


Abstract
201Tl imaging and dobutamine echocardiography (DE) can both identify viable myocardium. Prediction of functional outcome after revascularization remains suboptimal with either technique because of the relatively low specificity of 201Tl and low sensitivity of DE. This study was undertaken to develop an optimal testing strategy for prediction of postrevascularization functional outcome. Methods: Seventy-three patients (mean [±SD] left ventricular ejection fraction [LVEF], 32% ± 8%) underwent DE and resting 201Tl SPECT (4-h delayed imaging) before surgical revascularization. Dysfunctional segments with 201Tl activity ≥ 50% or with contractile reserve were considered viable. LVEF was assessed before and 3–6 mo after revascularization. Results: Analysis of receiver operator characteristic curves showed that the optimum criteria to predict improvement (≥5%) in LVEF after revascularization were ≥6 viable dysfunctional segments (using a 16-segment model) on 201Tl and ≥4 segments on DE. Sensitivity and specificity were 84% and 63% for 201Tl (P < 0.05 vs. DE) and 63% and 85% for DE (P < 0.05 vs. 201Tl). Changing the 201Tl criteria to improve specificity to 78% (≥8 segments) yielded a low sensitivity of 44%, and changing the DE criteria to improve sensitivity to 84% (≥2 segments) lowered specificity to 56%. Two sequential testing strategies were explored to achieve optimal sensitivity and specificity. In strategy 1, 33 (45%) of 73 patients with an intermediate likelihood of viability by 201Tl (5–8 viable segments) underwent DE. In strategy 2, 31 (42%) of 73 patients with an intermediate likelihood of viability by DE (2–4 viable segments) underwent 201Tl. For strategy 1, sensitivity did not change significantly (69%), whereas specificity was improved significantly (93%, P < 0.01 vs. 201Tl). For strategy 2, sensitivity improved significantly (78%, P < 0.05 vs. DE) and specificity remained unchanged (80%). Conclusion: Sequential testing by 201Tl SPECT and DE in a subgroup of patients with an intermediate likelihood of viability by either test significantly enhanced prediction of postrevascularization improvement of LVEF.
Gheorghiade and Bonow (1) reported in 1998 that an estimated 4.7 million patients in the United States had chronic heart failure, with 6-y mortality rates between 65% and 80%. The incidence of coronary artery disease in these patients may be as high as 70% (2). Therapeutic options for these patients include medical therapy, heart transplantation, and revascularization. Viability assessment may help to guide patient treatment; only in patients with substantial viability can revascularization be considered, because improvement of function and survival may be anticipated in these patients only (3). Several techniques have been developed, including 18F-FDG PET (4), SPECT with 201Tl (5,6) or 99mTc-labeled tracers (7), and dobutamine echocardiography (DE) (8). For routine clinical use, 201Tl (using either a rest-redistribution or a reinjection protocol) (5,6) and DE (8) may be the preferred techniques. However, studies have shown that both techniques may provide suboptimal information concerning identification of viable tissue and prediction of functional outcome after revascularization (9–11). 201Tl imaging has an excellent sensitivity but a somewhat lower specificity (9–11). Conversely, DE has a high specificity but a relatively lower sensitivity (9–11). The likelihood of improvement in left ventricular (LV) function after revascularization relates to the extent of (number of segments with) viability. We hypothesized that in patients with an intermediate likelihood of LV function improvement, as predicted by either test, sequential testing by the second modality may further classify the patient as having a high or low likelihood of viability. Hence, sequential performance of these tests may result in optimal diagnostic accuracy in patients with an intermediate likelihood of viability. Accordingly, this study was undertaken to develop an optimal testing strategy for prediction of functional outcome after revascularization using 201Tl and DE. All patients presented with depressed LV function, and most had heart failure as the predominant symptom.
MATERIALS AND METHODS
Patients and Study Protocol
Patients were eligible for the study if they had stable, chronic coronary artery disease; had depressed LV function on LV ventriculography; were already scheduled for surgical revascularization (coronary artery bypass grafting); had no significant valvular disease (patients with 3–4+ (moderate to severe) mitral insufficiency were excluded); and had an acoustic window adequate for echocardiographic evaluation (6 patients were excluded because of a suboptimal window).
Within 1 mo before revascularization, radionuclide ventriculography, resting echocardiography, 201Tl imaging, and DE were performed. 201Tl imaging and DE were performed within 1 wk. β-blockers were withdrawn 36 h before DE; all other cardiac medication was continued during both tests. Three to 6 mo after the revascularization, resting echocardiography and radionuclide ventriculography were repeated. Eighteen patients had been included in previous studies (12). The protocol was approved by the local Medical Ethics Committee, and each patient gave informed consent before inclusion in the study.
Assessment of Baseline Dysfunction and Functional Outcome
Regional LV Function.
Regional function was assessed by resting echocardiography before and 3–6 mo after revascularization. A 16-segment model, according to the American Society of Echocardiography (13), was used for the analysis. The LV was divided into 4 apical, 6 distal (anterior, anterolateral, inferolateral, inferior, inferoseptal, and anteroseptal), and 6 basal segments. The segments were classified as normokinetic, mildly hypokinetic, severely hypokinetic, akinetic, or dyskinetic. Previously reported inter- and intraobserver agreements for assessing resting wall motion were 84% and 87%, respectively (14).
Global LV Function.
LV ejection fraction (LVEF) (before and 3–6 mo after revascularization) was assessed by radionuclide ventriculography, performed at rest with the patient supine after administration of 740 MBq 99mTc. Images were acquired with a small-field-of-view gamma camera (Orbiter; Siemens Corp., Iselin, NJ), oriented in the 45° left anterior oblique position with a 5°–10° caudal tilt. The LVEF was calculated from the 45° left anterior oblique view by an automated technique. Improvement of global function after revascularization was defined as an LVEF increase ≥ 5% (15–17). Thus, the gold standard for viability on a patient basis was considered to be ≥5% improvement of LVEF after revascularization.
201Tl Imaging
201Tl SPECT was performed as described previously (9–11,18). In short, 111 MBq 201Tl-chloride were injected at rest, and 4-h delayed images were obtained. SPECT was performed on a single-head Orbiter camera. Thirty-two projections were obtained in a 180° orbit extending from the 40° left posterior oblique projection to the right anterior oblique projection, with an acquisition time of 60 s per projection. An energy window of 20% was centered on the 68- to 80-keV peak. Images were stored on a 64 × 64, 16-bit matrix. A Gamma-11 computer system (Compaq Computer Corp., Houston, TX) was used to process the tomographic data. Long- and short-axis tomograms were reconstructed from the 3-dimensional voxel matrix. Circumferential count profiles (60 radii, highest pixel activity per radius) from the 201Tl short-axis slices were generated and displayed in a polar map format. The polar maps were divided into 16 segments, aligning the 16 echocardiographic segments, so that the polar map data could be compared with the echocardiographic data. The polar maps were normalized for peak activity (100%), and segmental activities were expressed as percentage of the maximum. For the classification of viable and nonviable tissue in dysfunctional segments (determined by resting echocardiography), the normalized activity of the 4-h delayed images was used (9–11,18). Segments were considered viable when the activity was ≥50% and nonviable when the activity was <50% (9–11,18). The criteria for viability on a patient basis (how many dysfunctional but viable segments were needed to classify a patient as having viable myocardium) were determined by receiver operating characteristic (ROC) curve analysis.
DE
DE (low-dose protocol) was performed as described previously (14). First a 2-dimensional transthoracic echocardiogram in the standard apical and parasternal views and a 12-lead electrocardiogram were recorded at rest. Dobutamine was infused through an antecubital vein at dosages of 5 and 10 μ g/kg/min for 5 min at each dose. Continuous monitoring of the echocardiogram was obtained during the test and recorded on videotape at the last minute of both stages. The echocardiographic images were also digitized on an optical disk (CFM 800; Vingmed, Horten, Norway) or on a floppy disk (SIM 7000; Esaote Biomedica, Munich, Germany) and displayed side by side in a cine-loop format to facilitate the comparison of the rest and dobutamine images. A 3-lead electrocardiogram was continuously monitored, and a 12-lead electrocardiogram was recorded every minute. Blood pressure was measured by sphygmomanometry at each stage. Two experienced observers (in cases of disagreement, 3 observers) who were unaware of the clinical data, 201Tl results, and outcome data interpreted the echocardiograms. The DE studies were analyzed using the digitized rest and low-dose (5 and 10 μg/kg/min) dobutamine images, displayed in a cine-loop format, and also by reviewing the images recorded on the videotape. Myocardium was judged to be viable when dysfunctional segments improved during dobutamine stimulation (improvement from dyskinesia to akinesia was not considered to indicate viability). Dysfunctional segments without improvement were considered nonviable. Inter- and intraobserver agreements of 92% and 94% for the analysis of DE studies were reported previously (14). The criteria for viability on a patient basis (how many dysfunctional but viable segments were needed to classify myocardium as viable) were determined by ROC curve analysis.
Statistical Analysis
Continuous data were expressed as mean ± SD and compared using the Student t test for paired and unpaired data when appropriate. Univariate analysis for categoric variables was performed using the χ2 test with Yates correction. The optimal number of viable segments on 201Tl or DE (discriminating between patients with and without improvement of LVEF after revascularization) was determined by ROC curve analysis. The optimal cutoff value (number of segments) was defined as that providing the maximal sum of sensitivity and specificity. Sensitivity and specificity were based on their standard definitions. Differences between sensitivities and specificities (of the different modalities or sequential approaches) were determined by McNemar testing. For all tests, a probability value < 0.05 was considered significant.
RESULTS
Study Population
Seventy-three patients (68 men, 5 women; age range, 45–80 y; mean age, 61 y) with coronary artery disease and depressed LV function (mean LVEF, 32% ± 8%) who were scheduled for surgical revascularization were enrolled in the study. The reasons for revascularization were heart failure in 56 patients and angina pectoris in 17. Seventy-one patients (97%) had a previous infarction (>1 mo before entrance into the study), and 58 exhibited pathologic Q waves on the electrocardiogram. All patients had significant coronary artery disease on angiography (>50% reduction in luminal diameter of at least 1 major epicardial coronary artery). They had an average of 2.5 ± 0.7 stenosed vessels. All patients were stable during the study; none had unstable angina or myocardial infarction between revascularization and scintigraphy or after the intervention.
Baseline Function Versus Functional Outcome
A total of 1,168 segments were analyzed (in 73 patients), with 571 (49%) showing abnormal wall motion. Baseline dysfunction included dyskinesia in 20 segments (4%), akinesia in 264 (46%), severe hypokinesia in 106 (19%), and mild hypokinesia in 181 (32%). Wall motion improved in 201 segments (35%), including 67 that were mildly hypokinetic, 51 that were severely hypokinetic, and 83 that were akinetic or dyskinetic. Baseline LVEF ranged from 13% to 48%. In the entire group, LVEF improved modestly but significantly (32% ± 8% vs. 36% ± 10%, P < 0.05). The LVEFs before and after revascularization of the individual patients are shown in Figure 1. Thirty-two patients (44%) improved ≥5% in LVEF after the revascularization (from 31% ± 8% to 41% ± 9%). In 41 patients, LVEF did not improve ≥5% (33% ± 8% vs. 33% ± 8%). The characteristics of the patients with and without improvement are shown in Table 1; no significant differences were observed between the 2 groups, only the number of viable segments on 201Tl and DE was significantly higher in the patients with improved LVEF than in the patients without LVEF. Of interest, significantly more dysfunctional segments were classified as viable by 201Tl than by DE, both in the entire population (6.2 ± 3.6 vs. 2.9 ± 2.7, P < 0.01) and in the subgroups with and without improvement of LVEF (Table 1).

Individual LVEFs before and after revascularization (rev) in patients without ≥5% improvement of LVEF (A) and with ≥5% improvement of LVEF (B).
Clinical Data Before Revascularization, Grouped by LVEF Status After Revascularization
201Tl Imaging
ROC curve analysis showed that a cutoff value of 6 dysfunctional but viable segments yielded the highest sensitivity and specificity (Fig. 2; area under the curve, 0.76); 27 of 32 patients with an improvement of LVEF after the revascularization had at least 6 viable segments, and 26 of 41 patients with fewer than 6 viable segments did not improve. Using this cutoff level, 201Tl had a sensitivity of 84% and a specificity of 63%. When specificity was improved to 78% (by shifting the optimal cutoff value to at least 8 viable segments), the sensitivity declined to 44%.

ROC curve analysis of 201Tl data shows that cutoff value of 6 dysfunctional but viable segments yielded highest sensitivity and specificity for predicting improved LVEF after revascularization.
An intermediate likelihood of viability was defined as 5–8 dysfunctional but viable segments on 201Tl; this range was determined on the basis of the ROC curve (Fig. 2). Twenty-six patients (36%) had 4 or fewer viable segments on 201Tl and were classified as low likelihood; only 4 patients (15%) showed improvement of LVEF. Fourteen (19%) of the patients had at least 9 viable segments and were classified as high likelihood, with LVEF improving in 10 patients (71%). The remaining 33 patients had 5–8 viable segments, with LVEF improving in 17; these were classified as intermediate likelihood and were referred for DE.
DE
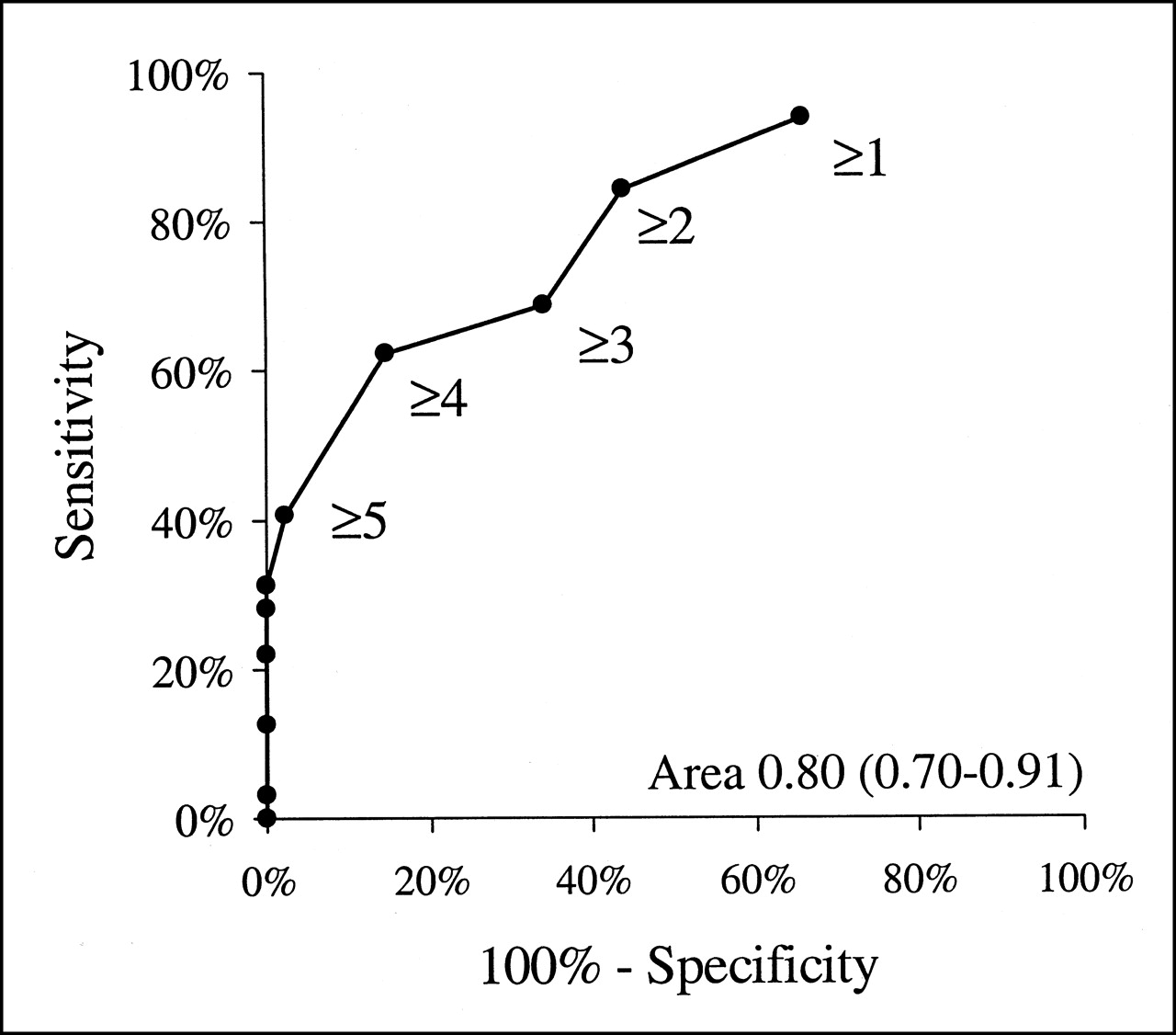
ROC curve analysis showed that a cutoff value of 4 dysfunctional but viable segments yielded the highest sensitivity and specificity (Fig. 3; area under the curve, 0.80); 20 of 31 patients with an improved LVEF after revascularization had at least 4 viable segments, and 35 of 41 patients with fewer than 4 viable segments did not improve. Using this cutoff level, DE had a sensitivity of 63% (P < 0.05 vs. 201Tl) and a specificity of 85% (P < 0.05 vs. 201Tl). When sensitivity was improved to 84% (by shifting the optimal cutoff value to at least 2 viable segments), the specificity was lowered to 56%.

ROC curve analysis of dobutamine echocardiographic data shows that cutoff value of 4 dysfunctional but viable segments yielded highest sensitivity and specificity for predicting improved LVEF after revascularization.
An intermediate likelihood of viability was defined as 2–4 dysfunctional but viable segments on DE; this range was based on the ROC curve (Fig. 3). Twenty-eight patients (38%) had fewer than 2 viable segments on DE and were classified as low likelihood; only 5 patients (18%) had improved LVEF. Fourteen (19%) of the patients had at least 5 viable segments and were classified as high likelihood, with 13 patients (93%) showing improved LVEF. The remaining 31 patients had 2–4 viable segments, with LVEF improving in 14; these were classified as intermediate likelihood and were referred for 201Tl.
Sequential Testing, Strategy 1
For strategy 1, 201Tl was performed as the initial test and DE was performed as an additional test on the patients with an intermediate likelihood of viability on 201Tl. Hence, in 33 (45%) of 73 patients, an additional test was needed to further assess the likelihood of improvement in LVEF (Fig. 4).
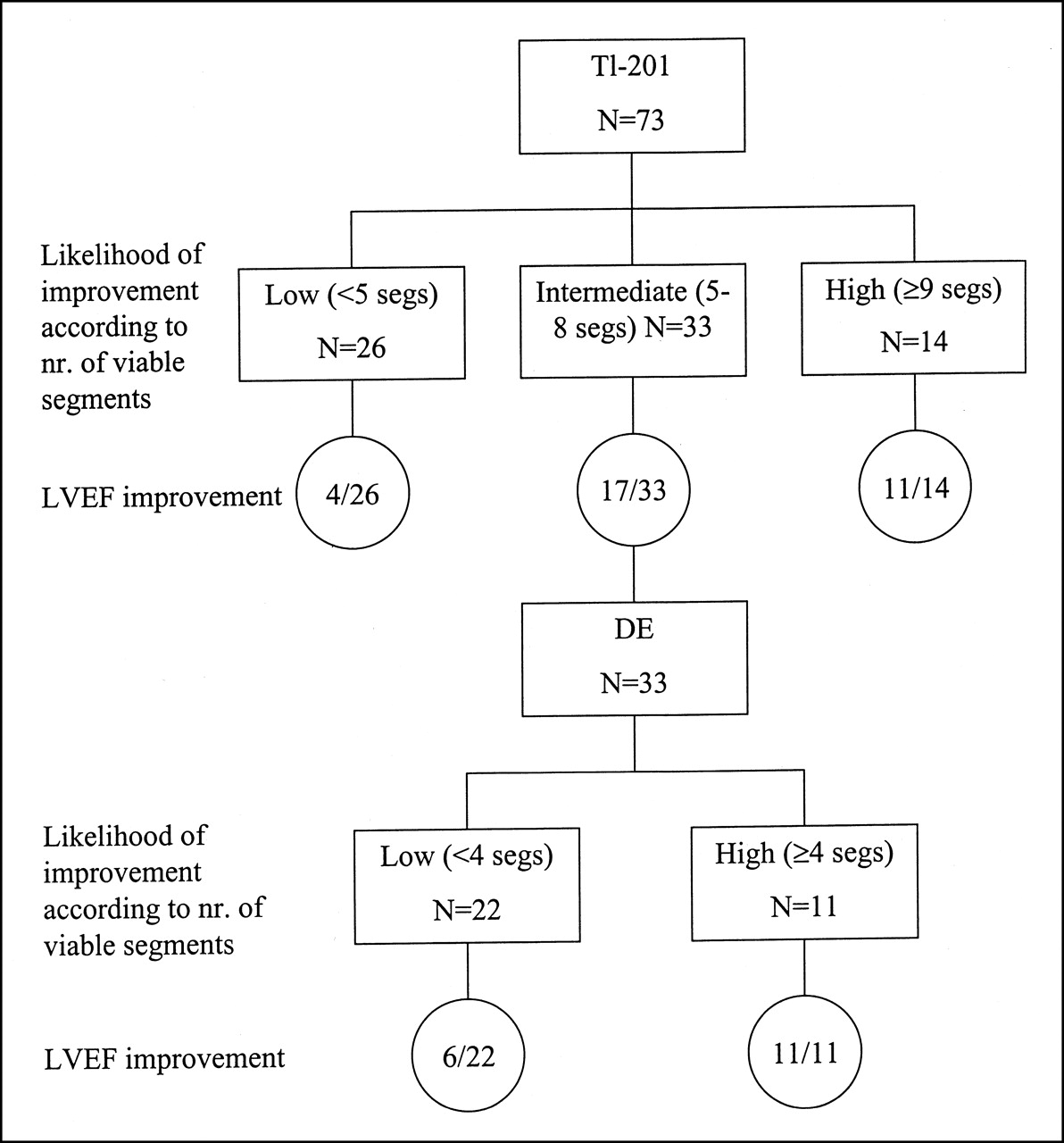
Flow chart of characterization (and outcome) of patients according to strategy 1 (201Tl was performed as initial test, and DE was performed as additional test on patients with intermediate likelihood of viability on 201Tl). nr. = number; segs = segments.
Twenty-two (67%) of these patients had fewer than 4 viable segments on DE and were subsequently classified as low likelihood; LVEF improved in 6 (27%) of them. The remaining 11 patients had at least 4 viable segments on DE and were classified as high likelihood; all (100%) exhibited improved LVEF after revascularization (Fig. 4).
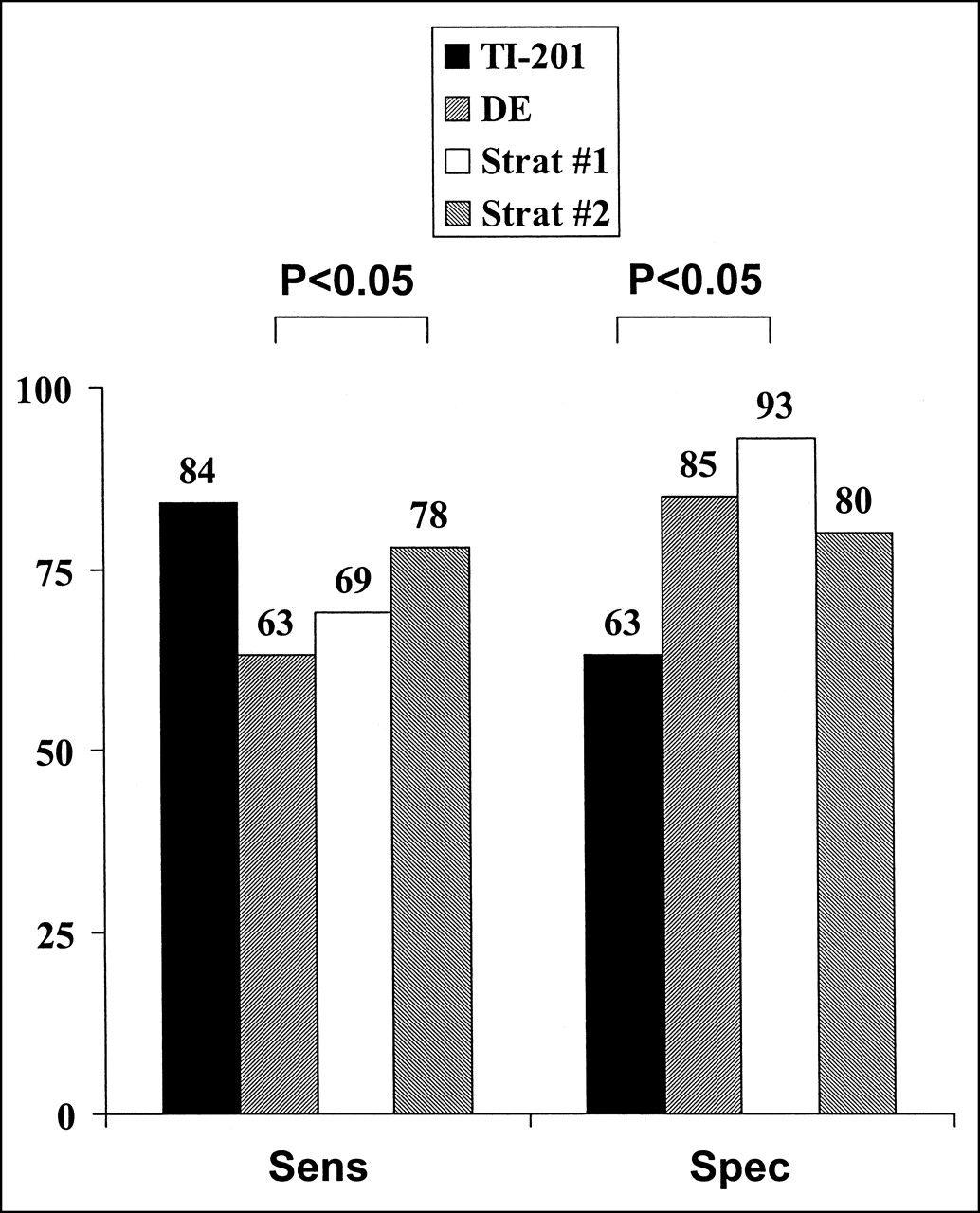
Thus, sequential testing correctly identified 22 of 32 patients with improvement of LVEF and 38 of 41 patients without improvement of LVEF, resulting in a sensitivity of 69% and a specificity of 93% (Fig. 5). Sequential testing according to strategy 1 improved specificity significantly compared with 201Tl alone (P < 0.05, Fig. 5). Moreover, the specificity of strategy 1 was not significantly different from that of DE alone or of strategy 2 (Fig. 5). Finally, the sensitivity of strategy 1 was not significantly different from that of 201Tl alone (P = 0.07) or of strategy 2 (Fig. 5).
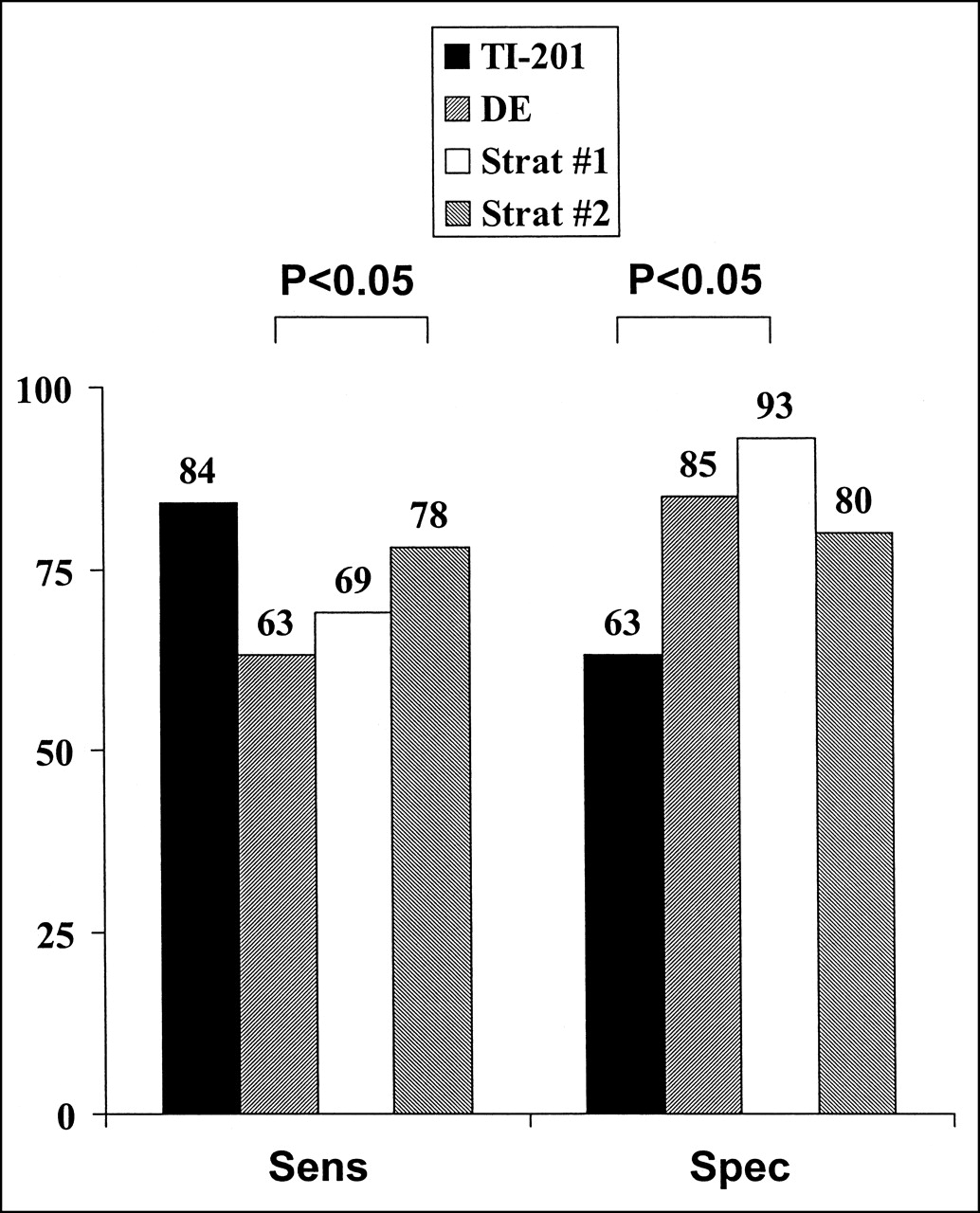
Bar graph shows sensitivities and specificities of 201Tl, DE, and sequential strategies (strategy 1: 201Tl was initial test, and DE was additional test; strategy 2: DE was initial test, and 201Tl was additional test) for predicting improved LVEF after revascularization. Sens = sensitivity; spec = specificity; strat = strategy.
Sequential Testing, Strategy 2
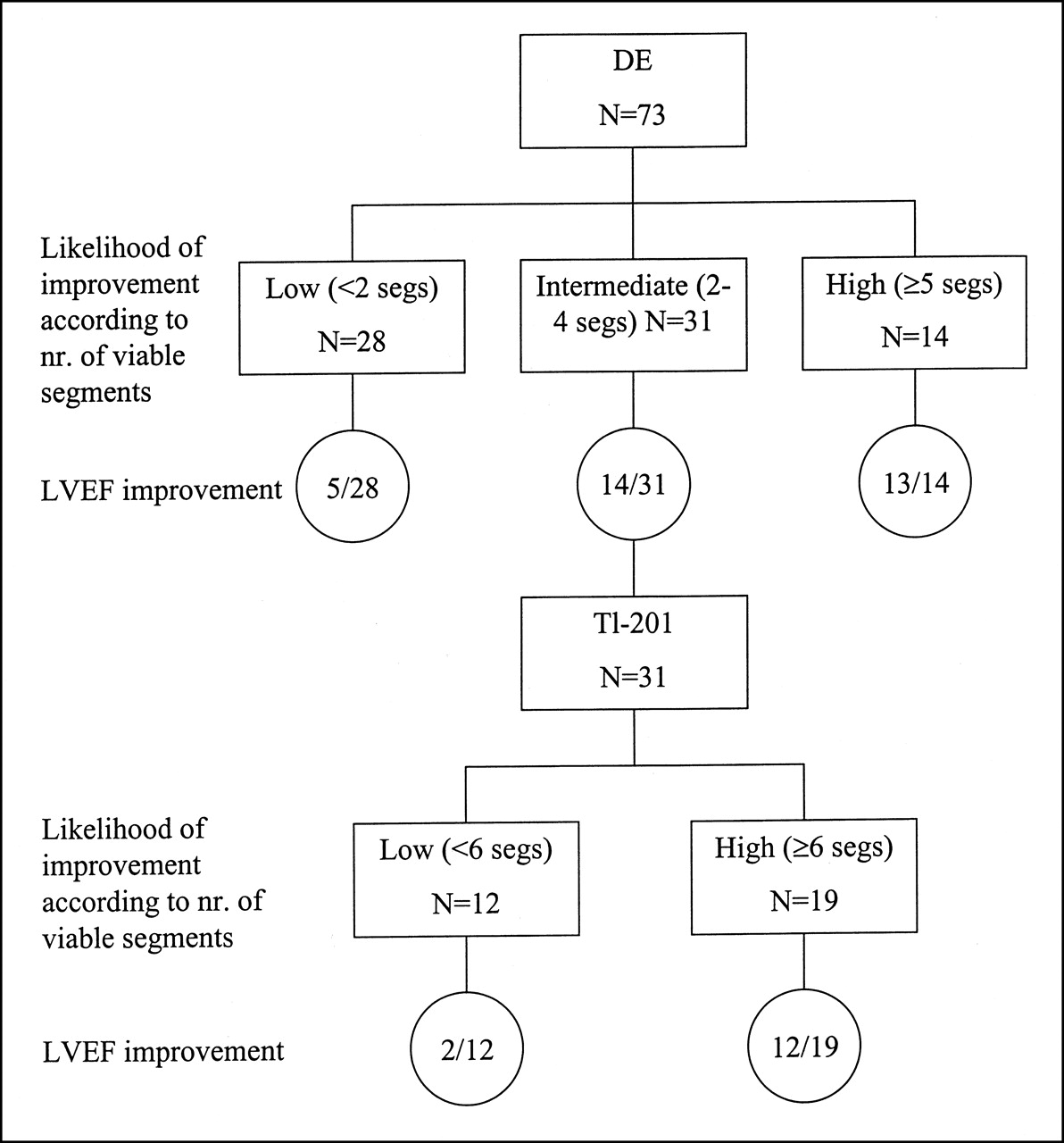
For strategy 2, DE was performed as the initial test and 201Tl was performed as an additional test on the patients with an intermediate likelihood of viability on DE. Hence, in 31 (42%) of 73 patients, an additional test was needed to further assess the likelihood of improvement in LVEF (Fig. 6). Twelve (39%) of these patients had fewer than 6 viable segments on 201Tl and were subsequently classified as low likelihood; LVEF improved in 2 (17%) of them. The remaining 19 patients had at least 6 viable segments on 201Tl and were classified as high likelihood; 12 (63%) exhibited improved LVEF after revascularization (Fig. 6).

Flow chart of characterization (and outcome) of patients according to strategy 2 (DE was performed as initial test, and 201Tl was performed as additional test on patients with intermediate likelihood of viability on DE). nr. = number; segs = segments.
Thus, sequential testing correctly identified 25 of 32 patients with improvement of LVEF and 33 of 41 patients without improvement of LVEF, resulting in a sensitivity of 78% and a specificity of 80% (Fig. 5). Sequential testing according to strategy 2 improved sensitivity compared with DE alone (P < 0.05, Fig. 5). Moreover, the sensitivity of strategy 2 was not significantly different from that of 201Tl alone or of strategy 1 (Fig. 5). Finally, the specificity of strategy 2 was not significantly different from that of DE alone or of strategy 1 (Fig. 5).
DISCUSSION
With the increasing number of patients presenting with heart failure (secondary to ischemic heart disease), assessment of myocardial viability has become more relevant for routine patient management (1–3,6,8). Many noninvasive tests have been developed for this purpose over the past 10–15 y (3,6,8). For clinical routine, 201Tl imaging and DE are used most frequently (5,6,8). However, both tests have proven suboptimal for the preoperative prediction of functional improvement (9–11). In the current study, we explored whether sequential use of these techniques (in a subset of patients with an intermediate likelihood of viability) enhanced the accuracy of predicting improved function.
The hallmark of viability for 201Tl SPECT is tracer retention on 4-h delayed images (5,6). Segments were classified as viable when the 201Tl activity was ≥ 50% (normalized to maximum tracer uptake), as was used in most of the 201Tl studies (9–11,18). Because the amount of viable tissue needed to predict improvement of LVEF after revascularization is unknown, ROC curve analysis was used to identify the number of viable segments best discriminating between patients with and without recovery of LVEF.
The optimal cutoff value was determined to be 6 dysfunctional segments containing ≥50% activity. Hence, at least 38% of the LV (6/16 segments) had to be viable on 4-h delayed 201Tl images to result in improvement of LVEF. At this cutoff level, a sensitivity of 84% was obtained at the cost of a somewhat lower specificity (63%), in line with the literature (9–11).
Identification of tissue viability with DE is based on demonstration of contractile reserve during infusion of dobutamine (8). A shortcoming of the technique is that a substantial percentage of the patients may have a suboptimal acoustic window. Dysfunctional segments were classified as viable when wall motion improved during the infusion of low-dose dobutamine. Myocardium was classified as viable using ROC curve analysis; the best trade-off between sensitivity and specificity was found at a cutoff level of 4 dysfunctional segments showing contractile reserve, in line with previous work from our laboratory in a different patient population (12). In other words, ≥25% of the LV (4/16 segments) had to be viable on DE to result in improvement of LVEF. Using this cutoff criterion, a high specificity (85%) was obtained at the cost of a lower sensitivity (69%), in line with the literature (9–11).
Attempts to improve the sensitivity of DE resulted in a loss of specificity because of the shape of the ROC curve (Fig. 3). Similarly, improving the specificity of 201Tl imaging resulted in a decline of sensitivity (Fig. 2). Thus, either modality alone could not provide optimal accuracy for predicting improved LVEF. Direct comparative studies between 201Tl and DE confirmed our findings (although these studies were performed on a segmental basis) (Table 2).
Direct Comparisons Between Resting 201Tl Imaging and DE (166 Patients, 8 Studies)
In the current study, we evaluated the use of sequential testing to increase the accuracy of predicting improved LVEF after revascularization. In the first strategy, 201Tl was performed as the initial test. On the basis of the ROC curve analysis, patients with at least 9 viable segments on 201Tl were considered to have viable myocardium and patients with 4 or fewer viable segments were considered to have nonviable myocardium. For these patients, no additional test was performed. For the 33 patients (45% of the population) with an intermediate likelihood of viability (5–8 viable segments), DE was performed to enhance diagnostic accuracy. Accordingly, sensitivity did not change significantly (69%), whereas specificity improved significantly (93%, P < 0.05 vs. 201Tl alone) (Fig. 5).
In the second strategy, DE was performed as the initial test. On the basis of ROC curve analysis, 201Tl was required for 31 patients (42% of the population). Use of sequential testing enhanced sensitivity significantly (78%, P < 0.05 vs. DE alone), whereas specificity remained unchanged (80%) (Fig. 5).
Hence, the strategies better predicted improved LVEF when applied together than when applied separately. The sensitivity and specificity of the 2 strategies were not significantly different, suggesting that the order of testing did not influence the results. The choice of the first test can therefore best be determined by local expertise and experience.
This study had several limitations. The first was that low-dose DE was performed. Recent data indicate that the use of combined low- and high-dose DE resulted in higher diagnostic accuracy for predicting functional recovery, with the higher accuracy being ascribed to integration of information about both viability and stress-induced ischemia (12,24). In the current study, however, the nuclear technique was resting 201Tl imaging, which also takes only viability (and not stress-induced ischemia) into account.
A second study limitation was that the 201Tl data were analyzed according to 201Tl activity on the delayed image; using redistribution as an additional criterion might have improved specificity. Alignment between scintigraphic and echocardiographic imaging modalities remains difficult, although much experience has been obtained in previous studies (14,15).
Finally, follow-up was 3–6 mo after revascularization; a longer time may be needed for the function of severely damaged myocardium to improve after revascularization. In particular, segments with 201Tl uptake without contractile reserve may need a longer time to improve in function.
CONCLUSION
The results of the current study indicated that sequential testing by 201Tl SPECT and DE on a subgroup of patients with an intermediate likelihood of myocardial viability by either test alone significantly enhanced prediction of postrevascularization improvement of LVEF. Sequential testing may be the method of choice for optimal assessment of myocardial viability and prediction of improved LVEF after revascularization.
Footnotes
Received Jul. 8, 2001; revision accepted Dec. 3, 2001.
For correspondence or reprints contact: Jeroen J. Bax, MD, Department of Cardiology, University Hospital Leiden, Rijnsburgerweg 10, 2333 AA Leiden, The Netherlands.
E-mail: jbax{at}knoware.nl
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Stunning, Hibernation, and Assessment of Myocardial Viability
- Radionuclide techniques for the assessment of myocardial viability and hibernation
- The Effect of Nitroglycerin on Myocardial Blood Flow in Various Segments Characterized by Rest-Redistribution Thallium SPECT
- Sequential Strategy Using Multimodality Viability Tests: Does It Work?