


Abstract
The purpose of this study was to evaluate the usefulness of SPECT during temporary carotid balloon occlusion testing and to evaluate the changes in regional cerebral blood flow (CBF) and regional cerebral perfusion reserve (CPR) after permanent carotid occlusion. Methods: Temporary balloon occlusion testing was performed on 40 patients (24 head and neck tumors, 16 aneurysms). During the balloon occlusion (total time, 30 min), 99mTc-ethylcysteinate dimer (ECD) was injected intravenously about 5 min before balloon deflation, followed by SPECT data acquisition. SPECT images were visually evaluated, and the severity of hypoperfusion on the occluded side was classified using 4 grades (normal, mild, moderate, and severe). The count ratio of the occluded side to the contralateral side (L/N ratio) was also analyzed. In 7 patients who subsequently underwent permanent carotid occlusion, CBF and CPR were quantitatively assessed using 133Xe inhalation dynamic SPECT at rest and after acetazolamide (ACZ) enhancement (CPR was defined as the percentage increase in CBF after ACZ), and the patients were followed up periodically. Results: SPECT after temporary occlusion showed moderate or severe hypoperfusion in 12 patients, whereas neurologic deterioration was observed in only 4 patients. The L/N ratios were 0.96 ± 0.03 in normal perfusion (13 patients), 0.93 ± 0.03 in mild hypoperfusion (15 patients), 0.83 ± 0.03 in moderate hypoperfusion (10 patients) and 0.66 ± 0.09 in severe hypoperfusion (2 patients) (P < 0.0001). In the 7 patients who underwent permanent carotid occlusion, CPR decreased after surgery (35% ± 7% vs. 7% ± 14%, P < 0.05), even though the resting CBF did not change (54 ± 8 mL/100 g/min vs. 52 ± 6 mL/100 g/min, not statistically significant). The steal phenomenon (rCPR < 0%) was observed in 3 patients, 1 of whom experienced transient hemiparesis when blood pressure dropped soon after surgery. On follow-up, the decreased CPR gradually improved and no infarction developed. Conclusion: SPECT is useful to detect cerebral hypoperfusion during carotid occlusion. Assessment of CPR is recommended to predict the potential risk of postsurgical complications and to follow up patients after permanent carotid occlusion.
It may be necessary to sacrifice a carotid artery in the treatment of patients with head and neck tumors or cerebral aneurysms. It is thus essential to evaluate whether the patient can tolerate temporary or permanent carotid occlusion and to predict the potential risk before the surgical procedures. Balloon occlusion testing (BOT) is useful for evaluating whether patients will tolerate temporary or permanent carotid occlusion and has been considered to result in a decrease in postsurgical complications after carotid occlusion (1–3).
Measurement of cerebral blood flow (CBF) has revealed that substantial cerebral hypoperfusion may occur when a patient does not show any neurologic symptoms during BOT and may thus predict the potential risk after carotid occlusion (4–6). Among several methods of CBF studies, SPECT using 99mTc-hexamethylpropyleneamine oxime (HMPAO) or 99mTc-ethylcysteinate dimer (ECD) has been increasingly applied in conjunction with BOT, because both tracers—99mTc-HMPAO and 99mTc-ECD—rapidly distribute in the brain and the image is constant long after injection (7). SPECT images acquired after the completion of BOT might still reflect the CBF distribution during BOT when the tracer was injected.
However, reports have indicated that ischemic events or infarction can occur after permanent carotid occlusion in some patients considered to be tolerant of carotid occlusion by BOT with SPECT (3,4,8,9). Although the cause of these ischemic events seems to be either embolic or hemodynamic, how hemodynamic change may occur after permanent carotid occlusion has not been sufficiently clarified.
In this study, we retrospectively evaluated the results of 40 consecutive initial patients who underwent BOT. The purpose of this study was to evaluate the usefulness of brain SPECT during BOT and to quantitatively evaluate the changes in regional CBF and cerebral perfusion reserve (CPR) in patients who were tolerant of BOT and subsequently underwent permanent carotid occlusion.
MATERIALS AND METHODS
Forty patients, 38 men and 2 women, with head and neck tumors (24 patients) or cerebral aneurysms (16 patients) underwent BOT of the internal carotid artery (ICA) to evaluate brain tolerance to ICA sacrifice. Patient age ranged from 21 to 75 y, with a mean of 56 y. Written informed consent was obtained from all patients or their relatives after a detailed explanation of the test procedures.
BOT proceeded as follows: Before the start of BOT, we performed conventional angiography on 3 or 4 vessels (bilateral internal or common carotid arteries and unilateral or bilateral vertebral arteries) and evaluated the collateral circulation from the circle of Willis. Afterward, a 5-French balloon catheter was placed into the ICA and inflated until contrast medium no longer flowed through the site of balloon occlusion. The patient’s neurologic status was continuously evaluated, and when any neurologic symptom was observed the balloon was immediately deflated. If no neurologic symptom was observed, balloon occlusion was continued for a total of 30 min. Approximately 740 MBq (20 mCi) of 99mTc-ECD were injected intravenously 5 min before balloon deflation. In other words, the delay between the start of balloon inflation and 99mTc-ECD injection was usually 25 min, except for patients with positive symptoms during BOT (99mTc-ECD was injected as soon as possible when patients showed a neurologic symptom). SPECT data were acquired for usually about 30 min after the test was completed.
SPECT with 99mTc-ECD was performed using a 4-head gamma camera (SPECT 2000H-40; Hitachi, Tokyo, Japan) equipped with low-energy high-resolution collimators. Data were acquired at 20 s per view, using 64 views and a 64 × 64 matrix, and were reconstructed using Butterworth filtered backprojection with a slice thickness of 4 mm. Attenuation correction was performed by the method of Chang (10). The 99mTc-ECD SPECT images during BOT were visually evaluated by 2 experienced nuclear physicians, and the degree of cerebral perfusion in the occluded hemisphere was classified by consensus reading into 1 of 4 grades: normal (symmetric) perfusion, mild hypoperfusion, moderate hypoperfusion, and severe hypoperfusion. The radioactivity count ratio (L/N ratio) of the lesion (occluded) side to the contralateral normal side was calculated, and the value was compared with the visual classification. Although there are no strict criteria to define the degree of perfusion abnormalities, it is generally accepted that the areas of diminished perfusion are abnormal when the activity is less than 90% of normal (11). In this study, all the areas evaluated as moderate or severe hypoperfusion showed L/N ratios of less than 0.9. We therefore considered patients as being brain tolerant when they had no neurologic symptoms and the L/N ratio was greater than 0.9.
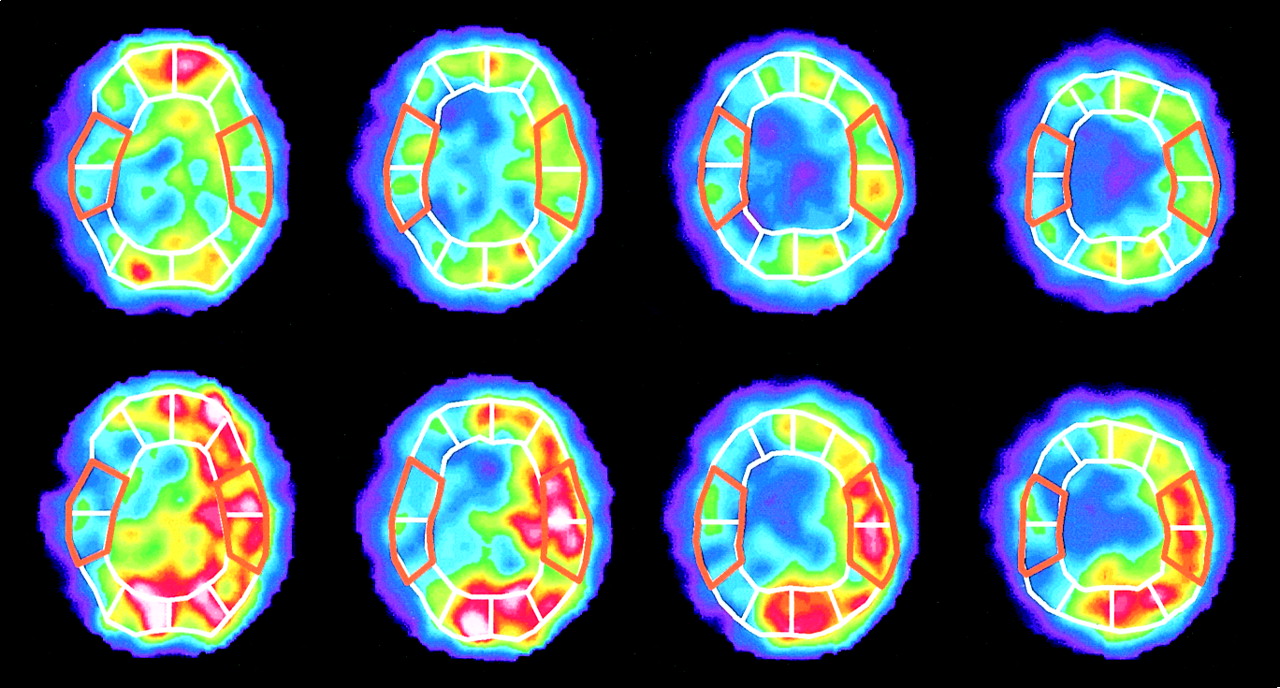
In 7 patients who were tolerant of BOT and subsequently underwent permanent carotid occlusion, quantitative measurements of CBF (in mL/100 g/min) using 133Xe inhalation methods were performed at rest and after enhancement with 1 g of acetazolamide (ACZ) (Diamox; Japan Wyeth Lederle Ltd., Tokyo, Japan). The CBF measurements were performed before and after permanent carotid occlusion and were repeated periodically during follow-up. Details of the methods of CBF measurement were described in 2 of our previous reports (12,13). In brief, patients inhaled 1.85 GBq of 133Xe gas and CBF was measured by dynamic SPECT (16 scans with a duration of 20 s each) according to the method of Kanno and Lassen (14). The CBF measurement was performed at rest and 15 min after intravenous injection of 1 g of ACZ. Both on the images at rest and on the images after ACZ, we placed a total of 12 regions of interest on the cerebral cortex approximately corresponding to the territories of the anterior cerebral artery, the middle cerebral artery (MCA), the posterior cerebral artery, and their border zones. In this study, we calculated the mean CBF in the MCA territories on the 4 topographic planes of the basal ganglia through the centrum semiovale (Fig. 1). The CPR was defined as the percentage increase in CBF after ACZ challenging. In our institute, the mean values of CBF and CPR in the MCA territories were 50.9 ± 3.9 mL/100 g/min and 40.8% ± 12.7%, which were obtained from 7 patients with nonruptured aneurysms (mean age, 59 ± 8 y) who had no neurologic deficit and no infarction on CT or MRI (12). According to these normal values, we defined the lower limits of the normal range (mean − 2 SDs) of CBF and CPR as 43 mL/100 g/min and 15%, respectively. The values of CBF and CPR were compared before and after permanent carotid occlusion by means of the Wilcoxon signed rank test, and P values less than 0.05 were considered significant.
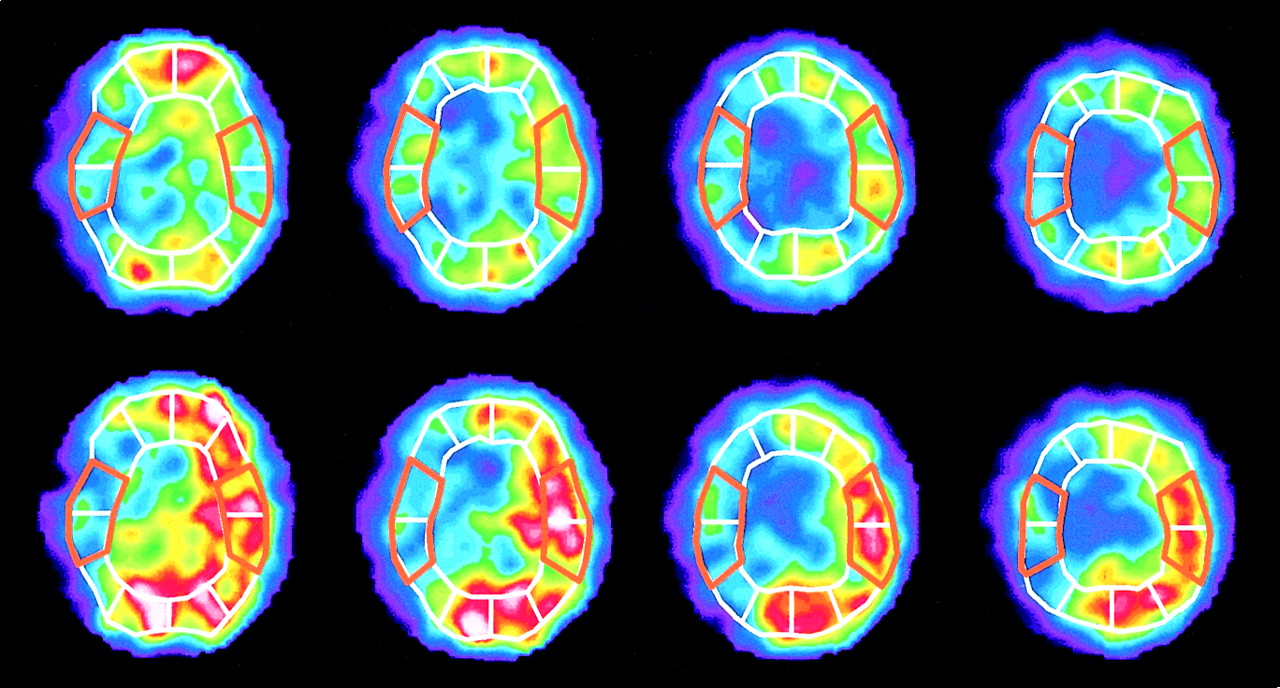
133Xe CBF images at rest (top row) and after ACZ enhancement (bottom row) with placement of regions of interest. Mean CBF is calculated in MCA territories on 4 slices from basal ganglia through centrum semiovale. CPR is defined as percentage increase in CBF after ACZ enhancement, or CPR = [(CBF [ACZ] − CBF [rest])/CBF (rest)] × 100 (%).
RESULTS
On angiography, cross-flow from the anterior communicating artery was good in 33 patients. In the other 7 patients, cross-flow from the anterior communicating artery was not good, but flow from the posterior communicating artery was good. Only 1 of these 7 patients showed transient symptoms (dysarthria and blindness), but the symptoms promptly disappeared.
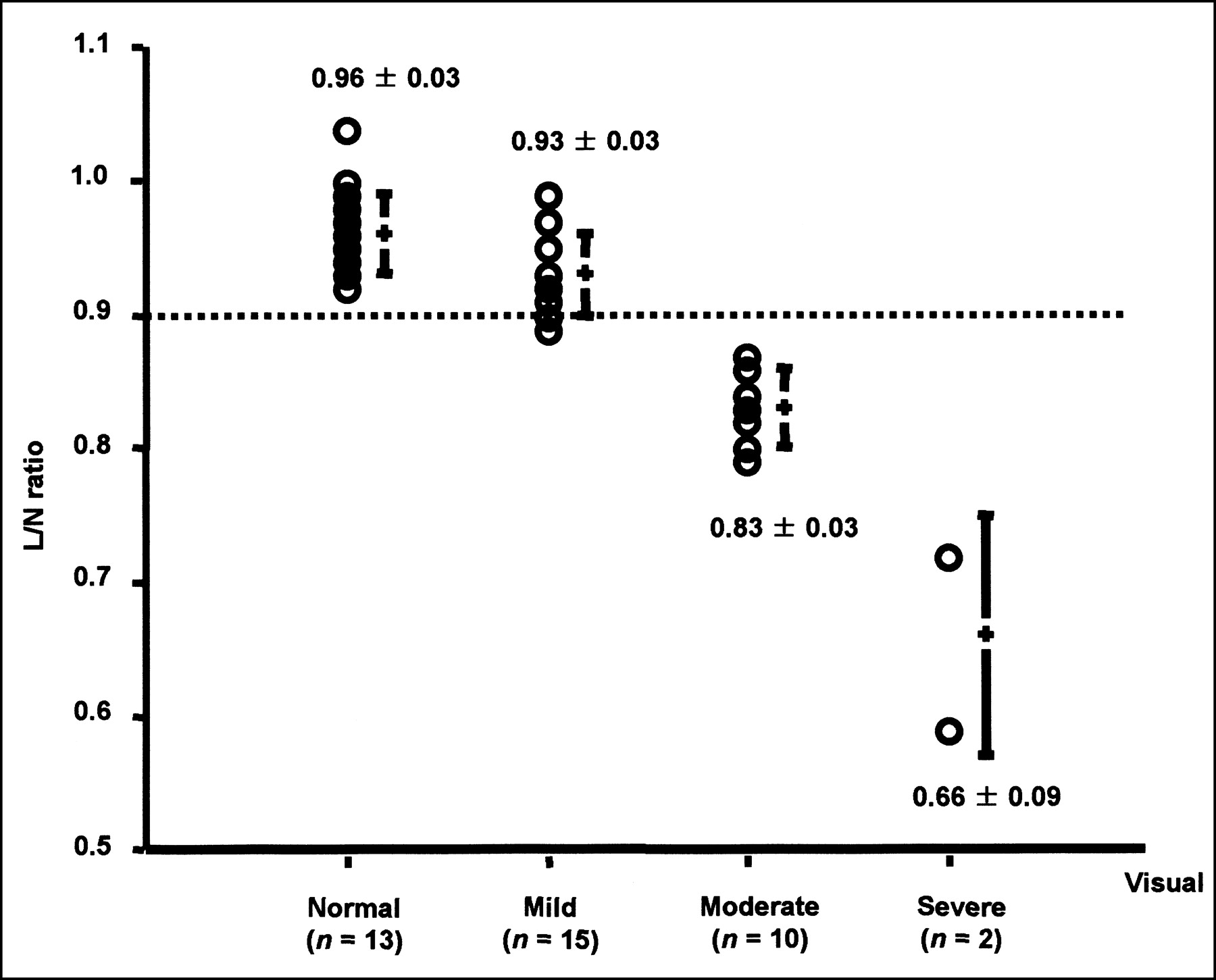
During BOT, neurologic symptoms were observed in only 4 patients, whereas 99mTc-ECD SPECT showed moderate or severe hypoperfusion in 10 of 36 patients (28%) who showed no neurologic symptoms during BOT (Table 1). Among the 14 patients with abnormal BOT results (symptom positive in 4 patients, symptom negative but SPECT positive in 10 patients), 9 patients had head and neck tumors (pharynx, 4; maxillary sinus, 1; ethmoid sinus, 1; brain, 1; neck tumor with unknown origin, 2). The other 5 patients had ICA aneurysms in the carotid siphon, including 1 with an aneurysm of the ICA and ophthalmic artery. The L/N ratios were 0.96 ± 0.03 in normal perfusion (13 patients), 0.93 ± 0.03 in mild hypoperfusion (15 patients), 0.83 ± 0.03 in moderate hypoperfusion (10 patients), and 0.66 ± 0.09 in severe hypoperfusion (2 patients) (P < 0.0001; Fig. 2).
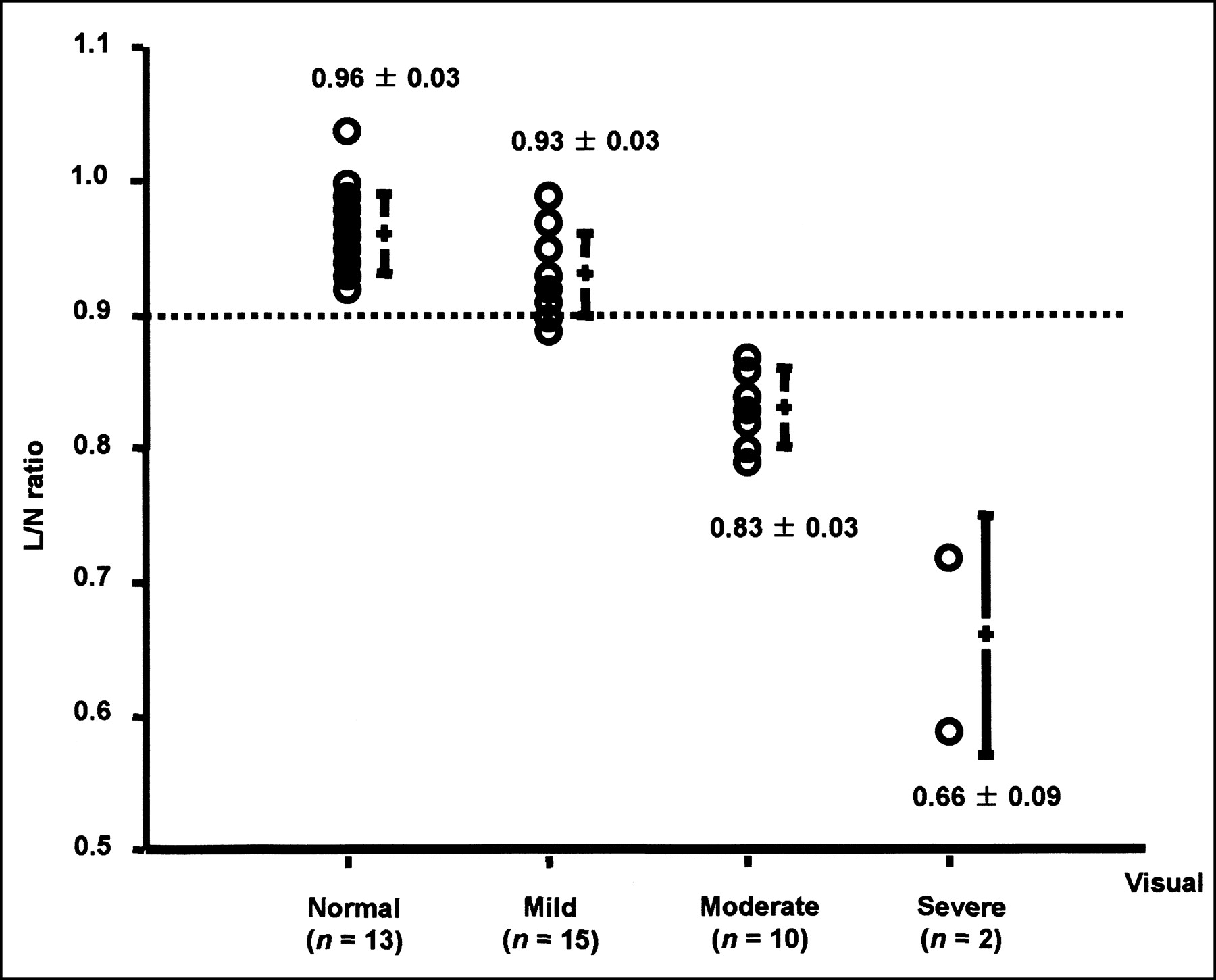
Comparisons of visual analysis and L/N ratio. Visual interpretation agrees well with L/N ratio. All cases of moderate or severe hypoperfusion show L/N ratios less than 0.9.
Symptoms and SPECT Findings During Balloon Occlusion Test
Baseline 99mTc-ECD SPECT was performed on only 6 patients. Of these 6 patients, only 1 patient with brain tumor showed slightly decreased cerebral perfusion (L/N ratio of 0.9) on the tumor side. Baseline SPECT in the other 5 patients showed normal symmetric perfusion.
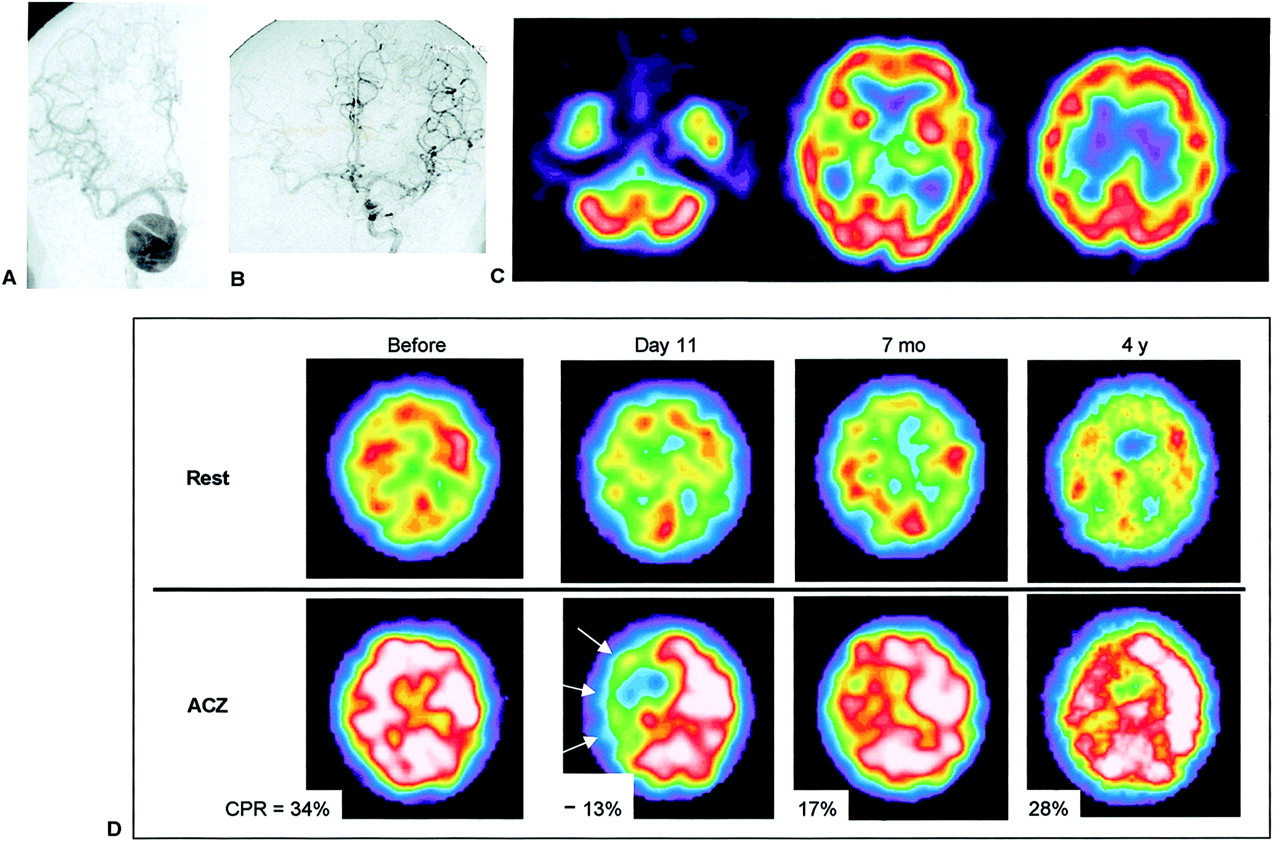
If feasible during surgery, preservation of the carotid artery was a priority. Of 21 patients with negative BOT who did not undergo permanent carotid occlusion, 17 patients were successfully treated without carotid sacrifice. Planned surgery was finally refused by the patients and their relatives in 2 instances, and the reconstruction surgeries were performed on 2 patients despite their testing negative. Finally, 7 patients who were tolerant of BOT subsequently underwent permanent carotid occlusion. Clinical information on these 7 patients is summarized in Table 2. In one patient (patient 4), a transient hemiparesis occurred soon after permanent occlusion of the right ICA when blood pressure dropped (Fig. 3). In another patient (patient 5), a small infarction that was probably due to a small thromboembolism was incidentally detected on follow-up MRI. No permanent neurologic deficit was observed in any patient.
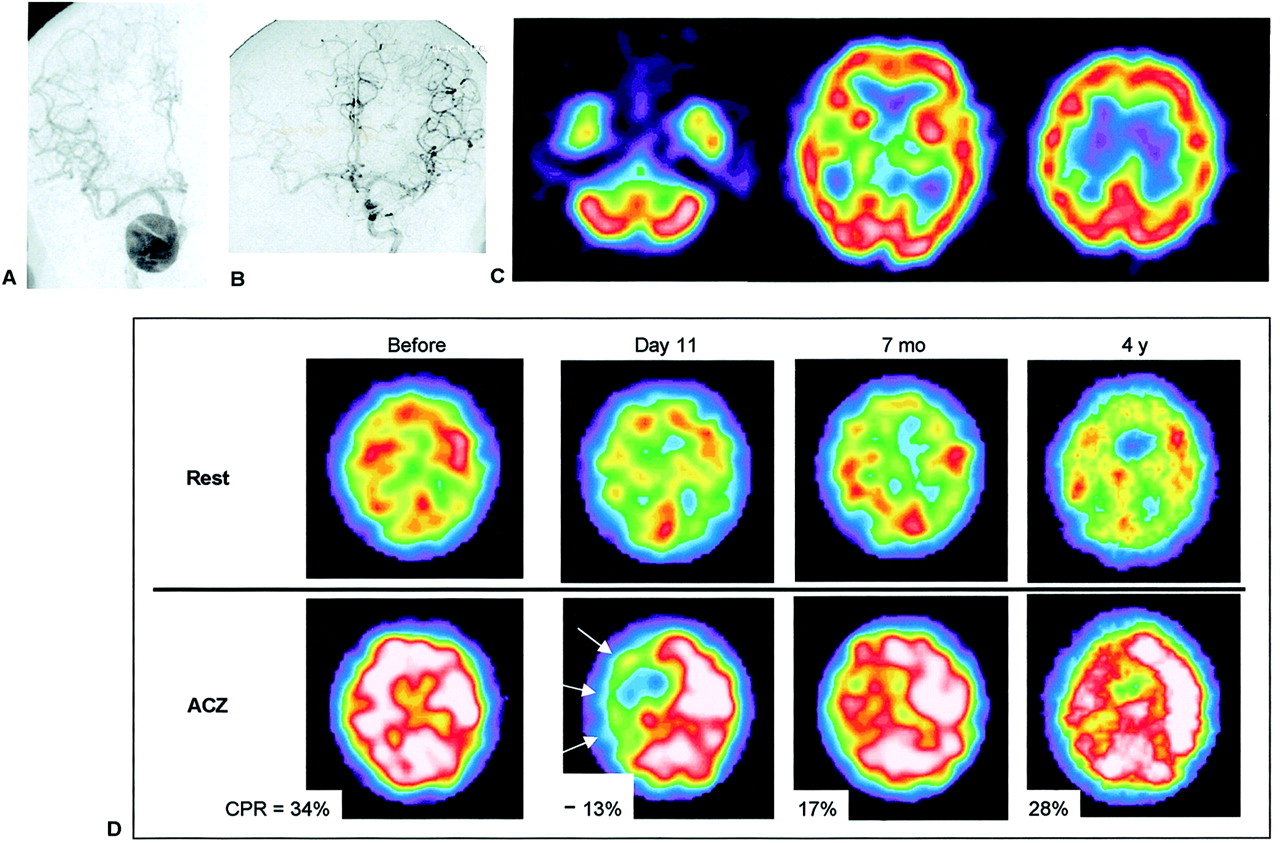
A 63-y-old woman (patient 4) with giant aneurysm of right ICA. (A) Right ICA angiogram shows giant aneurysm in carotid siphon. (B) Left ICA angiogram during BOT of right ICA shows good collateral cross-flow. (C) 99mTc-ECD SPECT images demonstrate symmetric cerebral uptake (L/N of 0.96), and no neurologic symptoms were observed. This patient was considered to be tolerant of carotid occlusion. However, after proximal occlusion of right ICA, she showed transient left hemiparesis when her blood pressure dropped. Her hemiparesis disappeared immediately after injection of vasoconstrictor, and no infarction developed. (D) 133Xe-CBF SPECT revealed normal CBF at rest but decreased CPR in right cerebral hemisphere (mean CPR in right MCA territory was −13% on day 11) (arrows). On follow-up, impaired CPR gradually improved.
Patients with Permanent Carotid Occlusion
The values for CBF and CPR before and after permanent carotid occlusion are shown in Figure 4. The resting CBF decreased a little after permanent carotid occlusion (from 54 ± 8 mL/100 g/min to 52 ± 6 mL/100 g/min), and both CBF before occlusion and CBF after occlusion were within the normal range. In contrast, CPR significantly decreased after permanent carotid occlusion (from 35% ± 7% to 7% ± 14%, P < 0.05). In 5 of 7 patients, CPR decreased below the normal range, and the steal phenomenon (rCPR < 0%) was observed in 3 patients.
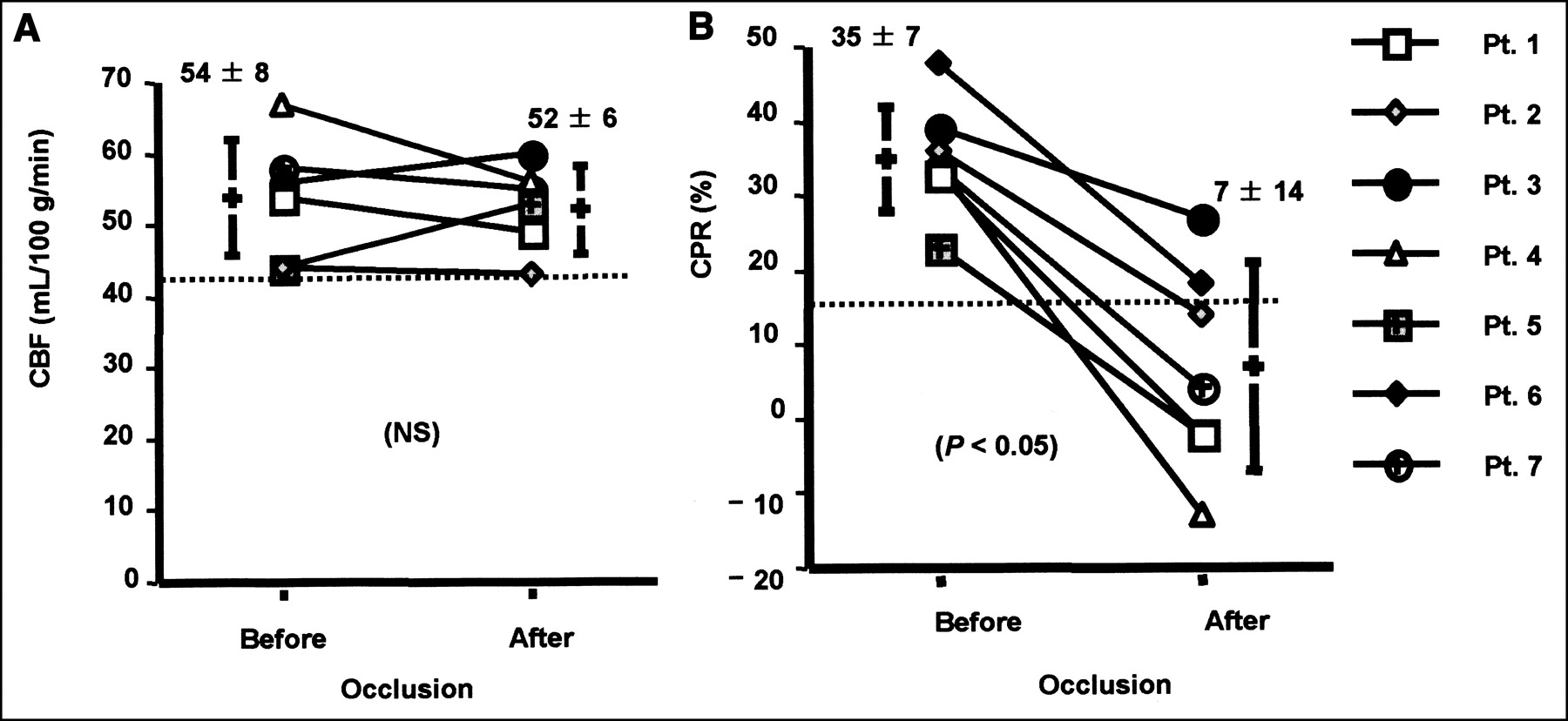
Comparisons of CBF and CPR before and after permanent carotid occlusion. (A) CBF changed slightly (54 ± 8 mL/100 g/min vs. 52 ± 6 mL/100 g/min, not significant (NS)). (B) CPR significantly decreased in all patients after permanent carotid occlusion (35% ± 7% vs. 7% ± 14%, P < 0.05). In 5 of 7 patients, CPR decreased below normal range (CPR < 15%), and steal phenomenon was observed in 3 patients.
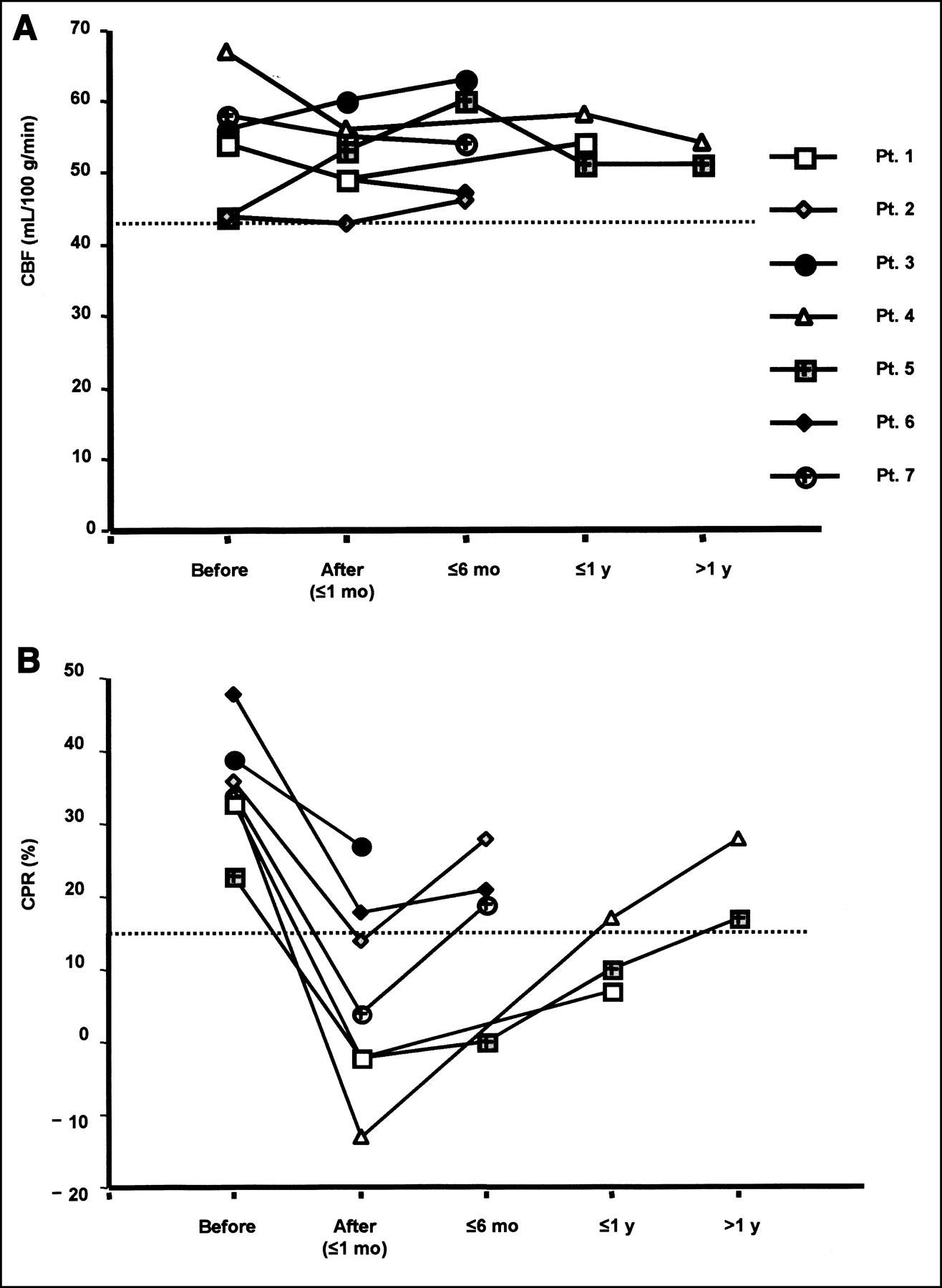
On follow-up, the CBF values varied a little but remained within the normal range. In contrast, the decreased CPR gradually improved on follow-up (until approximately 4 y) after permanent carotid occlusion (Fig. 5).
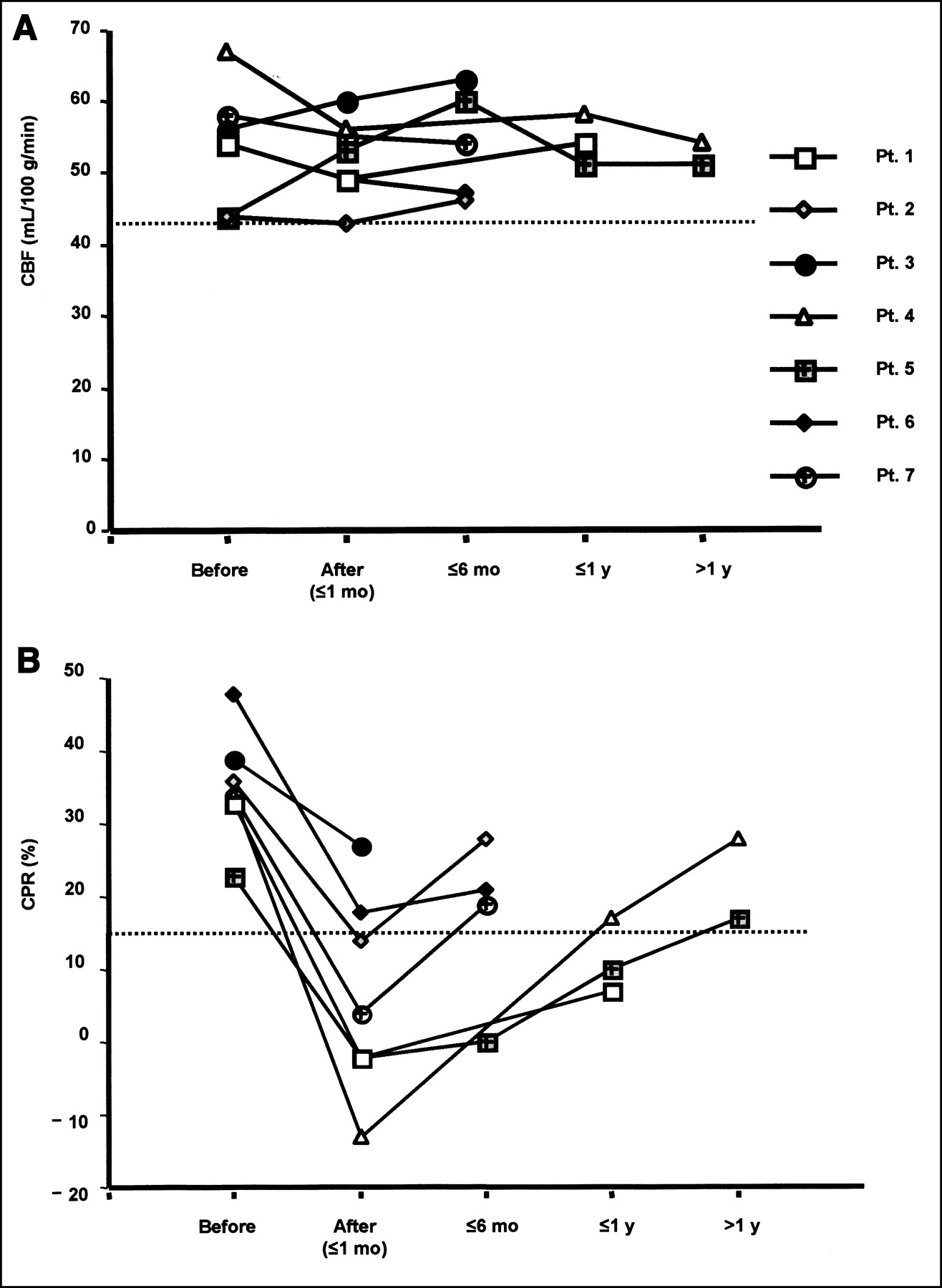
Changes in CBF and CPR on follow-up after permanent carotid occlusion. (A) CBF changed within normal range (CBF ≥ 43 mL/100 g/min). (B) In contrast, decreased CPR gradually improved after permanent carotid occlusion.
DISCUSSION
99mTc-ECD SPECT was useful for detecting hypoperfusion during BOT. In the current study, 99mTc-ECD SPECT showed moderate or severe hypoperfusion in 10 of 36 patients (28%) who showed no neurologic symptoms during BOT. This result is similar to previous findings (5,6). Simonson et al. (5) reported that 5 of 11 asymptomatic patients (45%) had decreased perfusion on 99mTc-HMPAO SPECT. Mathews et al. (6) also reported that 9 of 34 patients (26%) showed only perfusion defects on 99mTc-HMPAO SPECT. Thus, brain SPECT can depict clinically silent areas of decreased cerebral perfusion associated with asymptomatic BOT.
Previously, Nishioka (15) reported that nonselective occlusion of a carotid artery carried a 30% risk of ischemia of the ipsilateral hemisphere. Inadequate collateral circulation and thromboembolism are thought to be the 2 mechanisms causing ischemic complications (16). Although BOT cannot predict the risk of thromboembolism, which is a significant cause of delayed cerebral ischemia after carotid occlusion (8), inadequate collateral circulation (i.e., a cause of hemodynamic ischemia) should be detected by BOT before permanent occlusion to reduce the risk of ischemic complications. In reviewing the literature, Linskey et al. (3) reported that the risk of ischemic complications was reduced to 13% by selective carotid occlusion using BOT.
Because the distribution of 99mTc-labeled CBF tracers (99mTc-HMPAO and 99mTc-ECD) in the brain is stable after the first 5 min after injection, SPECT acquisition can be performed after completion of the test (i.e., still keeping a snapshot of the CBF image at the time of injection) (7). In this study, we preferred to use 99mTc-ECD rather than 99mTc-HMPAO, since the radiochemical purity and the stability of 99mTc-ECD are better than those of 99mTc-HMPAO after 30 min after the preparation (17,18). The excellent characteristics of 99mTc-ECD thus enable injection of the tracer at any time during 30 min of BOT. The tracer could be injected as soon as possible when any symptom developed during BOT, and we could confirm the location and magnitude of CBF reduction during BOT.
Baseline 99mTc-ECD SPECT was performed on only 6 patients in the current study. In these 6 patients, baseline SPECT showed normal symmetric perfusion, except for a patient with a brain tumor. Lorberboym et al. (8) also reported that all baseline studies (performed on 15/44 patients in their study) showed normal symmetric perfusion. Thus, although not performed in the current study and seemingly not necessary in all patient, baseline SPECT may be helpful to evaluate how CBF changed from the baseline condition during BOT. We would recommend that baseline SPECT be performed when abnormal perfusion is highly suspected at baseline and when abnormal or unexplainable findings are observed on SPECT during BOT.
Although no definite quantitative criteria are available to define perfusion abnormalities, an interhemispheric difference in activity greater than 10% (i.e., L/N ratio < 0.9) is generally accepted to be asymmetric (8,11). Monsein et al. (11) seemed to consider a 10% difference to be of high importance, and symmetric perfusion (L/N ratio ≥ 0.9) during BOT suggested brain tolerance against carotid occlusion. Palestro et al. (19) reported that the negative predictive value of symmetric perfusion (L/N ratio ≥ 0.9) during BOT was 100% in 14 patients who underwent carotid occlusion. When these reports are combined, the predictive value of negative (symmetric) SPECT findings for a satisfactory outcome after permanent carotid occlusion ranges from approximately 80% to 100% (4,11,19–21).
However, as shown in Figure 3, CPR decreased after carotid occlusion even though resting CBF did not change. In these settings, an ischemic event might occur when cerebral perfusion pressure drops. Thus, some patients with normal CBF during BOT may still have a risk of ischemic events after permanent carotid occlusion because of reduced CPR. In the current study, CPR was reduced in all patients, even though resting CBF was within the normal range after permanent carotid occlusion. Five of 7 patients (71%) showed subnormal CPR (<15%), and 3 of 7 patients (43%) showed the steal phenomenon.
Recently, an additional hypotensive challenge during BOT has been reported to be useful for decreasing the false-negative rate (21–24). Standard et al. (23) reported that 4 of 47 patients (9%) showed neurologic deficits during normotensive BOT, whereas 9 of the remaining 43 patients (21%) showed deficits during hypotensive BOT. The usefulness of the hypotensive challenge is still controversial. Its specificity may be decreased because of the addition of an unknown increased number of false-positive cases. However, the true rate of true-positives or false-positives is unknown, since patients may be successfully treated without carotid sacrifice or patients who test positive may undergo unnecessary revascularization. Despite these limitations, Standard et al. recommended hypotensive challenge during BOT, since the additional morbidity and mortality associated with revascularization procedures are low (3%–5%) and are preferable to the increased morbidity of hemispheric stroke associated with carotid occlusion.
Nishioka (15) reported that 89% of ischemic complications occurred within 96 h after carotid occlusion. In the current analysis, CPR substantially decreased early after permanent carotid occlusion and then gradually improved over several years (Fig. 5). This finding indicates that the risk of hemodynamic ischemia is also higher early after occlusion than late after occlusion. These observations emphasize that we should monitor patients carefully, especially early after carotid occlusion.
Reduced CPR can spontaneously improve on follow-up. Coyle and Panzenbeck (25) reported, for an experimental rat study, that a significant increase in the diameter of the anterior communicating artery occurred 6 wk after ligation of the ipsilateral carotid artery. This finding suggested that collateral circulation can rapidly develop after permanent carotid occlusion. However, little is known about how rapidly collateral circulation develops in humans after carotid occlusion. Widder et al. (26) reported a spontaneous improvement in CO2 reactivity over 5 y in 64% of patients with carotid occlusion. By semiquantitative analysis (by asymmetric index) using 123I-iodoamphetamine and ACZ, Hasegawa et al. (27) reported that sequential changes in hemodynamic reserve were observed in patients with major cerebral arterial occlusive disease, and Cao et al. (28) similarly reported that a spontaneous normalization in reduced vasodilatory capacity was observed on follow-up in 8 of 20 patients (40%) with major cerebral arterial occlusive disease. However, Cao et al. reported that reduced CPR was more likely to improve in patients with initially mildly reduced ACZ reactivity and with stenosis but not occlusion. In the current study, however, improvement in reduced CPR was observed in all patients with permanent carotid occlusion on follow-up, although the timing and magnitude of improvement varied widely.
Studies have shown that patients with highly impaired CPR and increased oxygen extraction fraction have an increased risk of developing stroke (29,30). In our study, a transient ischemic complication occurred soon after permanent carotid occlusion in 1 of 3 patients with the steal phenomenon after permanent carotid occlusion. It is important to periodically examine CBF and CPR in patients after permanent carotid occlusion, since the timing and magnitude of improvement in reduced CPR varies among patients.
CONCLUSION
Brain SPECT is useful for evaluating brain tolerance to carotid occlusion and is sensitive in detecting subclinical hypoperfusion during temporary BOT. Assessment of CPR is recommended in order to predict the potential risk of hemodynamic ischemia and to follow up patients after permanent carotid occlusion.
Acknowledgments
The authors thank the staff of the Departments of Radiology and Neurological Surgery at Ehime University School of Medicine. This article was presented, in part, at the 48th annual meeting of the Society of Nuclear Medicine; Toronto, Ontario, Canada; June 2001.
Footnotes
Received Mar. 15, 2002; revision accepted Jul. 26, 2002.
For correspondence or reprints contact: Yoshifumi Sugawara, MD, Department of Radiology, Ehime University School of Medicine, Shitsukawa, Shigenobu-cho, Onsen-gun, Ehime 791-0295, Japan.
E-mail: sugawara{at}m.ehime-u.ac.jp




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}