


Abstract
SPECT has the potential to add valuable information to the diagnosis and management of central nervous system (CNS) malignancy. Radioactive tracers including 99mTc-methoxyisobutylisonitrile (MIBI), or sestamibi, have been shown to be sensitive markers for brain tumors; however, their role in imaging children is poorly defined. Methods: We undertook a pilot study of 29 pairs of 99mTc-MIBI and MRI images from 20 children to explore the clinical usefulness of this tracer in CNS malignancy. Results: Tumor types that took up 99mTc-MIBI included brain stem glioma, fibrillary astrocytoma, other low-grade astrocytomas, and glioblastoma multiforme. Most tumors positive for 99mTc-MIBI uptake were astrocytomas, including those in the brain stem, cerebellum, and cortex. This method of nuclear imaging not only was able to identify the presence of a tumor but also could identify changes in the same tumor over time. Some correlation between histologic grade and 99mTc-MIBI uptake was observed. Several tumors, including craniopharyngioma, medulloblastoma, and optic glioma, were evident on MRI but not on 99mTc-MIBI SPECT. Conclusion: The results suggest that this modality is a potentially useful tool in the diagnosis and management of CNS malignancies, particularly higher-grade astrocytomas, in children.
Accurate neuroimaging can assist in the diagnosis, management, prognosis, and follow-up of central nervous system (CNS) malignancies in children. SPECT has been established as a potentially useful tool for the assessment of brain tumors (1–7). In adults with gliomas, SPECT using 201Tl has been applied to help differentiate between residual tumor and radiation necrosis (8) and predict the histologic grade (6)—information not easily attainable by MRI alone. Although some studies have suggested a similar usefulness for thallium SPECT in childhood brain tumors (9), other prospective studies have failed to demonstrate any clinical advantage over MRI (10).
99mTc-methoxyisobutylisonitrile (MIBI), or sestamibi, has been suggested to offer advantages over thallium for imaging of brain tumors (11). This molecule does not penetrate the intact blood-brain barrier. It is taken up by normal choroid plexus, pituitary, scalp, and nasopharyngeal tissues (2,11–13).
99mTc-MIBI uptake by viable tumor cells and brain malignancies is well established (2,9,14–16). Carcinoma cell lines accumulate 9 times more 99mTc-MIBI than do normal cell lines (17), and it is concentrated by numerous other human neoplasms (18,19). Human brain malignancies shown to accumulate 99mTc-MIBI include astrocytoma (11,20), acoustic schwannoma (13,21), CNS lymphoma (20), meningioma (11,13,22), metastatic brain tumors (23), and choroid plexus carcinoma (14).
99mTc-MIBI SPECT can add valuable information to CT for the differentiation of radiation necrosis from recurrent disease in adult brain malignancy (24). Despite the potential advantages and some experience with 99mTc-MIBI SPECT in children, a clear advantage over other modalities, including 201Tl SPECT, in imaging brain tumors has not been established (2,9,25,26).
We undertook a pilot study of 20 children with a variety of brain tumors to investigate the clinical utility of 99mTc-MIBI imaging in comparison with standard MRI methods. Our results provided evidence from a group of pediatric patients that this modality may be a potentially useful tool in the diagnosis, management, and follow-up of specific CNS malignancies of childhood.
MATERIALS AND METHODS
Patients
SPECT with 99mTc-MIBI and gadolinium-enhanced MRI were completed on 20 children with CNS malignancy. Informed consent was obtained from all parents or legal guardians. The study was approved by the ethics review committee at the Alberta Children’s Hospital. All eligible patients were sequentially enrolled and followed through the Southern Alberta Cancer Clinic and imaged between 1997 and 2000. Diagnoses were confirmed histologically with the exception of 4 brain stem gliomas, for which diagnosis was made radiologically. The longest time between MRI and 99mTc-MIBI imaging was 2 wk (1 patient), with the majority of study pairings being completed either the same day or within 72 h (mean ± SD, 1.2 ± 0.4 d). All but 3 study pairings were completed within 72 h. Several children received multiple pairs of MRI and 99mTc-MIBI scans, with 29 pairs of images being completed in total.
Imaging
Each patient was given an intravenous injection of 99mTc-MIBI at a dose calculated as body surface area divided by 1.73 and then multiplied by the adult dose of 1,000 MBq. Imaging was initiated 10–15 min later using a triple-head gamma camera (model 3000; Marconi Medical Systems, Cleveland, OH) equipped with low-energy, high-resolution collimators. The acquisition time was approximately 30 min. Reconstruction was by filtered backprojection, and images had a side thickness of 7 mm.
MR images were obtained on a 1.5-T unit with standard techniques. T1-weighted, T2-weighted, flare, and gadolinium-enhanced scans were obtained in multiple planes for all patients. These included axial, coronal, and sagittal projections that could easily be correlated with sestamibi images of the same views.
Image Analysis
99mTc-MIBI scans were analyzed and interpreted by the same nuclear medicine specialist who completed the scans. Gadolinium-enhanced MR images were analyzed by a neuroradiology specialist from the same institution. For the purposes of this study, both types of images were interpreted as either showing or not showing definitive evidence of a tumor. For cases in which repeated imaging was obtained, any evidence of an interval change from the previous set of scans was also noted. For all images, variables that were reported included tumor size, location, extent, contrast enhancement, vascular supply, and morphologic features such as solid versus cystic appearance.
Progression of tumor was determined clinically when a patient showed definitive signs of disease progression between scans. Definitive signs of progression included obvious clinical deterioration on examination or death directly attributable to the brain tumor.
RESULTS
A total of 29 pairs of MRI and 99mTc-MIBI scans from 20 children with CNS malignancy were included in the study. Age, sex, diagnosis, and tumor location are summarized in Table 1. The mean age of the children was 9.9 ± 4.4 y, and the age range was 5–17 y. This population included 12 boys and 8 girls.
Patient Profiles, Tumor Type, and Location
A wide variety of pediatric brain neoplasms took up 99mTc-MIBI. As summarized in Table 2, these included brain stem gliomas, pilocytic astrocytoma, glioblastoma multiforme, and choroid plexus carcinoma. Tumors with no demonstrable uptake of 99mTc-MIBI when tumor was evident on MRI included optic glioma, medulloblastoma, desmoplastic neuroepithelial tumor, craniopharyngioma, spinal anaplastic astrocytoma, low-grade astrocytoma, and ependymoma. Therefore, of the 29 sestamibi studies completed, 13 were true-positive, 13 were false-negative, and 3 were true-negative when positive MRI findings were used as definitive evidence of tumor. A false-negative result indicated either that no significant amount of radiotracer was taken up by the tumor or that the radiotracer had subsequently been expelled from the tumor at the time of imaging. In no instance was a positive 99mTc-MIBI result accompanied by a negative MRI result.
Tumor Histology, Grade, and Results of 99mTc-MIBI Imaging and MRI
An example of a positive sestamibi scan is shown in Figure 1, which depicts both the gadolinium-enhanced T1- and T2-weighted MR images and the 99mTc-MIBI SPECT images for patient 9, a 13-y-old girl with a glioblastoma multiforme tumor of the right frontotemporal region. In this patient, a close morphologic correlation was observed between the positive 99mTc-MIBI image and both MR images. MR and SPECT images of a brain stem glioma can be seen in Figure 2.

Glioblastoma multiforme of right frontotemporal region, revealed on T1-weighted MRI with gadolinium (A) and T2-weighted MRI (B), is also well defined on sestamibi scan (C).
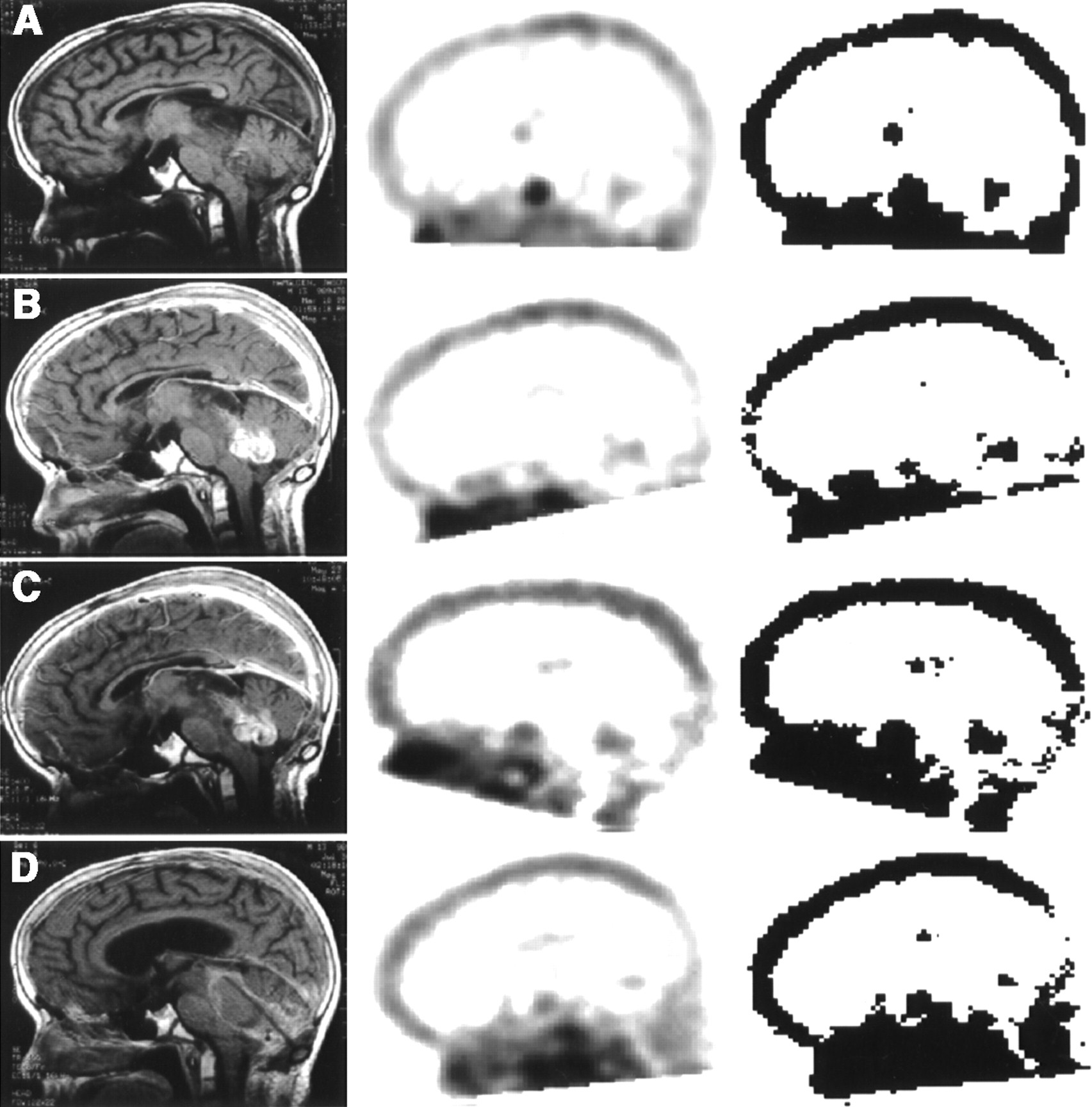
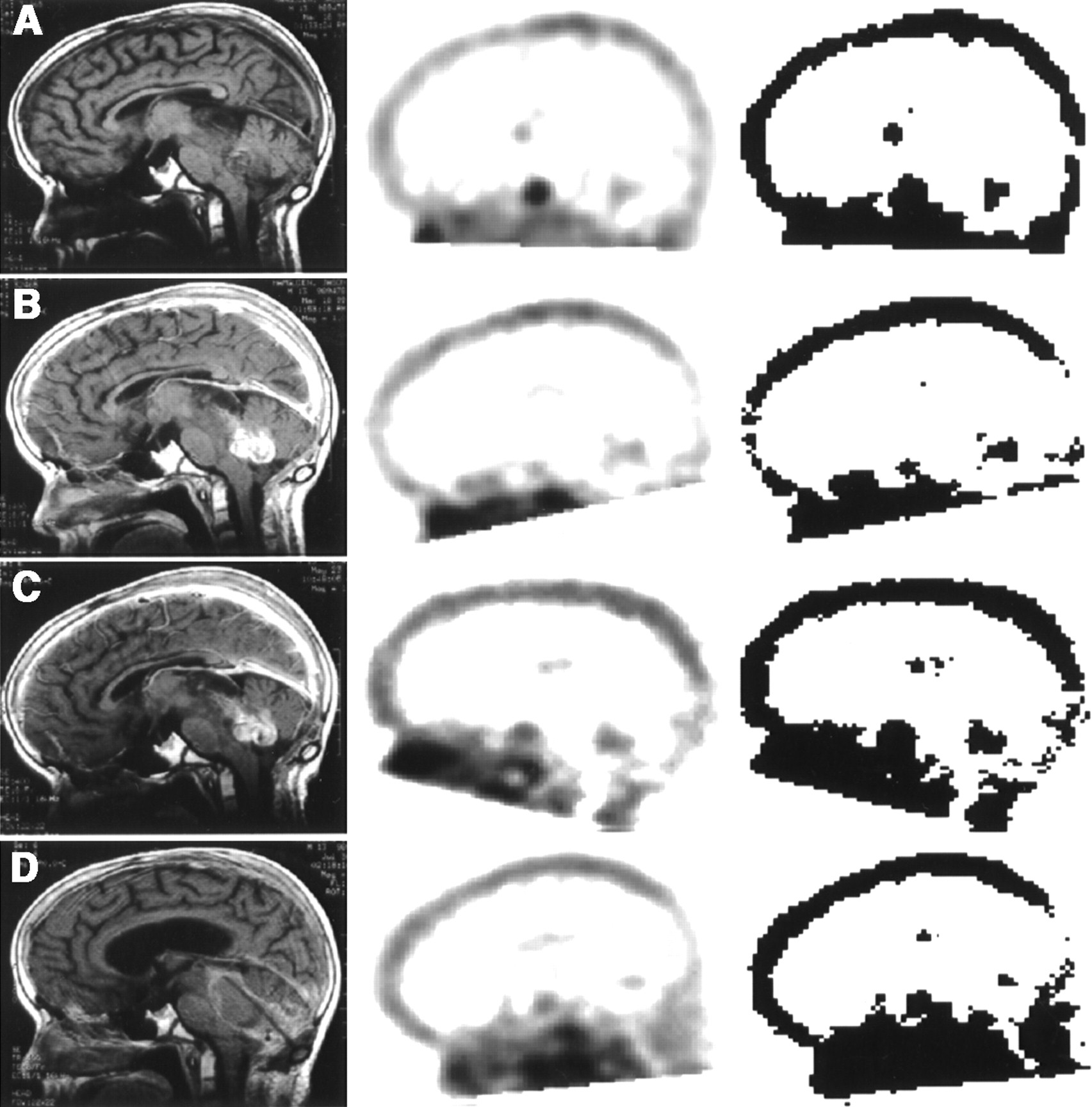
Serial pairings of sagittal MRI and SPECT images for 15-y-old boy with exophytic brain stem glioma. Third column is black-and-white version of original SPECT images. Baseline images (A) are compared with scans at 8 (B) and 12 (C) mo, both of which show increased signal on 99mTc-MIBI SPECT but no change on MRI. Final panel (D) demonstrates increased tumor on MRI at 16 mo, accompanied by decreased signal from SPECT.
Astrocytomas constituted the largest proportion of tumors in this group of children (23 pairs of scans from 15 children). Uptake of sestamibi appeared to depend in part on the histologic grade of the tumor. Of the 9 patients with intracranial astrocytomas for which histologic grading was available, 4 failed to demonstrate any positive sestamibi scans. In all of these cases, tumors were of grade I or II. Conversely, both patients with grade IV astrocytomas had positive sestamibi scans. Furthermore, of the remaining 7 nonastrocytoma tumors, the only positive sestamibi scans were in a patient with a high-grade (III) choroid plexus carcinoma.
Brain stem gliomas were the most consistently positive type of tumor in our limited sample, with 5 of 8 cases demonstrating uptake of the sestamibi tracer. All 3 of the brain stem gliomas that had negative sestamibi scans were located in the midbrain.
Normal cranial structures found to take up 99mTc-MIBI in this group of patients included the choroid plexus and the pituitary gland. In none of the 20 tumors imaged did this uptake by normal tissues interfere with the interpretation of the scan. Only 1 case of spinal cord tumor was included, and it failed to show up on SPECT despite its high grade.
Multiple pairs of MR and 99mTc-MIBI images were available for 6 children. A summary of the respective changes in both modes of imaging, the time course of these changes, and the progression or nonprogression of their illness is included in Table 3. In 2 of these 6 patients, sestamibi images remained negative at all times. In the remaining 4 patients, sestamibi activity was found to correlate well with changes found on MRI over the same period. Furthermore, in patient 3, increased tumor was noted on 2 consecutive sestamibi scans when MRI done at the same time revealed no interval change. On the final pairing for this patient, this trend was reversed: Increased tumor was noted on MRI, whereas the sestamibi scan showed decreased tumor. This progression is illustrated in Figure 2, which shows pairings of MR and SPECT images from time zero through 8, 12, and 16 mo, respectively. Throughout these changes, clinical evidence of disease progression was not seen until a few days before this child died. Therefore, the sestamibi scan was the first to show tumor progression, followed by MRI and finally by clinical signs.
Chronologic Changes in 99mTc-MIBI and MRI Results
DISCUSSION
Our results demonstrate the potential of 99mTc-MIBI to image many pediatric brain tumors. A positive SPECT scan using this tracer appears to depend in part on tumor histology, including both the type and the histologic grade of the tumor. Although MRI appears to be superior in many cases, the lack of consistent correlation that we observed between MRI and SPECT suggests that unique information may be available from each mode of imaging.
99mTc-MIBI is established as a marker of CNS malignancy (2,11,14,16,24–27), but further data are necessary to clarify the role in specific tumor types and the clinical value when these patients are followed over time. In our series, 9 of 20 lesions were positive, including both low-grade and high-grade astrocytic tumors. This finding is consistent with adult data showing positivity for multiple tumor types, including astrocytoma (11,20) and meningioma (11,13,22). However, in our study group, 11 of 20 tumors evident on MRI were not evident on SPECT. Those diagnoses included craniopharyngioma, ependymoma, desmoplastic neuroepithelial tumor, medulloblastoma, and some low-grade gliomas. This finding suggests a selectivity in tracer uptake or extrusion, which might be due to several factors. Regional blood flow, blood-brain barrier (BBB) permeability, tumor cell membrane adenosine triphosphatase pump, and mitochondrial content may influence uptake of radiotracers (5). Tracer needs to reach the tumor cells first through the bloodstream, and a correlation between cerebral blood flow and 99mTc-MIBI reactivity has been shown previously (27). The tracer must then leave the vascular lumen and cross the BBB. The inability of 99mTc-MIBI to enhance normal structures within the brain aside from the choroid plexus supports the importance BBB integrity.
In addition to being sealed by tight junctions, BBB endothelial cells also express the multidrug resistance 1 gene, the product of which is an adenosine triphosphatase membrane pump extruding a variety of toxins from the cells. 99mTc-MIBI is one of these substrates (16). Inhibition of multidrug resistance has been shown to delay excretion of 99mTc-MIBI (28). Without inhibition, the pump prevents the tracer from reaching the interstitial space. Choroid plexus tissue, the vasculature of which expresses neither tight junctions nor multidrug resistance 1, accumulates 99mTc-MIBI, supporting this concept. Consequently, tumors arising from this tissue are 99mTc-MIBI positive as well (14).
The next barrier that the tracer must pass to enter tumor cells is the cell membrane. Passage through the cell membrane may be influenced by several factors, including multidrug resistance, mentioned above. In addition, both regional blood flow distribution and mitochondrial oxidation capacity correlated well with 99mTc-MIBI uptake in cardiac myocytes (29,30). Intracellular parameters may also determine 99mTc-MIBI accumulation, which occurs in both mitochondria and cytosol, as well as in association with specific cellular proteins (31). In tumor cell lines, most 99mTc-MIBI has been demonstrated to associate with the mitochondria (32). Therefore, metabolically active and highly malignant tumors may be more strongly positive than are lower-grade tumors. Our finding of no positivity in craniopharyngioma and some low-grade tumors, combined with well-established positivity in high-grade glioma, fits this picture. However, other investigators have also demonstrated negativity in ependymoma and medulloblastoma (26), tumors that are both well vascularized and metabolically active, suggesting that the answer lies beyond tumor grade alone.
Similarly, the variable results we observed in low-grade gliomas, only half of which were positive for tracer uptake, merit further investigation. These tumors are frequently located in sites where complete surgical resection is difficult, such as the optic chiasm, basal ganglia, or brain stem. The biologic behavior of brain tumors remains difficult to predict by histology alone, and the success of nonsurgical treatments is limited. Therefore, clarifying the nature of the variability of SPECT findings in pediatric low-grade glioma has the potential to add a clinically valuable piece of information to allow a more accurate prediction of clinical behavior over time.
The effect of previous surgery, radiation, or chemotherapy on 99mTc-MIBI uptake is poorly established in the literature. In pediatric brain tumors, the progression of tumor at the edge of a previously resected site may be preferentially imaged by 99mTc-MIBI as opposed to 201Tl (2). Isolated case reports suggest that the 99mTc-MIBI signal is decreased in tumor cells after radiation treatment (27,33). Decreased SPECT activity after therapy despite no change in tumor size by CT or MRI has been shown (27), suggesting that such imaging may be a more sensitive measure of response to treatment. Our results from 6 patients for whom consecutive pairs of images were available are insufficient to significantly support an advantage of sestamibi scans. However, in 1 patient with high-grade glioma, progression on 99mTc-MIBI appeared to precede any evidence of progression on MRI or clinically. Therefore, similarities in the information available from SPECT may exist between adult and pediatric patients with brain tumors.
CONCLUSION
Our results demonstrate the potential uses of 99mTc-MIBI SPECT in the imaging of astrocytic pediatric brain malignancy. We suggest that larger studies be undertaken to better assess the clinical utility of this tool, particularly in low-grade gliomas of childhood.
Footnotes
Received Dec. 10, 2001; revision accepted Jul. 10, 2002.
For correspondence or reprints contact: Adam Kirton, MD, MSc, Department of Pediatrics, Alberta Children’s Hospital, 1820 Richmond Rd. SW, Calgary, Alberta T2T 5C7, Canada.
E-mail: adamkirton{at}hotmail.com
REFERENCES
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.