


Abstract
Balloon catheters filled with liquid radioisotopes provide excellent dose homogeneity for intracoronary radiation therapy but are associated with risk for rupture or leakage. We hypothesized that the safety of liquid-filled balloons may be improved once positron emitters with half-lives below 2 h are used instead of the high-energy β-emitters 166Ho, 186Re, or 188Re, all of which have a longer half-life of at least 17 h. Methods: To support this concept, the suitability of 18F (half-life, 109.8 min), 68Ga (half-life, 67.6 min), 11C (half-life, 20.4 min), 13N (half-life, 9.97 min), and 15O (half-life, 2.04 min) for intracoronary radiation therapy was evaluated. Potential tissue penetration of positron radiation was assessed in a series of phantom experiments using Gafchromic film. Antiproliferative efficacy of positrons emitted by 68Ga was investigated in vitro using cultured bovine aortic smooth muscle cells (BASMCs), and was compared with γ-radiation emitted by 137Cs. To characterize the remaining risk, we estimated radiotoxicity after accidental intravascular balloon rupture on the basis of tabulated isotope-specific doses (ICRP 53) and compared these values with 188Re. Results: Half-dose depth of tissue penetration measured in phantom experiments was 0.29 mm for 18F, 0.42 mm for 11C, 0.54 mm for 13N, 0.79 mm for 15O, and 0.9 mm for 68Ga. Irradiation of cultured BASMCs with positron radiation (68Ga) induced dose-dependent inhibition of proliferation with complete proliferative arrest at doses exceeding 6 Gy. ED50 and ED80 were 2.5 ± 0.4 Gy (mean ± SD) and 4.4 ± 0.8 Gy, respectively. Antiproliferative efficacy was equal to that of the 662-keV γ-radiation emitted by 137Cs (ED50, 3.8 ± 0.2 Gy; ED80, 8.0 ± 0.3 Gy). Estimates made for patient whole-body and organ doses were generally below 50 mSv/1.85 GBq for all investigated positron emitters. The same dose estimates for 188Re were 6–20 fold higher. Conclusion: Among the studied radioisotopes, 68Ga is the most attractive source for liquid-filled balloons because of its convenient half-life, sufficient positron energy (2.92 MeV), documented antiproliferative efficacy, and uncomplicated availability from a radioisotope generator. The safety profile for 68Ga is significantly better than that of 188Re, which suggests this radioisotope should be evaluated further in preclinical studies.
Intracoronary radiation therapy is currently considered the most promising breakthrough approach for preventing restenosis after angioplasty and stenting (1). However, the ideal radioisotope to treat coronary arteries with radiation has still not been defined. To date, most commercial systems use solid sources emitting either γ- or β-radiation. Although the advantage of such sources is that no liquid radioactivity can be spilled, centering a thin radioactive wire within a coronary artery can pose a problem. Centering is considered important for homogeneous delivery of radiation to the vascular target tissue once reliable and safe dose control is desired.
The high relevance of precise dose control has lead to the attempt to use conventional angioplasty balloon catheters filled with liquid radioactivity for irradiation of coronary lesions (2,3). Liquid-filled balloons are self-centering within the coronary artery. Thus, they define the geometry of the artery and are capable of exposing the source in direct contact with the target tissue, resulting in significantly enhanced homogeneity of delivered dose. However, balloons may rupture, and such accidents were recently reported to occur in up to 3.7% of patients submitted to balloon angioplasty and stenting (4). Because of this particular risk, radioisotopes originally used in source–wire systems (32P, half-life of 14 d; 90Y, half-life of 2.67 d) are generally not safe enough for the liquid-filled balloon approach.
Liquid radioisotopes with shorter half-lives have been proposed, including 186Re (half-life, 3.72 d) (5), 166Ho (half-life, 26.8 h) (6), and 188Re, a β-emitter of suitable radiation energy with a half-life of only 17.0 h (2,3,7). Recently, a clinical study has documented the feasibility and efficacy of the use of 188Re liquid-filled balloons in patients (8). It was claimed that an intravascular loss of 188Re caused by balloon rupture was not dangerous because of the rapid renal elimination of the radioactive compound. A whole-body dose of up to 0.16 mSv/MBq (8) was estimated to result from a typical in-patient balloon rupture with 188Re. In clinical practice, such an accident may provoke a total dose of 296 mSv once the typical in-balloon activity of 1.85 GBq 188Re was lost systemically. This estimate is 6 times higher than the upper threshold of 50 mSv allowed as the maximum annual cumulative dose for professionally exposed personnel. Although 188Re has the shortest half-life of the aforementioned radioisotopes for liquid-filled balloons, there is still an obvious potential for nonnegligible radiation exposure to the patient and for laboratory contamination once a balloon ruptures. Because of this particular risk, the majority of interventional cardiologists prefer to use solid radiation sources.
To overcome safety problems related to both patient exposure and laboratory contamination, we evaluated the isotopic table for radioisotopes that would provide enhanced safety through a physical half-life substantially shorter than that of 188Re while maintaining full therapeutic efficacy. This premise directed the search toward emitters of positron radiation that had previously not been considered for liquid-filled balloons, but theoretically should be suitable based on the expectation of similar tissue interactions for positrons and β-particles.
Positron emitters with half-lives ranging from 2.04 to 109.8 min traditionally used for PET were selected for investigation in this study. The goals were to investigate the feasibility, efficacy, and safety of positron radiation in phantom and cell culture experiments. Thus, this study seeks to characterize the penetration capability of positron radiation into tissue-equivalent media, to compare the expected antiproliferative efficacy of positrons with that of γ-radiation in cell culture, and to characterize the safety profiles of these positron emitters in comparison with other radioisotopes being evaluated for the liquid-filled balloon approach.
Materials and Methods
Radioisotopes and Dosimetry
We investigated 15O (half-life, 2.04 min), 11C (half-life, 20.4 min), 13N (half-life, 9.97 min), 18F (half-life, 109.8 min), and 68Ga (half-life, 67.6 min). H215O, 11CO2, 13NH3, and 18FDG were synthesized through routine protocols in the cyclotron laboratory serving the PET facility at the Indiana University School of Medicine. 68GaCl3 was eluted from a 68Ge–68Ga radioisotope generator. This generator (DuPont Gallium-68 Ionic Positron [IGG099]; Dupont Pharma Radiopharmaceuticals, Billerica, MA) delivers a maximum initial activity of 1.85 GBq 68GaCl3 in a volume of 5.0 mL. Elution can be repeated every 3 h, providing 87% of the nominal activity at this time point. The half-life of the mother 68Ge determining the shelf life is 271 d. Physical parameters characterizing the investigated radionuclides as well as other previously suggested radioisotopes are given in Table 1.
Physical Parameters* of Positron Emitters Investigated for Coronary Radiation Therapy in This Study and for β-Emitters Previously Suggested for Liquid-Filled Balloons
To provide precise dosimetry for short-lived radioisotopes used in these experiments, a computer program was written that continuously calculated the remaining radioisotope activity at any given time once the activity of the initial isotope preparation was entered. Before irradiation, this program informed continuously about the expected dwell time for a given target dose. During irradiation, the already accumulated dose and the remaining dwell time were displayed and the program called for source removal once the prescribed dose was reached.
Phantom Measurements for Assessment of Positron Penetration
For quantification of the penetration of positron radiation into tissue-equivalent media, standard angioplasty balloon catheters (outer diameter, 3.0 mm; length, 20 mm) (Comet; Guidant Corp., Santa Clara, CA) were inflated with liquid solutions of various positron-emitting radioisotopes for controlled irradiation of the radiosensitive film. The total volume of the balloons was 0.8 mL including balloon, shaft, and proximal connector, whereas the in-balloon volume was 0.14 mL. In-balloon activities ranged from 74 MBq to 3.7 GBq. Fifteen balloons (3 balloons per isotope) were inserted perpendicularly into circular holes that were punched into plain pieces (2 × 2 in.) of Gafchromic film (MD-55; Nuclear Associates, New York, NY) with a density similar to tissue. For closer simulation of the in vivo absorption of radiation, the balloons and film were submerged into a water bath for exposure. They were left in place until a clearly visible blue color appeared in proximity to the balloon, indicating appropriate response of the emulsion to ionizing radiation (Fig. 1A). Exposure times were recorded and ranged from 5 to 90 min. Film read-out was performed with a manual densitometer (aperture, 0.1 mm; filter, 600 nm) (TBX; Tobias Associates, Ivyland, PA) equipped with a dedicated precision micrometer mechanism designed to move films over the aperture of the instrument in precise steps of 0.25 mm. This evaluation system (film and densitometer) was calibrated by measuring the optic density of the film exposed to known radiation doses deployed by a calibrated 90Sr/90Y-eye applicator at the National Institute of Standards and Technology.

Phantom measurements to quantify positron penetration into tissue-equivalent medium using MD-55 Gafchromic film. (A) Exposure of film by balloon catheter filled with liquid radioactivity. (B) Exposed film showing concentric blue halo around hole with superimposed 2 rectangular axes for laser scanner read-out. (C) Typical result of evaluation of optical density of film (660 nm) indicating dose-over-depth function.
For evaluation of dose profiles over penetration depth, the optic density of exposed films was measured along 2 perpendicular axes and the radioactive balloons were inserted through the center of the holes. Thus, 2 curves were generated per film, giving 4 declining slopes describing local doses as a function of distance from the surface of the balloon (Fig. 1). For the purpose of comparing energy penetration of different radioisotopes, dose-over-depth curves were fitted by a monoexponential function and the half-dose depth was calculated using the approximated function.
In Vitro Experiments with Vascular Smooth Muscle Cells
Cultures of bovine aortic smooth muscle cells (BASMCs) were obtained by outgrowth from medial explants of thoracic aortas of cows within 4 h of slaughter. Initial outgrowth and established cells were maintained in culture using Dulbecco’s Modified Eagle’s Medium (DMEM) supplemented with 10% fetal bovine serum (FBS) in a humidified incubator equilibrated with a 5% CO2 atmosphere. Media were replaced every 3 d and cells were passaged every 7–10 d. All experiments were performed using cells that had been passaged ≤12 times. These cells exhibited typical morphologic characteristics of vascular smooth muscle in vitro and showed specific immunoperoxidase staining by a monoclonal antibody selective for smooth muscle α-actin.
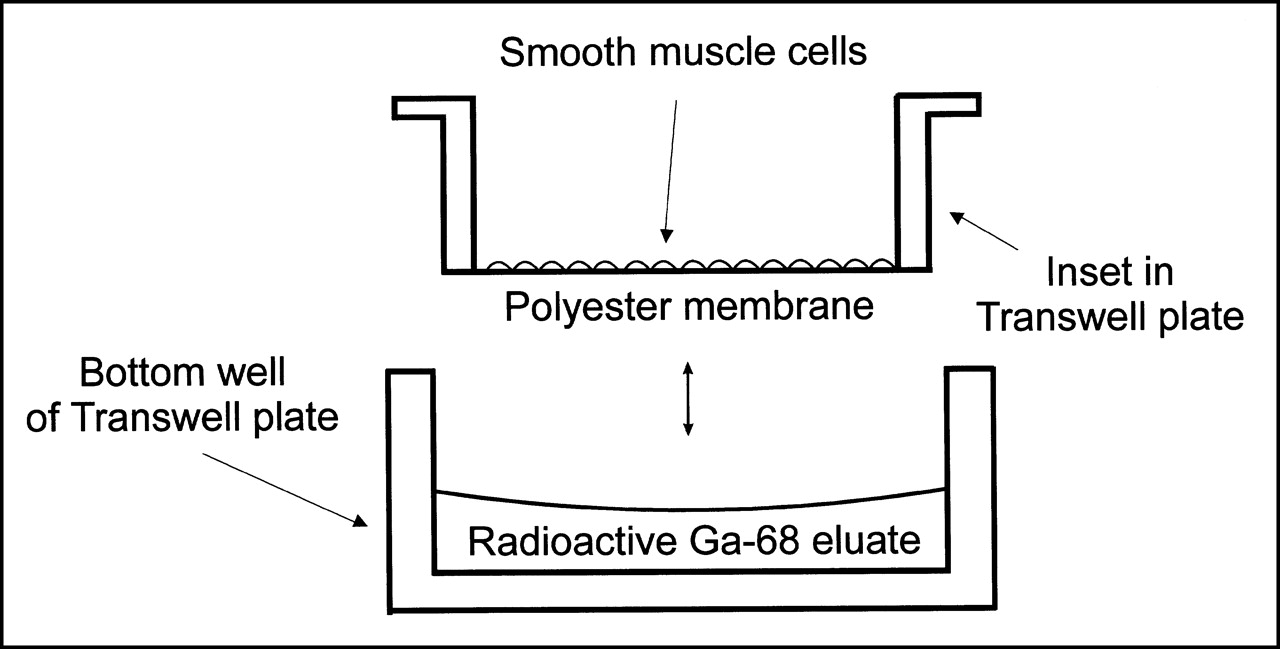
Smooth muscle cells growing on the surface of thin polyester membranes in the inset of conventional 6-well plates were exposed to positron radiation originating from liquid 68GaCl3 in direct fluid contact with the other side of this membrane. To avoid diffusion of the radioactive fluid through the membrane into the cell culture, thin polyester film (Parafilm; American National Can, Chicago, IL) was used for sealing. This particular radiation geometry is illustrated in Figure 2. This experiment included irradiation of 108 individual cultures (9 different doses, 6 different time points, double measurements).

Geometry for irradiation of bovine aortic smooth muscle cells with positron radiation emitted by liquid 68Ga. Diffusion of radioactive 68Ga atoms into cell culture was prevented by Parafilm sealing of polyester membrane separating cells from liquid radiation source.
Another series of 84 BASMC cultures (7 different doses, 6 different time points, double measurements) was treated with 0.66-MeV γ-radiation originating from a 137Cs source. Controlled dosage was obtained using an automated irradiation device (Gamma-Bestrahlungsanlage, Modell OB 29/4; STS Steuerungstechnik Strahlenschutz GmbH, Braunschweig, Germany) designed to irradiate blood bags before transfusion into patients.
Positron and γ-radiation at doses between 0 and 32 Gy were used to treat contact-inhibited cells in monolayers with cellular densities ranging from 70,000 to 100,000 cells/cm2. Immediately following the treatment, irradiation cells were trypsinized, passaged, and seeded into 6-well tissue-culture plates at approximately 10,000 cells/cm2. Cells were allowed to proliferate further under normal conditions with DMEM + 10% FBS. This experimental approach was chosen to simulate most closely the biologic status of smooth muscle cells residing in the wall of a coronary artery, where cells are normally quiescent but receive a proliferative stimulus at the time of angioplasty.
At 1, 3, 7, 11, and 15 d after irradiation, cells were trypsinized with Hanks’ balanced salt solution containing trypsin (0.5 mg/mL) and ethylenediaminetetraacetic acid (0.5 mmol/L) at each time point and counted with a standard hemocytometer. Staining with trypan blue was used for quantification of the fraction of dead cells. Each well was counted in duplicate, and cell counts were reported as mean ± SD. Morphologic appearance of cells was checked on a daily basis by phase–contrast microscopy and documented on color slide film using a 35-mm camera (OM-2; Olympus America, Melville, NY). To compare the antiproliferative effect of positrons with that of γ-radiation, ED50 and ED80 values were determined from the dose–response curves generated for the final cell counts obtained at day 15.
Modeling of Balloon Rupture and Laboratory Spill Scenario
Balloon Rupture.
Whole-body and organ doses a patient would theoretically receive because of an accidental balloon rupture under worst-case conditions were estimated. This estimation used published isotope-specific whole-body and organ doses that accrue after intravenous injection (9). These dose estimates resulted from theoretic modeling and rely on pharmacokinetic data measured with the individual radioisotopes in humans (10). Assuming a complete loss of an in-balloon activity of 1.85 GBq, Table 2 provides dose estimates for the investigated positron emitters together with recently published whole-body dose estimates for the intravascular loss of the same 188Re activity (8,11) with and without systemic perchlorate blockage (12–14). Because 188Re and 99mTc are chemically very similar, ICRP data for organ doses after systemic administration of 99mTc (9) were used to estimate 188Re organ doses by extrapolating the relative contribution of 99mTc organ doses to the 99mTc whole-body dose.
Whole-Body Dose Estimates* to a Patient After Accidental Systemic Loss of 1.85 GBq (All Values in mSv)
Operator Doses.
Estimates for radiation exposure of the interventional cardiologist doing the intracoronary radiation therapy were made based on model calculations assuming that positron radiation originated from a point source 5-cm deep inside the patient’s chest over a typical dwell time of 4 min. Further assumptions were an operator-to-patient distance of 1 m and complete positron absorption within the patient, such that only 511 keV of annihilation radiation reached the operator. Thus, operator doses were independent of the individually used positron emitter. X-ray–induced operator doses reported for typical diagnostic and interventional procedures (15) were used for comparison.
Spill of Liquid Radioactivity.
Another model calculation was made for estimating operator and personnel exposure caused by a spill of liquid 68Ga in the catheter laboratory. We assumed a loss of 370 MBq (20% of in-balloon activity) that would form a single spot on the floor, and assumed further that 50% of the spot activity could be successfully removed by decontamination. We also assumed that 2-cm–thick rectangular acrylic bars were used to cover the spot so that positrons were completely absorbed. Exposure rates for personnel standing on the contaminated area within reach of the penetrating 511-keV annihilation radiation were calculated at a distance of 30 cm from the source.
Statistical Analysis
All continuous variables represent mean values from duplicate experiments and are presented as mean ± SD, indicated by the error bars in Figures 3 and 4. ED50 and ED80 values for comparison of the antiproliferative efficacy of positrons with γ-radiation were determined by approximation of a sigmoidal function to the dose–response curves based on cell counts obtained at day 15. The Mann–Whitney rank sum test was used for statistical comparison.
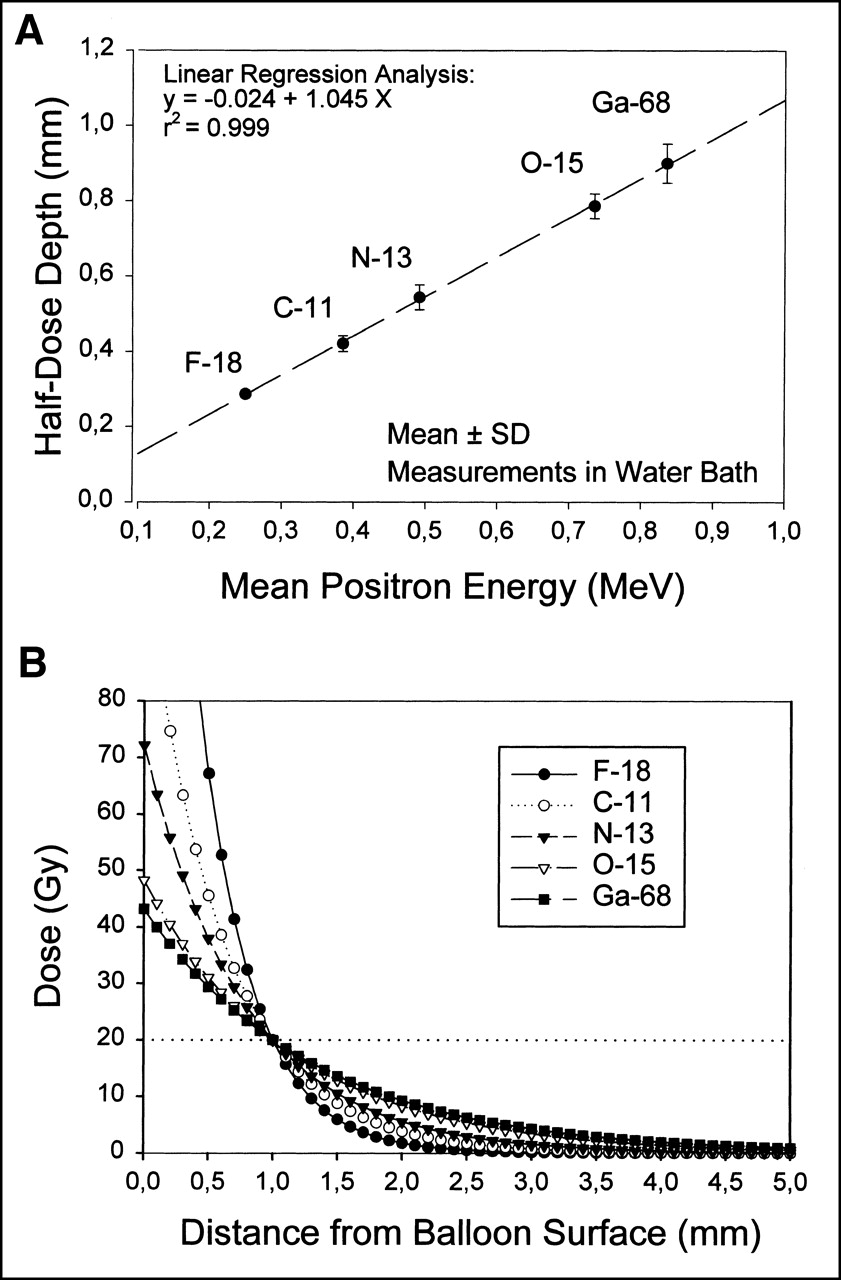
Results of phantom measurements. (A) Dependence of half-dose depth on mean positron energy measured with radiation-sensitive MD-55 Gafchromic films in water bath. Linear function is described by d½ = 0.024 + 1.045 Emean. (B) Dose-over-depth functions calculated from phantom measurements. Curves are normalized to dose of 20 Gy at 1 mm distance from balloon surface. Only 15O and 68Ga have acceptable dose distribution due to sufficient positron energy.
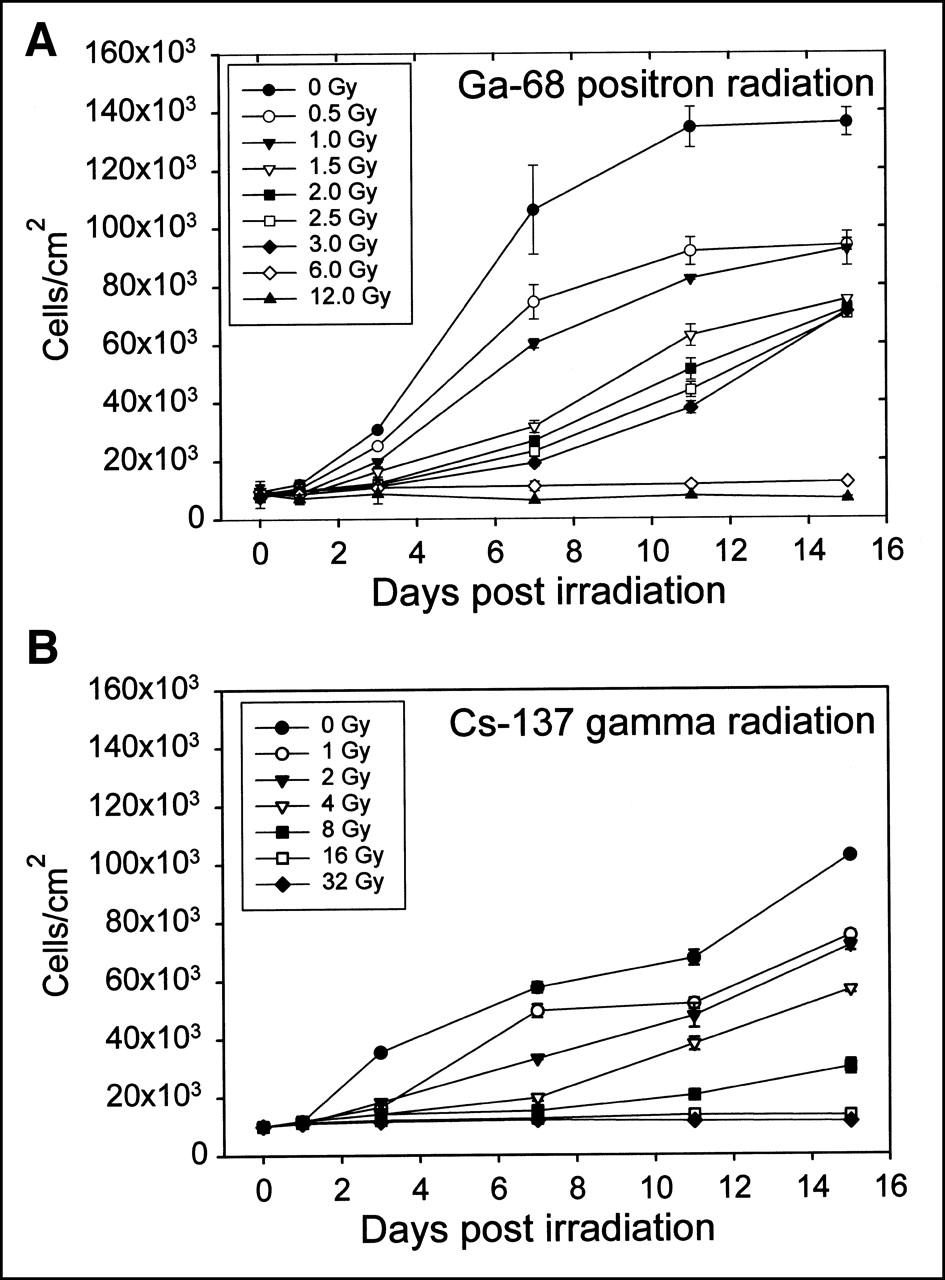
Dose–response curves characterizing the impact of 68Ga positron radiation (A) and 137Cs γ-radiation (B) on proliferation of cultured bovine smooth muscle cells.
Results
Dosimetric Measurements with Radiosensitive Film
Each film irradiated with positron radiation showed a blue halo concentrically expressed around the hole in the film where the radioactive balloon was inserted (Figs. 1A and 1B). These halos formed as a response of the self-developing emulsion to the absorbed dose. The blue color did not extend further than 4–5 mm beyond the edges of the hole, indicating a steep dose decline over distance from the balloon surface. None of the films showed blue color on the margins outside the halo. Thus, doses caused by the more penetrating annihilation radiation (511 keV) were, in general, below the detection threshold of the films (1 Gy).
Quantitative analysis of the dose-over-depth profiles evaluating optic density along 2 rectangular axes confirmed that monoexponential fitting of the obtained curves was possible with sufficient precision (r2 > 0.98), such that half-dose depth values could be reasonably calculated (Table 1). These values describing the potential capability of positron radiation to penetrate into tissue ranged from 0.29 ± 0.01 mm (18F) to 0.90 ± 0.03 mm (68Ga) and were found to be strictly linear, depending on positron energy. A function to describe this dependence was approximated by linear regression analysis (Fig. 3A) and is given by the term
 where d1/2 is half-dose depth (mm) and Emean is mean positron energy (MeV) (r2 = 0.999).
where d1/2 is half-dose depth (mm) and Emean is mean positron energy (MeV) (r2 = 0.999).
Endothelial Doses
Endothelial doses accruing in close contact with the balloon surface are generally higher than the desired adventitial target doses. The discrepancy between these 2 doses directly depends upon the slope of the absorption curves. Figure 3B displays a theoretic family of curves describing dose decline over tissue depth for each of the investigated radioisotopes. The functions in this graph were normalized arbitrarily to a dose of 20 Gy targeted to a prescription point located 1 mm remote from the balloon surface. 68Ga, with the highest half-dose depth, has the shallowest absorption profile, whereas the dose-decline of 18F is the steepest. For the assumed target dose of 20 Gy at a distance of 1 mm remote from the balloon surface, the endothelial doses were 43 Gy for 68Ga, 48 Gy for 15O, 72 Gy for 13N, and >100 Gy for 11C and 18F. Figure 3B also shows that doses measured at distances >5 mm from the balloon surface are negligible. Thus, coronary radiation therapy with positron-emitting radioisotopes provides for a focal dose deposition similar to approaches using β-radiation.
Inhibition of Cellular Proliferation
The main result of our cell culture experiments using positron and γ-radiation was the dose-dependent inhibition of smooth muscle cell proliferation observed in all experiments. Cells in unirradiated cultures generally proliferated most rapidly in each individual experiment. Proliferation rates declined with increasing doses in the range between 1 Gy and 6 Gy. Doses above 6 Gy sterilized the cultures such that no proliferation was observed anymore. There was also no stimulation of growth in cultures irradiated with low doses. The biologic response of smooth muscle cells to radiation is quantitatively described in more detail by Figure 4.
Trypan blue nuclear staining detected a fraction of dead cells per culture that was generally below 20%. There was no detectable relation between the fraction of stained cells and doses applied, including unirradiated control cultures.
The quantitative antiproliferative efficacy of positron and γ-radiation to inhibit proliferation was found to be similar. Averaged ED50 and ED80 values for inhibition of proliferation were 2.5 ± 0.4 Gy (mean ± SD) and 4.4 ± 0.8 Gy for positrons, and 3.8 ± 0.2 Gy and 8.0 ± 0.3 Gy for γ-radiation, respectively. The differences were not statistically significant.
Evaluation of Cell Morphology
We observed morphologic changes of cultivated cells as an immediate response to radiation. Unirradiated control cells generally had a spindly slim outer shape, whereas irradiated cells were plumper and had enlarged nuclei. There was an average of 3–4 mitoses per low-power field in the control cultures, whereas mitoses in cultures that were effectively growth inhibited were observed only occasionally. These morphologic abnormalities were seen 3 d after irradiation and persisted until termination of cultures after 15 d. However, even cells irradiated with the highest doses maintained their capability to attach and adhere to the surface of the cell culture flasks once they were split immediately after irradiation.
Theoretic Patient Doses in Case of Balloon Rupture
The potential hazard of accidental patient radiointoxication is small compared with the investigated positron emitters because of the radioisotopes’ short half-lives. Table 2 lists theoretic estimates for whole-body and organ doses accruing after a complete intravascular loss of an in-balloon activity of 1.85 GBq. Remarkably, the highest effective whole-body dose of any investigated positron emitter is only 50 mSv. This dose is on the upper margin of the annual cumulative dose maximally allowed for professionally radiation-exposed personnel and is considered safe. The highest organ doses among the positron emitters are 314 mSv for the bladder (18F) and 85.1 mSv for bone marrow (68Ga). The low theoretic positron emitter doses compare favorably with x-ray–induced patient doses accruing during a standard interventional procedure (skin entrance dose, approximately 400 mSv/15 × 15-cm field) (15), and are far below the threshold of 500 mSv, above which physiologic changes caused by acute radiation exposure have been described.
In contrast, an intravascular loss of an equal 188Re activity may result in much more severe radiointoxication with an estimated whole-body dose of 777 mSv (11) without perchlorate blockage and 296 mSv with perchlorate blockage (12). Critical organs for 188Re are the stomach (1,733 mSv), the bladder (1,136 mSv), and the ovaries (598 mSv). Perchlorate administration reduces these doses to 179 mSv (stomach) and 263 mSv (ovaries). The remaining doses to critical organs are still 6–20 fold higher than the highest theoretic positron emitter doses. Moreover, the perchlorate-induced reduction of doses to some organs occurs at the expense of significantly increased doses to the bladder (1,787 mSv) and testes (179 mSv).
Operator Exposure During Treatment and Caused by a Spill
The results of our theoretic modeling showed that even with positron emitters that produce penetrating 511-keV annihilation radiation, the majority of the dose to the operator accruing during a typical interventional treatment was caused by x-ray imaging (50–160 μSv). Only a comparably small increment of 6 μSv would be caused by positron annihilation radiation, assuming a typical dwell time for coronary irradiation of 4 min (Table 3).
Estimates for Operator-Received Doses Caused by Different Radioisotopes for Coronary Radiation Therapy: Comparison with Fluoroscopy
The exposure rate for personnel after a spill of any of the investigated positron emitters was estimated to be 111 mR/h/MBq at a distance of 30 cm from the radioactive spot once positron radiation was absorbed by appropriate acrylic shielding. According to our modeling assumptions, an initial dose rate of 15 mR/h would result from a spill of 185 MBq. After 3.5 h, rapid radioisotope decay would cause the remaining dose rate to fall to 2 mR/h. Thus, a spill scenario may effectively be mastered with immediate decontamination and acrylic shielding.
Discussion
The primary concerns with liquid-filled balloons for intracoronary radiation therapy is accidental balloon rupture or leakage with subsequent patient exposure or spillage of the therapeutic activity. This study seeks to support the hypothesis that even in such incidents, positron emitters provide significantly enhanced safety because of their short half-lives while maintaining full antirestenotic efficacy. We believe that this is the first study systematically investigating the majority of clinically available positron emitters for their potential usefulness for a safer coronary radiation therapy with liquid-filled balloons.
188Re is the most intensively investigated radioisotope for intracoronary radiation therapy with liquid-filled balloons (2,3,7,8,11,12). With a relatively short half-life of 17.0 h, it represents the safest choice to date. Hausleiter et al. (16) recently reported a case of balloon leakage with 188Re and perchlorate pretreatment in which only 10% of the in-balloon volume (150 MBq) was lost into the patient’s circulation. Dose estimations made for this particular accident resulted in 18 mSv to the whole body, and 220 mSv to the bladder wall (16). As reported, these doses were of little clinical concern in this particular patient. However, this accident represents a very favorable outcome of balloon leakage. Thus, the interventional cardiologist is left with the concern that substantially more than 10% of the in-balloon volume could be lost into the patient in other cases of balloon rupture or leakage, despite low inflation pressures. Conversely, had this accident occurred with 68Ga instead of 188Re, it would have resulted in a drastically lower patient exposure (whole-body dose of 3.0 vs. 18 mSv; bladder dose of 3.2 vs. 220 mSv). These differences are important and underline the safety gain achievable with 68Ga.
The pathophysiology of restenotic renarrowing of a coronary artery after balloon angioplasty includes elastic recoiling, smooth muscle cell proliferation and migration, synthesis of extracellular matrix, and late constrictive remodeling. These processes are initiated and controlled by adventitial cells like myofibroblasts (17) or macrophages (18), whereas the bulk of intraluminal restenotic tissue is formed by rapidly dividing smooth muscle cells. Thus, the shoulders of the balloon-induced transmedial tear from which smooth muscle cells originate and the adventitial cell lines need to be targeted with effective radiation doses. As such, it is important that therapeutic radiation emerging from an intracoronary source should have the potential to penetrate deep enough into vascular tissue for reaching the adventitia. However, it is also desirable that the radiation treatment is focused enough to ensure that the bulk of radiation energy is deployed within a few millimeters of the endothelial vessel wall.
We found that the half-dose depth of positron penetration depends upon positron energy. Assuming that the wall thickness of a diseased coronary artery is ≤1.0–1.5 mm, we concluded that the limited penetration capability of positrons emitted by 18F, 11C, and 13N may not be sufficient for targeting adventitial cell populations in a clinical setting. Only the more energetic positrons emitted by 15O and 68Ga would penetrate deep enough in the vessel wall for effective interaction with adventitial cells. The limited energy of 18F-, 11C-, and 13N-positrons has the other unfavorable consequence that very high luminal doses will emerge once dosimetry is tailored to an adventitial target using a prescription point 1 mm remote from the luminal surface (Fig. 3B).
A short physical half-life was the criterion under which the radioisotopes in this study were selected. However, too rapid isotope decay would make reliable intraprocedural dosimetry difficult. This limitation applies to 15O (with the shortest half-life of only 2.1 min in this study) and to 62Cu, a positron-emitting radioisotope with a half-life of only 9.74 min that was recently suggested for use in liquid-filled balloons by Chan et al. (19).
68Ga appears to be best suited for further consideration. Its half-life of 67.6 min was comfortably controlled by our dosimetry program. Another favorable feature of 68Ga was its simple availability from a 68Ge/68Ga radioisotope generator, which can be maintained on-site in any hospital with a nuclear medicine department.
We used the only commercially available generator to date (Dupont Pharma), a system designed to create line sources for transmission scans in PET studies. Although this generator does not give its dose in the desired small volume necessary for liquid-filled balloons, there are no principle obstacles preventing such modification in the future. The long shelf life of 6–9 mo makes the generator cost-effective because, assuming that 3 elutions per workday were performed over a period of 6 mo, a single therapeutic dose would cost roughly U.S. $130.
Another objective of this study was to ascertain that positron radiation has antiproliferative efficacy comparable with that of previously investigated radiation qualities (i.e., γ- and β-radiation). The in vitro experiments performed with bovine aortic smooth muscle cells found that cellular proliferation rates are inversely related to dose in cultures irradiated with both positron and γ-radiation. The calculated ED50 and ED80 values indicated that both types of radiation are equally effective, at least in these in vitro experiments. Stimulatory rather than suppressive effects of subtherapeutic doses, as reported from previous porcine studies with β-radiation (20), were not observed. Another interesting finding was that the cell death rate was low (generally below 20%), although cultures irradiated with doses higher than 6 Gy were completely sterilized. This finding was compatible with the assumption that doses in the investigated range induce only sublethal radiation damage, probably caused by DNA double-strand breaks rather than cell killing. Therefore, irradiated cells will not die as long as they do not enter into cell cycle for replication.
Although the antiproliferative effect of positron emitters is similar to that of β- and γ-radiation, the balloon rupture-related patent exposure is much less severe with short-lived positron emitters than with 188Re or other radioisotopes. Taking into consideration the whole-body and organ doses listed in Table 2, a patient suffering an accidental intravascular balloon rupture would receive an uncritical maximal whole-body dose of 50 mSv with 68Ga under worst-case circumstances. The same accident with 188Re would provoke a 6-fold higher whole-body dose of 296 mSv and a series of concerning organ doses even once perchlorate blockage of 188Re uptake was performed. These data documented the most substantial advantage of using short-lived positron emitters and underlined the validity of the basic premise on which this study was performed.
Conclusion
Based on documented high penetration capability, generator availability, and proven antiproliferative efficacy, we suggest that 68Ga be considered as an attractive candidate for safe and efficient coronary radiation therapy with liquid-filled balloons. We believe that this approach may warrant further experimental and clinical testing.
Acknowledgments
The authors thank the staff of the cyclotron laboratory serving the Indy-PET scanner for technical assistance in isotope preparation. Nicole Karthein is also acknowledged for her excellent help with cell-culture preparations. The study was supported by a research grant provided by Guidant Corporation and a stipend from Max-Kade Foundation, New York, NY.
Footnotes
Received Sep. 26, 2000; revision accepted Jan. 24, 2001.
For correspondence or reprints contact: Hans-Peter Stoll, MD, Medical Clinic III, Cardiology, University Hospital Homburg/Saar, 66421 Homburg/Saar, Germany.




{kind=link}
{kind=link}
{kind=link}
{kind=link}