


Abstract
Monoamine oxidase (MAO) regulates neurotransmitter concentration in the brain and is also an important detoxifying enzyme in peripheral organs. It occurs in 2 subtypes, MAO A and MAO B. Their relative ratios in different organs are variable, depending on the particular organ and species, making it difficult to extrapolate measures from animals to humans. The purpose of this study was to investigate the feasibility of imaging MAO B in peripheral organs in humans with PET. Methods: Nine healthy subjects (7 males, 2 females; mean age ± SD, 37 ± 7 y) received 2 dynamic PET studies of the torso area 2 h apart with 11C-l-deprenyl and deuterium-substituted 11C-l-deprenyl (11C-l-deprenyl-D2). Time-activity curves for heart, lungs, liver, kidneys, and spleen and arterial plasma input were measured for each study. The uptake at plateau and the incorporation quotient (IQ = uptake/plasma input) as well as model terms K1 (which is a function of blood flow) and k3 and λk3 (which are kinetic terms proportional to MAO B) were compared to identify organs that showed reduced values with deuterium substitution (deuterium isotope effect) characteristic of MAO B. In addition, a sensitivity analysis compared the 2 tracers with respect to their ability to quantify MAO B. Results: Heart, lungs, kidneys, and spleen showed a robust deuterium isotope effect on uptake, IQ, k3, and λk3. The arterial plasma input function was significantly larger for 11C-l-deprenyl-D2 than for 11C-l-deprenyl. Liver time-activity curves were not affected by deuterium substitution and model terms could not be estimated. In organs showing an isotope effect, λk3 showed the rank order: kidneys ≥ heart > lungs = spleen. A sensitivity analysis showed that 11C-l-deprenyl-D2 is a better index of MAO activity than 11C-l-deprenyl. Conclusion: This study demonstrates that (a) the deuterium isotope effect is useful in assessing the binding specificity of labeled deprenyl to peripheral MAO B; (b) MAO B can be visualized and quantified in the heart, lungs, kidneys, and spleen but not in the liver; (c) with the exception of the liver, which cannot be measured, MAO B activity is highest in the kidneys and heart; and (d) quantitation in organs having high levels of MAO B is improved by the use of 11C-l-deprenyl-D2, similar to prior studies on the brain. This study indicates that 11C-l-deprenyl-D2 will be useful for measuring the effects of different variables, including tobacco smoke exposure on MAO B activity in peripheral organs in humans.
Monoamine oxidases (MAOs) are flavin-containing enzymes occurring in the brain and in peripheral organs. They oxidize amines from both endogenous and exogenous sources, thereby regulating the concentration of neurotransmitter amines as well as many xenobiotics. MAO occurs in 2 subtypes, MAO A and MAO B. These are different gene products and have different inhibitor and substrate specificities (1). MAO A preferentially oxidizes norephinephrine and serotonin and is selectively inhibited by clorgyline (2), whereas MAO B preferentially breaks down benzylamine and phenethylamine and is selectively inhibited by l-deprenyl (3). Both forms oxidize dopamine (4). Their relative ratios in different organs are variable, depending on the particular organ and species, making it difficult to extrapolate measures from animals to humans.
Medical interest in MAO has historically focused on the brain, beginning with the serendipitous discovery that a MAO inhibitor drug that was being used to treat tuberculosis improved mood in these patients (5,6). This led to the development of MAO inhibitor drugs to treat diseases of central origin, including depression (7), Parkinson’s disease (8), and Alzheimer’s disease (9). However, peripheral MAO represents a vast and complex mechanism for regulating circulating catecholamines and amines from exogenous sources and for regulating blood pressure (10,11). In this sense, peripheral MAO plays a protective role. This is well illustrated by reports of hypertensive crises occurring when individuals taking MAO inhibitor drugs ingest foods containing tyramine, a vasoactive chemical compound occurring in many fermented foods (11). In fact, a common warning in the prescription of many drugs is to avoid coadministration with MAO inhibitor drugs.
The metabolites from MAO-catalyzed oxidation are also of medical interest. MAO generates a molecule of hydrogen peroxide for each molecule of amine that is oxidized. There is evidence that hydrogen peroxide may play a role in cell signaling and function (12). Additionally, MAO-generated hydrogen peroxide is a potential source of oxidative damage via the iron-catalyzed generation of hydroxyl radicals (13). MAO B catalyzes the conversion of 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine (MPTP) to 1-methyl-4-phenylpyridinium ion (MPP+), which is toxic to dopaminergic neurons in brain, leading to Parkinson’s disease. MAO B inhibitor drugs such as l-deprenyl prevent MPTP-induced toxicity (14). Although most studies of MPTP toxicity have focused on the brain, there is speculation that species differences in toxicity may be due to species differences in peripheral MAO B, which would oxidize MPTP to MPP+, which cannot cross the blood-brain barrier (15,16).
We have developed methods for imaging MAO A and B in the human brain using PET and 11C-labeled irreversible inhibitors clorgyline and l-deprenyl, and we have used these methods to investigate the effect of drugs, tobacco smoke, and aging on MAO A and B in the human brain (17–21). We report the extension of this approach to investigate the feasibility of imaging MAO in peripheral organs in humans. We undertook this study to assess the feasibility of measuring the effects of tobacco smoke, which we have shown to inhibit MAO in human brain (18,19), as well as the effects of other substances on MAO activity in peripheral organs. This is relevant because peripheral inhibition of MAO could contribute to smoking toxicity. We used the deuterium isotope effect (22,23) to identify organs where the image clearly represents MAO activity, and we applied compartmental modeling to quantify MAO activity in organs showing an isotope effect similar to that of prior studies in the human brain (23). This study focused specifically on the measurement of peripheral MAO B in humans using paired studies of 11C-l-deprenyl and deuterium-substituted 11C-l-deprenyl (11C-l-deprenyl-D2).
MATERIALS AND METHODS
Subjects
These studies were approved by the Institutional Review Board at Brookhaven National Laboratory, and written informed consent was obtained from each subject after the procedures had been explained. Nine healthy subjects (7 males, 2 females; mean age ± SD, 37 ± 7 y) were recruited by newspaper advertisements and word-of-mouth. Exclusion criteria included medical illness that may affect monoamine levels or monoamine metabolism; a history of drug or alcohol abuse including nicotine; the current use of herbal medicines or medications that may affect monoamine levels or monoamine metabolism; a positive urine screen for drugs of abuse. All 9 volunteers completed both sets of scans, although only the data from 8 were used because of movement during the scan in 1 subject, which degraded the image and prevented region-of-interest (ROI) placement.
PET Scans
PET scans were run on a whole-body, high-resolution positron emission tomograph (HR+; Siemens/CTI, Knoxville, TN; 4.5 × 4.5 × 4.8 mm at center of field of view) in 3-dimensional dynamic acquisition mode. Subjects were positioned with their torso in the tomograph and their arms overhead and outside of the camera with a goal of having both the heart and the kidneys in the field of view. A transmission scan was obtained with a 68Ge rotating rod source before each emission scan to correct for attenuation before each radiotracer injection. Catheters were placed in an antecubital vein for radiotracer injection and in the radial artery for blood sampling. 11C-l-Deprenyl and 11C-l-deprenyl-D2 were prepared as described (24,25). Each subject received both tracers with a time interval of 2–3 h between injections. Six of the subjects had 11C-l-deprenyl first and 3 of the subjects had 11C-l-deprenyl-D2 first. The dose of 11C-l-deprenyl or 11C-l-deprenyl-D2 averaged 240.5 ± 33.3 MBq (6.5 ± 0.9 mCi); the specific activity was about 9,250 MBq/μmol (250 mCi/μmol) at the time of injection. Sequential PET scans were obtained immediately after injection for a total of 60 min with the following timing: 6 × 20-s frames; 4 × 60-s frames; 2 × 120-s frames; 10 × 300-s frames. During the PET scan, arterial blood samples were automatically withdrawn (Ole Dick Instruments, Hvidovre, Denmark), every 2.5 s for the first 2 min, then every minute from 2 to 6 min, and then at 8, 10, 15, 20, 30, 45, and 60 min. Each arterial blood sample was centrifuged, the plasma was pipetted, and the radioactivity was counted. Plasma samples at 1, 5, 10, 20, 30, 45, and 60 min were analyzed for 11C-l-deprenyl (or 11C-l-deprenyl-D2) as described (26).
ROIs
Emission data were corrected for attenuation and reconstructed using filtered backprojection. For the purpose of region identification for the 11C-l-deprenyl (or 11C-l-deprenyl-D2) scans, time frames from dynamic images taken from 0 to 60 min were summed. Planes were added in groups of 2 to obtain 16–30 planes for ROI placement. The number of planes was determined by subject positioning (i.e., whether or not both the heart and kidneys were in the field of view). ROIs were drawn directly on PET scans using an atlas for reference (27). ROIs for the following areas were obtained for the purpose of this analysis: heart, lungs, liver, kidneys, stomach, and spleen. Regions for each organ were identified on 2 or 3 planes and the weighted average was obtained. Right and left lung and right and left kidney regions were averaged. For the kidneys, the region placement was made on the cortex because the medulla was devoid of radioactivity. The regions were then projected to the dynamic scans to obtain the concentration of 11C versus time and expressed as a percentage of the total injected dose per cm3.
Kinetic Analysis
Time-activity curves for 11C-l-deprenyl and 11C-l-deprenyl-D2 were compared to identify organs that showed the reduction in binding rate characteristic of the deuterium isotope effect. PET time-activity data for 11C-l-deprenyl and 11C-l-deprenyl-D2 for these organs as well as the time-activity data from arterial plasma were used to calculate an incorporation quotient (IQ), which is equal to the average uptake at plateau/plasma integral over 60 min and normalizes organ uptake for the amount of radiotracer in the plasma. The uptake (% dose/mL) was obtained by examining the time-activity curves and averaging the time points that occurred during the plateau phase. The plateau occurred at slightly different times for the different organs: 12.5–60 min for lungs, liver, and heart; 17.5–60 min for spleen; and 9–60 min for kidneys. A 3-compartment model was used to calculate K1, the plasma-to-organ transfer constant, which is related to blood flow; k2, which is related to the transfer of tracer from the organ to plasma; and k3, the kinetic constant controlling the rate of binding to MAO B. MAO B concentration was not determined directly but, rather, inferred from the model term k3. However, because estimates of k2 and k3 are highly correlated, a bias can occur in the estimation of k3. This is particularly problematic in regions of high MAO B concentration in which k2 may be underestimated, leading to an underestimation of k3 and of the inferred relative enzyme concentration. Using the combination model parameter λk3, the correlation problem is reduced because λk3 depends on the ratio k3/k2. We also previously found that reproducibility in test-retest studies is improved using λk3 rather than k3 as the model parameter for comparison (28). The combination parameter, λk3, is used as an index of MAO B. λ is defined as K1/k2 and is independent of blood flow (29). We have previously used a similar model to estimate functional MAO B activity in the human brain (23).
For each organ, the residual blood volume in the organ (30) was applied as a correction factor and model terms for the lung were also corrected for 70% air in the volume of interest (31). The residual blood volumes that were used for the spleen, heart, lungs, and kidneys were 25%, 7%, 5%, and 7%, respectively. Spillover was minimized by fitting the data using times >1.5 min, for which the blood radioactivity is substantially less than the peak value that occurs generally at times <1 min. Partial volume is more difficult to correct and could introduce errors if misapplied. Because the organs studied should have the same partial-volume effects across subjects, we accept this as a bias but one that contributes a similar amount to each subject.
Sensitivity of Model Parameters
The ability to accurately estimate λk3 depends on its value relative to K1. When λk3 ≫ K1 (or equivalently k3 ≫ k2), uptake depends primarily on K1 and is relatively insensitive to changes in k3 or λk3. Using Ki (the influx constant (32)) given by K1k3/(k2 + k3), as a measure of uptake, the sensitivity of Ki to changes in λk3 can be calculated in terms of the normalized derivative ∂Ki/∂λk3(λk3/Ki).
Because ∂Ki/∂λk3(λk3/Ki) = 1 − λk3/(K1 + λk3), the maximum value is 1. As λk3 increases relative to K1, the sensitivity decreases. To illustrate this, a plot of ∂Ki/∂λk3(λk3/Ki) versus λk3 was generated for K1 values of 0.25, 0.50, 1.0, 1.5, 2.0, and 2.5 mL/min/mL.
Statistical Analysis
The plasma input function, the IQ, and the model terms K1, k2, k3, λk3, and k3/k2 for heart lungs, kidneys, and spleen for 11C-l-deprenyl and 11C-l-deprenyl-D2 were compared using paired-samples t tests. We realize that there is a multiple-comparison concern, but it is not feasible to do a good correction for so many tests. We provided the P values (2-sided) for those considered significantly different so the readers could make a better judgment. We examined the rank order of the IQ, K1, and λk3 using a repeated-measures general linear model to examine the homogeneity of the ROIs. (Only the IQ was calculated for the liver because no model fit to the data could be obtained.) There are 4 ROIs: heart, lungs, kidneys, and spleen. Eight subjects are included in the analysis, but there are only 23 observations available because of the fact that all organs were not visualized on all subjects. The analysis was performed using SAS PROC GLM (SAS Institute Inc., Cary, NC).
RESULTS
It was not possible to image both heart and kidneys in the same session for all of the subjects. Kidney images were obtained for 7 subjects and heart (and lung) images were obtained for 5 subjects. The liver was in the field of view for 8 subjects and the spleen was in the field of view for 6 subjects. Summed images of 11C-l-deprenyl and 11C-l-deprenyl-D2 from 7 to 60 min for 1 subject are shown in Figure 1. There is a large reduction in uptake with 11C-l-deprenyl-D2 relative to 11C-l-deprenyl that can be seen for the kidneys and a less apparent reduction for the heart, lungs, and spleen because they have significantly less accumulation than the kidneys.
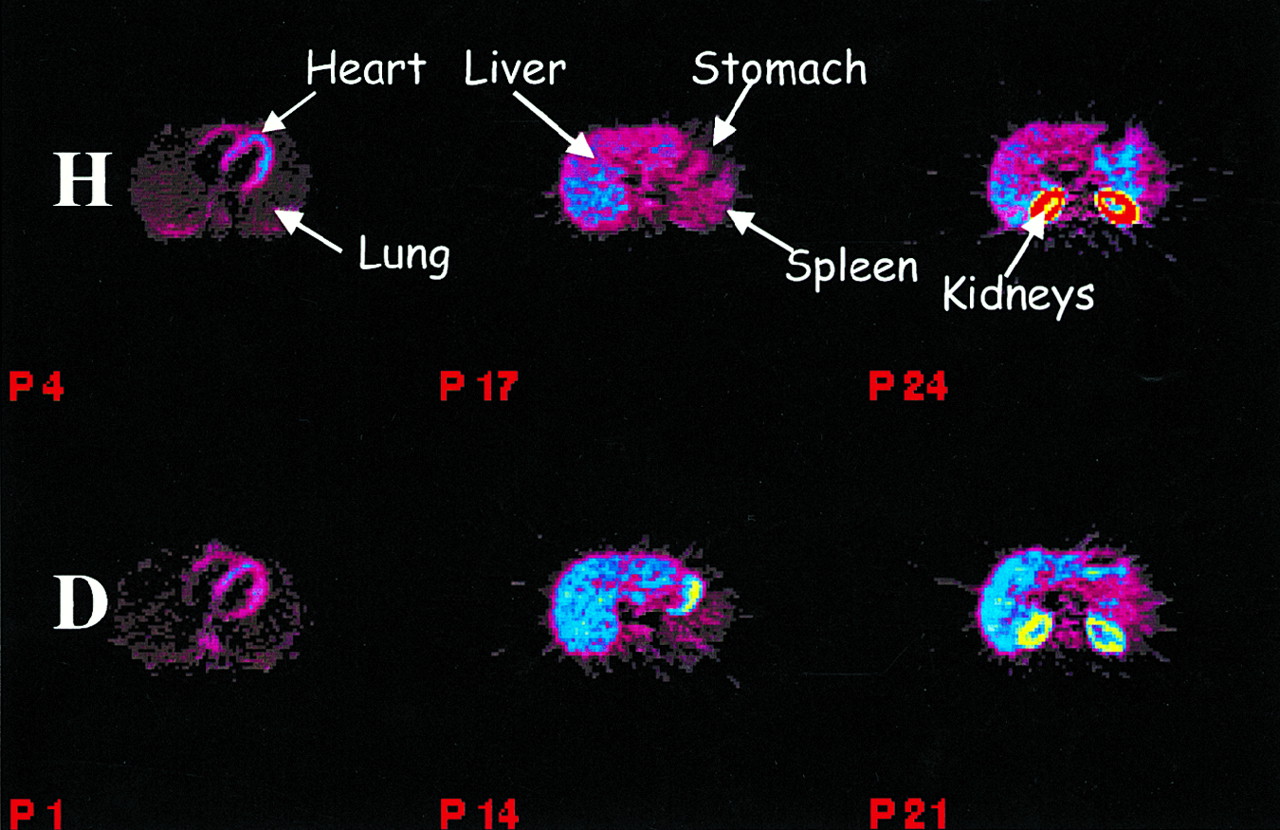
Summed images (from 7 to 60 min) for 1 subject for 11C-l-deprenyl (H) (top row) and 11C-l-deprenyl-D2 (D) (bottom row). Planes from left to right show heart and lungs (planes 4 and 1); liver, stomach, and spleen (planes 17 and 14); and kidneys (planes 24 and 21). Note reduced accumulation of 11C with 11C-l-deprenyl-D2. Rainbow color scale is used.
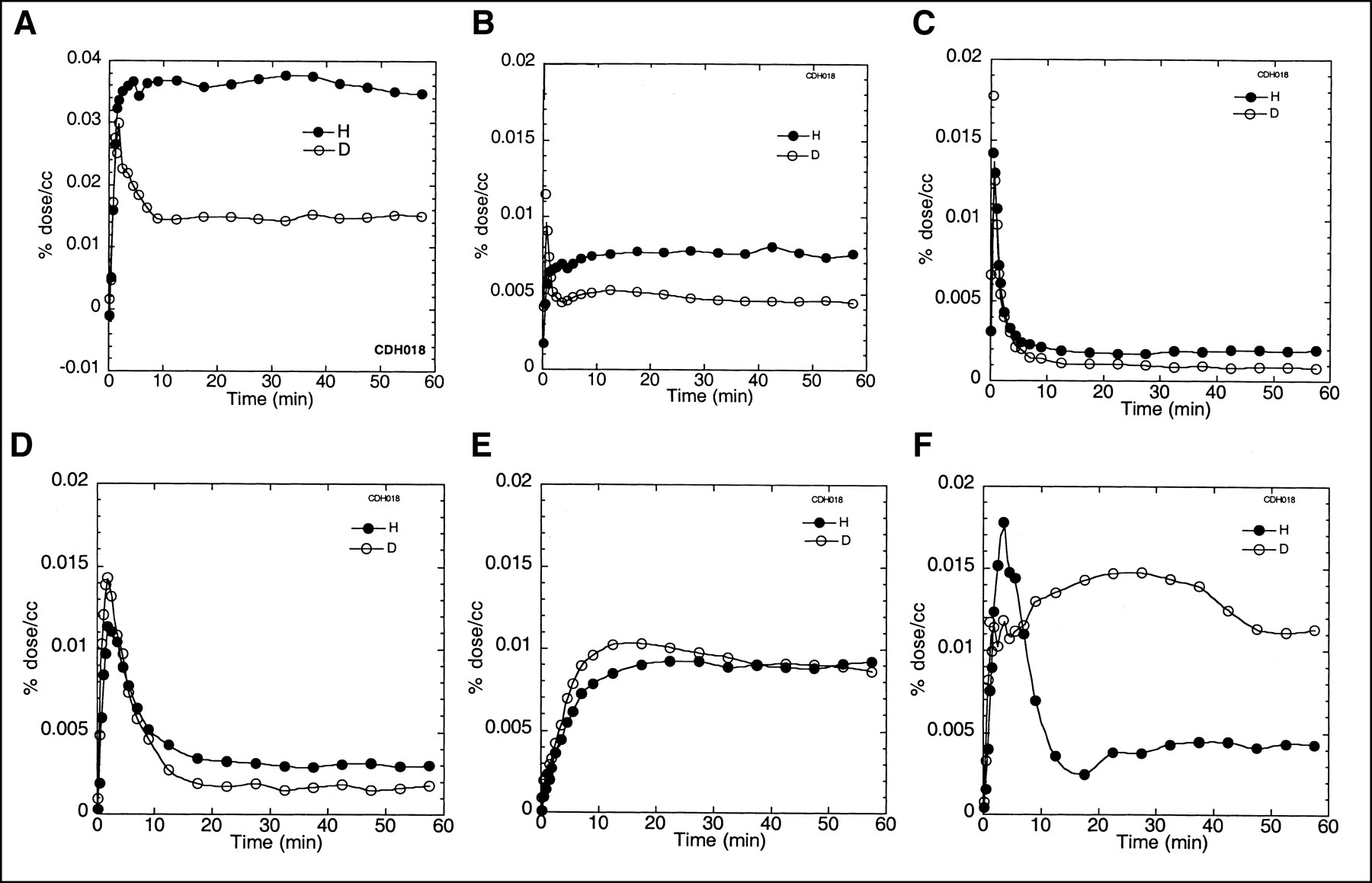
Time-activity curves for kidneys, heart, lungs, spleen, and liver for 1 subject are shown in Figure 2. The highest uptake occurred in the kidneys. For the kidneys, the uptake curves differed for the 2 tracers with 11C-l-deprenyl typically peaking at around 5 min and leveling off at about 5–10 min. In contrast, 11C-l-deprenyl-D2 showed a very rapid initial rise and fall, peaking at around 5 min with a plateau at around 10 min at about half the value of 11C-l-deprenyl. The pattern in the heart was similar to that of the kidney with a significant reduction in 11C concentration at the plateau with deuterium substitution. The 11C concentration at the plateau was considerably lower for the heart than for the kidneys for both tracers. For the lungs there was a very rapid uptake with a peak at 0.5 min followed by a rapid clearance and a plateau at around 12 min. Deuterium substitution reduced the concentration of 11C at the plateau in the lungs. The time-activity curves for the spleen were somewhat similar to those for the lungs with a rapid uptake peaking at 1–2 min followed by a rapid washout and a plateau at around 10 min. The 11C concentration at the plateau was reduced with deuterium substitution. For the liver there was a slower uptake for both tracers with a peak around 10 min and a plateau thereafter for both tracers.
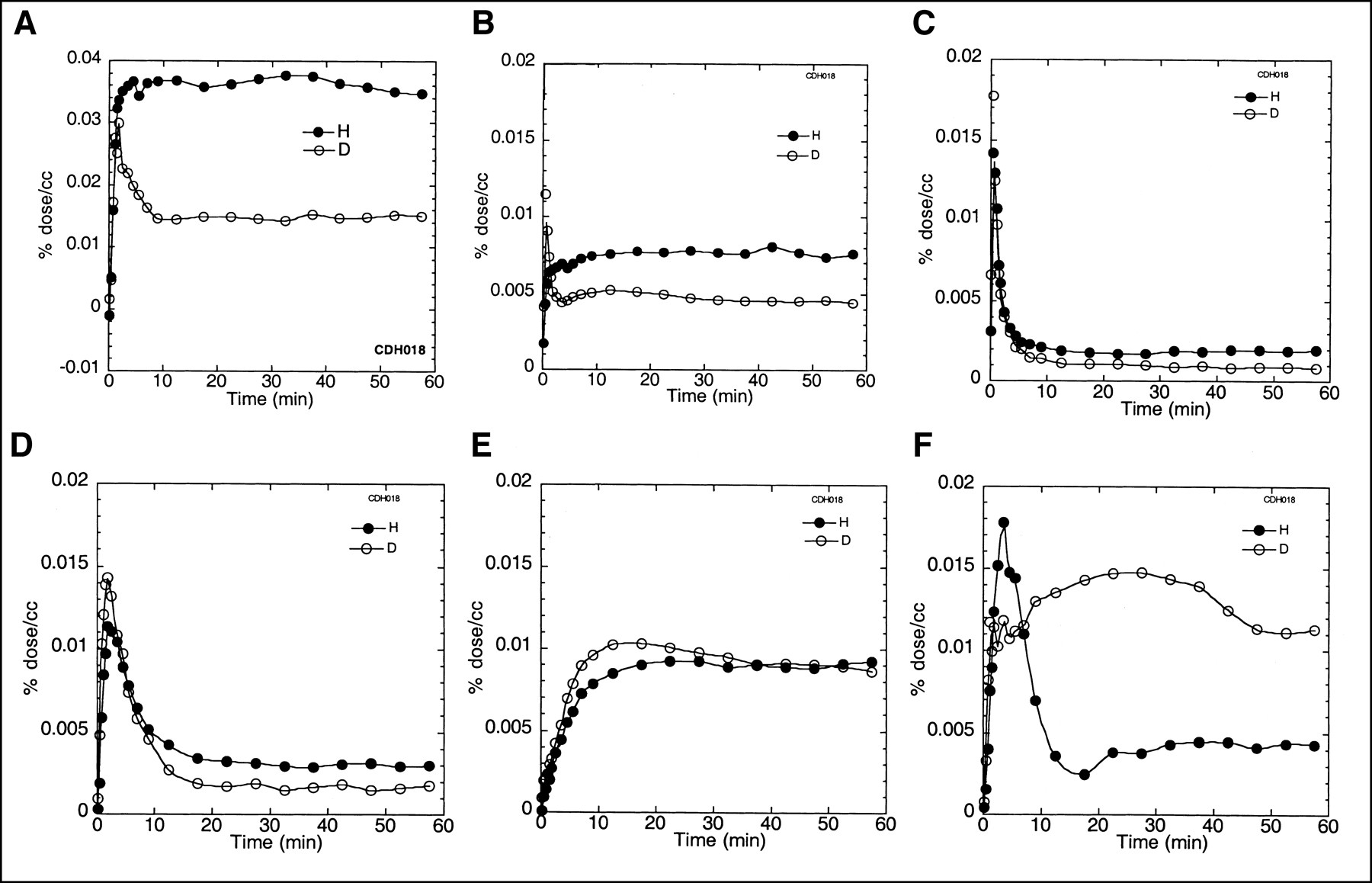
Time-activity curves for 1 subject for kidneys (A), heart (B), lungs (C), spleen (D), liver (E), and stomach (F) after injection of 11C-l-deprenyl (H; •) and 11C-l-deprenyl-D2 (D; ○). Note that maximum value of ordinate for heart, lungs, spleen, liver, and stomach is only half that of kidneys (0.02%/mL vs. 0.04%/mL).
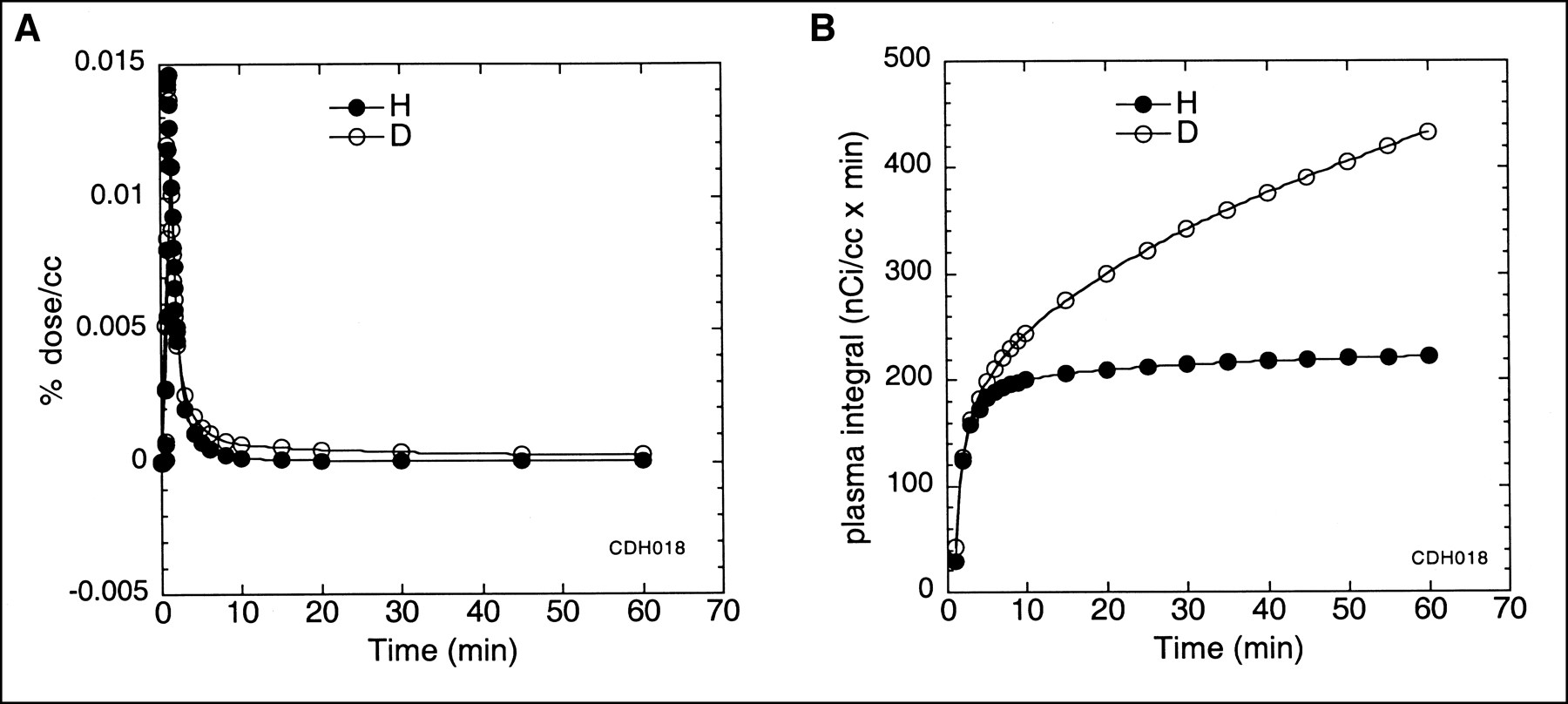
The input function (radiotracer concentration vs. time) was significantly higher for 11C-l-deprenyl-D2 than for 11C-l-deprenyl (8,621 ± 1,406 vs. 11,507 ± 1,406 Bq/mL × min [233 ± 38 vs. 311 ± 38 nCi/mL × min]; paired t, −7.6; P < 0.0001). Time-activity curves and the corresponding integrals are shown for 1 subject in Figures 3A and 3B, respectively.
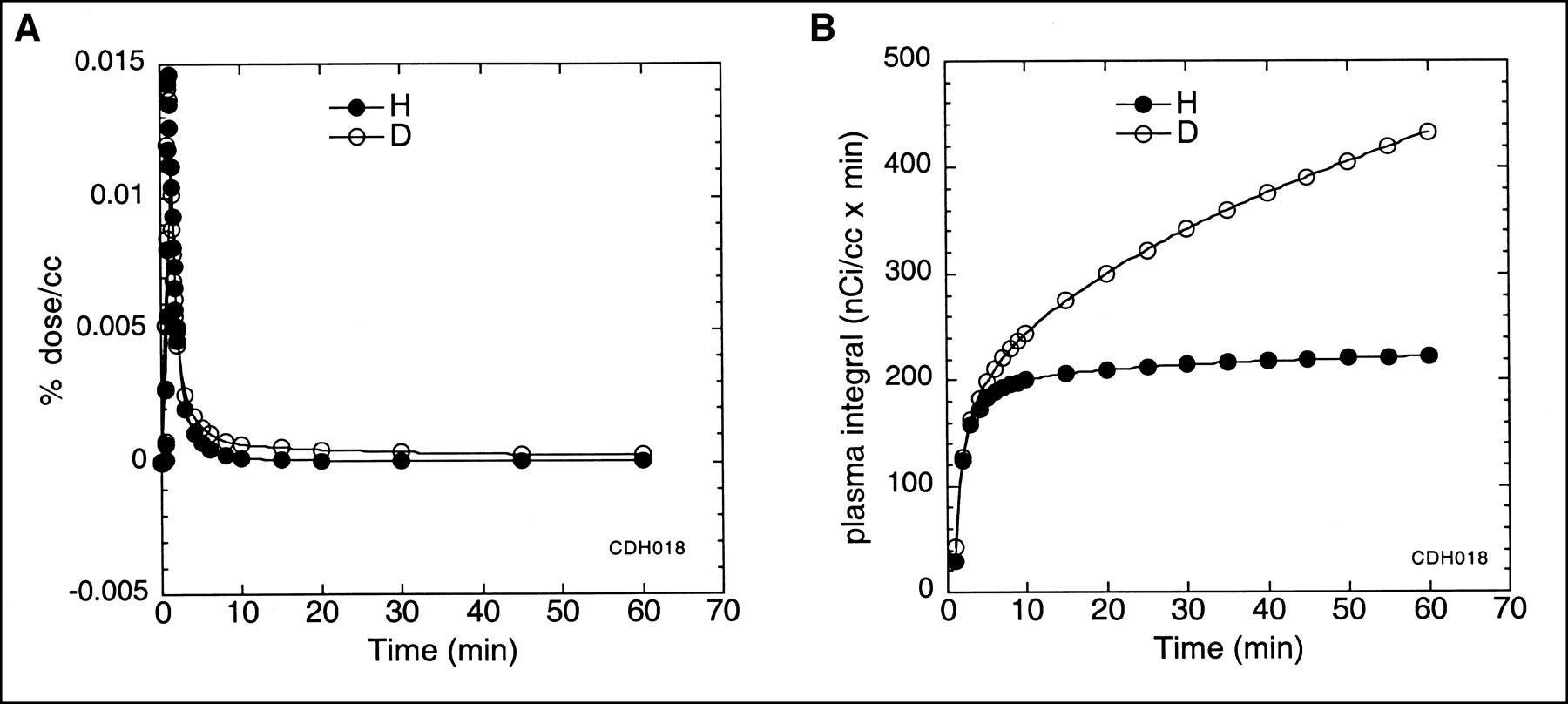
(A) Time-activity curves for arterial plasma for 11C-l-deprenyl (H; •) and 11C-l-deprenyl-D2 (D; ○). (B) Plasma integral for time-activity curves show that value of arterial plasma input function is greater with deuterium-substituted tracer.
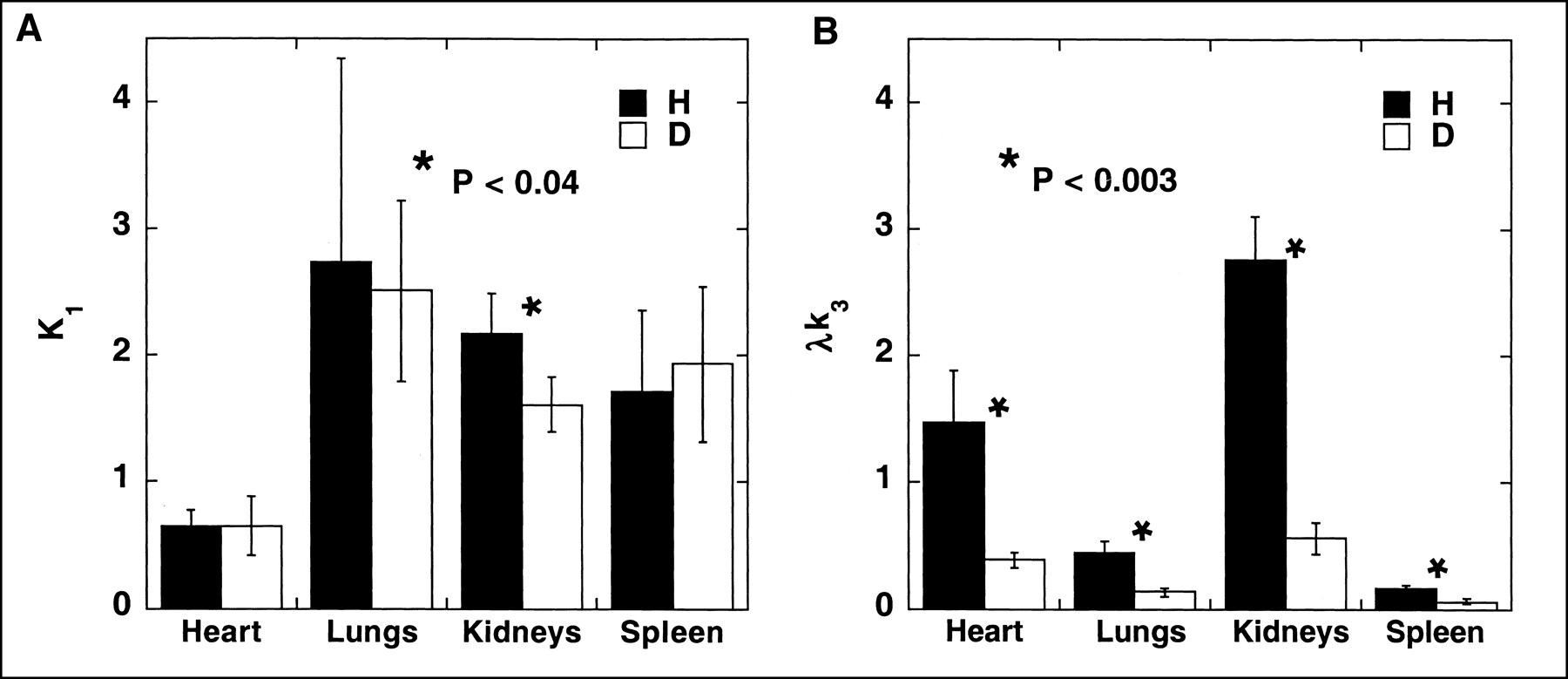
The average values for the IQ and the model terms K1, k2, k3, λk3, and the k3/k2 ratio are shown in Table 1 for each tracer. K1, which is related to blood flow, did not differ between 11C-l-deprenyl and 11C-l-deprenyl-D2 except for a small effect in the kidney (P = 0.04). In contrast, the IQ, k3, λk3, and k3/k2 were significantly different for the 2 radiotracers for the heart, lungs, kidneys, and spleen with 11C-l-deprenyl being 1.8–5.7 times higher than 11C-l-deprenyl-D2 (P < 0.003). Average values for K1 and for λk3 are shown in the bar plot in Figures 4A and 4B.
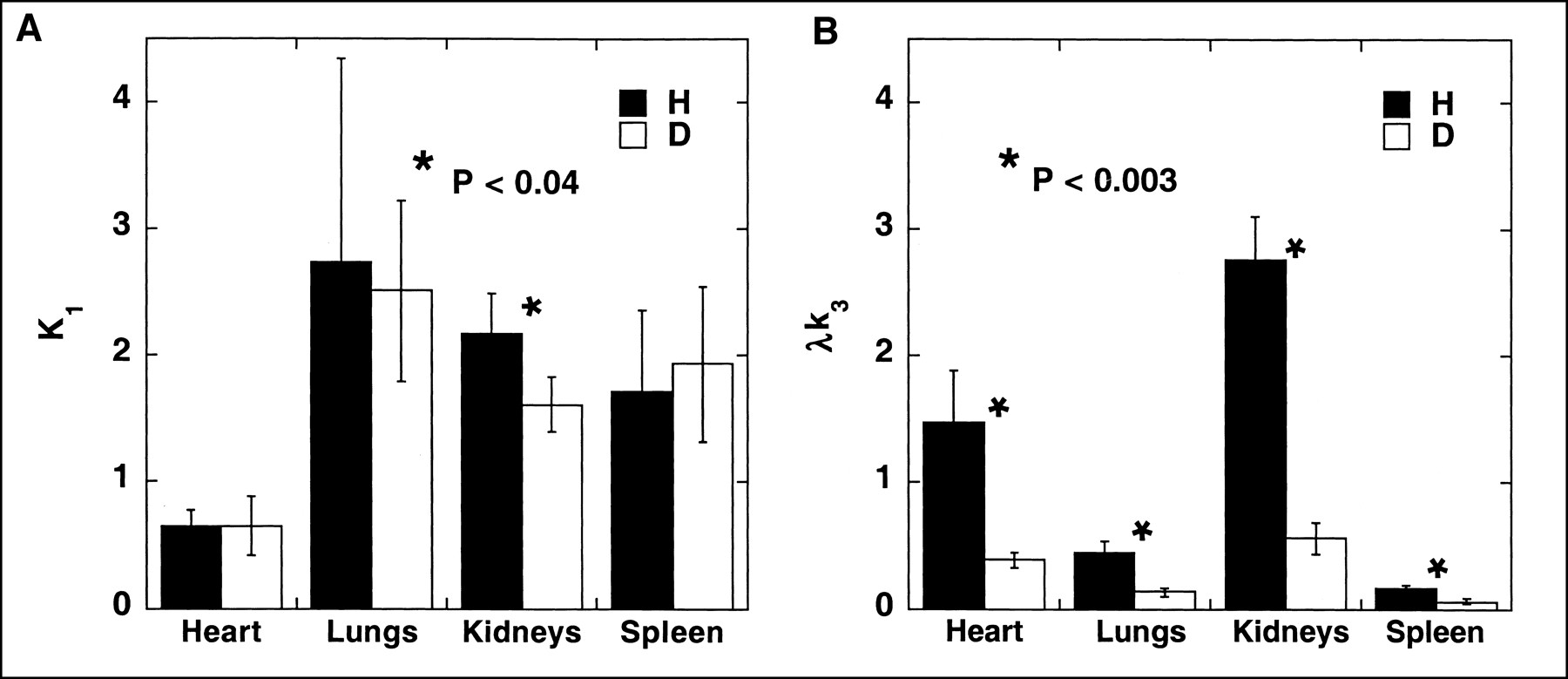
(A) Bar graph compares plasma-to-brain transfer function (K1) for 11C-l-deprenyl (H; ▪) and 11C-l-deprenyl-D2 (D; □). (B) Bar graph compares λk3, which is index of MAO B activity. Note that values for K1 did not differ except in kidney, which was barely significant (P < 0.04) in contrast to λk3, which showed marked significant reductions in all organs (P < 0.003).
Values for IQ and Model Terms for 11C-l-Deprenyl (H) and 11C-l-Deprenyl-D2 (D) Calculated Using 3-Compartment Model
Similar to prior studies on the brain (23), the sensitivity of λk3 to changes in MAO B concentration is degraded as the value of λk3 increases, and this is exacerbated with smaller values of K1 (Fig. 5). Thus, the sensitivity to differences in MAO B concentration is greater for 11C-l-deprenyl-D2 than for 11C-l-deprenyl because the values of λk3are smaller (Fig. 4B). In addition, though the IQ and λk3 are highly correlated for all of the organs for both 11C-l-deprenyl and 11C-l-deprenyl-D2 (P < 0.02), there is a danger in general of using the IQ parameter rather than λk3 as an index of MAO B activity because it is dependent on blood flow.
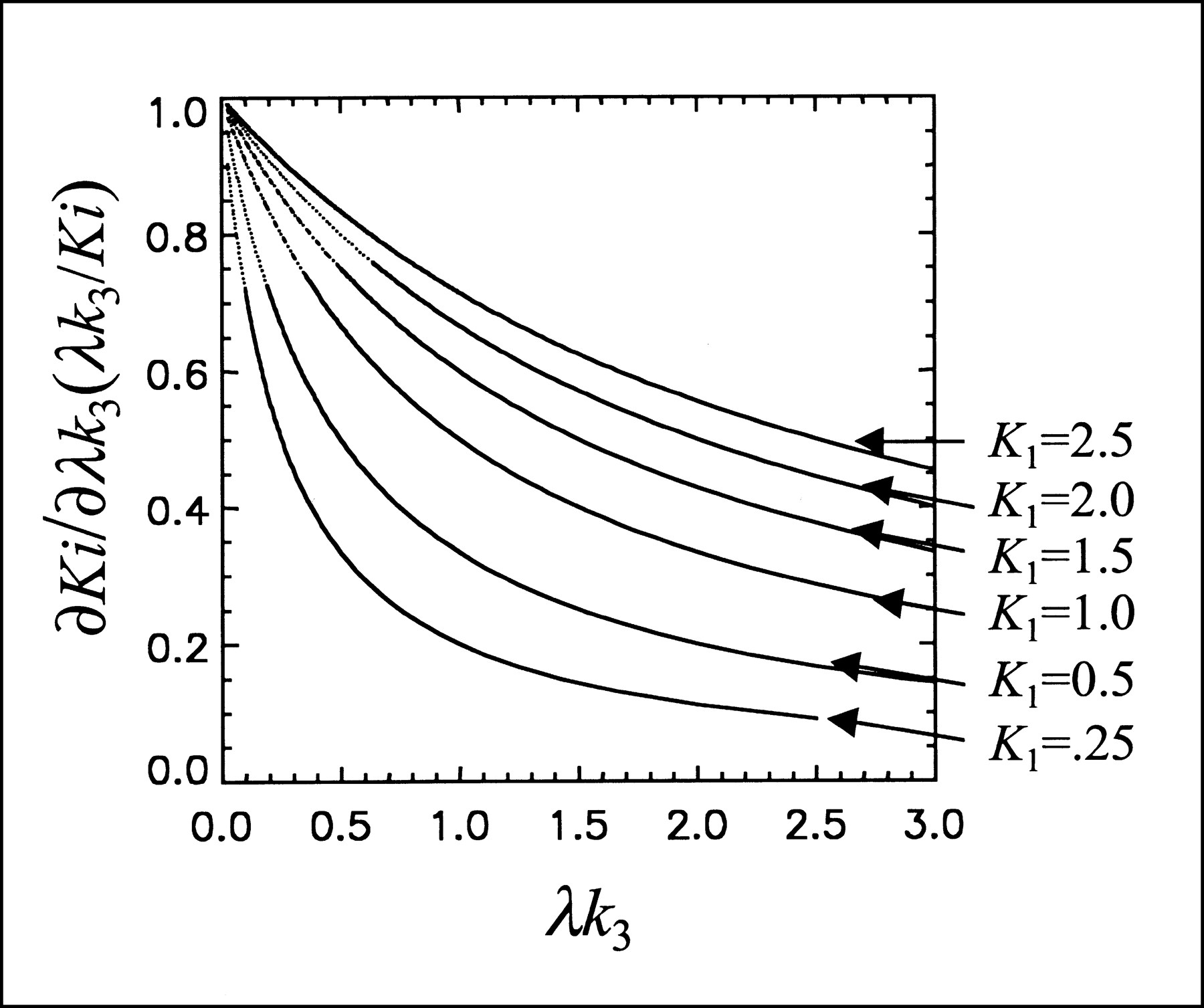
Plot of ∂Ki/∂λk3(λk3/Ki) vs. λk3 for K1 values of 0.25, 0.50, 1.0, 1.5, 2.0, and 2.5 mL/min/mL. Note that when Ki changes very little with relatively large changes in λk3, uptake is flow limited. With larger values of K1, Ki is sensitive to changes in λk3 over much wider range than for lower values.
For both 11C-l-deprenyl and 11C-l-deprenyl-D2, the values of λk3between the 4 organs are significantly nonhomogeneous (F3,12 = 42 for 11C-l-deprenyl-D2 and 100 for 11C-l-deprenyl; P < 0.0001). Pairwise comparison was performed using Tukey’s method (33). We found that all ROI pairs are significantly different except the lungs and spleen. The order of λk3 is: kidneys ≥ heart >* lungs = spleen (*significantly different using Tukey’s test at the familywise error rate of 0.05, 2-sided). A similar analysis for K1 showed that the value for the heart is significantly smaller than that for the lungs, spleen, and kidney, which are not significantly different from one another.
DISCUSSION
Postmortem studies in humans have reported high MAO B activity in the liver, myocardium, kidney, duodenum, and lung, with very little activity in the spleen (34,35), and immunohistochemical studies have determined the cellular localization of both MAO A and B in several human tissues outside of the central nervous system (36,37).
We now report the first results of studies exploring the feasibility of imaging MAO B activity in peripheral organs in healthy human subjects. We patterned these exploratory studies on our use of deuterium-substituted 11C-l-deprenyl as a mechanistic tool for PET studies of MAO B in the human and baboon brain (23,25). 11C-l-Deprenyl is a suicide inactivator of MAO B. It irreversibly inhibits the enzyme by covalently binding to it after being activated by cleavage of the C-H bond on the methylene carbon of the propargyl group. Because a carbon-deuterium bond is more difficult to cleave than a carbon-hydrogen bond, the rate of binding in brain is reduced when 11C-l-deprenyl is substituted with deuterium atoms in the methylene group. Thus, the utilization of the deuterium isotope effect has the potential to identify the specific molecular event in the interaction between the labeled compound and the organ. Accordingly, we compared the kinetic patterns of 11C-l-deprenyl/11C-l-deprenyl-D2 pair in different organs in healthy volunteers to determine those in which the rate of binding is reduced by deuterium substitution. The use of the isotope effect rather than a specific MAO B inhibitor drug avoids the confounds of drug-induced changes in other parameters such as blood flow and also avoids potential risks associated with MAO inhibition in healthy subjects. A similar strategy has been used in mechanistic PET studies on the heart with 18F-6-fluorodopamine (38) and with 11C-phenylephrine (39).
In paired studies comparing 11C-l-deprenyl and 11C-l-deprenyl-D2, the heart, lungs, kidneys, and spleen were unambiguously visualized and each showed a reduction in uptake and reduced values of k3 and λk3 with deuterium substitution, indicating that MAO B is responsible for all or part of the organ binding. Moreover, the kinetic pattern indicated that, after an initial rapid influx and clearance, binding is irreversible in these organs.
Irreversibly binding tracers such as 11C-l-deprenyl, which show a rapid rate of binding, are difficult to quantify in organs of high MAO activity because binding can be limited by tracer delivery. Thus, it is important to try to achieve a balance between a sufficiently high binding rate to the molecular target to give a statistically meaningful counting rate in an ROI yet a slow enough binding so that flow is not the rate-limiting step. A high k3/k2 ratio indicates a high rate of binding relative to efflux and a potential underestimation of binding. This has been referred to as the flow-limited situation and is illustrated in Figure 5. This applies to some extent to the binding of 11C-l-deprenyl but less for 11C-l-deprenyl-D2 in the kidneys. Deuterium substitution reduces the value of k3/k2 by a factor of 3–4 for all organs examined, demonstrating the advantage of using 11C-l-deprenyl-D2 to quantify MAO B in peripheral organs where the signal represents MAO B. This is similar to our observation that 11C-l-deprenyl-D2 is superior to 11C-l-deprenyl for studies of MAO B in the human brain (23).
There are some potentially important differences between the brain and peripheral organs in terms of radiotracer quantification. In the brain, hydrophilic metabolites are normally excluded by the blood-brain barrier. This is not the case in peripheral organs; thus, it is possible that nonspecific binding may dominate the image even in the presence of the specific molecular target such as MAO if an organ serves as a major excretory pathway for labeled metabolites. We were surprised to find that we could use the arterial input function of the parent tracer in our model calculations for the heart, lungs, kidneys, and spleen, indicating that the influx of labeled metabolites did not contribute measurably to the image. However, the pattern in the liver did not change significantly with deuterium substitution and differed from that for other peripheral organs (even though the liver is known to have high MAO B (34)), and we were not able to calculate model terms. Although the IQ for the liver shows a 30% reduction due to the fact that the plasma input from 11C-l-deprenyl-D2 is larger than that from 11C-l-deprenyl (Table 1), the inability to calculate model terms indicates that liver clearance may be a pathway for the excretion of labeled metabolites, thereby limiting the use of this method to measure liver MAO B.
We note that there is considerable intersubject variability in the model term λk3 for the 4 organs. The coefficient of variation expressed as a percentage ranges from 13% to 27% for 11C-l-deprenyl and from 15% to 29% for 11C-l-deprenyl-D2 (Table 1). This is larger than the intersubject variability for brain MAO B. For example, in baseline measures of brain MAO B in healthy individuals with 11C-l-deprenyl-D2 (28), the coefficient of variation ranges from 11% to 17%. The factor or factors contributing to the variability in peripheral organ MAO B among individuals is not known.
In organs showing an isotope effect, MAO B activity is greatest in the kidney and the heart with somewhat lower activity in the lung and the spleen. This is the general pattern reported in postmortem studies (34) with the exception of the liver (which has been reported to have the highest MAO B activity but which we could not quantify). High kidney MAO B activity is of interest because MAO breaks down filtered dopamine in the kidney (40). Kidney dopamine is believed to exert a natriuretic effect through inhibition of different transport systems, including the Na+-K+pump, the Na+H+ antiporter, and Na+-P cotransporter.
MAO B activity has been reported to be very high in the human duodenum, presumably serving a protective role in breaking down vasoactive amines present in foods (11,34). Both 11C-l-deprenyl and 11C-l-deprenyl-D2 showed high accumulation in the gut area. We have not yet performed ROI analysis of the gut area because of the difficulty in organ identification. We did note that the stomach showed high accumulation of radioactivity consistent with the presence of MAO in the stomach (41); however, the kinetic patterns for 11C-l-deprenyl versus 11C-l-deprenyl-D2 were different among different individuals. Thus, gut and stomach activity will require further study.
CONCLUSION
We have shown that the deuterium isotope effect is useful in assessing the binding specificity of labeled deprenyl to peripheral MAO B and that MAO B can be visualized and quantified in the heart, lungs, kidneys, and spleen but not the liver. Of the organs in which MAO B can be visualized, MAO B is highest in the kidneys and heart. Quantitation is improved by the use of 11C-l-deprenyl-D2, similar to prior studies on the brain. This study indicates that 11C-l-deprenyl-D2 will be a useful radiotracer for measuring the effects of physiologic variables such as age and disease as well as the effect of therapeutic drugs and tobacco smoke on peripheral MAO B, similar to studies of MAO B inhibitor drugs on the brain. Whole-body MAO B imaging may also be useful in identifying target organs in drug development and in determining drug dosing regimes for therapeutic MAO B inhibitor drugs under development for the treatment of neurodegenerative and other diseases.
Acknowledgments
The authors are grateful to Robert Carciello, Donald Warner, Payton King, Noelwah Netusil, Bud Jayne, and Pauline Carter for advice and assistance in performing these studies. We are also grateful to the people who volunteered for these studies. This work was performed at Brookhaven National Laboratory under contract DE-AC02-98CH10886 with the U.S. Department of Energy and supported by its Office of Biological and Environmental Research and by National Institutes of Health grant NS 15380.
Footnotes
Received Dec. 26, 2001; revision accepted Jun. 11, 2002.
For correspondence contact: Joanna S. Fowler, PhD, Chemistry Department, Brookhaven National Laboratory, Upton, NY 11973.
E-mail: fowler{at}bnl.gov





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}