


Abstract
A33, a monoclonal antibody that targets colon carcinomas, was labeled with 125I or 131I and the relative therapeutic efficacy of the 2 radiolabeled species was compared in a human colon cancer xenograft system. Methods: Nude mice bearing human SW1222 colon carcinoma xenografts were administered escalating activities of 125I-A33 (9.25–148 MBq) or 131I-A33 (0.925–18.5 MBq), 125I- and 131I-labeled control antibodies, unlabeled antibody, or no antibody. The effects of treatment were assessed using the endpoints of tumor growth delay and cure. Results: Tumor growth delay increased with administered activity for all radiolabeled antibodies. Approximately 4.5 times more activity was required for 125I-A33 to produce therapeutic effects that were equivalent to those of 131I-A33. This ratio was approximately 7 for a nonspecific, noninternalizing isotype-matched, radiolabeled control antibody. Unlabeled A33 antibody had no effect on tumor growth. Approximately 10 times more activity of 125I-A33 produced toxicity similar to that of 131I-A33, and this ratio fell to approximately 6 for radiolabeled control antibody. Conclusion: Treatment with 125I-A33 resulted in a relative therapeutic gain of approximately 2 compared with 131I-A33 in this experimental system.
The effectiveness and toxicity of radiolabeled monoclonal antibody (mAb) therapy of tumors are dependent on the radionuclide used. Most clinical treatments and preclinical studies have been performed using 131I, primarily because of extensive clinical experience with 131I in the treatment of thyroid disorders but also because of its availability, ease of labeling, and convenient 8-d half-life. 131I emits β-particles, which provide the majority of the local absorbed radiation dose in targeted sites, and a 364-keV γ-photon. The range of the β-emissions of 131I (approximately 1 mm) is sufficient to irradiate tumor cells not directly targeted by the radiolabeled antibody by cross fire. However, it is also sufficient to irradiate most of the blood-forming cells of the bone marrow. Moreover, the high-energy photon that permits patient imaging gives rise to nonspecific and undesirable irradiation of the whole body.
mAb A33 is a murine IgG2a that recognizes a cell-surface antigen expressed homogeneously in >95% of colon carcinomas but not in normal tissue with the exception of colon epithelium (1). In vitro studies have shown that after binding to cell-surface antigens, mAb A33 is internalized through cytoplasmic vesicles, transported to perinuclear regions, and subsequently exteriorized in an intact form (2). The whole process of uptake, internalization, and release may then repeat. Internalization of iodinated antibodies usually results in rapid deiodination and release of the radioiodine from the cell. However, this is not seen with mAb A33. Prolonged retention of radioactivity in tumor sites was observed in a clinical study of 125I-labeled mAb A33 (3) that showed the in vivo stability of the iodinated antibody.
Uniformity of antigen expression is a necessary but not sufficient condition to ensure the uniformity of the distribution of radiolabeled antibody. However, it is suggestive that radioimmunotherapy using radionuclides with shorter ranges than 131I may have a potential role. The existence of a relatively uniform antibody distribution in human tumor xenografts grown in nude mice between 4 h and 4 d after administration of 50–200 μg humanized A33 has been reported (4). Because internalization of the antibody–antigen complex does not lead to rapid deiodination, 125I may be a rational choice for therapeutic radionuclide.
The decay of 125I by electron capture results in the emission of a large number of low-energy Auger electrons, most of which possess ranges of <2 nm in tissue. These short-range electrons and the charge buildup on the daughter tellurium atom are responsible for the high linear energy transfer (LET)-type damage produced by 125I decays, when incorporated directly into the DNA of target cells (5–7). 125I decays that occur within the cell but not in intimate contact with DNA produce low LET-like damage—that is, cell survival curves are shouldered resembling those produced by x-ray irradiation (7,8). The K-shell Auger and internal conversion electrons possess ranges up to 17 μm (8,9), and the L-shell electrons have a range of approximately 1 μm. These longer range emissions do not yield high LET-type damage; however, they do reach the nuclear DNA from the cell surface. Nevertheless, intracellular accumulation of 125I will yield substantially greater dose to the cell nucleus (by a factor of 2–3) (2) than cell-surface accumulation. In addition, the relative importance of cross dose (i.e., from decays outside the cell of interest) is significantly less for 125I than for 131I. In the case of 125I, this is the result of its longer range emissions, whereas for 131I, decays within several millimeters (a vastly larger volume) may contribute to the cross dose.
The therapeutic effects of 131I- and 125I-A33 have been studied in phase I/II clinical trials for advanced colon cancer (3,10). The maximum tolerated activity for 131I-A33 was 2.78 GBq/m2 (75 mCi/m2) in heavily pretreated patients, similar to other studies with 131I-labeled murine monoclonal antibodies. For 125I-A33, bone marrow toxicity was not seen after administered activities as high as 12.95 GBq/m2 (350 mCi/m2).
In this study, the biologic efficacy and toxicity of 125I-A33 were compared with 131I-A33 in an SW1222 colon cancer xenograft model grown in nude mice.
MATERIALS AND METHODS
Cell Line
The human colon carcinoma cell line SW1222 was maintained in Eagle’s medium as described (11). The cells were kept in a 37°C atmosphere (5% CO2) and harvested using 0.1% trypsin and 0.02% ethylenediaminetetraacetic acid (GIBCO, Grand Island, NY).
Human Tumor Xenografts
Four- to 6-wk-old athymic female Swiss (nu/nu) mice (body weight, 20–25 g) from our in-house nude mouse facility were injected with 10 × 106 SW1222 cells in the left thigh muscle. After 5–7 d, mice bearing tumors of 140–900 mg were selected. The radiolabeled mAb A33 or an IgG2a control antibody was injected intravenously in the retroorbital plexus after the mice were anesthetized with Avertin, which was made fresh from 2,2,2-tribromoethanol (Pfaltz and Bauer, Inc., Waterbury, CT) in a solution of 3-methyl-1-butanol (Sigma Chemical Co., St. Louis, MO) as described (11).
Labeling of mAbs
Iodination of mAb was performed by the chloramine-T method (11). In brief, 125I or 131I was added to mAb solution in the presence of 200 μL chloramine-T (2.0 mg/mL) for 1 min. The reaction was quenched with 200 μL sodium metabisulfite (10 mg/mL). Labeled antibody was separated from free iodine using a NAP 25 column (Pharmacia Biotech, Piscataway, NJ).
Specific activities for 125I-labeled antibodies ranged from 640 to 925 MBq/mg (17–25 mCi/mg) for A33 (mean, 780 MBq/mg [21 mCi/mg]) and from 925 to 1,225 MBq/mg (25–33 mCi/mg) for the IgG2a control (mean, 850 MBq/mg [23 mCi/mg]). For 131I-labeled antibodies, the specific activities were between 830 and 1,110 MBq/mg (22–30 mCi/mg) for A33 (mean, 930 MBq/mg [25 mCi/mg]) and from 355 to 440 MBq/mg (9.6–12 mCi/mg) for the IgG2a control (mean, 395 MBq/mg [11 mCi/mg]).
The immunoreactivity of radiolabeled antibody was tested on antigen-positive cell pellets as described (1). Immunoreactivities ranged from 29% to 40% for 125I-A33 (mean, 34%) and from 36% to 55% (mean, 47%) for 131I-A33.
Tumor Therapy and Control Studies
A total of 169 mice were divided into groups of 4–9 mice. Fourteen groups were administered varying amounts of mAb A33 labeled with either 125I or 131I. The activities of 125I-A33 ranged from 9.25 to 148 MBq (0.25–4 mCi), with antibody masses from 10 to 230 μg. For 131I-A33, activities ranged from 0.925 to 18.5 MBq (0.025–0.5 mCi), with antibody masses from 3.3 to 24 μg. Eleven groups received varying amounts of a mouse myeloma protein IgG2a, kappa UPC 10 (Sigma Chemical), nonspecific control mAb labeled with either 125I or 131I. Activities ranged from 27.7 to 92.5 MBq (0.75–2.5 mCi) for 125I and from 0.925 to 41.8 MBq (0.025–0.4 mCi) for 131I. One group was administered 250 μg unlabeled mAb A33, and 5 groups served as growth controls. Tumor size was measured bidimensionally with calipers, and the volume was calculated assuming elliptic geometry.
Initial tumor sizes were between 0.14 and 0.90 cm3 (mean, 0.44 cm3). Mice with tumors of differing sizes were divided into each group such that the tumor size spectrum for each group was similar. In earlier localization experiments, antibody uptake did not appear to be affected by tumor size (data not shown). The tumors were measured every 3 or 4 d for 100 d or until the death of the animal. Mice were killed when the tumor caused apparent discomfort in walking or when its volume exceeded 2 cm3.
RESULTS
Tumor Growth Delay
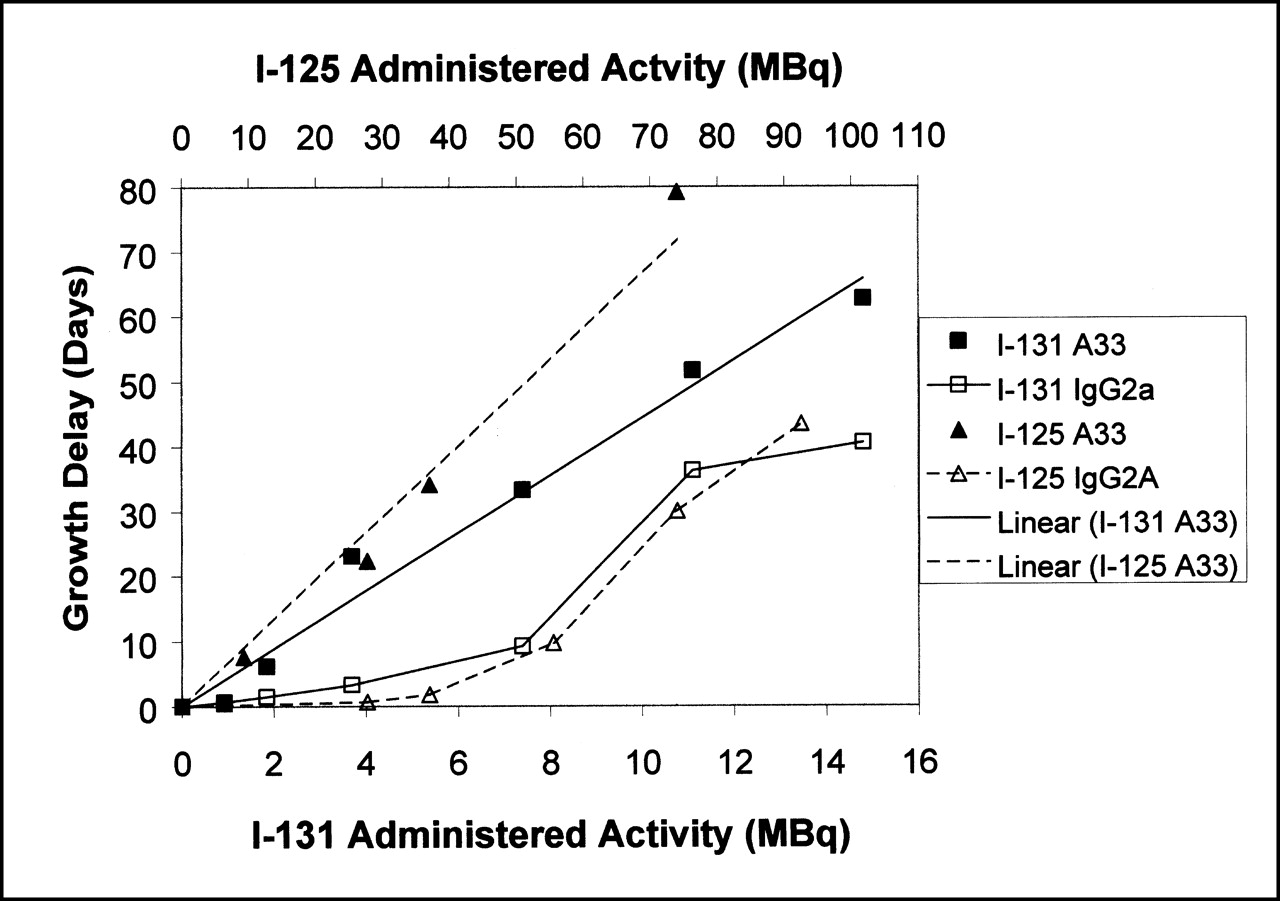
The full set of tumor growth curves for each animal in the different treatment groups indicated a clear relationship between administered activity and response, although significant variability was seen within each group. The results are expressed in terms of the behavior of the median tumor volume, normalized to initial volume, as a function of time (Figs. 1A–1D). Figure 1 indicates that tumor growth was retarded after treatment to an extent that was dependent on the amount of activity administered. On the basis of these curves, we calculated the times required for the median tumor volume in each group to grow to 2.5 times its initial size. The tumor growth delay was defined as the difference between these times for the treatment groups and that for the control (untreated) group. Figure 2 shows tumor growth delay as a function of administered activity for the radiolabeled specific and nonspecific antibodies, which indicates the existence of a dose–response relationship for all radiolabeled antibodies (note the different activity scales for 125I- and 131I-labeled species). The difference in effectiveness of radiolabeled specific and nonspecific antibodies is clearly evident.
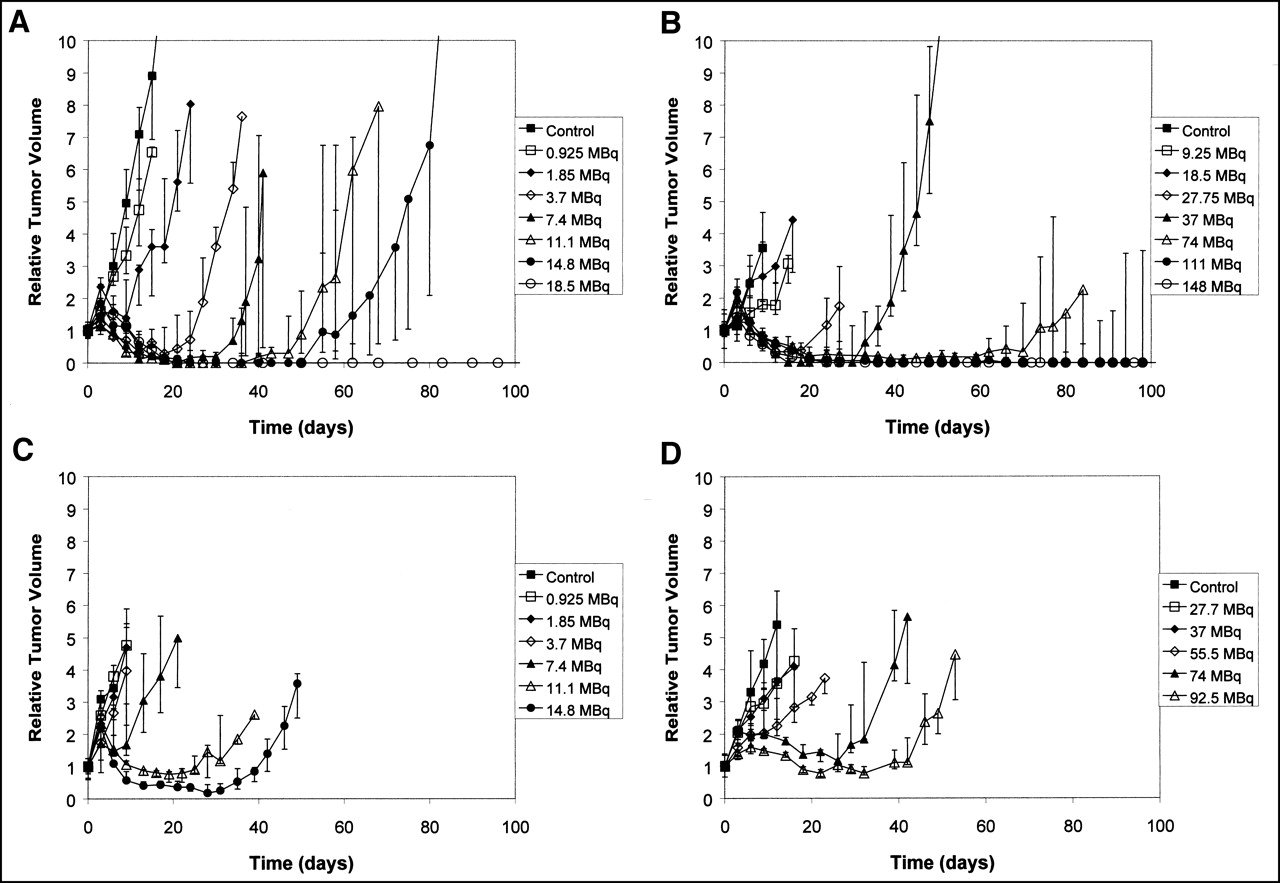
Median tumor volume, normalized to initial volume, as function of time in nude mice bearing SW1222 xenografts when treated with 131I-A33 (A), 125I-A33 (B), 131I-IgG2a (C), and 125I-IgG2a (D). Error bars correspond to 25 and 75 percentiles of each treatment group.

Tumor growth delay (d) with increasing activities of radiolabeled A33 and IgG2a. A33 data were fitted by linear regression yielding slopes of 0.97 d/MBq and 4.4 d/MBq for 125I and 131I, respectively.
Linear regression analysis was used to estimate the average slopes of the growth delay curves versus activity curves for the specific antibodies. For 125I-A33 the slope was 0.97 d/MBq, whereas for 131I-A33 it was 4.4 d/MBq. We conclude that 131I-A33 was around 4.5 times more effective than 125I-A33 in terms of administered activity for the endpoint of tumor growth delay. For the nonspecific antibodies, the relative effectiveness was estimated by adjusting the scales of the activity axes until the response curves became coincident. As seen in Figure 2, 131I-IgG2a was approximately 7 times more effective than 125I-IgG2a on the basis of administered activity.
No apparent therapeutic effect was evident in the group treated with 250 μg unlabeled mAb A33 compared with the growth control group (data not shown), as reported (12).
Tumor Cure
Tumors were considered cured if they failed to regrow over the period of observation (100 d after treatment). Radioimmunotherapy with 125I-A33 yielded a relationship between tumor cure probability and administered activity that was approximately linear (Fig. 3). For 131I-A33, the relationship was less predictable. Occasional tumor cures were seen at intermediate administered activities of 131I-A33 (3.7–11.1 MBq), but a higher value (14.8 MBq) did not produce any cures. Four of 5 tumors in this group became temporarily undetectable but subsequently recurred between day 40 and day 80. The highest activity of 131I administered (18.5 MBq) resulted in tumor cures in all 4 animals in that group (Fig. 3).

Tumor cure probability vs. administered activity for 131I-A33 and 125I-A33.
Neither 125I- nor 131I-labeled control IgG2a antibodies produced any tumor cures with the exception of 1 cure of 5 animals that were given 131I-IgG2a at the highest activity (14.8 MBq) (data not shown).
Toxicity of Radiolabeled mAbs on Mice
Before initiating the dose–response study, we performed a preliminary experiment to examine the toxicity induced by radiolabeled antibodies in tumor-bearing mice and to estimate the maximum tolerated activities for the different radiolabeled species. The results of this study are summarized in Tables 1 and 2. Briefly, we found that the maximum tolerated activities of 125I- and 131I-A33 were 185 MBq (5.0 mCi) and 18.5 MBq (0.5 mCi), respectively, in this model system. Activities of >185 MBq 125I-A33 and >18.5 MBq 131I-A33 caused petechiae, which became apparent after 2 d and confluent after 4 d, as well as progressive weight loss. All of these animals died within a relatively short time, during which no tumor responses were seen. No gastrointestinal toxicity was noted. Therefore, we estimated the ratio of 131I- to 125I-A33 activities for equivalent toxicity to be approximately 10.
Toxicity in SW1222-Bearing Mice with A33 Tumor-Specific Antibody
Toxicity in SW1222-Bearing Mice with Nonspecific Antibody
Forms of toxicity that were similar to those produced by radiolabeled A33 were seen with 125I- and 131I-labeled control IgG2a. Animals that received ≥111 MBq (3 mCi) 125I-IgG2a survived for 10–14 d. Three of 5 mice that received 18.5 MBq (0.5 mCi) 131I-IgG2a died within 16 d (mean, 25 d) with similar symptoms. Therefore, for this nonspecific antibody, we estimate the ratio of activities for equal toxicity to be approximately 6.
No major toxicity was seen after treatment with antibodies labeled with either radionuclide at the levels used in the dose–response experiments.
DISCUSSION
These results indicate that the relative efficacy of 125I versus 131I is dependent on the molecule to which the radioiodine is bound and also on the biologic effect under investigation. When associated with the A33 antibody, 125I was approximately 4.5 times less effective than 131I for the endpoint of SW1222 regrowth delay in terms of administered activity. When bound to nonspecific IgG2a antibody, the relative efficacy was around a factor of 7 for the same endpoint.
Previous studies using A33 trace-labeled with 125I on the same xenograft system as we used suggested that the average absorbed dose to tumor was approximately 0.5 Gy/MBq and, by inference, the average absorbed dose to tumor from 131I was estimated to be 3.7 Gy/MBq (11). The ratio of these values is approximately 7, whereas the ratio of activity for equivalent tumor effect was approximately 4.5. This finding implies that 125I-A33 was more therapeutically effective than 131I-A33 on the basis of average absorbed dose. When labeled to the nonspecific IgG2a antibody, the 7-fold difference in activity for equivalent therapeutic efficacy is compatible with the difference in absorbed dose for similar tumor uptake and clearance. 131I-A33 was found to be approximately 10 times more toxic than 125I-A33 on the basis of administered activity. In contrast, for the nonspecific IgG2a, the 131I-labeled antibody was approximately 6 times more toxic on the basis of administered activity.
A possible interpretation of these findings is that there is a geometric enhancement of absorbed dose to the nuclei of cells that have internalized 125I-A33, which causes its biologic effectiveness to be greater than expected for extracellular or surface-bound activity. Although 125I decays in the cytoplasm will not result in a greater radiobiologic effectiveness per unit dose, the average dose per decay to the nucleus of an antigen-positive cell will be higher than that to an antigen-negative cell. The radiation dose from a radionuclide source decreases with distance according to the inverse square law and as a result of electron attenuation. Additionally, because antigen-positive tumors will accumulate radionuclide to a greater extent than antigen-negative cells, the dose enhancement will be significantly greater than from geometric factors alone. For 125I, the electron emission ranges are so short that the self-dose contribution can exceed that from electron cross fire and small changes in the subcellular distribution can have a significant impact on the effectiveness of the radiopharmaceutical (13). The geometric enhancement for 131I-A33 is insignificant because the self-dose to the targeted cell is small relative to the cross-dose contribution from the longer range β-emissions. S factors have been calculated for the dose to the nucleus from 125I decays distributed uniformly in the cytoplasm and on the cell membrane, but not specifically for distributions within extracellular space (13). For example, for a cell of 10 μm with a nuclear diameter of 6 μm, the calculated S factors are 6.12E-04 and 2.34E-04 Gy/Bq·s, respectively, a ratio of 2.6. For 131I, the corresponding values are 4.57E-04 and 2.63E-04 Gy/Bq·s, a ratio of 1.75. This indicates that the proximity of the decay to the cell nucleus is a more significant determinant of cellular self-dose for 125I than it is for 131I. In the case of 125I-IgG2a, internalization does not occur and the geometric enhancement is absent. The ratio of activities of nonspecific antibody for equivalent effects on tumor growth is given simply by the ratio of absorbed dose per unit administered activity.
The dose-limiting toxicities for these radiolabeled antibodies were hematologic. Differences in relative toxicity between radiolabeled antibodies are caused primarily by the higher tolerance of the animals to 125I-A33. If a significant proportion of the A33 antibody is in the tumor, there will be less present in the circulation and also reduced cross-fire irradiation of distant normal tissues by the short-range electrons emitted by 125I. The blood clearance has been reported to be significantly different between A33 and IgG2a (4). In the first 24 h, blood levels fell from 36 to 9.5 percentage injected dose per milliliter (%ID/mL) for 125I-A33 and from 38 to 16 %ID/mL for 125I-IgG2a. For 131I-A33 in a mouse model, the reduction in normal tissue irradiation will be less significant because of the longer range of its β-emissions and penetrating γ-photon. For the nonspecific IgG2a, a reduced amount of antibody is bound to tumor and more is present in the circulation. The 6 times higher effectiveness of 131I in this context again simply reflects the differences in absorbed dose per unit administered activity.
The effects of internalizing mAbs labeled with either 125I or 131I have been studied by several other groups. Woo et al. (14) observed a dose-dependent induction of chromosome aberrations in colon cancer cells targeted by the internalizing mAb 17-1A labeled with 125I. These effects were not seen with noninternalizing 125I-labeled control antibodies. Bender et al. (15) found that the internalizing mAb 425 labeled with 125I was more toxic to glioma cells in vitro and xenografts in vivo than the 131I-labeled species. Behr et al. (16) reported superior therapeutic results in a xenograft system with 125I-labeled mAb CO17-A than with 131I-CO17-A. In this study, human colon cancer xenografts in nude mice were treated at the maximally tolerated dose. Our data are broadly in agreement with these previous studies.
Although not investigated here, the relative therapeutic efficacy of 125I- and 131I-labeled antibodies will depend on the intratumoral distribution of the targeting agent. In tumors of significant size, the delivery of radionuclides by molecular vectors may be impeded by difficulties in tissue penetration (17). For 125I-labeled antibody therapies to be effective, the antibody must localize on all tumor cells. Immunohistochemical studies have shown that the A33 antigen is expressed uniformly in most colorectal cancers (1) and that the A33 antibody reaches a uniform distribution within SW1222 tumors by 24 h (18). In the experiments we performed, the A33 antibody localized with sufficient uniformity to cure tumors in mice at administered activities of 125I ≥74 MBq.
CONCLUSION
The therapeutic efficacy of 125I-A33 was compared with that of 131I-A33 in a human colon carcinoma xenograft model. Approximately 4.5 times higher activities of 125I were required for an equivalent tumor growth delay relative to that of 131I. The relative toxicity to mice injected with mAb A33 labeled with 131I or 125I was around 10:1 in terms of administered activity. On this basis, the relative therapeutic gain is a factor of approximately 2. In contrast, little difference was found between the activity ratios for equivalent biologic effects using nonspecific, noninternalizing control antibodies labeled with either 125I or 131I.
Acknowledgments
This study was supported in part by National Institutes of Health grant CA 33049.
Footnotes
Received Oct. 20, 2000; revision accepted Apr. 9, 2001.
For correspondence or reprints contact: Els C. Barendswaard, MD, Department of Pathology, New York University School of Medicine, 550 First Ave., New York, NY 10016.
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Curative Multicycle Radioimmunotherapy Monitored by Quantitative SPECT/CT-Based Theranostics, Using Bispecific Antibody Pretargeting Strategy in Colorectal Cancer
- Noninternalizing Monoclonal Antibodies Are Suitable Candidates for 125I Radioimmunotherapy of Small-Volume Peritoneal Carcinomatosis
- Preliminary Report of a Phase I Study of Combination Chemotherapy and Humanized A33 Antibody Immunotherapy in Patients with Advanced Colorectal Cancer
- Phase I Study of Anticolon Cancer Humanized Antibody A33