


Abstract
Methylphenidate (MPH) is an effective symptomatic treatment of attention deficit hyperactivity disorder (ADHD), but the mechanisms of its therapeutic action have not been fully elucidated. To address this issue, we assessed the effects of discontinuation of chronic MPH treatment on regional cerebral blood flow (rCBF) in ADHD patients. Methods: Twenty-two prepubescent boys with ADHD (age range, 8.2–11.5 y) and 7 healthy volunteers were studied with SPECT on and off MPH. Their rCBF data were automatically normalized to whole-brain counts and coregistered with standard anatomic space. rCBF changes were evaluated with statistical parametric mapping based on voxel-by-voxel ANOVA. Results: When the subjects were not taking MPH, rCBF was higher in the motor, premotor, and the anterior cingulate cortices (Brodmann’s areas 4, 6, and 32). Conclusion: Brief discontinuation of MPH treatment is associated with increased motor and anterior cingulate cortical activity. Our findings suggest that MPH treatment modulates motor and anterior cingulate cortical activity directly or indirectly. Alternatively, our findings may be related to MPH withdrawal. These data provide novel information on the potential mechanisms of the therapeutic action of MPH. Furthermore, they are clinically relevant to the commonly occurring brief interruptions in MPH treatment.
- methylphenidate
- statistical parametric mapping
- SPECT
- attention deficit hyperactivity disorder
- motor cortex
- anterior cingulate cortex
Attention deficit hyperactivity disorder (ADHD) is a common condition characterized by locomotor hyperactivity, impulsivity, and inattention. These core ADHD symptoms may be attributable in part to inadequate response inhibition as evidenced by deficits on executive function tasks such as response inhibition and corresponding functional and structural abnormalities of the prefrontal cortex and the striatum (1–3). Thus, ADHD is a neuropsychiatric syndrome characterized by neuroanatomic defects associated with excessive motor behaviors that may stem from central inhibitory deficits.
Most ADHD patients show symptomatic response to methylphenidate (MPH) and other psychostimulants; thus, understanding the mechanism of their effect is critical to understanding the biology of ADHD (4,5). The activity of MPH on the molecular level is linked to its competition with dopamine on the dopamine transporter, but the neurophysiologic mechanism of its therapeutic effect is not fully understood (6). The neurophysiologic effects of MPH in ADHD are heterogeneous and encompass the prefrontal cortex, sensory cortex, motor cortex (MC), anterior cingulate cortex (ACC), parietal cortex, striatum, and thalamus (7–12). The reasons for the variability across studies may include differences in techniques of image acquisition and analysis, subject populations, treatment status, and diagnostic criteria. It has been suggested that MPH may specifically correct the striatal activation deficits in ADHD; however, indirect evidence indicates that the behavioral effects of stimulants are not specific (9,13).
Although the MC and ACC have important roles in locomotor activity and attention, respectively, few studies have assessed whether these regions are directly affected by MPH treatment. The rationale for such an investigation is supported by dopaminergic agonist- and antagonist-induced increases and decreases in intracortical inhibition of the MC and premotor cortex (14). Moreover, in a preclinical study, MPH treatment was associated with reduced blood flow in the MC (15). With humans, similar results were obtained in some studies (7,8,11). Hence, the decrease in MC activity after MPH in ADHD may suggest an additional mechanism for the therapeutic action of MPH, that is, enhancement of intracortical inhibition (16).
To further understand the neurophysiologic mechanism of MPH action, we studied a cohort of ADHD patients when they were taking MPH (the “on-MPH condition”) and when they were not taking MPH (the “off-MPH condition”). Using the 99mTc-labeled blood flow tracer ethylcysteinate dimer (ECD) and SPECT and statistical parametric mapping (SPM), we performed an automated within- and across-subject voxel-by-voxel analysis of the entire brain (17). 99mTc-ECD is trapped within the cytoplasm, reaching a steady state less than 1 min after injection and reflecting average regional neuronal activity over this period (18). Despite relatively low spatial resolution, SPECT has cost and availability advantages over PET and may lack the selection bias against severely hyperactive subjects, who could be excluded from the functional MRI (fMRI) datasets because of motion artifacts. Based on the results of prior studies, our primary hypothesis was that discontinuation of chronic MPH treatment would affect regional cerebral blood flow (rCBF) in the prefrontal cortex, the MC and supplementary MC, the ACC, and the corpus striatum.
MATERIALS AND METHODS
Subjects
ADHD candidates were recruited from a cohort of patients who were diagnosed by their primary care physicians, treated with MPH for an average of 12 wk (range, 8–16 wk), and demonstrated a clinical response. Potential candidates (both ADHD patients and healthy volunteers [controls]) were told about the study, including the risks and the benefits to participants and society. Those who expressed interest were referred to our research team. The study protocol was approved by the institutional review board. The parents gave written informed consent, and the children assented to participate in the study. The ADHD diagnosis was confirmed by a multidisciplinary team and was based on a minimum of three 45-min meetings and a thorough direct and collateral history. The final diagnosis was made by team consensus and was based on the ADHD criteria listed in the 4th edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-4 (19)) and a review of data from supplemental instruments, which included the Swanson, Nolan, and Pelham (SNAP) Scale and the Conners’ Parent and Teacher Rating Scales (20,21). Exclusion criteria were treatment with medications other than MPH; an intelligence quotient < 85 (Wechsler Intelligence Scale for Children); and a history of head trauma, premature birth, or a chronic medical or additional psychiatric disorder other than ADHD. Seven controls matched to the ADHD group by age, sex, intelligence quotient, and demographics were recruited from the same primary care pediatric practices. Twenty-two ADHD patients (average age, 10 y; age range, 8.2–11.5 y) and 7 controls (average age, 10 y; age range, 9–11 y) completed the study.
Image Acquisition
Each subject had 2 imaging sessions 1–3 wk apart: one in the on-MPH condition and another in the off-MPH condition. The order of the scans was counterbalanced in both groups. For the on-MPH scan, the ADHD patients received their usual prescribed dose of MPH (range, 10–30 mg) 2 h before the imaging session and the controls received a single 10-mg dose. For the off-MPH scan, MPH was withheld for 36 h before the scan for the ADHD patients. The off-MPH condition in the ADHD patients was 36 h off MPH after an average of 6 wk on the drug, whereas in the controls, the off-MPH condition was 36 h after a single dose.
Activation Task
To maintain a uniform activation state, subjects began performing a “go/no-go” task 2.5 min before administration of the radiopharmaceutical. We used the stimulus-controlled version of the task, as described by Vaidya et al. (9). Briefly, it consisted of 6 alternating go or no-go blocks lasting 25 s each. A block is a 25-s interval that begins with task instructions requiring action or inaction in response to a consonant letter displayed on the screen (“press mouse for all letters” for the go blocks; “do not press mouse for X” for the no-go blocks) followed by a consonant letter on each trial. X was not presented and C occurred on 50% of the go trials. X occurred on 50% of the trials in the no-go block. Other letters were not repeated in either block. Task performance data have not been recorded and were unavailable for subsequent analysis.
Imaging Session Procedure
After intravenous line placement for tracer injection and a go/no-go task practice session, the subjects performed the task using a mouse-operated desktop computer (Macintosh Quadra; Apple Computer, Inc., Cupertino, CA) in a quiet semidark room. The radiopharmaceutical was injected 2.5 min after the beginning of the 5-min task. After completion of the task, the subjects were placed supine on a stretcher and 20 to 30 min later were transferred to the scanner for imaging.
Radiopharmaceutical and Instrumentation
An age-adjusted dose (average, 480 MBq [13 mCi]) of 99mTc-ECD (Neurolite; Dupont, Billerica, MA) was administered, and the subject continued to perform the go/no-go task for an additional 2.5 min. Images were recorded using a triple-head scanner (MULTISPECT 3; Siemens, Des Plaines, IL) with a resolution of 8 mm in full width at half maximum (FWHM), high-resolution parallel-hole collimators, a photopeak centered at 140 keV with a 15% window, a rate of 22 s per frame with 3° increments, 40 frames per detector (a total of 120 frames), and a 128 × 128 matrix. Data were recorded using a dedicated computer system (ICON; Siemens) and were reconstructed using filtered backprojection with a low-pass Butterworth filter, order 6, at 0.55 cycles per centimeter. Images were corrected for attenuation using Chang’s first-order method.
Data Analysis
Image acquisition and analysis were performed by a team that was unaware of the clinical data. Images from each subject were aligned to each other using a rigid-body coregistration algorithm. After realignment, images were normalized to a standard stereotactic template (17,22) using affine transformations and nonlinear image warping (7 × 8 × 7 basis functions) (23). The normalized images were smoothed by being convolved with an isotropic FWHM 12-mm gaussian kernel. This step reduced the effects of image noise and conditioned the data for subsequent statistical tests performed using SPM99 (Wellcome Department of Cognitive Neurology, London, U.K.) implemented in MATLAB (The MathWorks, Inc., Natick, MA). Groups of images were compared with voxel-by-voxel paired t tests within SPM99 (24), producing statistical parametric maps of the t statistic of the rCBF differences between on-MPH and off-MPH scans within and between ADHD and control groups. Also, changes in rCBF resulting from MPH administration in the ADHD patients were compared with changes in the controls to detect significant changes in the ADHD patients over and above those in the controls (the “difference of differences”). Statistically significant differences between sets of data were assessed at each voxel with a threshold of t = 3.42, P < 0.001. To correct for correlated multiple comparisons, clusters of voxels that survived this threshold were assessed further using the theory of random gaussian fields (25), which calculated the significance of clusters on the basis of their peak height and spatial extent (150 voxels, P < 0.05).
RESULTS
Behavioral
The behavioral results are shown in Table 1. The mean hyperactivity index (±SD) on the Conners’ Teacher Rating Scale was 66.5 ± 11.5 in ADHD patients and 41.1 ± 3.5 in controls. The mean SNAP scale hyperactivity scores in ADHD patients were 1.6 ± 0.9 for the teacher scale and 2.0 ± 0.7 for the parent scale. The mean number of DSM-4 hyperactivity and inattention criteria met by ADHD patients was 7.3 ± 1.8 and 8.5 ± 0.8, respectively, whereas in the controls the mean number was 0.9 ± 1.6 and 0.8 ± 1.0, respectively. All scores were recorded in the off-MPH condition, and all differences between the ADHD and control subjects were statistically significant at P < 0.01 (2-tailed t tests).
Hyperactivity Index on Conners’ Teacher Rating Scale, SNAP Score, and Number of ADHD DSM-4 Criteria Met by Study Subjects
Imaging
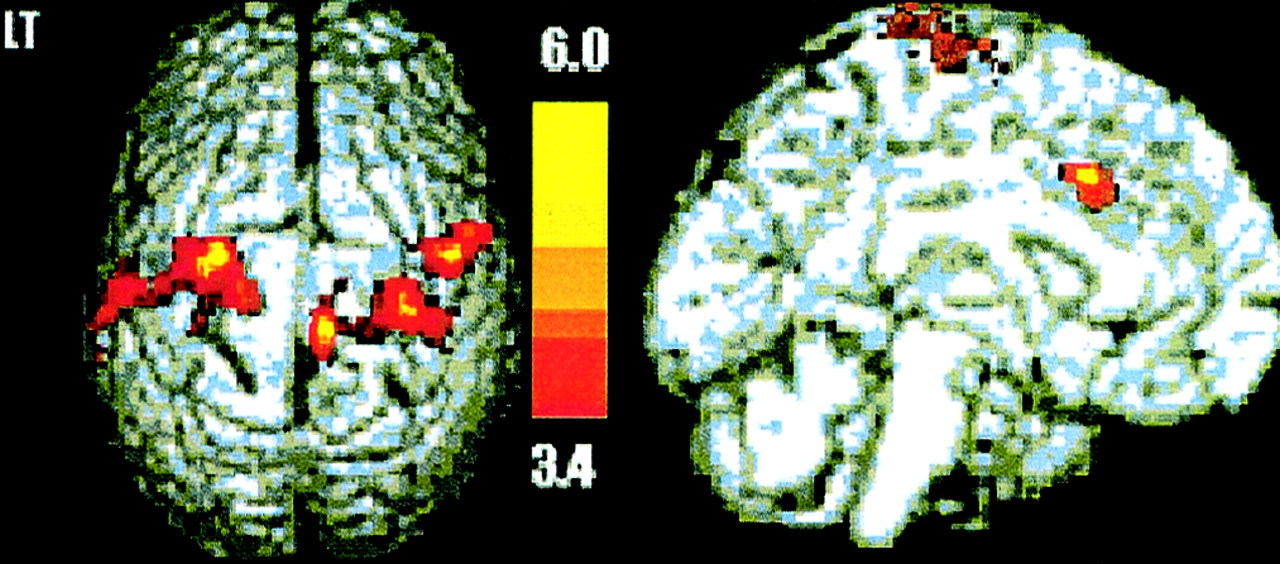
The imaging results are shown in Figure 1 and Table 2. In the ADHD group, the rCBF in the MC and premotor cortex bilaterally; in Brodmann’s area (BA) 4 and BA 6; and in the anterior cingulate gyrus, BA 32, was significantly higher in the off-MPH condition than in the on-MPH condition (P < 0.05, corrected for multiple comparisons). The change in blood flow in the off-MPH condition was also inspected at a reduced level of significance (P < 0.05, uncorrected for multiple comparisons) to investigate possible trends in the data that may not be detectable at the commonly accepted level of significance. Even at this lower level of significance, no MPH effect was seen in any additional brain regions. In the control group, no significant difference in rCBF was seen between the on- and off-MPH conditions at either level of significance. The difference between ADHD patients and controls was not significant at either threshold, and the ADHD patients showed no significant rCBF changes over and above those in the controls.
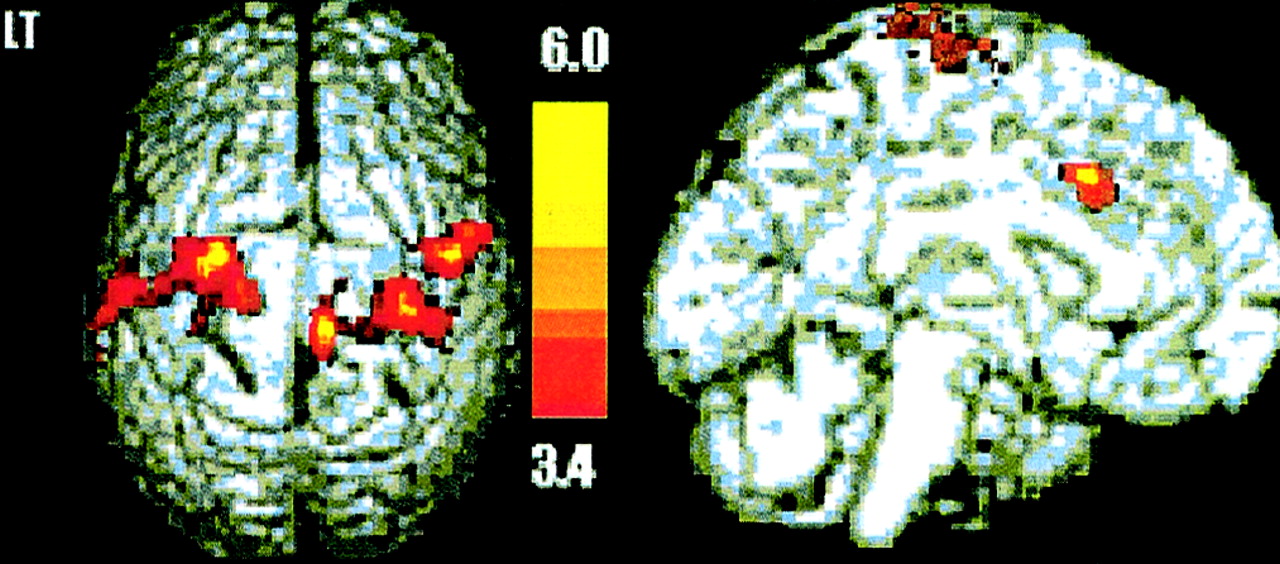
ADHD group subtraction image, on vs. off MPH. Superior and sagittal projections, over standard template, of statistical parametric (t) maps of distribution of differences between on-MPH and off-MPH conditions. Higher rCBF on MPH is seen in bilateral precentral gyri and ACC (Table 2) at t range of 3.4–6.0. P < 0.05, corrected for multiple comparisons. LT = left.
Location of Significant rCBF Increases After Discontinuation of MPH
DISCUSSION
Locomotor hyperactivity is a core clinical symptom of ADHD that decreases when patients are receiving MPH (26,27). We found increased 99mTc-ECD uptake in the ACC and the MC in a cohort of MPH-treated ADHD patients 36 h after the drug was discontinued. In some rat models of ADHD, baseline locomotor activity is decreased with administration of low to moderate doses of MPH, whereas in normal rats MPH is associated with reduced MC blood flow (15,28). Furthermore, automated voxel-based parametric analysis of perfusion SPECT in adults also showed a decrease in MC perfusion after dextroamphetamine, which shares many pharmacologic properties with MPH (29). Thus, clinical response to MPH by our subjects would be expected to translate into lower MC activity and reduced perfusion, as shown by our data.
A recent transcranial magnetic stimulation study suggested that MPH might also have a direct inhibitory effect on the MC by enhancing intracortical inhibition (14,16). This mechanism is also consistent with our findings.
Our data do not directly confirm the findings of a recent study by Vaidya et al. (9), which relied on a cohort of participants and an activation paradigm similar to ours. This study used blood oxygenation level-dependent (BOLD) fMRI to examine the effects of the task and MPH on brain activity. The findings included increased prefrontal activity on MPH in both ADHD and control groups and increased striatal activity only in the ADHD group. The value of direct comparison of our findings with Vaidya et al. is limited by the differences in study variables, statistical approach, and temporal resolution of SPECT and BOLD fMRI. Nevertheless, our findings could be reconciled with the prefrontostriatal dysfunction hypothesis in ADHD since both the MC and the ACC receive inhibitory prefrontostriatal input (30).
The ACC has a role in multiple aspects of attention, such as irrelevant stimulus filtering and error monitoring (31). The ACC is functionally subdivided into affective and cognitive divisions (3,32). The affective division includes BA 25, BA 33, and rostral part of BA 24; has extensive connections with the limbic system; and is involved in affective functions such as emotional learning, assigning emotional valence to stimuli, and maternal-infant interactions. The cognitive division includes BA 24 and BA 32 and is engaged both in response selection and in cognitively demanding information processing. Deficient processing of incoming information is thought to underlie the inattention and distractibility in ADHD (28). Children with ADHD perform below normal levels on tests of executive function such as the continuous activation task, the go/no-go task, or the Stroop color test, which require functions involving the ACC (9,33). The effect of MPH on ACC activity has not been studied with a technique and paradigm comparable to ours; however, there is indirect evidence that ACC function is abnormal in ADHD patients. Compared with controls, ADHD patients had inadequate ACC activation during a range of tests of executive function, such as the continuous activation task and the Stroop color test (3). In an imaging study on adults, Bush et al. (3) found that ADHD patients, but not controls, performing the Stroop color test failed to activate the ACC. On the basis of the task involved and the location of activation in controls (Talairach coordinates: −3, 21, and 37; BA 32), Bush et al. assigned the location of the activation deficit in their ADHD sample to the cognitive division of the ACC. The Talairach location of our finding (Table 2) overlaps that reported by Bush et al.; however, because of the low resolution of SPECT and the potential affective impact of the go/no-go task (frustration and anxiety), which can be greater in ADHD patients who are off MPH, we cannot assign our finding to the cognitive division of the ACC with certainty. We hypothesize that in the absence of MPH, higher ACC blood flow reflects a compensatory increase in task-related cognitive effort. Although we addressed some of the methodologic issues of ADHD-imaging studies by using an automated analysis of whole-brain images and a uniform active baseline activation state in a sizable sample, our results should be interpreted with several caveats. We studied an all-male cohort both because we wanted to achieve a clinically homogeneous sample and because of the difficulty in recruiting girls from a clinic-referred population (4,34). Therefore, our results may not apply to girls with ADHD. The duration of drug discontinuation was dictated by the lack of clinical evidence of tolerance to MPH, indicating that a period exceeding 5 MPH half-lives should render our subjects free of MPH effects (35). In contrast, the evidence of sensitization and tolerance to cocaine, which shares many pharmacologic properties with MPH, indicates that this issue requires further investigation (6,36). If tolerance to MPH exists, 36 h may not be enough for the striatum and the prefrontal cortex to revert to their pre-MPH state, explaining why we did not find an MPH effect there (28,37–39). Moreover, the effect of MPH withdrawal may obscure the effects of ADHD on the off-MPH rCBF pattern for both the location and the magnitude of differences between the off- and on-MPH scans. Thus, if there were withdrawal effects on rCBF beyond 36 h of abstinence, the effects of withdrawal could not be separated from the effects of ADHD. The MPH administration schedule in our study was also constrained by the inability to administer chronic MPH to the controls or to discontinue MPH for more than 36 h in the ADHD patients. Schedules of MPH administration in our 2 groups are comparable only under an assumption of no MPH effect beyond 36 h. The small sample size further limits the interpretability of the negative findings in the control group. Difficulties in recruiting healthy young children for brain imaging studies involving radiopharmaceuticals suggests that alternative methods, such as transcranial magnetic stimulation and fMRI, should be considered when studying these populations (16,34). Finally, our results were for a group, and no claims can be made about their predictive value in individuals. Recent advances in ligand design and image analysis indicate that SPECT studies of ADHD could move beyond blood flow to the imaging of dopamine, norepinephrine, and 5-hydroxytryptophane transporter ligands and pixel-based discriminant mapping methods, permitting sensitive and valid statistical comparison of individual patients with the control dataset (40,41).
CONCLUSION
SPM analysis of a sizable and well-characterized sample of prepubescent boys with ADHD showed that discontinuation of MPH treatment was associated with increased MC, premotor cortex, and ACC activity. These new findings are compatible with the phenomenology and prefrontostriatal deficit hypothesis of ADHD but suggest that additional mechanisms for the therapeutic action of MPH, such as intracortical inhibition, should be considered.
Acknowledgments
This study was supported in part by grants from the El Camino District Hospital Board and the National Institute on Drug Abuse.
Footnotes
Received Dec. 5, 2001; revision accepted May 17, 2002.
For correspondence or reprints contact: Daniel D. Langleben, MD, Treatment Research Center, 3900 Chestnut St., Philadelphia, PA 19104.
E-mail: langlebe{at}mail.med.upenn.edu
REFERENCES
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Association between long-term stimulant treatment and the functional brain response to methylphenidate in adolescents and adults with attention-deficit/hyperactivity disorder
- Proceed, with Caution: SPECT Cerebral Blood Flow Studies of Children and Adolescents with Attention Deficit Hyperactivity Disorder