


Abstract
Intraarterial thrombolytic therapy has been used recently for treatment of acute ischemic stroke within 6 h after onset. Although hypoactivity of 99mTc-hexamethylpropyleneamine oxime (HMPAO) in stroke has been well documented, hyperactivity of HMPAO has not been evaluated in sufficient detail. The purpose of this study was to evaluate the incidence and clinical importance of hyperactivity of HMPAO in management of patients with acute ischemic stroke. Methods: We retrospectively investigated HMPAO SPECT in 90 patients with acute ischemic stroke within 6 h after onset. The lesion-to-contralateral radioactivity ratios (L/Cs) were calculated on the SPECT images before treatment and were compared with the imaging results of CT or MRI (or both). Results: Hyperactivity of HMPAO, accompanied by surrounding hypoactivity, was observed in 6 of 90 patients (7%) within 6 h after onset. The L/Cs ranged from 1.17 to 2.95. Two patients showed hyperactivity in the cortex and the other 4 patients showed hyperactivity in the basal ganglia. Angiography confirmed spontaneous recanalization of occluded vessels in accordance with the area of hyperactivity. In both patients with cortical hyperactivity, cerebral infarctions were revealed on follow-up CT; in 1 patient, hemorrhagic transformation developed after intraarterial thrombolytic therapy. In 3 of the 4 patients with hyperactivity in the basal ganglia, follow-up CT showed no infarction in the surrounding hypoperfused cortex (selective intraarterial thrombolytic therapy was performed on 2 patients), although various degrees of infarction were observed in the basal ganglia. Obvious infarctions developed in the basal ganglia and the cortex of the other patient. Conclusion: Hyperactivity of HMPAO could be seen in the basal ganglia and the cortex within 6 h after onset, reflecting spontaneous recanalization. The areas of hyperactivity may develop infarctions, whereas the accompanying areas of hypoactivity could be rescued by selective intraarterial thrombolytic therapy.
Intraarterial thrombolytic therapy has been performed to rescue the ischemic brain and improve neurologic outcome in patients with acute ischemic stroke (1). In general, the critical time range for intraarterial thrombolytic therapy is <6 h after onset (1,2). SPECT with 99mTc-hexamethylpropyleneamine oxime (HMPAO) has been reported to be useful for evaluating brain tissue reversibility before treatment and for predicting the outcome (3–9). Hypoactivity of HMPAO in the area of ischemia has been well documented in relation to the indications of thrombolytic therapy, whereas hyperactivity of HMPAO within 6 h after onset has not been well elucidated.
HMPAO hyperactivity has been well documented in the subacute phase of cerebral infarction, and it usually occurs at the site of infarction (10–12). HMPAO hyperactivity is much less common during the acute phase of ischemic stroke (12,13), and the outcomes of HMPAO hyperactivity were different in several reports (4,12,14–16). Moreover, most of the SPECT images evaluated in previous studies were acquired in the acute but relatively late phase (usually after 5–6 h after onset), whereas the critical time range for intraarterial thrombolytic therapy has been reported to be <6 h after onset. Thus, the predictive value of HMPAO hyperactivity for infarction in the acute ischemic stroke is still controversial.
Shimosegawa et al. (4) reported cases of HMPAO hyperactivity within 6 h after onset of ischemic stroke, and in all cases HMPAO hyperactivity developed into low-density areas on follow-up CT. Although Shimosegawa et al. reported cases of hyperactivity only in the cortex, we have encountered some cases of hyperactivity in the basal ganglia as well, which were accompanied by areas of cortical hypoactivity corresponding to the site suggested by clinical symptoms. The purpose of this study was to evaluate the incidence and final outcome of HMPAO hyperactivity within 6 h after the onset of ischemic stroke, with reference to indications of intraarterial thrombolytic therapy.
MATERIALS AND METHODS
Ninety consecutive patients (50 men, 40 women; age range, 35–91 y; mean age ± SD, 69 ± 11 y), whose clinical diagnosis was acute ischemic stroke and whose brain SPECT scans with HMPAO were performed within 6 h after onset, were retrospectively evaluated. After completion of brain SPECT, 48 of the 90 patients (53%) were treated with intraarterial thrombolytic therapy. The time of onset was determined by reliable information obtained from the patients or their relatives (or both) and rounded to the nearest hour. Written informed consent was obtained from all patients or their relatives.
CT was performed on all patients on admission to exclude intracranial hemorrhage. Patients who had lacunar infarction or a clear low-density area on CT corresponding to the site suggested by clinical symptoms and who had critical systemic conditions were also excluded from the study. SPECT with HMPAO was performed using a rotational gamma camera (GCA 602A; Toshiba, Tokyo, Japan) or a 4-head gamma camera (SPECT 2000H-40; Hitachi, Tokyo, Japan) equipped with a low-energy, high-resolution collimator. Patients were injected with 740–1,110 MBq (20–30 mCi) HMPAO prepared immediately after CT scanning. About 5 min later, SPECT data were acquired with 12 s per view in 60 views by the single-head gamma camera and with 10 s per view in 64 views by the 4-head gamma camera. Both data acquisitions were performed in a 64 × 64 matrix and completed within about 12 min. The data were reconstructed using Butterworth-filtered backprojection and a slice thickness of 7 mm for the former camera and 4 mm for the latter camera. Attenuation correction was performed by Chang’s method (17). The estimated error of this method was <5% by regions-of-interest (ROIs) analysis (4). Linearization correction proposed by Lassen et al. (18) was performed by assuming that the normal cerebellar blood flow was 55 mL/100 g/min.
The ROIs were placed symmetrically on the lesion (i.e., the hypoactivity area corresponding to the site suggested by clinical symptoms) and on the contralateral normal brain. When the hyperactivity areas were visually observed within or adjacent to the lesions, the ROIs were also placed on the area of hyperactivity. The lesion-to-contralateral radioactivity ratios (L/Cs) were calculated and compared with the results of CT or MRI (or both).
RESULTS
Hyperactivity of HMPAO was detected in 6 of 90 patients (7%) within 6 h after onset. Clinical information and the imaging findings of these patients are summarized in Table 1. All areas of hyperactivity were surrounded or adjoined by areas of hypoactivity (except in 1 patient) corresponding to the site suggested by clinical symptoms. Two patients (patients 1 and 2) showed hyperactivity in the cortex and the other 4 patients (patients 3–6) showed hyperactivity in the basal ganglia. Angiography (performed on patients 1, 3, and 6), which was performed immediately after SPECT scanning, confirmed spontaneous recanalization of occluded vessels in accordance with the area of hyperactivity because they showed capillary blush or early venous filling (or both) in the corresponding vascular territory. Both patients with cortical hyperactivity showed cerebral infarction on subsequent CT; in 1 patient, hemorrhagic transformation occurred after intraarterial thrombolytic therapy (Fig. 1). In 3 of the 4 patients with hyperactivity in the basal ganglia, follow-up CT showed no infarction in the surrounding hypoperfused cortex (selective intraarterial thrombolytic therapy was performed on 2 patients), although small infarctions were observed in the basal ganglia (Fig. 2). Infarctions developed in the basal ganglia and the cortex of the other patient (patient 4) without thrombolytic therapy.
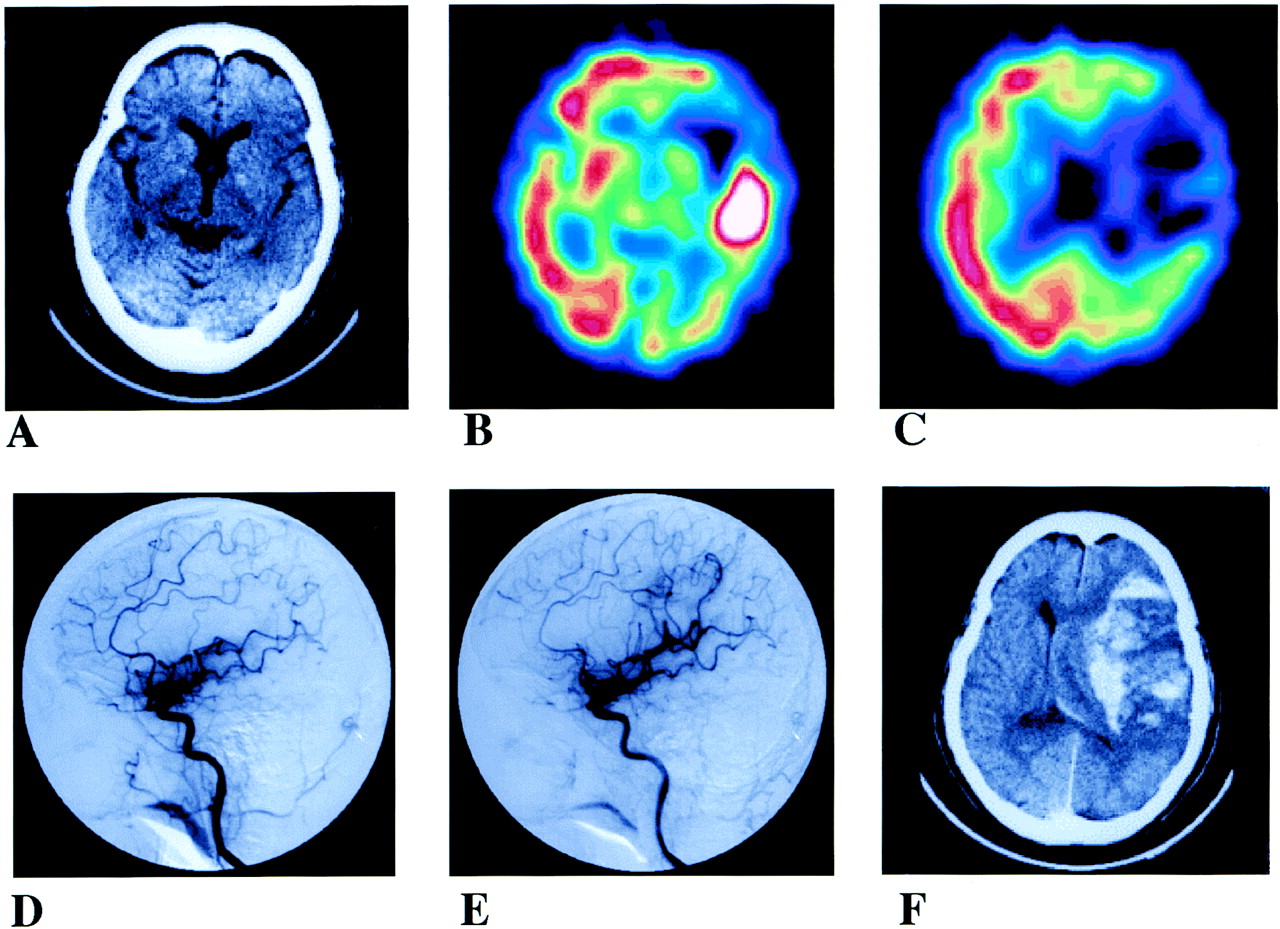
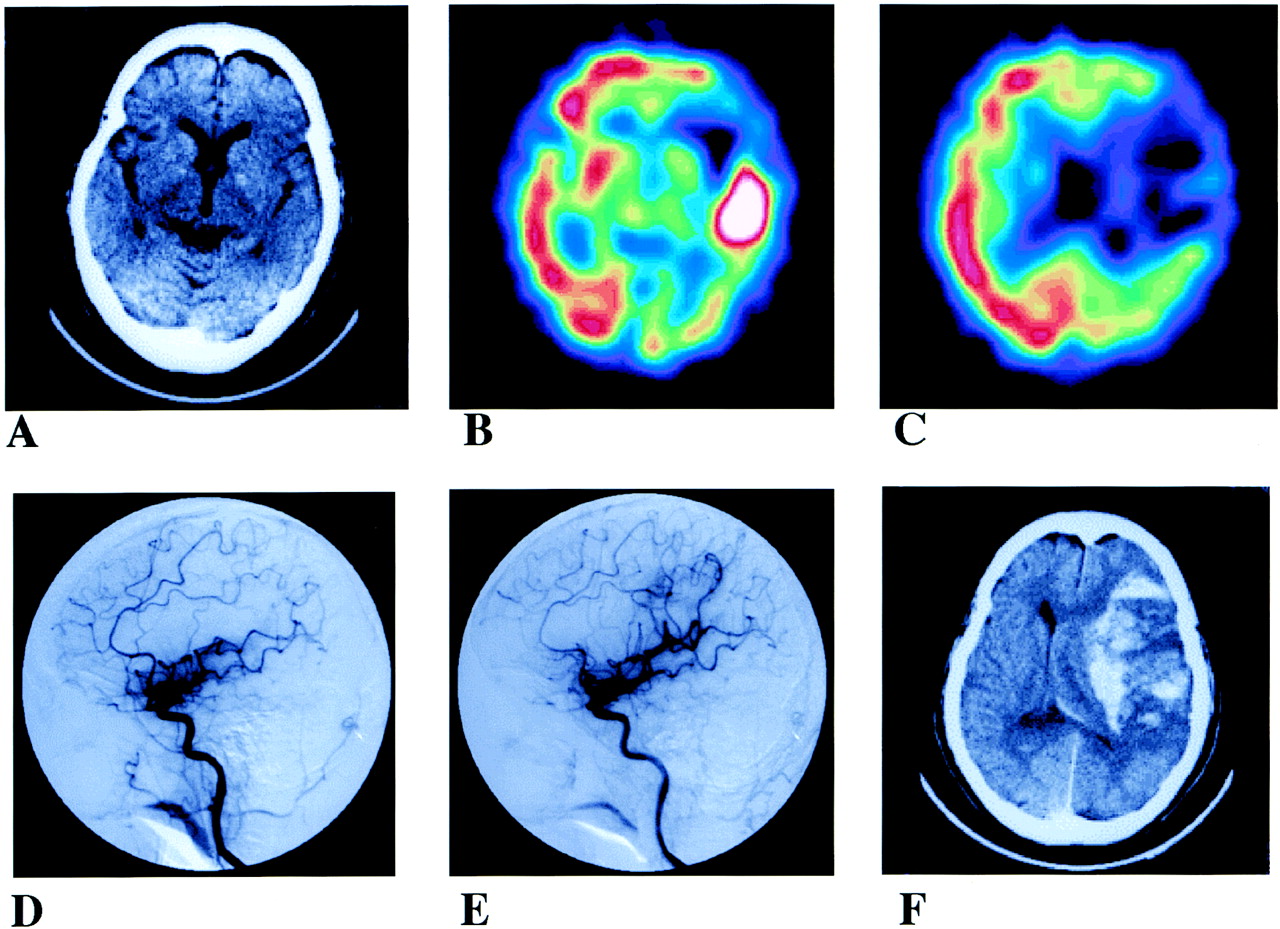
A 70-y-old woman (patient 1) with right hemiparesis and aphasia. (A) CT image obtained 1.5 h after onset shows no definite abnormal density. (B and C) SPECT images with HMPAO obtained 3 h after onset show area of hyperactivity in left temporal cortex with surrounding cortical hypoactivity. L/C of area of hyperactivity is 2.95 and that of area of hypoactivity is 0.33. (D) Angiogram (lateral view) of left internal carotid artery (ICA) obtained 3.5 h after onset (before treatment) shows middle cerebral artery (MCA) occlusion but spontaneous recanalization (i.e., capillary blush and early venous filling) in temporal region. (E) Angiogram (lateral view) of left ICA obtained 4.5 h after onset (after intraarterial thrombolysis) shows partial recanalization of left MCA. (F) CT image obtained 9 h after onset shows hemorrhagic transformation with extensive brain edema in left temporal region.

A 64-y-old man (patient 3) with right hemiparesis and aphasia. (A) SPECT image obtained 2 h after onset shows remarkable hyperactivity in left basal ganglia with surrounding cortical hypoactivity in left middle cerebral artery (MCA) territory. L/C of area of hyperactivity is 2.64 and that of area of hypoactivity is 0.48. (B) Angiogram of left interrnal carotid artery (ICA) obtained 3 h after onset (before treatment) shows occlusion of distal horizontal portion of left MCA, whereas spontaneous recanalization (i.e., capillary blush) is seen in perforating arteries. (C) Angiogram of left ICA after intraarterial thrombolytic therapy shows complete recanalization of left MCA. (D) SPECT image obtained on day 3 shows normalized perfusion in left MCA territory. (E) CT image obtained on day 3 shows small and slightly decreased density area in left basal ganglia but cortex of left MCA territory is normal. (F) Follow-up SPECT image 3 mo later shows slightly decreased activity in left basal ganglia and cortex.
Clinical Information of Patients with HMPAO Hyperactivity
DISCUSSION
In this study, hyperactivity of HMPAO was observed in 6 of 90 patients (7%) with the acute phase of ischemic stroke within 6 h after onset. This incidence is similar to that reported by Shimosegawa et al. (4). Although cases of cortical HMPAO hyperactivity have been reported (4), we also found hyperactivity in the basal ganglia.
Hyperactivity of HMPAO has usually been observed in the subacute phase of cerebral infarction (10–12). During the subacute phase, relatively increased cerebral blood flow (CBF) and decreased oxygen metabolism (i.e., luxury perfusion) (19) could occur in the areas of infarction, reflecting altered blood–brain barrier and new capillary formation with loss of autoregulation. Although hyperactivity of HMPAO seen in the subacute phase did not always indicate hyperperfusion (or hyperfixation) (11,20), areas of HMPAO hyperactivity usually turned into complete infarction in the chronic phase.
It has been reported recently that hyperactivity of HMPAO could occur in the acute phase of infarction, and it has usually been reported to reflect hyperperfusion derived from reperfusion in the ischemic area (4,12,15,20). However, the outcomes of hyperperfusion have been different in several reports (4,12,14–16,21–23). Baird and Donnan (12) reported that the area of hyperactivity of HMPAO was seen in 7% of cases (11/170) within 48 h after onset and was usually normal on follow-up CT. Marchal et al. (23) reported in a PET study that the area of hyperperfusion in the acute phase showed little or no metabolic alternation and was associated with excellent recovery. In contrast, Shimosegawa et al. (4) and Shintani et al. (15) reported patients with HMPAO hyperactivity in the acute phase (within 6 h after onset), in whom obvious infarctions were confirmed on follow-up CT.
Olsen and Lassen (22) reported in a 133Xe intracarotid injection study that focal cerebral hyperemia was found in 29% of cases (21/73) of acute ischemic stroke within 72 h. Three different types of hyperemia were reported: border-zone hyperemia (n = 8) with occluded arteries seen in the border zone of acute infarcts; postischemic hyperemia (n = 8) without occlusion (presumably associated with recanalization) seen in infarcts (n = 5) and noninfarcts (n = 3); and remote hyperemia (n = 5) seen at some distance from the infarcted area (21,22). Postischemic hyperemia was usually more severe than the other 2 types of hyperemia, but it did not always lead to cell necrosis (22). In our study, HMPAO hyperactivity was considered as postischemic hyperemia in 4 of the 6 patients (patients 1, 3, 4, and 6) because recanalization was confirmed in the area corresponding to the area of hyperactivity. However, the type of hyperperfusion was undetermined in patients 2 and 5.
Similar to the results reported by Shimosegawa et al. (4), the areas of HMPAO hyperactivity within 6 h after onset changed into the low-density areas on follow-up CT in our study, although the degrees of infarction were varied. In the cases of cortical hyperactivity, almost the same size of infarction was observed, whereas the size of the infarct was smaller than that of the area of hyperactivity in the cases of basal ganglia hyperactivity. Thus, hyperactivity of HMPAO could occur in reversible and irreversible brain tissue after reperfusion. In other words, it was difficult to estimate the tissue viability solely by the CBF image.
In the area of hypoperfusion, it may be possible to estimate the tissue reversibility by the duration of ischemia and the degree of hypoperfusion (4,7,9). Shimosegawa et al. (4) reported that the infarcted and noninfarcted brain could be distinguished by an L/C of 0.6 within 6 h after onset. Ezura et al. (7) reported that a residual relative regional cerebral blood flow (rCBF) of ≥70% did not develop infarction, and they recommended that patients with a residual relative rCBF between 35% and 70% might be good candidates for intraarterial thrombolytic therapy. Indeed, in our patients without thrombolytic therapy, the areas of mild hypoperfusion (patients 2 and 5) did not develop infarction, whereas the area with an L/C of <0.6 developed infarction (patient 4). The hypoperfusion areas with L/Cs between 0.35 and 0.60 were salvaged by thrombolytic therapy (patients 3 and 6). In contrast, as seen in patient 1, a residual relative rCBF of <35% may put a patient at risk for hemorrhage even if successful recanalization could be achieved within 6 h after onset (5,7,9).
Thus, prediction of tissue viability in the hypoperfusion area could be done by assessing the duration and degree of ischemia after onset. However, prediction of tissue viability in the area of hyperperfusion is difficult. In previous experimental studies, a threshold-type relationship between the severity of CBF reduction and the magnitude of postischemic hyperperfusion was reported (24). It has also been shown that the magnitude of postischemic hyperperfusion could be changed by the time course after reperfusion and that various degrees of hyperperfusion could be seen in both severe and mild ischemic areas (24,25). In contrast to the experimental studies, it is difficult to determine the actual time of reperfusion in humans in cases of spontaneous occurrence without obvious improvement of symptoms. Indeed, in this study, defining the actual time of spontaneous reperfusion in all patients was difficult. However, marked hyperperfusion within a few hours (e.g., in patients 1 and 3) may suggest that spontaneous recanalization occurred within a short interval after irreversible tissue damage after the preceding severe ischemia.
We also found hyperactivity in the basal ganglia (4 cases), although it was not reported in the study of Shimosegawa et al. (4). We speculate that the mechanism of hyperactivity in the basal ganglia is as follows: First, the embolus could migrate from the top of the internal carotid artery or from the proximal portion of the middle cerebral artery to the distal portion of the middle cerebral artery. Second, the magnitude of ischemia could be severe in the basal ganglia because of the poor collateral circulation; hence, hyperperfusion could occur after spontaneous recanalization in the basal ganglia.
There is concern about making the decision to use intraarterial thrombolytic therapy in such patients with hyperperfusion within 6 h after the onset of ischemic stroke. The final outcome of the hyperperfusion area could be either reversible or irreversible depending on the preceding depth and duration of ischemia. Severe hyperemia associated with arterial reopening could occur either before or after an infarct was established. An attempt to increase blood flow in an acutely occluded and ischemic area seems to be reasonable, although it is meaningless and possibly harmful if the artery has already opened and the previously ischemic area has already become hyperemic (22).
CONCLUSION
Hyperactivity of HMPAO could be seen within 6 h after the onset of cerebral ischemia, reflecting spontaneous recanalization of occluded vessels. Hyperactivity could occur in the basal ganglia and in the cortex and is usually accompanied by a surrounding area of hypoactivity. Although an area of hyperactivity may develop into various sizes of infarct, the surrounding cortical ischemia could be salvaged when selective intraarterial thrombolytic therapy is possible. It is necessary to pay attention to the areas of hyperactivity and hypoactivity on HMPAO SPECT, especially when intraarterial thrombolytic therapy is considered in patients with acute ischemic stroke.
Acknowledgments
The authors thank the staff in the Departments of Radiology and Neurological Surgery at our institute and also thank Dr. Kenya Murase and Dr. Masaharu Sakoh for their thoughtful suggestions and advice. This article was presented at the 47th Annual Meeting of the Society of Nuclear Medicine, St. Louis, MO, June 3–7, 2000.
Footnotes
Received Feb. 5, 2001; revision accepted May 14, 2001.
For correspondence or reprints contact: Yoshifumi Sugawara, MD, Department of Radiology, Ehime University School of Medicine, Shitsukawa, Shigenobu-cho, Onsen-gun, Ehime 791-0295, Japan.
REFERENCES
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Recommendations for Imaging of Acute Ischemic Stroke: A Scientific Statement From the American Heart Association
- Guidelines and Recommendations for Perfusion Imaging in Cerebral Ischemia: A Scientific Statement for Healthcare Professionals by the Writing Group on Perfusion Imaging, From the Council on Cardiovascular Radiology of the American Heart Association