


Abstract
In some patients with well-differentiated thyroid carcinoma, dosimetry is necessary to avoid toxicity from therapy and to guide prescription of the administered activity of radioiodine. Methods: The presentations and courses of 2 patients exemplify the points. In the second patient, the clues to the need for dosimetry were the large size of the tumor and high circulating levels of thyroxine in the absence of exogenous hormone. The other patient manifested hyperthyroidism from stimulation of the tumors by thyroid-stimulating immunoglobulin. Dosimetry was performed by published methods. Results: Dosimetry of radioactivity in the body and blood warned of increased irradiation per gigabecquerel of administered 131I. In each patient, the tumors sequestered a substantial amount of administered 131I and secreted 131I-labeled hormones that circulated for days. In 1 patient, the blood time–activity curve was complex, making a broad range of predictions for irradiation to blood and bone marrow. Still, dosimetry gave information that helped to avoid severe toxicity. At, respectively, 1.85 and 2.2 GBq 131I, initial treatments were relatively low. There was a modest escalation in subsequent administered activities. Leukopenia with neutropenia developed in each patient, and one had moderate thrombocytopenia and anemia, but toxicity appeared to be transient. Each patient had a marked increase in well-being and evidence of reduced tumor function and volume. Conclusion: Two patients with advanced, well-differentiated thyroid carcinoma illustrate the need for dosimetry to help prevent toxicity to normal tissues from therapeutic radioiodine. Conversion of radioiodide to circulating radiothyroxine by functioning carcinomas increases the absorbed radiation in normal tissues. Yet, dosimetric data acquired for 4 d or more may be insufficient for accurate calculations of absorbed radiation in blood. Guidelines suggested for avoiding toxicity are based on the circulating thyroxine concentrations, the presence of thyroid stimulators, the amount of radioactivity retained in the body at 48 h, and the general status of the patient.
- thyroid carcinoma
- hyperthyroidism
- radioiodine
- dosimetry
- bone marrow toxicity
- thyroid-stimulating immunoglobulin
For more than 50 y, radioiodine has been used to treat patients with well-differentiated thyroid carcinoma. After treatments, reductions in tumors have been frequent, and marked toxicity has been uncommon. Nevertheless, bone marrow suppression and radiation pneumonitis have developed consequent to irradiation of normal tissues from the administered 131I. Such untoward events are most likely in patients who have a substantial volume of tumor and avidly concentrate the radionuclide. Yet, these patients appear to have the most to gain from higher activities of administered 131I.
Almost 40 y ago, Benua et al. (1) used data and observations of patients to establish dosimetric guidelines to prevent serious toxicity from 131I therapy in patients with thyroid carcinoma. A few reports indicate that these guidelines have served well to prevent bone marrow suppression and radiation pneumonitis (2–4). However, the proposed dosimetry has been applied infrequently, probably because most patients have not had tumors large enough to raise the radiation of normal tissues to the threshold, even when large activities (e.g., 7.4–11.1 GBq [200–300 mCi]) of 131I were administered. Nevertheless, dosimetry may prove invaluable for the individual with advanced functioning carcinoma.
Reported here are 2 patients, each with bulky metastases that not only sequestered iodine but also secreted thyroxine, features that predict higher than usual radiation rates of normal tissues when 131I is administered. These patients illustrate the need to consider dosimetric principles. The treatments with 131I were prescribed taking into account the high functional capacity of the tumors, dosimetric guidelines, the extent of disease, and reasonable expectations from the treatments. Also shown is the concept that induction of hypothyroidism to bring out endogenous thyroid-stimulating hormone (TSH) for stimulation of residual cancer may be not only unnecessary but also undesirable when the cancer is functioning in the absence of TSH. The dosimetry indices of absorbed radiation by body and blood (as a surrogate for bone marrow) can be simplified, and estimates can be made by any nuclear medicine laboratory. Such estimates will help ensure safer yet effective therapy for some patients.
MATERIALS AND METHODS
The patients were instructed to ingest a low-iodine diet (5) for 1 wk before testing and until 1 d after therapy was administered. In anticipation of relatively high sequestration rates of 131I by the tumors, diagnostic activities of 18.5 and 37.0 MBq (0.5 and 1.0 mCi) were administered to patients 1 and 2, respectively. Dosimetry methods have been described before (2,6–8) and are reviewed here briefly. After swallowing the radioiodine, each patient was asked not to void for 2 h. At 2 h, the radioactivity in the patient was counted while the patient was sitting 2.5 m from a thyroid uptake probe, the field of which encompassed virtually the entire body. The geometric mean of the anterior and posterior counts, minus the background, was calculated to determine the total dose administered. At intervals, the patient voided and counting was repeated to determine the fraction of 131I retained in the body. The measurement at 48 h was of particular interest because the guidelines for safety are based on this value.
Blood samples were obtained at 2 and 4 h and then daily if possible; 1 mL was counted in a well counter. Absorbed doses were calculated following the MIRD schema (9). Cumulated activity in the blood was obtained by integrating the area under the time–activity curve, with the tail of the curve assigned the 8-d physical half-life of 131I (10,11). For the nonpenetrating radiation of 131I, an absorbed fraction of 1 was assumed. Computerized calculations (12) gave similar results. In the initial patient evaluations, blood samples were obtained for 4 or 5 d. The guidelines proposed for safety were ≤200 cGy to the blood and ≤4.4 GBq retained in the body at 48 h, or 3.0 GBq if diffuse lung metastases were present (1).
RESULTS
Patient 1
This woman was 79 y old in 1997 when hyperthyroidism developed and progressed to congestive heart failure and atrial fibrillation. Her left shoulder became painful and limited in motion. Her thyroid gland was enlarged but lay low in her neck. Imaging with 131I portrayed diffuse activity in the thyroid gland, focal activity in the upper mediastinum and left shoulder, and focal activity irregularly in the lungs. Treatment with propylthiouracil, digoxin, and diuretics relieved her dyspnea; anticoagulant therapy was also instituted. Multiple lung nodules were seen on a chest radiograph and CT scan. Fine-needle aspiration of a lung nodule produced thyroid follicular cells.
The patient was first seen at the University of Michigan Medical Center in October 1997. Her thyroid-stimulating immunoglobulin (TSI) was elevated at 6.2 as an index (normal value, ≤1.3 at Mayo Clinic Laboratory, Rochester, MN), giving the diagnosis of Graves’ disease in addition to metastatic thyroid carcinoma. A total thyroidectomy was performed in late November with the goals of reducing the excess secretion of thyroid hormone and of enabling better imaging and treatment of the metastases. Histology revealed extensive replacement of the gland with well-differentiated papillary carcinoma containing a few areas of poorly differentiated cells; the tumor invaded the surrounding skeletal muscle.
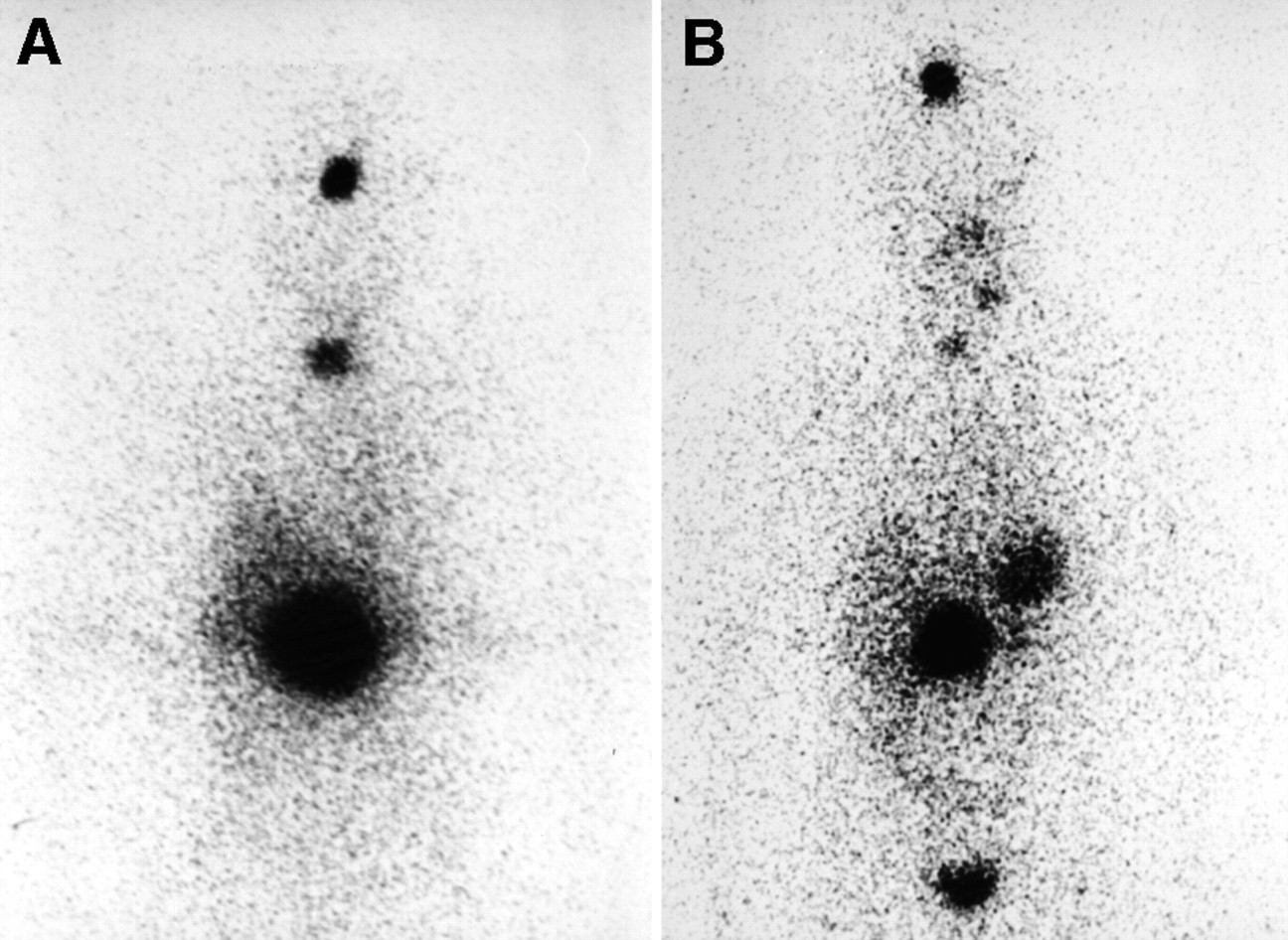
Propylthiouracil was not resumed after surgery, and hyperthyroidism and heart failure again developed (Table 1A). In January 1998, scintigraphic images depicted irregular but generalized and intense 131I concentrations in the lung fields and foci of activity in multiple bony sites (Fig. 1A). The chest radiograph (Fig. 2A) showed multiple nodules that were possibly larger than a few months before, and destruction by the tumor was evident in the left shoulder; heart failure was also obvious. The serum thyroglobulin level was >30,000 ng/mL
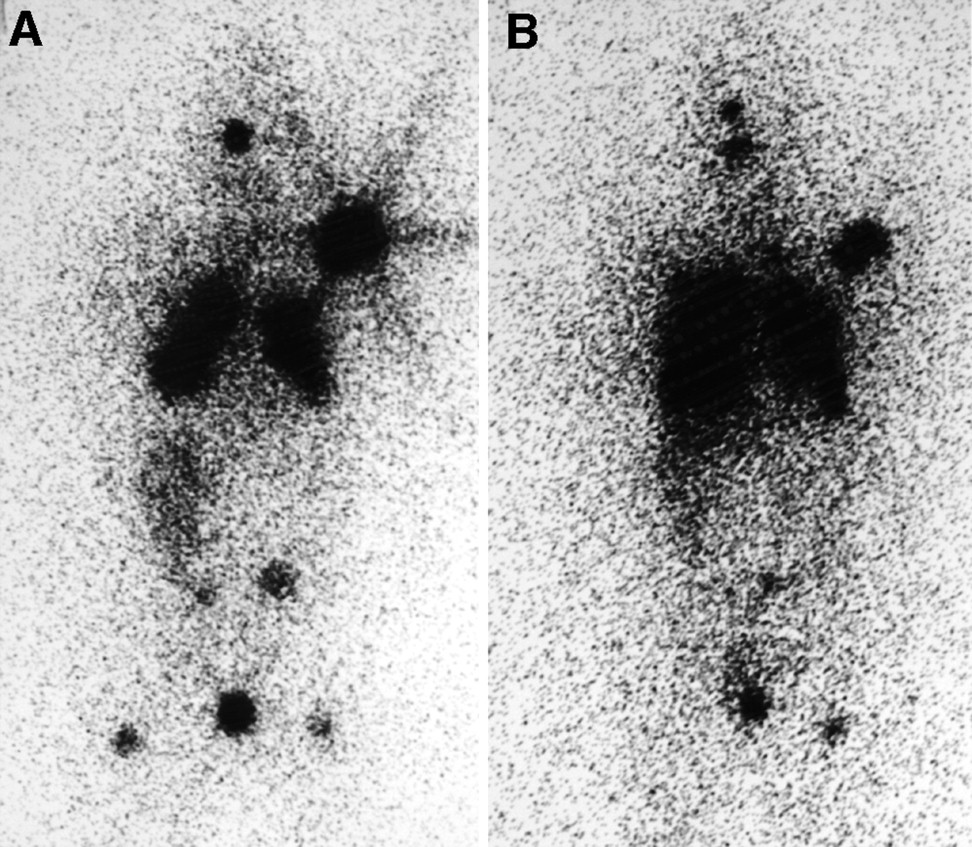
Anterior scintigraphic images of patient 1 made 48 h after 18.5 MBq of diagnostic 131I were administered. (A) Before first 131I therapy, radioactivity concentrations are seen irregularly throughout both lungs, in left shoulder, and in skull and as small foci in spine, pelvis, and femurs. Activity in liver is contiguous with and below that in right lung. (B) Before fifth 131I therapy, although lungs appear more prominent, radioactivity concentration is overall less and absent from some regions of small foci.

Anterior radiographs of chest of patient 1. (A) Before first 131I therapy, macronodules are readily visible in upper lungs and are widespread. Heart failure is evident. (B) After all 5 131I therapies, nodules appear slightly smaller and heart failure has disappeared although cardiomegaly persists.
Hormone and Dosimetric Data
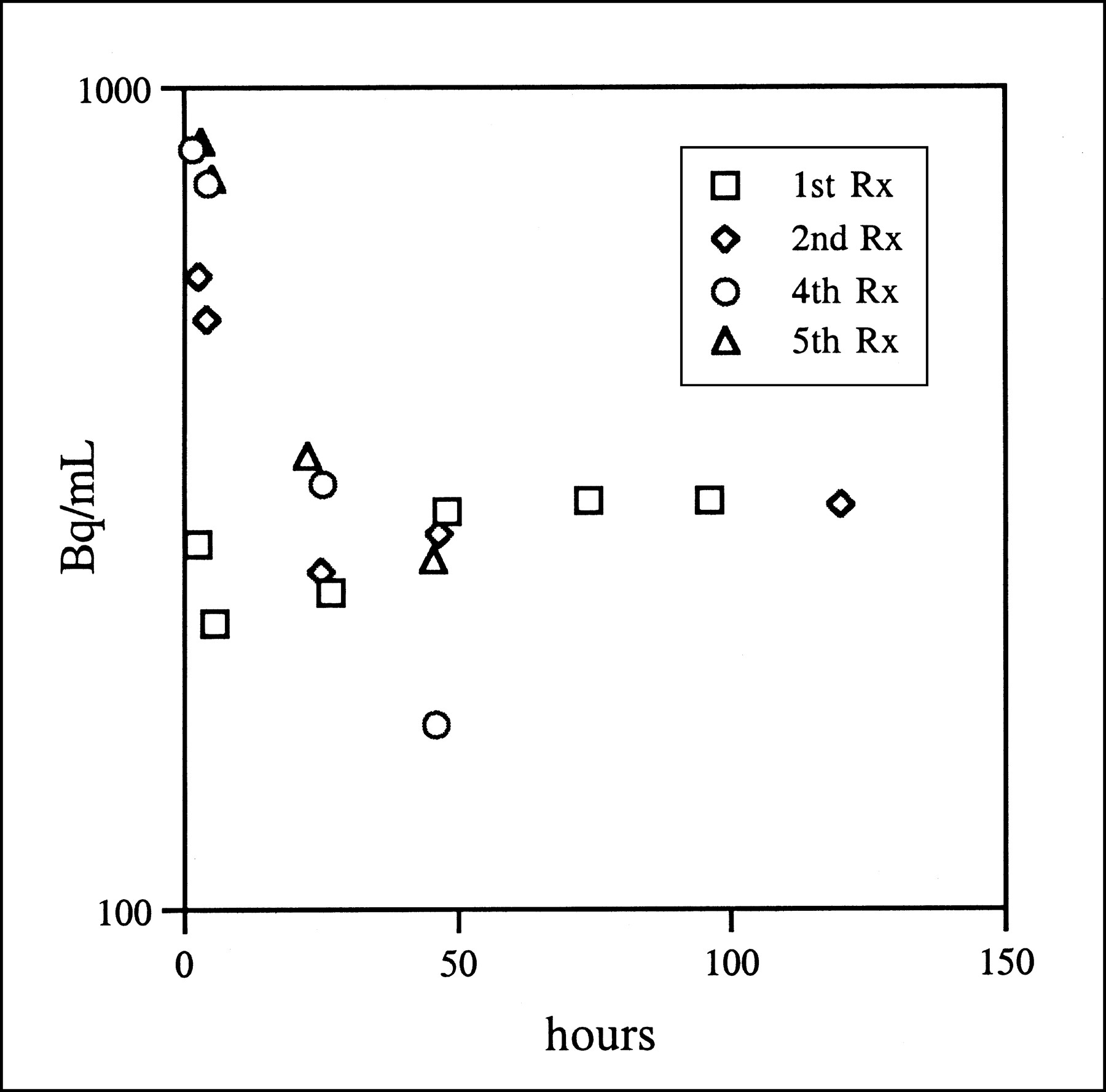
Eighty-five percent of the diagnostic activity was retained in the patient’s body at 48 h (Table 1A). The initial goal was to end the hyperthyroidism and, at the same time, keep the absorbed radiation within the guidelines. Radioiodine (1.85 GBq) was prescribed and calculated to deliver 194 cGy to her blood. However, because the time–activity curve for blood radioactivity (Fig. 3) was complex and inscribed an initial decline in activity from excretion of radioiodide and a subsequent rise presumably from the appearance of radiothyroxine secreted by the tumors, the calculation was recognized as an estimate. Images of the administered therapeutic radioactivity at 48 h showed no previously unseen metastases. Hematologic values did not become abnormal after the dose was given (Table 2A). Propylthiouracil was resumed.

Time–activity curves from patient 1 after diagnostic 131I. Radioactivity declines in first 2 studies but then rises and plateaus as radioiodide is converted into secreted radiothyroxine. Initial declines in radioactivity are slower before treatments 2, 4, and 5 than before treatment 1 because radioiodide is being sequestered less rapidly by thyroid tumors. Rx = treatment.
Hematologic Data Related to 131I Therapies
In April 1998, the general pattern of data was about the same except that the antithyroid medication prevented hyperthyroid symptoms, and heart failure had largely resolved. The blood time–activity curve now showed a slower initial decline because of a slower uptake of radioiodide by tissues but was otherwise similar to that in January (Fig. 3). After cessation of the antithyroid drug, the patient was given 2.6 GBq radioiodine (Table 1A). Her blood dose was estimated at 275 cGy, but from the experience with the prior treatment, tolerance of a larger administered activity was expected, and an end to her hyperthyroidism was urgently needed. Mild, temporary leukopenia arising from lymphopenia later developed (Table 2A).
In September 1998, the patient’s TSH level was elevated to 11.1 mU/L 1 wk after the antithyroid medication had been discontinued. She was much improved and was walking 1.6 km (1 mile) per day. Atrial fibrillation had spontaneously resolved. The pain had disappeared from her left shoulder, and mobility of the joint had improved. The scintigraphic pattern was unchanged except that the intensity of 131I in tumors appeared to be less. Blood samples were clotted. Body retention of 131I was 77% at 48 h (Table 1A), similar to that in April, and on the basis of previous experience we decided that she could tolerate a modestly larger treatment activity. Thus, 3.15 GBq 131I were administered to reduce her tumor volumes, which, in the lung, had not clearly changed. When her TSH level remained elevated, thyroxine (0.05 mg/d) was added to her program. Leukocytes declined to 3,100/μL, again from lymphopenia.
In January 1999, the patient remained clinically well but required digoxin and a diuretic because her heart was still enlarged and aortic valve disease was evident. Thyroxine had been discontinued for 6 wk, and her TSH level was 17.8 mU/L (Table 1A). At 4%, her TSI was slightly less. Thyroglobulin was still >30,000 ng/mL, and chest radiography findings were unchanged. For the first time, scintigraphy showed fewer lesions, in that some of the smaller tumors in bone were not seen. Her body retention of diagnostic 131I had declined to 29% at 48 h, and her blood time–activity curve, measured only until 48 h, no longer showed a rise after an initial decline (Fig. 3). Because she had tolerated a blood dose of 275 cGy, we thought a modest increase in the administered activity would not inflict serious toxicity. Moreover, the tail of the time–activity curve was likely to have a half-life less than the 8 d used in the standard calculation of absorbed radiation dose, and the administered 5.7 GBq would therefore impart less than the calculated 311 cGy (Table 1A). The administered activity was still modest by usual standards. Again, a mild and temporary leukopenia developed, this time from a slight depression of neutrophils as well as lymphocytes.
The patient’s thyroxine dose was increased to 0.1 mg/d to keep her TSH concentration in the low normal range; this medication was again discontinued 6 wk before her evaluation in July 1999. Although she had few symptoms of hypothyroidism, her TSH level had risen to 48 mU/L. Thyroglobulin was still markedly elevated. Radiography again showed no clear change in her lung tumors; scintigraphic images portrayed the major tumors, and some of the smaller tumors were no longer visible (Fig. 1B). However, in the presence of hypothyroidism, her body retention of 131I at 48 h had risen to 58%, and the terminal half-life of radioactivity in her blood time–activity curve was slowed from 0.9 to 2.3 d (Fig. 3). We believed that another 131I treatment should be given to see if the tumor could be reduced, but in view of the greater body and blood retention of radioactivity compared with the preceding January, the amount of administered activity was reduced to 4.8 GBq. Insufficient importance was given to the calculated absorbed dose of radiation in blood, 416 cGy, which was actually higher than that in January. At that point we could not readily determine whether the more prominent TSH stimulation enhanced the uptake of 131I by tumors above the level produced by the still-circulating TSI, and hypothyroidism was allowed to prevail during the treatment. Images of the therapeutic dose confirmed the disappearance of some of the smaller bone metastases as seen on diagnostic scintigraphy; no new tumors were present.
During the next few weeks, The patient’s blood elements declined substantially: leukocytes to 1,900/μL, neutrophils to 1,200/μL, platelets to 59,000/μL, and hemoglobin to 7.2 g/dL (Table 2A). Subsequently, 2 units of blood were transfused to restore her hemoglobin; her platelet levels rose to near normal, and her leukocyte levels increased but remained subnormal.
The patient had, at that time, received a cumulative activity of 18.1 GBq 131I. In January and March 2000, her radiographs showed the lung tumors to be slightly smaller (Fig. 2B), and her thyroglobulin level was 17,800 ng/mL, a substantial value but less than at the outset of treatment (Table 1A). Her TSI was lower but still elevated at 3.1. The patient felt almost as well as before the onset of her illness. No further 131I treatments were planned unless the lung tumors increased in size or number.
Patient 2
In 1978, at the age of 60 y, this woman underwent a partial thyroidectomy that was said to have removed thyroid cancer. She had no symptoms related to the cancer until back pain began in 1996. In mid 1997, weakness in her lower legs began to impair walking. At the same time, urinary retention developed and a neurogenic bladder was discovered. The symptoms arose from a 6-cm mass that on CT was seen to involve the right psoas muscle, destroying the L1 vertebra and impinging on the thecal sac. Needle biopsies produced follicular thyroid tissues. An indwelling catheter was inserted. The patient received external-beam irradiation of 4,500 cGy to her back tumor.
A CT scan portrayed thyroid tissue that extended substernally in each lobe. In September 1997, the residual thyroid tissue in the patient’s neck was surgically excised. The right thyroid gland adhered to the trachea and contained a 5-cm nodule. The nodule exhibited well-differentiated microfollicles, and the accompanying vascular invasion and mitotic figures led to the diagnosis of follicular carcinoma.
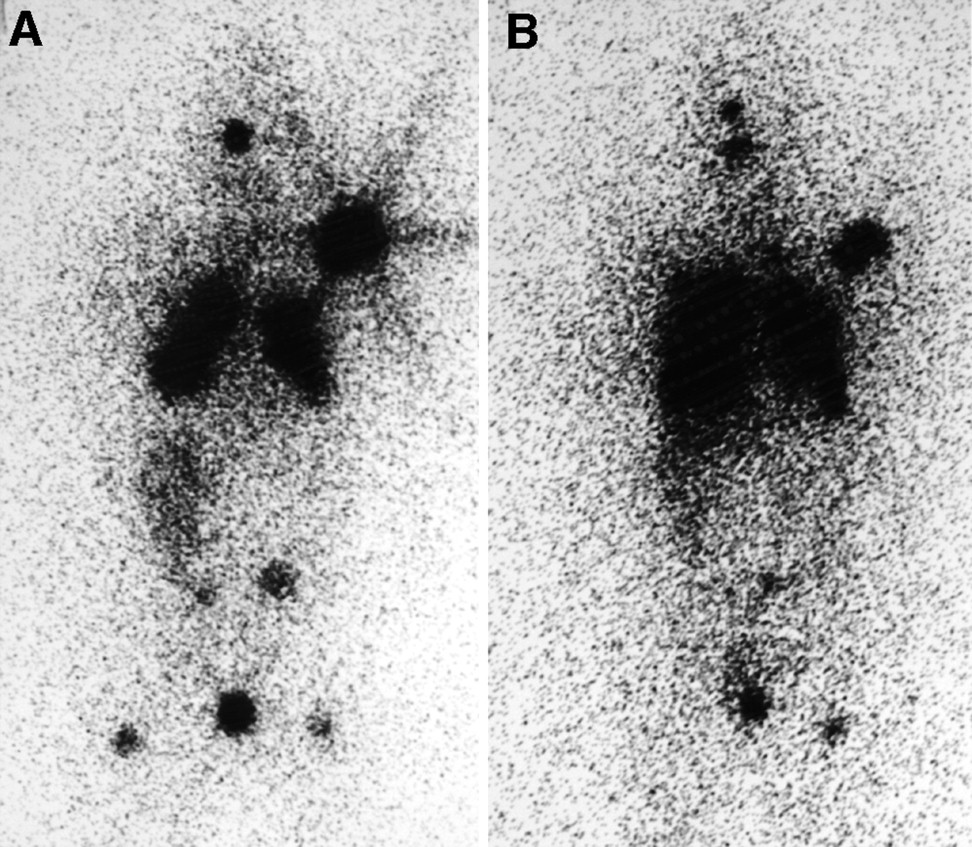
Because of difficulty with transportation, the patient did not return for further evaluation and treatment until December 1997. She was receiving several medications for back pain that radiated down both legs. Weakness prevented walking, but sensory function was intact. Her urinary catheter was still in place. Clinical hypothyroidism was not obvious. Although she was receiving no oral thyroid hormone, her serum thyroxine level was 7.6 μg/dL and her TSH level, at 18 mU/L, was only modestly elevated (Table 1B). At 4,800 ng/mL, her thyroglobulin level was markedly elevated. No TSI was present, but the tumor appeared to function with some autonomy. Scintigraphy depicted an intense concentration of 131I in the tumor in her back (Fig. 4A) and a focus of radioactivity in her frontal bone that correlated with a destructive lesion in the skull seen on radiography. Another focus in her upper left neck reflected a presumed lymph node metastasis, but no tissue was evident in the thyroid bed. CT of her spine revealed enlargement of the mass since the radiation therapy (Fig. 5A).

Anterior scintigraphic images of patient 2 obtained 48 h after 35 MBq of diagnostic 131I were administered. (A) Before first 131I therapy, largest concentration of radioactivity is in region of tumor in upper lumbar spine. Other foci of metastases are in skull and mid neck. Radioactivity in liver is above and to right of spine tumor. (B) Before third 131I therapy, radioactivity concentrations in spine and skull are less intense. Foci in separate neck node metastases are visible. Stomach is visible, and bladder activity is at bottom.
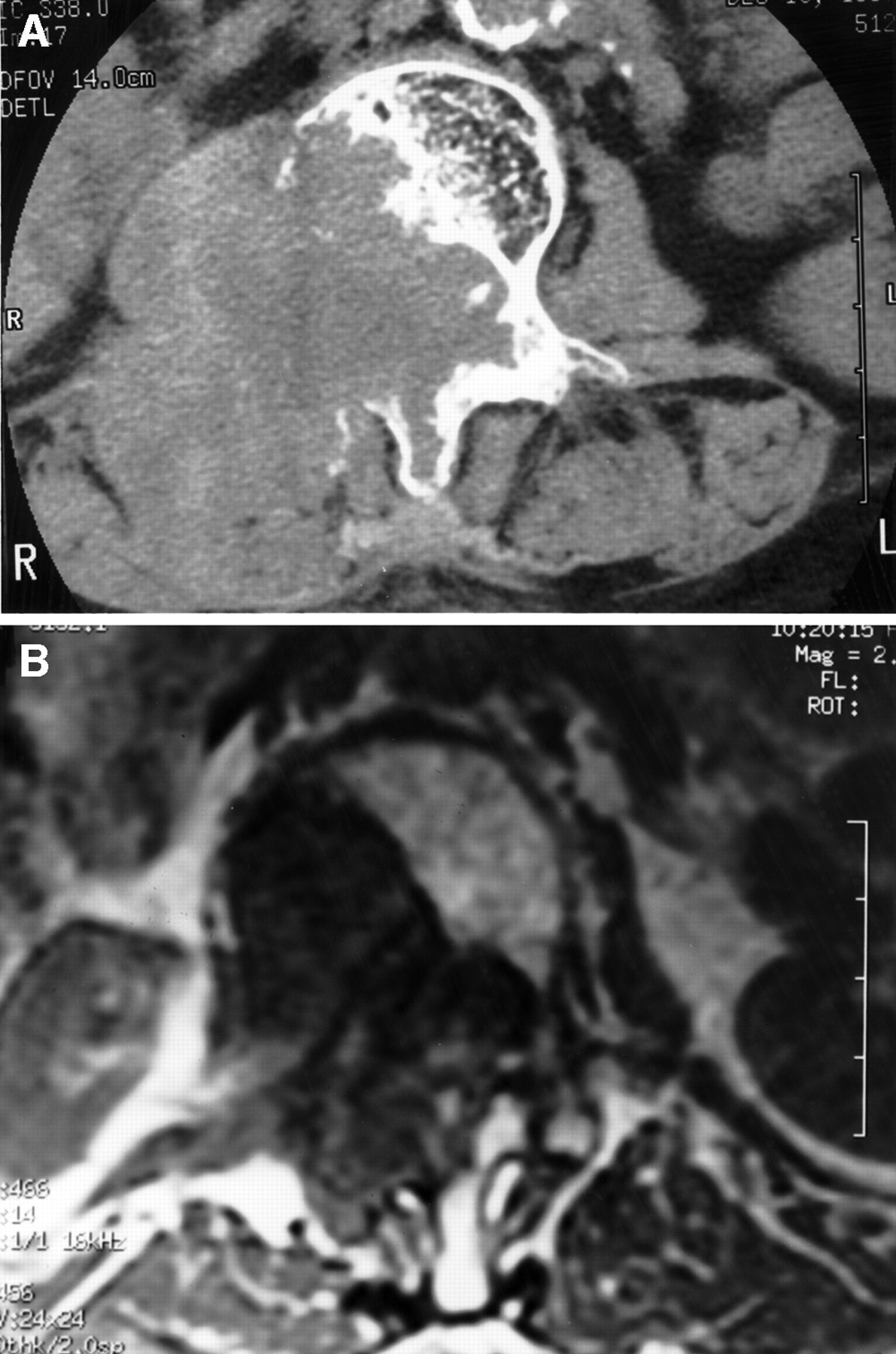
CT (A) and MR (B) images of patient 2. Before first 131I therapy, CT section shows partial destruction of L1 vertebra and soft-tissue mass to right. Before third therapy, MR section shows similar destruction of L1 but markedly reduced soft-tissue mass.
Dosimetry showed 58% retention of the diagnostic dose of 131I at 48 h. Blood radioactivity did not show a decline and subsequent rise as in the first patient, but the decline during 72 h was relatively slow; from the 2.2-GBq 131I therapy, the absorbed radiation dose in the blood was estimated to be 222 cGy (Table 1B). Images made after the therapeutic dose portrayed no previously unidentified tumors. The patient then was given thyroxine, 0.125 mg/d. Hematologic findings did not change after these treatments (Table 2B), but the thyroglobulin level declined to 480 ng/mL and the TSH level fell to 1.1 mU/L (Table 1B). By April, she had less pain was able to ambulate with a walker and to urinate without a catheter.
In September 1998, the patient’s clinical improvement was sustained. She had discontinued her thyroxine treatment for 6 wk, and again, clear clinical hypothyroidism did not develop; her TSH level rose to only 8 mU/L. Her thyroglobulin level in the absence of exogenous thyroid hormone had risen to 1,310 ng/mL, a value considerably less than that before 131I treatment. CT of the spine showed a diminution in the volume of the lumbar tumor. Her scintigraphic pattern of diagnostic 131I was similar to that in December. Retention of 131I in her body was 39% at 48 h and less than measured previously. Blood samples were not assayed. On the basis of the data available and experience from the first therapy, 4.6 GBq 131I were administered. A mild decline in leukocytes (lymphopenia) was seen at approximately 6 wk, but no other toxicity was evident. At that time her TSH level, 21 mU/L, was even higher despite thyroxine therapy, but her thyroglobulin level was at its lowest, 110 ng/mL
The patient could not return for evaluation until February 2000. Her clinical improvement was sustained, and she required only intermittent medication for pain. Thyroxine therapy had not yet reduced the TSH level to within the normal range, and the thyroglobulin concentration was similar to that measured in the previous examination, 150 ng/mL. When the thyroxine was stopped for 5 wk, her TSH level rose to 34 mU/L and her thyroglobulin level rose to 247 ng/mL (Table 1B). Although 131I concentrations were less intense in the tumors, the scintigraphic pattern was again unchanged (Fig. 4B). An MR image of her spine showed a further reduction in the soft-tissue component of the tumor (Fig. 5B). The destructive lesion in her skull was radiographically the same. As was the case for patient 1, we could not determine whether TSH increased what appeared to be autonomous function by the tumors.
The patient’s retention of diagnostic radioiodine, 23% at 48 h, was less than previously. Again, blood radioactivity was not measured, but because endogenous synthesis of thyroxine was then lower (free thyroxine, 0.67 ng/dL) and body absorbed radiation per gigabecquerel was calculated to be less, she was given a third treatment with 131I, at 5.6 GBq, to prolong the partial remission (Table 1B). She then had a cumulative activity of 12.4 GBq. Although preceding leukocyte and neutrophil counts were normal, she manifested moderate leukopenia and neutropenia at the time of treatment; the values fell slightly afterward (Table 2B).
DISCUSSION
Thyroid carcinomas rarely produce sufficient thyroid hormone to cause hyperthyroidism. Since a review of the literature on the subject in 1990 (13), 2 articles (14,15) have recorded the newer cases. Most of the affected patients manifested follicular carcinomas; few had the papillary type. Although 6 patients have been cited as exhibiting TSIs (16–20), 3 may not have been in this category because the assay for the immunoglobulins lacked specificity (19,20). Our first patient appears to be unique in exhibiting both papillary histology and stimulating immunoglobulins.
Life-threatening acute toxicity is rare, and profound bone marrow depression is uncommon in patients treated with 131I for thyroid cancer. Moderate administered activities are unlikely to exceed the level of safety, but the presence of bulky functioning tumors, especially those that secrete thyroid hormone, warns that the margin for safety is reduced. Yet, patients with these manifestations also present an opportunity to impart radiation that will substantially reduce the morbidity of the carcinomas. The dosimetric guidelines to help prevent acute toxicity have not been reassessed recently but probably still define thresholds that deserve attention.
Two clues to a risk of toxicity from moderate activities of 131I (e.g., 3.7–7.4 GBq [100–200 mCi]) are the presence of a large amount of tumor and a serum thyroxine level within or above the reference range. In the absence of appreciable normal thyroid tissue and of exogenous hormone therapy, a measurable concentration of serum thyroxine implies secretion of thyroxine by the neoplasm. After treatment with 131I, several radiolabeled compounds are released to the circulation (21), but the most persistent will likely be radiothyroxine, which will circulate with a half-life of 3–4 d (22) and much longer than radioiodide. The circulating radiothyroxine will impart levels of radiation to the bone marrow not seen in the usual patient with thyroid carcinoma. Moreover, radiothyroxine will enter the circulation for some days, and the blood level of radioactivity may rise and only gradually decline in a pattern difficult to predict.
Estimates of blood radiation based on body retention data (23) will not be valid in the presence of increasing levels of radiothyroxine. Calculations of absorbed radiation to the blood should be valuable indices of toxicity from 131I treatments. Unfortunately, blood dosimetry is not easy. Moreover, blood radioactivity measured for as long as 8 d may show little or no decline in activity (1), and little information will be available on which to base the tail of the time–activity curve. Data collected for 4 d for clearance fitting (24) will also not be sufficient for constructing complex curves of blood radioactivity. In our first patient, blood activity appeared to be at constant levels from 48 to 96 h (and probably longer) in the study preceding the first treatment, and for as long as 120 h in the study preceding the second treatment. A subsequent 8-d half-life for blood activity (1) is a conservative assumption, but the error is unknown and may be substantial.
In addition, calculations of radiation absorbed by the bone marrow from the blood have not considered the rising levels of blood radioactivity. Thus, the published ratios of marrow-to-blood activity (25) cannot be used to predict absorbed marrow doses in patients with functioning thyroid tissue.
When recombinant human TSH was used to stimulate function in residual thyroid carcinoma in euthyroid patients, excretion of radioiodide from the body was seen to be more rapid than when the same patients were hypothyroid (26). This change became apparent in our patient 1 when her hyperthyroid state was converted to marked hypothyroidism before her fifth treatment with 131I. Recognition of the more prolonged retention of 131I led to the prescription of less 131I activity than for the prior therapy. Even so, bone marrow depression followed. The effects of increasing hypothyroidism were not seen in the calculations made for patient 2 because her hypothyroidism was present to approximately the same degree at the time of each treatment.
The onset of hypothyroidism might have accounted for the observations recorded for a patient who, after dosimetry measurements, received 7.4 GBq 131I, with disappearance of several metastases and no toxicity (4). When the same patient was given an additional 9.25 GBq without repetition of dosimetry, profound bone marrow depression developed.
From our experience, we recommend several guidelines for the 131I treatment of patients with thyroid carcinoma. Patients with bulky, functional metastases may retain 131I longer than do most individuals with well-differentiated carcinoma. Our first guideline is that for these unusual patients, body retention of 131I should be measured, as is easily done, and the value at 48 h should be used for guidance. Retention > 30% should be considered a warning of increased radiation to normal tissues.
Although hyperthyroidism caused by tumor function is rare, carcinomas that secrete thyroid hormones at lesser levels are probably not, and patients with these types of cancer are also at increased risk from radiation of the bone marrow. Much more common are patients who have had subtotal thyroidectomy and retain sufficient normal thyroid tissue to produce substantial amounts of radiothyroxine if the ablative dose of 131I is >3.7 GBq. In the absence of exogenous hormone, a serum thyroxine level that is near normal, normal, or elevated indicates that radiothyroxine will be secreted and will circulate to increase the irradiation of the bone marrow. This effect will occur even if the serum thyroxine is derived from secretion by normal thyroid tissue. If the level of serum thyroxine is measurable, dosimetry will be enlightening; in the absence of dosimetry, 131I doses can be reduced reasonably. The maximum permissible dose based on 48-h retention of 131I should be reduced, and as our second guideline, we propose a reduction to 50% if the patient is hyperthyroid, 60% if euthyroid, and 75% if mildly hypothyroid.
As an example, for patient 1 the first treatment with 131I would have been based on a 48-h retention of 87%. Guidelines (1) state that the maximum administered activity permitted in the body at 48 h in the presence of diffuse lung metastases is 3 GBq, and without further consideration, her treatment could have been 3 GBq/0.87, or 3.45 GBq. However, in the presence of hyperthyroidism, our proposal would be to reduce the maximum administered activity to 50%, or 1.72 GBq. She actually received 1.85 GBq. The last treatment would have been based on a 48-h retention of 58%; her maximum treatment would then have been 3 GBq/0.58, or 5.17 GBq. Because she was hypothyroid yet still had measurable production of thyroxine (free thyroxine, 0.4 ng/dL), her administered activity should have been reduced to 75% of 5.17 GBq, or 3.88 GBq. She actually received 4.81 GBq, and bone marrow suppression developed.
Our third guideline is that attainable goals of therapy should be determined by the general health of the patient, the extent of the tumor, and the metabolic response to thyroid hormone. Care should be taken not to worsen the condition of patients, especially those in frail health or with already depressed bone marrow function. Distant metastases are difficult to eradicate, and in particular, macronodules in lung and bone deposits usually persist even after many treatments. In addition, the presence of TSI may increase the aggressiveness of thyroid carcinomas (27,28). On the other hand, hyperthyroidism can be eliminated by 131I therapy, and as in our patient 1, remarkable clinical improvement can follow attainment of this limited goal alone. Relief of pain and of neurologic deficits is also an obvious and achievable goal, as in our patient 2. Additional treatments with 131I may reduce tumor volume and prolong a partial remission, but this goal is not easily defined, and care should be taken to avoid toxicity in its pursuit.
Hypothyroidism will increase the levels of circulating TSH, but carcinomas that are stimulated by TSI or that function autonomously may not gain much, if any, function from the actions of TSH. Moreover, if TSI is present, it is likely to persist as long as the neoplasm remains a source of antigen. Suspicion should be aroused when euthyroidism is reached with little or no thyroxine therapy. Our final guideline is that imaging should be performed when TSH levels are low, normal, or slightly elevated to determine the function of the neoplasms. If 131I is reasonably sequestered by the tumors (as estimated from body retention of 131I and scintigraphic patterns), then treatments with radioiodine may best be performed without increasing TSH stimulation by thyroxine withdrawal or by injections of recombinant human TSH. As in patient 1, the hypothyroid state can reduce the target-to-background ratio by disproportionately increasing retention of 131I in normal tissues.
CONCLUSION
As exemplified by our 2 patients, individuals with advanced, well-differentiated thyroid carcinoma will benefit from treatments with 131I. However, moderate to high levels of administered activity will pose a risk of toxicity to normal tissues when substantial amounts of tumor or normal thyroid gland are present, especially if radioiodide is converted to circulating radiothyroxine. In our 2 patients, administered radioactivities were curtailed on the basis of dosimetry measurements. Although dosimetry of radioactivity in blood samples acquired for 2–5 d gave warning, absorbed radiation doses eluded accurate calculations. As a basis for prescription of administered activities of 131I, we suggest taking into account the concentration of circulating thyroxine; the retention of radioactivity in the patient’s body at 48 h; the presence of the thyroid stimulators, TSH and TSI; and the overall status of the patient.
Acknowledgments
The authors thank Drs. Adam Tonakie, Ian Kirkwood, Zita Ballok, Shyam Dandamudi, and Ernesto Chioko for caring for the patients. Dr. David Jamadar gave valuable insights into the changes on radiographs. Judith Csoka provided expert typing and editing. Sue Lawson provided invaluable technical assistance.
Footnotes
Received Nov. 7, 2000; revision accepted Feb. 15, 2001.
For correspondence or reprints contact: James C. Sisson, MD, Division of Nuclear Medicine, Hospital B1 G505A, University of Michigan Health System, Ann Arbor, MI 48109-0028.
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Complications of Radioactive Iodine Treatment of Thyroid Carcinoma
- Uncommon Causes of Thyrotoxicosis
- Differentiated thyroid cancer presenting with thyrotoxicosis due to functioning metastases
- Increasing Efficacy and Safety of Treatments of Patients with Well-Differentiated Thyroid Carcinoma by Measuring Body Retentions of 131I