


Abstract
Bronchodilator aerosols are frequently administered to infants with bronchiolitis but with little success. The efficacy of aerosol treatments depends mainly on adequate targeting of the aerosol particles to the inflamed airways. This study evaluated the lower respiratory tract distribution characteristics of nebulized bronchodilators in infants with acute bronchiolitis. Methods: Twelve infants (mean age ± SD, 8 mo ± 4 mo) who were admitted for acute respiratory syncytial virus bronchiolitis were treated with 99mTc-albuterol aerosol. γ-Scintigraphy was used to assess total body and lung deposition as well as pulmonary distribution of the medication. Results: Of the total 6-min nebulized dose (i.e., drug aerosol dose leaving the nebulizer [not the nebulizer charge]), 1.5% ± 0.7% reached the right lung, with only approximately one third of that (0.6%) penetrating to the peripheral lung zone. There was 7.8% ± 4.9% deposition in the upper respiratory and gastrointestinal tracts and 10%–12% remained on the face. No correlation was found between any of the deposition indices and the clinical response data or any of the demographic parameters (e.g., height, weight, body surface area, or clinical score). Conclusion: Poor total aerosol deposition in infants may be related as much to their small conducting airways as to the disease state. There is considerable room for improvement in aerosol delivery in this age group, with greater emphasis on targeting narrowed peripheral airways with superfine aerosols.
Despite conflicting results about their efficacy, bronchodilator aerosols generated by jet nebulizers are still commonly used for treating bronchiolitis (1). A recent survey found that nearly all centers administer bronchodilators to most respiratory syncytial virus (RSV) bronchiolitis patients, with the β-agonist drug albuterol being prescribed most commonly (2).
Successful aerosol therapy depends mainly on targeting an adequate dose of drug to the appropriate receptors in the respiratory tract (3). Greater lung deposition, if appropriately targeted to the airways, should lead to greater clinical benefit. For example, the efficacy of inhaled bronchodilators is related by a characteristic dose-response curve to the quantity deposited in the lungs (4,5). Therefore, knowledge of the lung dose, its regional distribution, and the manner in which pulmonary drug targeting may be affected by large and small airway obstruction in bronchiolitis is very important if aerosol therapy is to be optimized. The poor response to bronchodilator (and steroid) aerosols in bronchiolitis may be accounted for, at least in part, by inadequate aerosol delivery to the peripheral airways.
The only established technique currently available for providing noninvasive information about the total and regional deposition of inhaled compounds in the respiratory tract is γ-scintigraphy (6,7). By providing information about the dose deposited at various sites, including those within specific regions of the lung fields, this technique yields information that is impossible to obtain by other means (8). As such, γ-scintigraphy answers important questions regarding the pulmonary dose and the distribution within the lung and has been successfully applied in the evaluation of drug delivery in infantile pulmonary diseases such as bronchopulmonary dysplasia (BPD), cystic fibrosis (CF), and asthma (9–11). However, to our knowledge, no studies have been conducted to investigate the airway dose and distribution of aerosolized medications in bronchiolitis to determine if medications are capable of being delivered to affected lung regions.
This study evaluated the dose and distribution of the inhaled β-agonist bronchodilator 99mTc-albuterol in acute RSV bronchiolitis.
MATERIALS AND METHODS
Twelve (5 girls, 7 boys; mean age ± SD, 8 ± 4 mo) (Table 1) spontaneously breathing, wheezy infants, who were hospitalized with a diagnosis of acute bronchiolitis, were enrolled in the study. The diagnosis of bronchiolitis was made in the presence of a history of upper respiratory tract infection followed by the acute onset of respiratory distress with cough, breathlessness, and wheeze and clinical signs of chest hyperinflation, tachypnea, rhonchi, or crepitations occurring during a winter epidemic of bronchiolitis attributed to RSV (12). The clinical status on admission was scored according to the respiratory rate (RR), oxygen saturation (SatO2), subcostal indrawing, chest auscultation, and general evaluation, with each parameter graded on a scale of 0–2. This score, which was a compilation of other scoring systems used in bronchiolitis (13–15), quantifies the clinical severity of bronchiolitis: A mild clinical stage is characterized by a score of 0–4; 5–7 indicates moderate disease, and 8–10 indicates severe disease.
Patient Characteristics
Inclusion criteria were as follows: (a) first episode of wheezing present for <48 h; (b) proven RSV infection (Testpack radioimmunoassay kit [Abbott Laboratories, Chicago, IL], RSV on material obtained by nasopharyngeal aspiration); (c) age >4 wk and <2 y; (d) admitted to hospital for >12 h; (e) bronchodilator treatments administered at least once every 3 h and on inhaled β-agonist treatment only.
Subjects were excluded if they had a family history of asthma or atopy or if they had cardiopulmonary disease such as BPD, congenital heart disease, immunodeficiency, or CF.
Written informed consent was obtained from the parents or guardians. The study protocol was approved by the Hospital ethics committee and the Ministry of Health.
The dose and distribution of inhaled aerosol were evaluated scintigraphically 12–24 h after admission. No change in treatment schedule or clinical assessment and management occurred except for administration of the prescribed regularly scheduled, study treatments in the nuclear medicine department. These mimicked the treatment provided on the ward.
Medication
For each study treatment, the Micromist jet nebulizer (Hudson Respiratory Care Inc., Temecula CA) attached to a face mask was charged with 2.5 mg albuterol (0.5 mL of 0.5% Ventolin) respirator solution (Glaxo Wellcome, Ware, U.K.) diluted to a total of 3 mL with 0.9% saline labeled with 74–185 MBq 99mTc-diethylenetriaminepentaacetic acid. The addition of 99mTc has no physical effect on aerosol characteristics because the total contribution of this material to the total volume of medication is negligible. If a drug solution and a radiolabeled solution are mixed within the nebulizer chamber, the resulting aerosol droplets will contain drug and radiolabel in proportion to their original concentrations (4,6). Previous studies have shown that this does not alter the aerosol characteristics of what is essentially a normal saline solution (16,17).
The nebulizer was driven by an oxygen cylinder at a flow rate of 8 L/min for exactly 6 min. To maintain constant experimental conditions throughout the study we used a fixed time interval rather than the more subjective and variable sputtering technique, in which nebulization continues until no further visible mist is seen. Under these conditions, the Micromist nebulizer has a mass output of 0.26 mL/min and produces particles with a mass median aerodynamic diameter (MMAD) of 4.2 μm and a geometric SD of 1.8 (18). We used the same brand of nebulizer and units from the same batch as well as identical connecting tubing, source of oxygen, and flow conditions.
The primary outcome measures were lung aerosol deposition and intrapulmonary distribution measured scintigraphically. Immediately on completion of aerosol administration, the infant was placed under a gamma camera (SP-6; Elscint, Haifa, Israel) fitted with a low-energy, parallel-hole collimator, interfaced to a computer. Posterior and anterior images were obtained for 60 s (or until a minimum of 100,000 counts was acquired).
Correction for Tissue Attenuation
Because attenuation of radioactivity is dependent on chest size and body mass and these parameters varied greatly between patients, an attenuation correction factor was determined for each patient (19). An acrylic cylinder, 30 cm in diameter and 3 cm deep and filled with a solution of known amount of 99mTc (37–74 MBq), was used as a flood source. A fresh 99mTc flood source was made for each patient. A transmission scan was obtained before the treatment, with the infant lying on the scintigraphy bed with a flood source beneath it; prone and supine lung scans were obtained, and the geometric mean of the counts was calculated. Another scan was obtained without the infant. The square root of the ratio of the counts obtained without the infant (No) to the geometric mean of the counts with the infant (Nt) provided the individual attenuation correction factor. This factor was used to correct for the extent to which the infant’s thorax or upper abdomen (or both) attenuated γ-radiation originating in the respiratory and gastrointestinal tracts.
Image Analysis
Gamma-camera counts in various body areas were measured in the following regions of interest (ROIs): (a) Head: This ROI encompasses the head, including the face and the oropharynx. (b) Trachea, esophagus, and gastric areas: It was difficult to differentiate between the trachea and the underlying esophagus when using planar images. Thus, these regions were drawn as 1 ROI and were combined with the gastric ROI because all 3 regions contribute little to the effect of using bronchodilators. Increased deposition in these areas may contribute to systemic side effects but not to the bronchodilator response. (c) Lung: For regional lung distribution, only the right lung was assessed to avoid corruption of the data by activity in the lower esophagus and stomach behind and adjacent to the left lung (20). The central region at the medial border was 0.5 of the lung height and 0.5 of the lung width; the remaining outer part of the lung was defined as the peripheral region (Fig. 1B) (20). Delineation of lung boundaries was accomplished by superimposing lung dimensions from chest radiographs onto the scintigraphic images or, when these were not available, by transmission scan.
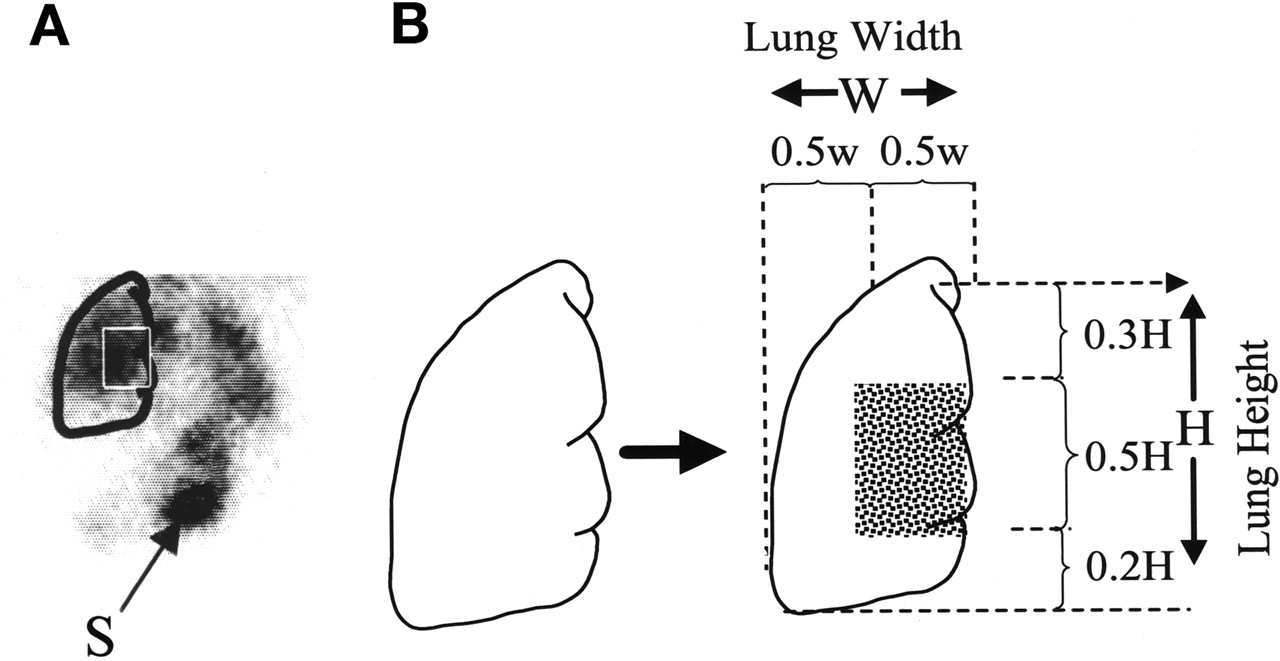
(A) Anterior image of lungs of patient with bronchiolitis. S = stomach. (B) Diagram of peripheral and central regions of lung used to determine regional aerosol distribution (modified from Phipps et al. (20)).
All ROIs were drawn by 1 author. The coefficient of variation of the counts for this observer was measured with 100 repeated drawings of a single ROI and was found to be 3.5%. Although misalignment of images (for example, posterior vs. anterior) may occur during analysis, we believe no correction for this was necessary, as it should not influence the total lung counts.
The total counts per minute in each ROI were converted to megabecquerels using Equation 1, which was derived from Macey and Marshall (21). Equation 1 incorporated the attenuation factor obtained previously and a camera sensitivity calculation:
 Eq. 1 where T is the activity in the lungs (MBq), G is the geometric mean of the counts per second corrected for background and decay (cps), E is the efficiency factor for the camera and collimator (cps/MBq), and
Eq. 1 where T is the activity in the lungs (MBq), G is the geometric mean of the counts per second corrected for background and decay (cps), E is the efficiency factor for the camera and collimator (cps/MBq), and  is the attenuation correction factor.
is the attenuation correction factor.
Deposition in each ROI was expressed as a percentage of the amount of radioactivity delivered from the nebulizer (not as absolute activity) because nebulizer output is variable (22). The amount delivered from the nebulizer (nebulizer output) was equivalent to the difference in radioactivity in the nebulizer before and after nebulization as measured in a dose calibrator (Capintec, Ramsey, NJ).
Secondary outcome measures consisted of the following clinical observations, which were recorded before and 20 min after completion of treatment: (a) SatO2 by pulse oximetry (on the same FiO2 as before the treatment); (b) RR (breaths per minute); and (c) heart rate (HR [beats per minute]).
Precautions
To minimize contamination, 99mTc-albuterol treatments were administered in a special room that was used only for this purpose. The patient and a physician were the only ones allowed in this room at any time. The nebulizer mask was modified (using 1-way valves and absolute filters) to prevent radioactive aerosol from leaking into the room air. A caregiver held each infant in a seated position with the neck slightly extended, and the mask was held firmly against the infant’s face, even while the infant was crying.
To avoid radioactive contamination of each infant’s chest, the child’s body was enclosed in a special nylon bunting, which was removed immediately after completion of the inhalation treatment.
Statistics
Results are presented as means ± SD. The Kolmogorov-Smirnov test was used to check for normal distribution. Statistical tests were 2-sided t tests conducted at the 0.05 level. Deposition data and clinical response were related by simple regression.
RESULTS
Demographic data and clinical scores of each infant are shown in Table 1. Infants were graded clinically as suffering from bronchiolitis of mild or moderate severity. The average output of the nebulizers at the outport was 40% ± 12% of the initial charge.
Individual total right lung and regional right lung 99mTc-albuterol deposition during acute bronchiolitis is shown in Table 2. Of the total 6-min nebulized dose (i.e., drug aerosol dose leaving the nebulizer [not the nebulizer charge]), 1.5% ± 0.7% reached the right lung with only approximately one third of that penetrating to the peripheral lung zone. There was 7.8% ± 4.9% deposition in the upper respiratory and gastrointestinal tracts and 10%–12% remained on the face. The remainder was found within the tubing and face mask and on the exhalation filter.
Deposition Data
The clinical response data are shown in Table 3. Treatment resulted in a statistically significant increase in the mean SatO2 (92.9% before and 95.5% after treatment; P < 0.01) and the HR (141 beats per minute before and 155 beats per minute after treatment; P < 0.05). There was also a reduction in the RR (56 breaths per minute before and 46 breaths per minute after treatment; P < 0.01). No correlation was found between any of the deposition indices and the clinical response data or any of the demographic parameters (e.g., height, weight, body surface area, or clinical score). Four infants cried much more than the others during aerosol treatments. Surprisingly, in the light of anecdotal evidence that crying greatly diminishes aerosol delivery to the lungs of infants (11) and similar baseline characteristics, the lung deposition of 99mTc-albuterol and the clinical response did not differ from that of the rest of the group.
Clinical Parameters Before and 20 Minutes After Completion of Aerosol Treatment
DISCUSSION
This study evaluated the fate of therapeutic aerosols in acute bronchiolitis. We found that during the acute stages of the disease, with the nebulizer used, the amount of drug reaching the right lung was only 1.5% ± 0.7% of the delivered dose. Most of the drug mass never reaches the bronchiolar target, and only one third of the total lung dose actually deposits in the more peripheral airways. This finding may explain why nebulized bronchodilator therapy often fails in acute bronchiolitis and may also explain the lack of response to nebulized corticosteroids in most studies (23). Aerosol studies in adults suggest that total lower respiratory tract (LRT) deposition and intrapulmonary aerosol distribution are influenced by patient-related and aerosol generation and delivery system-associated factors. Patient-related factors in this study include altered airway anatomy and physiology, as reflected in a rapid RR, and altered breathing patterns associated with airflow obstruction. The pathophysiologic and clinical features of RSV bronchiolitis are mainly the result of terminal and respiratory bronchiolar and alveolar inflammation characterized by mucosal edema and luminal plugging by inflammatory exudate resulting in airway obstruction. The associated pneumonitis and microatelectasis mainly account for the often-marked hypoxemia due to ventilation-perfusion mismatch (24). These pathophysiologic abnormalities increase airflow resistance and reduce compliance, thus causing rapid and shallow breathing. Therefore, it is not surprising that total lung deposition and particularly peripheral aerosol deposition are very poor in acute bronchiolitis. This presents a problem in infants because of their extremely small airway caliber even when they are well.
The results of our study of acute bronchiolitis in infants are similar to those obtained in infants with other obstructive airway diseases, even though the latter were in clinically stable condition and had a somewhat different pathophysiology. Mallol et al. (10) found that lung deposition in 5 infants with CF was 2.0% ± 0.7% of the nebulized dose, Chua et al. (25) found a lung deposition of 1.3% in 12 infants with CF, and Fok et al. (9) found a lung deposition of 1.74% ± 0.21% in 13 infants with BPD.
The dose of medication reaching the bronchiolar region in infants might be limited primarily by their normally small airway caliber if the aerodynamically large aerosol particles generated by most small-volume nebulizers (commonly used in clinical practice) are used. Further studies using formulations or devices (or both) that produce much smaller aerosol particles are warranted. In this regard, particle-size selective valved holding chambers, such as the AeroChamber (Trudell Medical International, London, Ontario, Canada), selectively remove approximately 90% of a normal saline aerosol over 2.8 μm (26) and provide pressurized metered-dose inhaler (pMDI)-generated 99mTc-albuterol aerosols of MMAD approximately 1.8 μm. Because this would considerably improve the therapeutic ratio, much larger doses of bronchodilator medication could be safely targeted to the 1- to 2-mm peripheral airways. Furthermore, with the recent introduction of the MMAD of 1.1-μm beclomethasone dipropionate pMDI solution aerosol (QVAR; 3M Pharma, St. Paul, MN), the hypothesis that smaller aerosol particles might provide greater therapeutic benefit in bronchiolitis could be tested (27).
CONCLUSION
In infants with acute RSV bronchiolitis, aerosolized bronchodilators reach the affected terminal airways poorly. The overall LRT deposition fraction provided in 6 min of nebulization is only approximately 1.2% of the nebulizer charge, mainly in the central and intermediate conducting airways. Although this pattern is considerably different from that of older children and adults, it differs little from that described in infants with other, primarily obstructive, pulmonary diseases. In infants, total aerosol deposition and distribution of medication within the LRT, with commonly used relatively large-particle clinical aerosol generators, may be more related to age and upper respiratory tract airway caliber than to the clinical status or underlying disease. There is considerable room for improvement in aerosol delivery in this age group because, in the light of this study, it must be assumed that the poor response to therapy in previous studies may, at least in part, have been associated with failure to target a sufficient dose of the therapeutic aerosols to the affected peripheral airways. A combination of much smaller drug particles and a relatively larger dose of medication targeted specifically to the peripheral airways may improve the therapeutic response and therapeutic ratio.
Acknowledgments
Test kits for detection of RSV were generously donated by Ilex Medical Systems (Tel-Aviv, Israel).
Footnotes
Received Aug. 28, 2001; revision accepted Dec. 18, 2001.
For correspondence or reprints contact: David Groshar, MD, Department of Nuclear Medicine, Bnai Zion Medical Center, P.O. Box 4940, Haifa, 31048 Israel.
E-mail: d.groshar{at}b-zion.org.il
REFERENCES
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- Incorporating a Nebulizer System Into High-Flow Nasal Cannula Improves Comfort in Infants With Bronchiolitis
- High-Flow Nasal Cannula and Aerosolized {beta} Agonists for Rescue Therapy in Children With Bronchiolitis: A Case Series
- Imaging in Aerosol Medicine
- Clinical Controversies in Aerosol Therapy for Infants and Children
- The effect of 3% and 6% hypertonic saline in viral bronchiolitis: a randomised controlled trial
- Feasibility of aerosol drug delivery to sleeping infants: a prospective observational study
- Nebuliser hood compared to mask in wheezy infants: aerosol therapy without tears!