


Abstract
Previous study of the bleomycin-induced lung injury model suggested that 111In-labeled antirat intercellular adhesion molecule-1 (aICAM-1) might be a useful acute respiratory distress syndrome (ARDS) diagnostic agent. We further investigated the ability of 111In-aICAM-1 to detect inflammation in another ARDS lung injury model. Methods: 111In-labeled rat polymorphonuclear leukocytes (PMNs), 111In-aICAM-1, 111In-labeled normal mouse IgG (nmIgG), and 111In-labeled rat serum albumin (RSA) were injected into rats 18–24 h before kill. Biodistributions, scintigraphic images, and lung ICAM-1 upregulation were obtained in uninjured rats and in rats after injury with oleic acid. Results: 111In-RSA and 111In-nmIgG localized in inflamed lung at 5 min postinjury (PI). 111In-PMN uptake increased significantly only at 24 h PI. 111In-aICAM-1 localization increased significantly (30%–60%) at 1 h PI and remained elevated up to 24 h PI. Lung/blood ratios (L/B) at 1 and 4 h PI were very low (<0.6) for 111In-nmIgG and 111In-PMN rats; however, for 111In-aICAM-1 rats, they were >1 and 25%–60% higher than those for the control samples. A low L/B suggests poor inflammation detection on the images. Images and region-of-interest analysis confirmed that only 111In-aICAM-1 could distinguish inflamed lungs at 4 h PI. ICAM-1 was upregulated at 4 and 24 h PI. Conclusion: In this model, 111In-aICAM-1 detected lung inflammation very early in the course of the disease. These results support the suggestion that 111In-aICAM-1 could be a very early, highly specific ARDS diagnostic agent and may be useful to detect a wide range of inflammations.
- inflammation
- acute respiratory distress syndrome
- adhesion molecules
- inflammation imaging
- immunoscintigraphy
Acute respiratory distress syndrome (ARDS) represents a group of diseases that have the common pathologic manifestation of acute diffuse lung injury. Its estimated incidence ranges from 8 to 75 people per 100,000, and it is associated with a mortality rate of 36%–60% (1–3). In many instances, multi-organ system failure follows the acute lung injury phase and is typically the primary cause of death. The most common cause of ARDS, accounting for 37%–45% of all cases, is gram-negative sepsis (2–4). Also, fat emboli from major bone fractures in some patients (approximately 25%) can cause direct pulmonary injury that leads to ARDS (3). The syndrome typically arises 24–72 h after the inciting incident (5). This period provides an opportunity to identify those patients in whom ARDS may develop, and it also provides time to begin prophylactic therapy. No specific therapy has been found to be beneficial; instead, the patient is managed in terms of respiratory, circulatory, and nutritional support (2,6). Recently, several new treatments, including inhaled nitrous oxide (7), instilled surfactant (8), and interleukin-1 receptor antagonist (9) have been attempted with ARDS and related disorders, but they have achieved little improvement in patient survival.
The mechanisms involved in the pathogenesis of ARDS are undoubtedly numerous, complex, and poorly understood (2). Various cells and mediators have been implicated (10–13). It is very difficult to establish whether a cell type or mediator precedes injury, causes injury, or is a secondary manifestation of that injury. Certainly, polymorphonuclear leukocytes (PMNs) have been shown to be present in high numbers in the lungs of patients with ARDS (14,15) and in animal models of ARDS (16,17) and have thus been implicated in the pathogenesis of the disease. Complicating the role of PMNs in ARDS is the observation that ARDS develops in neutropenic patients (18). Nevertheless, many studies of patients and animal models either directly or indirectly implicate PMNs (or their products) in the pathogenesis of ARDS. Investigators have been looking for clinical predictors of ARDS and have considered various mediators and cells without much success (19–22).
A hallmark of an acute infection/inflammation is the invasion of the site by large numbers of PMNs. A critical component of this directed movement is the ability of the PMNs to marginate in the blood vessels near the inflammation. An essential margination component is the expression of adhesion molecules, namely, intercellular adhesion molecule-1 (ICAM-1) on endothelial cells and its counter-receptor, leukocyte function antigen-1 (LFA-1), on the neutrophil surface (23,24). The interaction of LFA-1 and ICAM-1 allows the PMNs to become firmly attached to the endothelial cell. LFA-1 is expressed at low basal levels but is upregulated by a variety of proinflammatory agents. ICAM-1 is expressed constitutively and is also upregulated by various proinflammatory agents. The upregulation of ICAM-1 is usually long lasting with a maximum at 8–10 h and remains elevated for 2–7 d. This finding suggests that an antibody to ICAM-1 has the potential to be an early and specific inflammation detection agent, because ICAM-1 upregulation precedes PMN localization and remains elevated.
99mTc- and 111In-labeled white blood cells (WBCs) are commonly used for acute inflammation detection and could be useful to identify patients in whom ARDS may develop. However, these agents are not without limitations (25,26). The preparation of each agent is very labor intensive (2–3 h) and requires specialized equipment. In addition, most community hospitals lack the expertise for such preparation and send the autologous blood to a commercial radiopharmacy for labeling, which adds an additional 1–2 h. Although imaging with 99mTc-WBCs can be performed within 1–4 h after injection, the rapid excretion of 99mTc into the bowel and the particularly transient uptake in the lung complicate inflammation detection in these areas. Thus, many laboratory and clinical studies are looking for a suitable replacement (26–28). Most of the agents being studied are targeted against antigens present on PMNs and thus dependent on an increased concentration of PMNs at the inflammatory site (26). We propose that 111In-labeled mouse monoclonal antihuman ICAM-1 antibody (hum-aICAM-1) may be able to detect events in this disease even earlier than other agents because ICAM-1 upregulation precedes PMN localization. Thus, 111In-hum-aICAM-1 could provide a highly specific, less expensive, and earlier means of inflammation detection. We showed previously in bleomycin-induced lung injury that the inflammation can be detected as early as 4 h after initiation (29).
In this study, we investigated the ability of 111In-labeled mouse antirat ICAM-1 antibody (aICAM-1) to detect inflamed lung in the oleic acid (OA) model of fat emboli–induced lung injury. This agent was compared with 111In-PMNs, which are the current standard agent, and 111In-labeled rat serum albumin (RSA) and 111In-labeled normal mouse polyclonal IgG (nmIgG), two markers of endothelial integrity.
MATERIALS AND METHODS
OA Model of Lung Injury
CDF:(F344)ClrlBR Fischer rats (Charles River Laboratories, Worthington, MA) were anesthetized, and each animal was injected intravenously with 300 μL of a suspension of OA (Sigma Chemical Co., St. Louis, MO). The suspension comprised 30 μL pure OA suspended in 270 μL 0.1% bovine serum albumin (30). Sham-injury (uninjured) animals received an injection of an equal volume of saline.
Preparation of 111In-Labeled Proteins
The coupling of cyclic anhydride diethylenetriaminepentaacetic acid (DTPA) to aICAM-1 (Seikagaku Corp., Tokyo, Japan), nmIgG (Sigma Chemical Co., St. Louis, MO), or RSA (Sigma Chemical Co., St. Louis, MO) and the addition of 111In (NEN Life Science Products, Boston, MA) to the protein-DTPA complex were performed as described previously (31). Each protein was conjugated with 0.8–1.3 DTPA/molecule, and DTPA conjugation had no significant effect on immunoreactivity.
Preparation of 111In-PMNs
PMNs were harvested by lavage of the peritoneal cavity of normal rats with 60 mL heparinized saline (2 U/mL) 16 h after the intraperitoneal injection of 0.1% glycogen (20 mL in saline) (32). This method consistently yielded >1 × 108 PMNs per animal with a purity >95%. 111In-oxine, approximately 18.5 MBq/106 cells, was added to the cell suspension and incubated for 20 min at room temperature, and labeled cells were separated by centrifugation. Labeling efficiency averaged 70%–80%, and cell viability was always >85% as tested by the eosin-dye exclusion test.
Biodistribution of 111In Radiopharmaceuticals in OA Model of Lung Injury
Rats (3 per group) received an intravenous injection of 1 × 108 111In-PMNs containing 370 kBq at 18–24 h before their scheduled kill time. OA was injected at 15 min, 30 min, 1 h, 4 h, 24 h, and 72 h before kill. Also, rats (3 or 4 per group) were injected intravenously with 111–222 kBq radioactivity containing 10 μg 111In-nmIgG, 111In-RSA, or 111In-aICAM-1. For 111In-nmIgG and 111In-RSA, the radioactivity was injected at 18–24 h, and OA was injected at 5 min, 15 min, 30 min, 1 h, 4 h, 24 h, and 72 h (RSA only) before kill. The 5-min OA injection time was chosen because that is before detectable lung injury, and the 72-h OA injection time was chosen because that is when the lung injury begins to resolve spontaneously (30,33). For the 111In-aICAM-1 experiments, the antibody was injected at 24 h and OA was injected at 1, 4, and 24 h before kill. This injury and biodistribution protocol was used previously with bleomycin (Fig. 1) (27). In the uninjured rats, a sham injection with saline was performed concurrent with the 111In-labeled radiopharmaceutical injection. Generally, experiments were performed with 2 or 3 time points and a control group. The data were then combined using each control group as a reference, and a percentage for the control group was computed. At the time of the kill, whole organs and tissues were removed and weighed, and the radioactivity was measured (31). Data were computed as both percentage injected dose per gram of tissue (%ID/g) and percentage injected dose per organ (%ID/O).
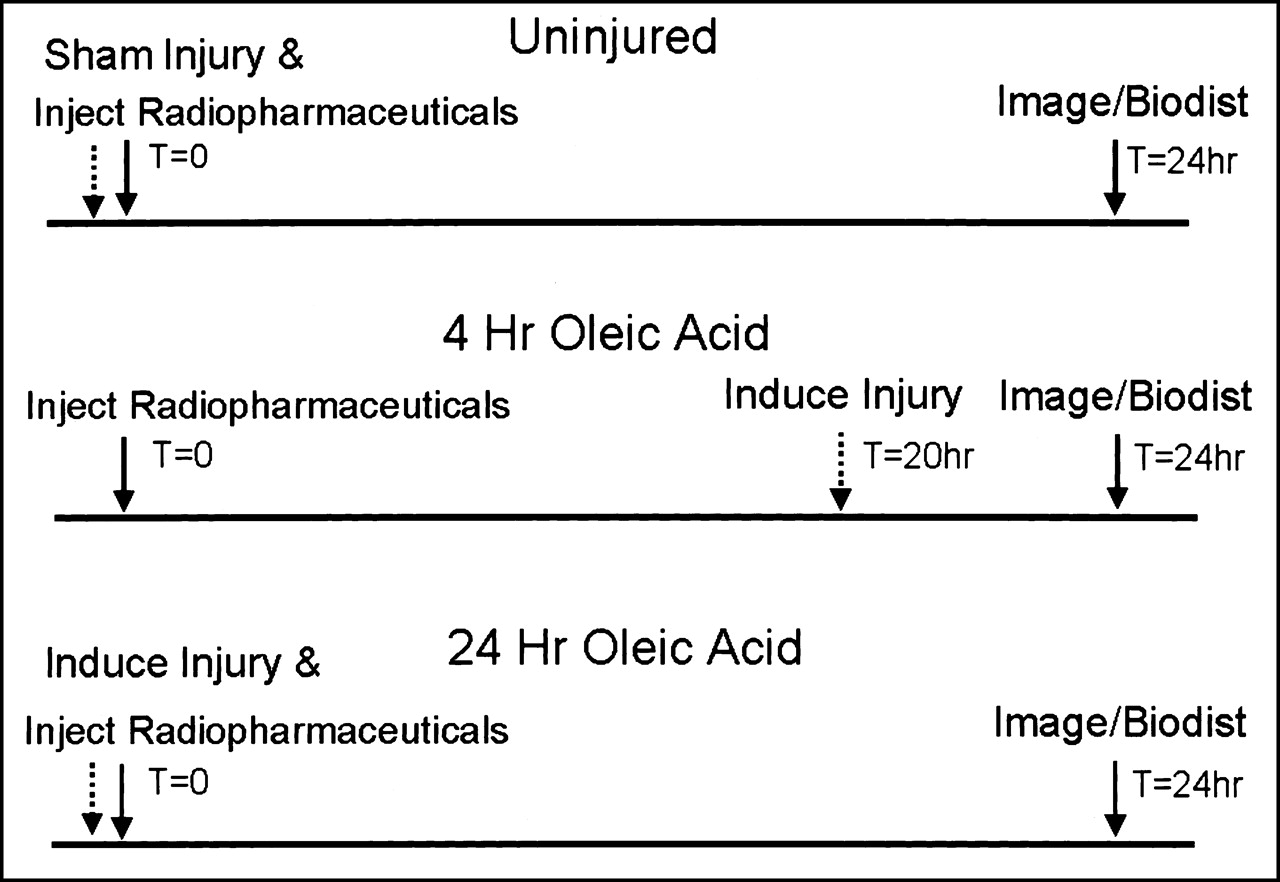
Experimental time line for injection of 111In-labeled radiopharmaceuticals (solid arrow), injury with OA or sham injury (dotted arrow), and imaging or biodistribution (solid arrow) of rats. Only 2 injury times, 4 and 24 h, are shown for clarity.
When the data were analyzed for each radiopharmaceutical, we observed a consistently larger injury-induced increase in the %ID/O values compared with %ID/g values in the lung. We hypothesized that in this acute lung injury model, the inflammatory process caused a rapid accretion of fluid in the lungs. Any fluid increase would reduce any increase in %ID/g compared with %ID/O for these labeled compounds. For each labeled molecule, approximately a doubling of lung weight occurred, which peaked at 30 min–1 h PI (P < 0.001, compared with the uninjured lung) and then declined. This waxing and waning followed the course of the injury in this model (30). In all subsequent data, only %ID/O was compared because of this injury-induced lung weight increase. These data also showed that fluid influx was extremely rapid after the initiation of injury.
Imaging
Rats were imaged in the supine position at 24 h after injection of approximately 1.85 MBq containing 10 μg of sterile filtered 111In-labeled proteins or 0.5 × 108 111In-PMNs, suspended in 0.5 mL saline (31). Briefly, anterior views of the upper torso using a pinhole collimator were obtained at 4 and 24 h PI as described above, and 100,000 counts were collected (Fig. 1). To obtain a quantitative estimate of organ and tissue localization, regions of interest (ROIs) were drawn around organs and tissue background. The counts per pixel from the ROIs were corrected for background and 111In decay and divided by the acquisition time and injected dose for normalization.
Immunofluorescence of Lung Tissue
Lungs from rats at 4 and 24 h PI were excised, frozen in liquid nitrogen, cryostat sectioned, and assayed for the presence of ICAM-1 immunofluorescence as described previously (29).
Statistical Analysis
A one-way ANOVA with the Newman–Keuls test was applied to compare the effect of time PI for the labeled radiopharmaceuticals and to compare the different radiopharmaceuticals at the same time (34).
RESULTS
Uptake of 111In-PMNs, 111In-aICAM-1, 111In-nmIgG, and 111In-RSA in OA-Injured Rats
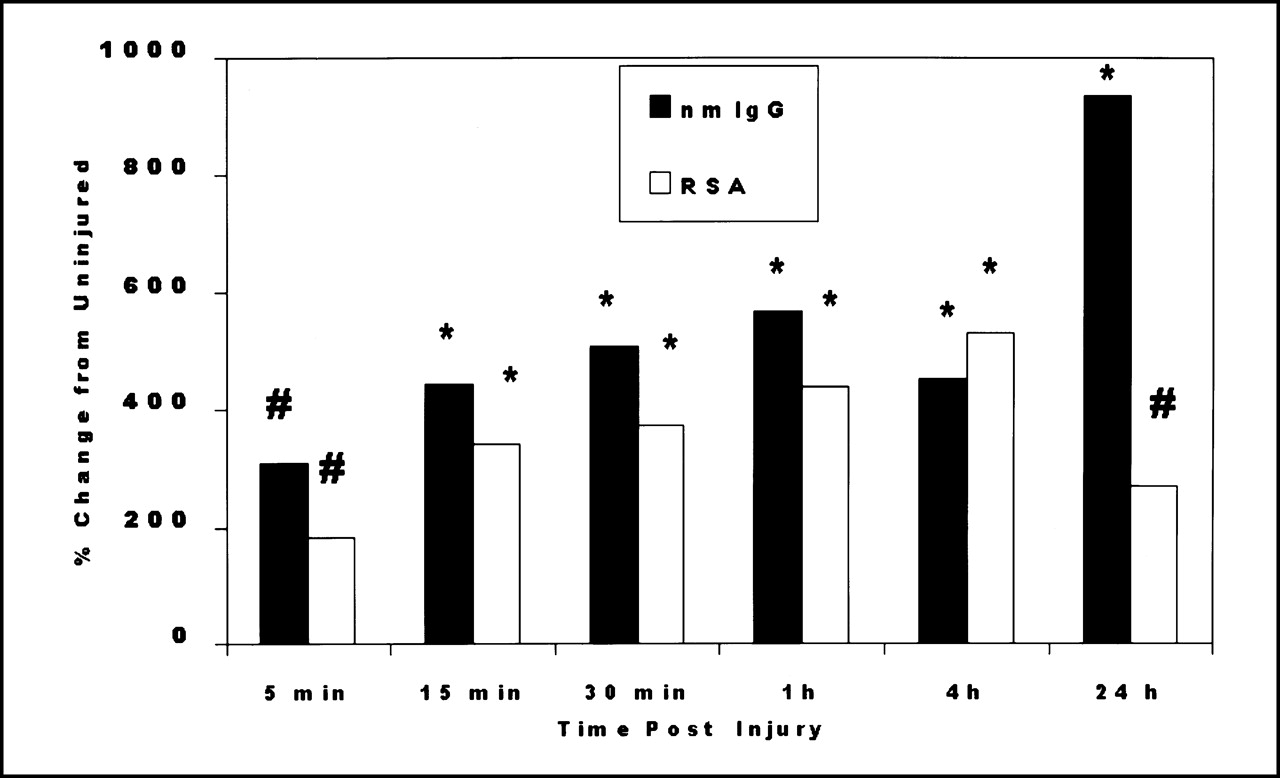
Figure 2 shows the uptake in injured lung for two labeled proteins, which are indicators of endothelial permeability. The uptakes of 111In-nmIgG and 111In-RSA in the lung increased dramatically two- to threefold at 5 min and were similar until 24 h (Fig. 2). Lung function measurements (33) and histology (30) indicate lung damage 15 min after injection of OA. At 24 h, 111In-RSA in the lung declined (P < 0.005, vs. 4 h). In contrast, 111In-nmIgG uptake doubled (P < 0.001, vs. 4 h). Injury did not cause the presence of 111In in other tissues to change except in the kidney (for 111In-nmIgG), which showed a modest but significant decline, and in the blood (for 111In-RSA), which was elevated modestly in activity as the injury progressed (data not shown). These data show that endothelial leakiness can be detected as early as 5 min PI in this model.

Effect of time after OA injury on lung uptake of 111In-RSA and 111In-nmIgG. Data are given as percentage change compared with uninjured lung using %ID/O values (#, P < 0.05; *, P < 0.001).
Although the endothelial barrier was disrupted, no significant increase in 111In-PMN lung uptake occurred until 24 h PI (Fig. 3). At that time, a dramatic, approximately 25-fold increase occurred, compared with the control uninjured lung. In contrast, at 1 h PI, rats injected with 111In-aICAM-1 had a modest but significant increase in lung activity, which increased at 24 h. No significant change in 111In-PMN uptake occurred in most other tissues after the lung injury initiation. The exception was in the spleen, where a significant, approximately 50% reduction occurred, compared with the uninjured value, only at 24 h (data not shown). This reduction would be consistent with recruitment of PMNs from the spleen to other tissues, particularly the lung, at 24 h. Also, kidney activity increased significantly at 4 h and remained elevated (26%–50%) (data not shown). For 111In-aICAM-1, the kidney was also the only tissue that showed a consistent significant increase in antibody accumulation as a function of injury (data not shown).

Effect of time after OA injury on lung uptake of 111In-PMNs and 111In-aICAM-1. Data are given as percentage change compared with uninjured lung using %ID/O values (#, P < 0.05; *, P < 0.001).
Lung-to-Tissue Ratios
The data from Figures 2 and 3 suggest that 111In-nmIgG would be an excellent early inflammation detection agent because of the high early uptake (5 min to 4 h); 111In-aICAM-1 and 111In-PMNs would be poor in comparison. However, this finding does not take into account that target detection is dependent on the ratio of the target (in this case, the lung) to the tissue background. To estimate the detection ability of each agent, a ratio was computed using different tissue backgrounds that could interfere with the detection of lung inflammation (Fig. 4). Thus, target detection is based on the increase of the ratio from the uninjured value. Animals injected with 111In-PMNs showed only at 24 h a significantly high lung-to-blood ratio (L/B), which is consistent with the results shown in Figure 3. This high L/B was mainly a result of low blood activity (approximately 1 %ID/O) and suggests that inflammation detection by imaging would be likely only at 24 h PI.

Effect of time after OA injury on L/B (A) and L/H (B) for 111In-PMNs, 111In-aICAM-1, and 111In-nmIgG. Data were computed using %ID/O values (*, P < 0.001; +, 0.05 < P < 0.1; #, P < 0.05).
The 111In-aICAM-1 results, which showed a modest injury-induced increase in lung activity, showed a large increase (not quite significant) in L/B at 1 h PI (Fig. 4). More importantly, the early (1 and 4 h) L/B and lung-to-heart ratios (L/H) were >1; the L/B was sixfold (P < 0.001) and the L/H was twofold (P < 0.001) greater than the comparable 111In-nmIgG values. This result was caused primarily by very low blood and heart uptake, 5 and 0.2 %ID/O, respectively, at this time PI. Even at 24 h, the 111In-aICAM-1 L/B was still approximately threefold (P = not significant) greater than the 111In-nmIgG value. This finding suggests that the injured lung might be detected visually as early as 4 h PI with 111In-aICAM-1.
However, in the 111In-nmIgG-injected rats, although the ratios increased significantly very early in the injury progression (1 h) (Fig. 4), the L/B was very low, <0.2 (Fig. 4A). Although a large increase was seen at 1–4 h PI, the low L/B suggests that the high blood background (27 %ID/O) could obscure the injured lung. Thus, in this early time frame, 111In-aICAM-1 could be a better imaging agent compared with 111In-nmIgG. As injury progressed to 24 h, both ratios for 111In-nmIgG-injected rats doubled at 24 h PI (>4 h, P < 0.001) (Fig. 4). This result suggests that the injured lung might be detectable at this time, because the blood activity was reduced to 20 %ID/O.
Imaging of 111In-PMNs, 111In-aICAM-1, and 111In-nmIgG in OA-Injured Rats
The imaging of these radiopharmaceuticals generally followed what we observed in the tissue ratio data. Figure 5 shows the deposition of these compounds at 4 and 24 h PI with OA. In the upper-torso images of uninjured rats injected with 111In-PMNs, only the intense uptake in the liver can be detected. At 4 h PI, the lung uptake was no greater than the tissue background, but liver activity remained. As the injury progressed to 24 h, activity is clearly apparent and well defined in both lungs.
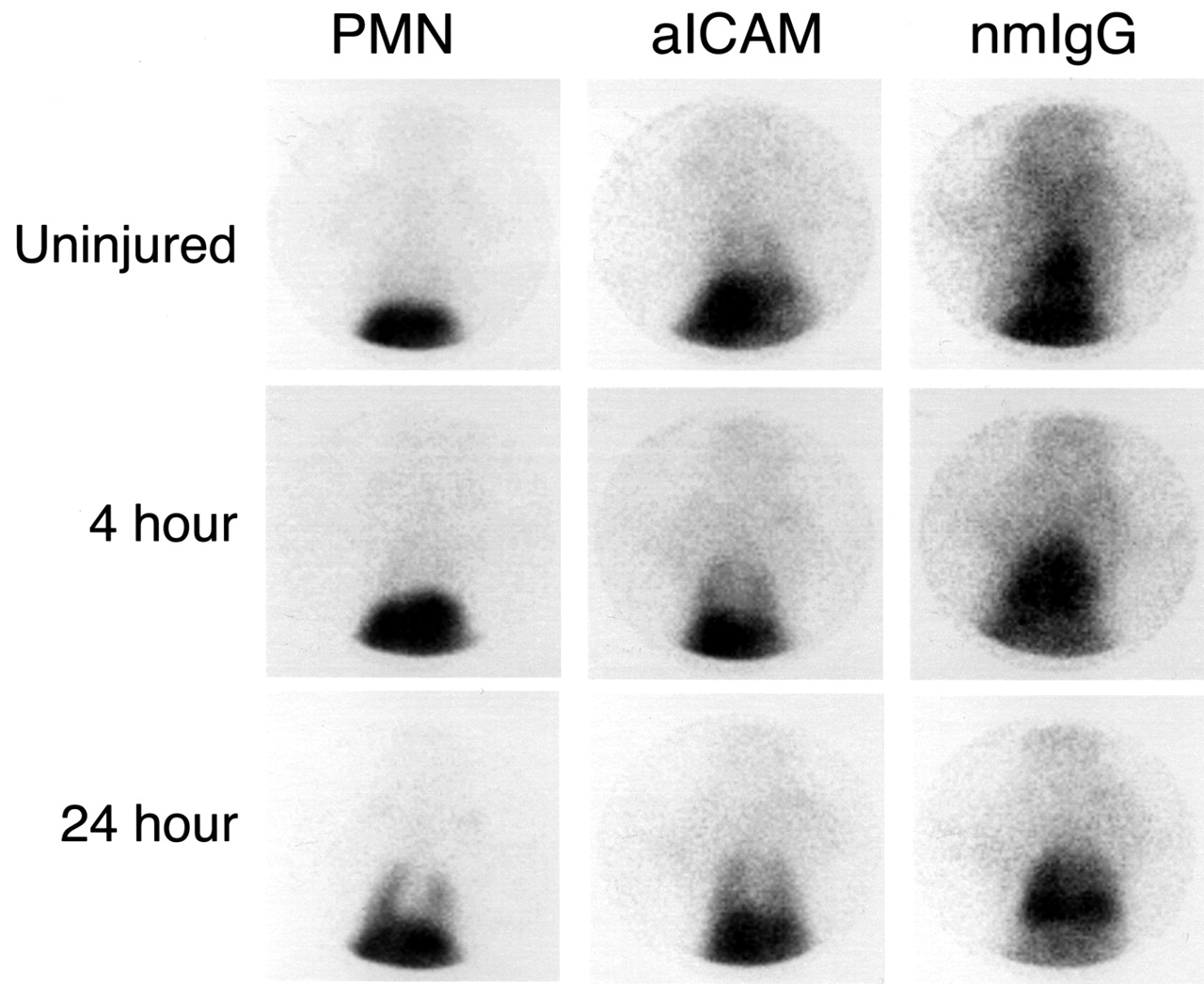
Pinhole scintigrams of upper anterior torso of uninjured rats and rats at 4 and 24 h after OA injury injected with 111In-PMNs, 111In-aICAM-1, or 111In-nmIgG. Animals were imaged at 24 h after injection with GE gamma camera (General Electric, Milwaukee, WI).
In the uninjured animals, 111In-aICAM-1 localized mainly in the liver, and some activity was seen in the lung fields. In contrast to the 111In-PMN images, the 4-h 111In-aICAM-1 images of the injured rat show that the lung fields are visible, defining the cardiac shadow (Fig. 5). Activity was also present in the liver. At 24 h, although no change in liver activity was seen, activity in the lung clearly defined the 2 lung lobes. The tissue background, although not as low as 111In-PMNs, is lower than that visible in the 111In-nmIgG images. Also, little activity is seen in the bone or bone marrow in any of the images. Thus, 111In-aICAM-1 can detect lung injury earlier than 111In-PMNs, which was suggested by the tissue ratios (Fig. 4).
The image of the 111In-nmIgG uninjured rat showed only cardiac blood and liver activity and very little lung activity. At 4 h PI, the image showed a high concentration of activity in the cardiac blood pool (Fig. 5). Although the lung fields were not well defined, the activity in the lungs appeared higher than the tissue background. Liver activity, although higher than background, is not nearly as intense as the cardiac blood pool. As injury progressed (24 h), the activity in the lung field intensified. The most intense areas appeared to be in the lung bases, and some activity was seen in the upper lobes. The cardiac blood at 24 h PI was not nearly as intense as at 4 h and can be distinguished from the lungs. Liver uptake was lower than the lungs and similar to the uptake in the 4-h image. These images are consistent with the predictions from the tissue ratio data.
To obtain quantitative information from the images, a ROI analysis was performed. Table 1 shows that for 111In-PMNs, a modest 40% increase in lung count density occurred at 4 h compared with the uninjured animals. In contrast, a 500%–600% significant enhancement occurred at 24 h. Lung activity was comparable with heart activity in the uninjured rat and at 4 h PI. However, at 24 h PI, the lung count density was double the heart activity when the lungs were clearly visible. In contrast, lung values from the 111In-aICAM-1-injected animals increased significantly (200%) at 4 h. More important, the lung count density was approximately 30% greater than the heart value at this time, and this relationship improved at 24 h (approximately 180% greater). Although lung cpm/pixel values in 111In-nmIgG rats were elevated significantly as early as 4 h, heart and liver values were comparable. This finding explains why it was difficult to detect the inflamed lungs.
Effect of OA-Induced Lung Injury on ROI Analysis of Rats Injected with 111In-Labeled Agents
Expression of ICAM-1 on Lung Tissue
Previous data showed that ICAM-1 was upregulated as early as 30 min PI (33). Figure 4 shows that ICAM-1 remains upregulated at 4 h (Fig. 6C) and 24 h (Fig. 6E) PI; the increased fluorescence intensity is apparent in the injured lung compared with lung tissue from uninjured rats (Fig. 6A). Control experiments with no added aICAM-1 showed no fluorescence intensity from either uninjured or injured lung tissue (Figs. 6B, 6D, and 6F).

Expression of ICAM-1 immunofluorescence in cryostat sections of OA-injured and uninjured rat lung. Sections were processed for immunofluorescence using aICAM-1 as first antibody in lung from uninjured rat (A), rat injured at 4 h (C), and 24 h before kill (E). For control samples, no aICAM-1 was used as first antibody in lung from uninjured rat (B), rat injured at 4 h (D), and 24 h before kill (F). Rhodamine-conjugated goat antimouse IgG was used as second antibody in all sections (magnification, ×788).
DISCUSSION
Our data suggest that 111In-aICAM-1 is a useful indicator of acute inflammation development in this model. Images showed that inflamed lungs could be detected very early (4 h PI) in the course of injury. The 24-h images were somewhat better. This result was consistent with biodistribution data, target-to-background ratios, and ROI analysis. Some data even suggested that 111In-aICAM-1 may detect injury as early as 1 h PI. Although 111In-nmIgG localized extremely early (within 5 min) in injured tissue, it was difficult to detect the inflamed lung in the scintigraphic images because of high blood-pool activity in the heart. In contrast, 111In-PMNs, which are the currently used acute inflammation detection agent, could not detect inflamed lungs until the injury had progressed at least 24 h in this model.
Our data also show that 111In-aICAM-1 is highly specific. 111In-aICAM-1 localization was increased as early as 1 h PI and remained elevated at our latest data point (24 h). A previous study showed that ICAM-1 is upregulated at 30 min PI in this model (33). The immunofluorescence data presented in this study show that ICAM-1 remained upregulated as long as 24 h PI. If 111In-aICAM-1 localization was related solely to injury-induced endothelial barrier disruption, we would expect very early and high lung uptake. For example, both 111In-nmIgG and 111In-RSA uptake increased dramatically as early as 5 min PI and peaked at 1 h PI, and these values were 568% and 440% greater, respectively, than those for the uninjured lung (Fig. 2). However, the lung uptake of 111In-aICAM-1, even at 1 h, was rather modest (32% increase) (Fig. 3). Thus, the likely driving force for 111In-nmIgG and 111In-RSA lung uptake was the high blood concentration (approximately 20–27 %ID/O) combined with the endothelial barrier disruption. In contrast, the low blood concentration (4–5 %ID/O) of 111In-aICAM-1 most likely required an active process, namely, ICAM-1 upregulation, for localization. We showed the high specificity of this labeled antibody in another model of lung injury (29). However, in this model, the injury-induced endothelial barrier disruption preceded ICAM-1 upregulation.
We propose using 111In-hum-aICAM-1 in patients at risk for ARDS similarly as it was used in this study. In patients at a high risk for ARDS, there appears to be a 24–72 h period after the inciting incident during which ARDS may develop (5). The labeled antibody would be injected, and the patient would be imaged sequentially over the next 72 h. Our data suggest that although little human 111In-aICAM-1 would be circulating, lungs that became inflamed would be detected readily as early 4 h but at least within 24 h. Imaging up to 72 h might be possible, because beyond 4 h after injection, 111In-aICAM-1 disappears very slowly (31). Although no therapeutic intervention has been found to be effective, with this early-detection method, interventions could be started and tested in the earliest stages of the disease.
111In-hum-aICAM-1 has several advantages over the existing agents. The preparation is simple and requires only the addition of 111In. This choice would eliminate the preparation problem associated with both 111In- and 99mTc-labeled WBCs. Blood handling is unnecessary. If the animal data can be translated to humans, we would expect a low constant lung uptake and very low uptake in bone, bone marrow, and intestines. This situation would make inflammation detection in these areas much easier. Studies are in progress to attach 99mTc to aICAM-1, which could further improve this agent and make it useful to detect a wide array of inflammations (35). The half-life for 99mTc is consistent with the localization time frame for this antibody.
CONCLUSION
We have developed a labeled antibody that takes advantage of the role of adhesion molecules in the inflammatory process. This new radiopharmaceutical localizes rapidly with high specificity in two animal models of lung inflammation. This compound has the potential to rapidly diagnose ARDS and other inflammatory processes to allow early therapeutic interventions. Whether this potential will be realized must await patient trials.
Acknowledgments
This research was supported in part by faculty research grants from the University of Connecticut Health Center.
Footnotes
Received Oct. 12, 2000; revision accepted Mar. 8, 2001.
For correspondence or reprints contact: Ronald E. Weiner, PhD, Division of Nuclear Medicine, University of Connecticut Health Center, MC-2804, 263 Farmington Ave., Farmington, CT 06030.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}