Values are mean ± SEM for 10 subjects (5 for ACE inhibitor control subjects). *P < 0.05 vs. control subjects. #P < 0.05 vs. NIDDM patients. ##P < 0.01 vs. rest. White bars = NIDDM patients; black bars = control subjects.
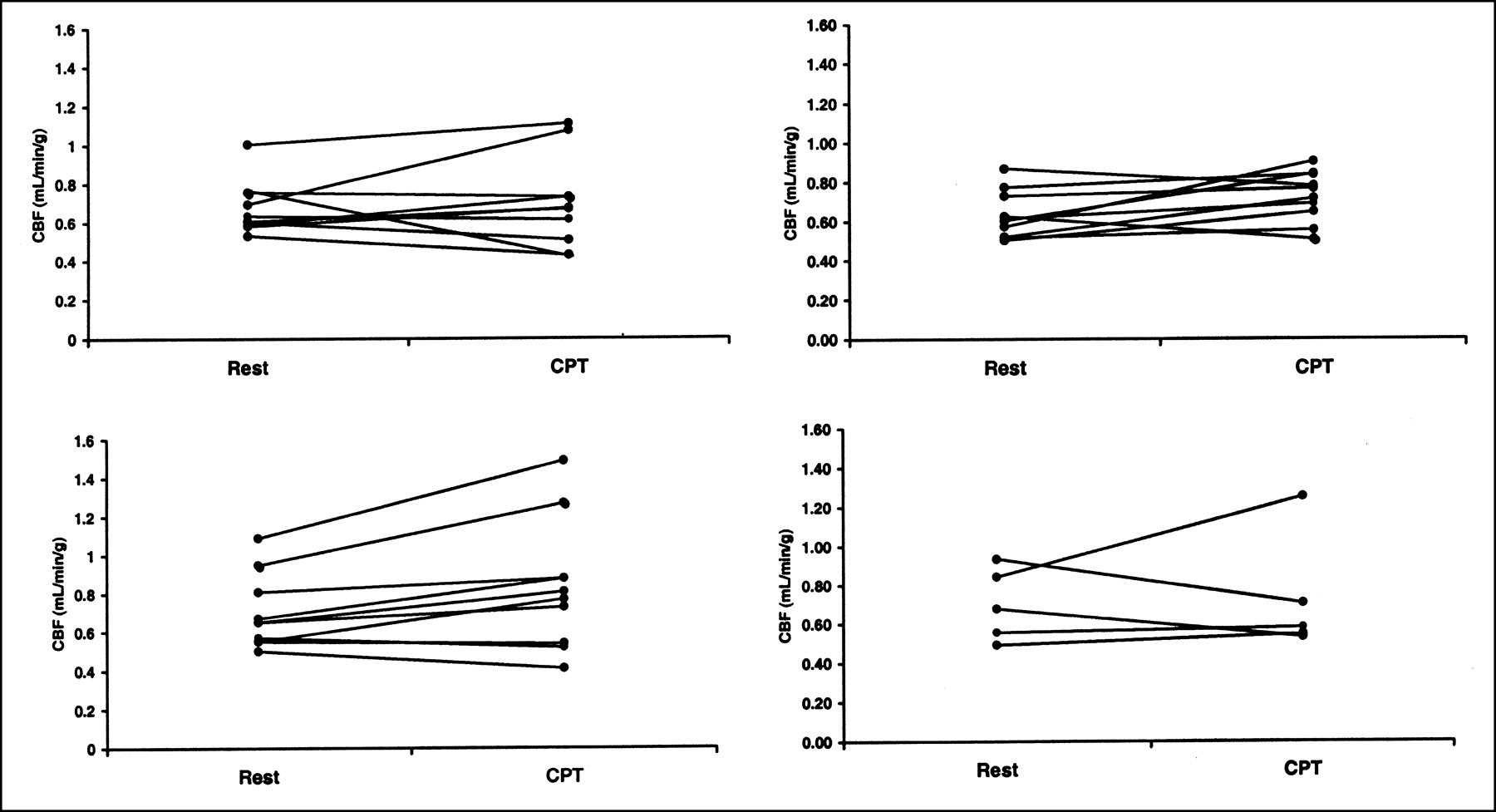
Individual CBF responses to CPT in saline-treated (left panels) or perindoprilat-treated (right panels) NIDDM patients (top panels) or control subjects (bottom panels).
Hemodynamics During CPT
CPT increased the rate-pressure product (RPP) approximately 30% in both the NIDDM group and the control group (Table 2; P < 0.01). Infusion of ACE inhibitor did not change the increase in RPP in response to CPT in any of the groups.
Hemodynamics During Rest and Cold Pressor Test Performed With and Without ACE Inhibition with Perindoprilat
DISCUSSION
In this study, we demonstrated with PET that maximal coronary flow is reduced in normotensive, normoalbuminuric NIDDM patients. This finding agrees with the findings of a previous study (9). The major factor connected with a reduction in CBF seems to be hyperglycemia (10). Concordant with this was our finding that NIDDM patients had significantly higher fasting glucose levels and hemoglobin A1c levels. Because none of the patients had signs of coronary artery disease (no symptoms; normal exercise electrocardiography findings), it is likely that the cause of abnormal flow regulation may, in part, be dysfunction of the endothelium. This idea is supported by the ability to induce endothelial dysfunction in healthy volunteers by hyperglycemia (11). The fact that infusion of an ACE inhibitor normalized the maximal CBF supports the absence of epicardial coronary artery disease in our patients. The beneficial effect of ACE inhibition on endothelial function in NIDDM has been described in a previous study (12). We used dipyridamole for the induction of maximal CBF. Does dipyridamole-induced maximal CBF reflect endothelial function? Although the direct effect of dipyridamole acting through adenosine is exerted on vascular smooth muscle and thus is not endothelium dependent, the subsequent increase in flow through shear stress has been found to lead to release of vasodilators from the endothelium. In concordance with this finding, a previous study showed that the coronary flow response to adenosine relates, in part, to endothelium-dependent vasodilatation (13). Furthermore, the mechanisms of adenosine-induced epicardial coronary artery dilatation also seem predominantly to be endothelium dependent (14). Taken together, the dipyridamole-induced CBF increase to a major part seems to reflect endothelial function in patients without structural coronary artery disease.
CPT is also regarded as a way of studying endothelial function, primarily based on comparison with the response to intracoronary infusion of acetylcholine. Through nociception, CPT activates the sympathetic nervous system and the release of catecholamines from the adrenal medulla to the blood. Although the catecholamines directly lead to vasoconstriction, the increased oxygen demand of the myocardium indirectly leads to a secondary increase in CBF in the normal heart. The net effect in the normal heart is vasodilatation and increased CBF. However, in patients with endothelial dysfunction, the loss of vasodilating mechanisms leads to insufficient or absence of vasodilation and increase in CBF. In our study, CPT increased CBF in most of the control subjects (7/10) but not in the NIDDM patients, although the hemodynamic responses were similar. This finding strongly suggests dysfunction of the endothelium in NIDDM. A concordant recent finding was that, when CPT was used in healthy volunteers and NIDDM patients with normal coronary angiograms, the flow increase in the left anterior descending coronary artery was significantly lower in the NIDDM patients although the increase in RPP was similar (15). The significant increase in CBF by CPT during ACE inhibition in the NIDDM group suggests improvement or normalization of endothelial function during ACE inhibition. The increase in CBF in response to CPT was not significant in the control group during ACE inhibition, but that is obviously explained by the low number of control subjects receiving perindoprilat. However, the findings regarding NIDDM patients are not weakened, because the same 10 patients were studied both during placebo and during ACE inhibition: With saline infusion, CBF increased in 4 NIDDM patients during CPT whereas CBF decreased in 6. During ACE inhibition, CBF increased in 8 of the 10 patients.
The increases in CBF during CPT are small even in control subjects, and CBF increased in only 7 of 10 subjects. CPT is therefore less useful for the study of endothelial function than would be dipyridamole, for example. In theory, this limitation could be circumvented by use of a stronger CPT. However, the test is also limited by the pain perceived by the subjects. A difference stemming from our use of foot immersion instead of hand immersion could also be argued. We find such a difference unlikely, since the increase in RPP in our study was similar or even higher than that found by others (15,16). Thus, the stimulus must have been quantitatively adequate. Furthermore, a study directly comparing different ways of performing CPT found equivalent cardiovascular responses using hand and foot immersion (17). Taking these factors together, we believe that foot CPT and hand CPT provide equivalent information on myocardial vasomotion.
CONCLUSION
This study indicated that dipyridamole may be useful for the noninvasive examination of coronary endothelial dysfunction. In contrast, CPT seems less useful for this purpose because of the small and inconsistent CBF changes in response to the test.
Footnotes
Received Apr. 12, 2002; revision accepted Aug. 21, 2002.
For correspondence or reprints contact: Andreas Kjaer, MD, PhD, DMS, Section 4011, Department of Clinical Physiology and Nuclear Medicine, Blegdamsvej 9, DK-2100 Copenhagen, Denmark.
E-mail: kjaer{at}mfi.ku.dk
REFERENCES
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Cardiac Positron Emission Tomography
- Impact of Type 2 Diabetes on Nitric Oxide and Adrenergic Modulation of Myocardial Perfusion
- Insulin Improves Myocardial Blood Flow in Patients With Type 2 Diabetes and Coronary Artery Disease
- Clinical Evaluation of a New Concept: Resting Myocardial Perfusion Heterogeneity Quantified by Markovian Analysis of PET Identifies Coronary Microvascular Dysfunction and Early Atherosclerosis in 1,034 Subjects
- Coronary Circulatory Dysfunction in Insulin Resistance, Impaired Glucose Tolerance, and Type 2 Diabetes Mellitus