


Abstract
This investigation examined the prognostic power of first-pass radionuclide angiocardiography (RNA) ejection fraction compared with clinical information and myocardial perfusion imaging in patients undergoing pharmacologic stress testing. The value of RNA and myocardial perfusion imaging in predicting death or nonfatal myocardial infarction (MI) is well established. However, limited information exists on the usefulness of combined myocardial perfusion imaging and RNA to predict prognosis, especially in patients undergoing pharmacologic stress testing. Methods: We identified 240 patients who underwent pharmacologic stress testing with myocardial perfusion imaging and combined RNA. The patients were followed for a mean of 1.4 y. Cox proportional hazards models were used to assess the value in predicting death and MI. Multivariable models were generated to assess the independent incremental predictive value of clinical and nuclear imaging variables. Kaplan-Meier survival and event-free survival estimates were examined in patients with low (≤45%) versus high (>45%) ejection fractions. Results: Clinical information, myocardial perfusion imaging, and RNA ejection fraction were significant predictors of the death/MI composite outcome (χ2 = 7.4, 14.0, and 21.8, respectively). The addition of myocardial perfusion imaging to the clinical information provided incremental prognostic information (χ2 = 15.2). The addition of RNA ejection fraction provided further predictive information (χ2 = 22.5). However, when RNA ejection fraction was first added to the clinical information, myocardial perfusion imaging had no incremental prognostic value. Conclusion: For hard cardiac events, RNA ejection fraction provides prognostic information besides that provided by clinical and myocardial perfusion imaging. In patients who cannot exercise and are undergoing noninvasive evaluation with pharmacologic stress testing and myocardial perfusion imaging, ejection fraction should be measured simultaneously for risk assessment optimization.
Despite significant improvements in the management of patients with ischemic heart disease and the decreasing mortality rate attributable to myocardial infarction, cardiovascular disease remains the leading cause of death in developed nations. Early identification of patients at high risk for cardiac events can guide management and may improve survival. Clinical information and noninvasive stress testing with myocardial perfusion imaging or radionuclide angiocardiography (RNA) have been shown to provide important prognostic information in patients with known or suspected coronary artery disease (1–14). The excellent prognosis of those patients with normal findings on perfusion imaging has been confirmed by multiple studies showing annual cardiac event rates (death or nonfatal myocardial infarction [MI]) in the range of 1%; patients with abnormal perfusion findings have significantly higher event rates (6,9,15). Similarly, rest and exercise stress ejection fraction as measured by RNA has also been shown to correlate well with outcome (12–14).
The development of 99mTc-labeled myocardial perfusion tracers and improved computer technology in recent years has enabled the assessment of both myocardial perfusion and ventricular function during a single injection of radiopharmaceutical (16,17). However, relatively little prognostic information exists on the usefulness of combined testing with myocardial perfusion imaging and first-pass RNA, especially in patients who cannot exercise and must undergo pharmacologic stress testing. The purpose of our investigation was to examine the relative prognostic power of first-pass RNA ejection fraction compared with clinical information and myocardial perfusion imaging in patients who have a high pretest likelihood of coronary artery disease and are to undergo pharmacologic stress testing.
MATERIALS AND METHODS
Patient Population and Clinical Information
Between September 1993 and July 1998, 26,993 patients underwent a nuclear cardiology examination at Duke University Medical Center. Nearly half (12,815) of these patients had perfusion imaging, and 4,422 patients underwent pharmacologic stress testing because of their inability to exercise adequately or their medical condition (low exercise tolerance, systemic hypertension, left bundle branch block, claudication, cerebral vascular accident, or degenerative joint disease). Of these patients, 353 underwent combined assessment with myocardial perfusion and first-pass RNA for measurement of ejection fraction. We identified 240 patients with a high likelihood of coronary artery disease who also underwent cardiac catheterization either before (78 patients) or after (162 patients) nuclear imaging. The catheterization database represents a high-risk population for coronary artery disease and includes detailed patient characteristics with extensive follow-up on outcome. Patients with congenital heart disease, significant valvular disease, or previous heart transplantation were excluded.
Demographic and clinical information was collected prospectively for all patients. The study population comprised patients having a moderate-to-high likelihood of coronary artery disease. A prognostic clinical risk index that had previously been validated was generated for each patient using baseline clinical characteristics collected from a history and physical examination, as well as electrocardiography (ECG) results (1). The clinical index included age, sex, chest pain descriptors (typical angina, frequency, course), congestive heart failure symptom severity, history of MI, vascular disease (peripheral vascular disease, cerebrovascular disease, carotid bruits), S3 heart sound, and ECG findings (ST-T waves, Q-wave changes, left bundle branch block, right bundle branch block, left axis deviation, intraventricular conduction defect, premature ventricular contractions).
Pharmacologic Stress Testing
Dobutamine.
Pharmacologic stress testing with dobutamine hydrochloride (Eli Lilly, Indianapolis, IN) was performed using an established protocol. Briefly, an intravenous infusion of 10 μg/kg/min was initiated, with escalation of the infusion rate by 10 μg/kg/min every 3 min until 85% of the age-predicted target heart rate was reached or until the study needed to be ended because of patient symptoms or evidence of significant ischemia. The maximum dobutamine infusion rate was 40 μg/kg/min. Adjunctive intravenous atropine sulfate (≤1 mg) was used when the maximum dobutamine infusion rate failed to achieve the target heart rate. 99mTc-sestamibi was injected when any of the above endpoints was reached, and the dobutamine infusion was discontinued. The ECG findings were continuously monitored throughout the study. Heart rate and blood pressure were recorded at 3-min intervals during testing and recovery until hemodynamic parameters returned to baseline.
Dipyridamole.
Dipyridamole (DuPont Pharmaceuticals Co., North Billerica, MA) was administered intravenously using a standard protocol. An infusion rate of 0.142 mg/kg/min for 4 min was used. Blood pressure, heart rate, and continuous ECG findings were monitored during pharmacologic stress and recovery until hemodynamic parameters returned to baseline. 99mTc-sestamibi was administered 2 min after completion of the dipyridamole infusion. Intravenous aminophylline (75–250 mg) was used to reverse significant dipyridamole-induced side effects.
Adenosine.
Adenosine (Fujisawa Healthcare, Inc., Deerfield, IL) was administered using an infusion pump at a rate of 0.142 mg/kg/min for 6 min. 99mTc-sestamibi was injected 3 min into the adenosine infusion. Heart rate, blood pressure, and continuous ECG findings were monitored.
Arbutamine.
Arbutamine (Gen Esa; Gensia, San Diego, CA) was administered through a computerized closed-loop system. The system continuously monitored heart rate and blood pressure and controlled the infusion rate according to preselected maximum heart rate parameters. The infusion rates varied from 0.8 to 12 μg/kg/min. As with dobutamine stress testing, the infusion was continued until 85% of the maximum predicted heart rate was achieved or until the study needed to be ended because of significant side effects or ischemia. 99mTc-sestamibi was injected at the study endpoint, and the infusion was discontinued.
Combined Myocardial Perfusion and Ventricular Function Studies
In all patients, 99mTc-sestamibi SPECT perfusion studies at rest and during pharmacologic stress were performed on the same day. First-pass RNA studies were performed at rest before all pharmacologic stress studies and only during peak stress for dobutamine studies using a previously described protocol (16). Briefly, first-pass RNA during rest was performed after intravenous administration of 259–370 MBq (7–10 mCi) 99mTc-sestamibi (through an external jugular or antecubital vein) using a multicrystal gamma camera (Picker International, Cleveland, OH). Myocardial perfusion imaging was performed with patients in the supine position 1 h after 99mTc-sestamibi injection.
Subsequently, patients underwent pharmacologic stress testing followed by an injection of 777–1,110 MBq (21–30 mCi) 99mTc-sestamibi. RNA ejection fraction was calculated using previously validated methods (11). Perfusion images were interpreted using a 12-segment model and a severity scoring system as follows: 0 = normal perfusion, 1 = mildly decreased perfusion, 2 = moderately decreased perfusion, and 3 = severely decreased perfusion. A summed stress score (SSS) was derived by adding the severity scores for the abnormal segments during stress imaging.
Patient Follow-Up
Baseline clinical, RNA, myocardial perfusion imaging, and catheterization results were collected prospectively and entered into a computerized database. Follow-up data were obtained by mailed questionnaire or telephone interview at 6 mo and 1 y after catheterization and yearly thereafter. The mean duration of follow-up was 1.4 y, with a maximum of 4.6 y (25th percentile = 0.3 y; 75th percentile = 2.2 y). All outcomes were confirmed with clinical data or death certificate information by reviewers who were unaware of the clinical, angiographic, or nuclear cardiology imaging data. Two-year follow-up for survival was >95% complete. The criteria used to diagnose follow-up cardiac events have previously been described by our group (12).
Statistical Analysis
Medians with 25th and 75th percentiles were calculated for continuous baseline characteristics. Categoric variables were described as percentages.
Cox proportional hazards models were used to assess independent predictors of death (all causes) or the death/MI composite endpoint. Variables initially tested using univariate analysis included the clinical risk index, a summed stress perfusion score derived from the 12-segment model, rest first-pass RNA ejection fraction, and peak stress ejection fraction during dobutamine infusion. These variables were preselected on the basis of previously published studies (6,9,11,12) indicating the more powerful predictive value of SSS over summed rest score and ejection fraction measurements over left ventricular volumes. Model assumptions were assessed, and continuous measurements were appropriately transformed.
Multivariate Cox proportional hazard models were then created to assess the independent and incremental predictive contribution of the summed stress perfusion score and RNA ejection fraction after adjusting for baseline risk. Variables were entered into the model in a manner similar to the sequence in which information is obtained when a patient is referred for noninvasive cardiac evaluation using nuclear testing, that is, clinical information followed by the nuclear cardiology test results. The entry of myocardial perfusion and function variables, however, was alternated to identify the most predictive variable and any incremental prognostic information. We assessed the incremental contribution of perfusion and function variables by comparing the likelihood-ratio χ2 values for the model containing only clinical variables with those for the model containing clinical variables plus perfusion information. This result was then compared with a model comprising clinical, perfusion, and functional data. The differences in the χ2 values between models were then used to estimate the incremental contribution of each variable to the overall model of prognosis. Kaplan-Meier overall survival and event-free survival curves were constructed with stratification by rest ejection fraction ≤ 45% or > 45%. Differences in Kaplan-Meier curves were compared by the log-rank test, with statistical significance defined as P < 0.05.
RESULTS
Patient Clinical and Angiographic Characteristics
The demographic and clinical characteristics of the patient population are presented in Table 1. Cardiac risk factors and angiographically significant coronary artery disease were present in the majority of patients. Previous MI was present in one half of the patients, and revascularization procedures (percutaneous transluminal coronary angioplasty or coronary artery bypass grafting) had been performed on 55% of the study population. Only 19% of the patients had no significant coronary artery disease. Mean SSS values as well as first-pass RNA-derived ejection fractions for the entire population are also displayed in Table 1.
Patients’ Clinical and Demographic Characteristics
Pharmacologic Stress Testing
Dobutamine stress perfusion imaging and RNA were performed on 167 patients (70%), whereas vasodilator stress provocation was performed with dipyridamole on 58 patients (24%) and with adenosine on 2 patients (1%). The arbutamine protocol was used for 13 patients (5%). No serious adverse reactions were encountered during pharmacologic stress testing.
Outcome Events
The primary outcomes of interest in this study were death and a death/MI composite endpoint. In this patient population, 39 deaths occurred (16%) and 47 patients (20%) reached the composite endpoint during the follow-up period.
Univariate Models
Univariate or unadjusted relationships between the clinical index, myocardial perfusion as measured by SSS, RNA rest ejection fraction, and the endpoints are presented in Table 2. Each of these variables was a significant predictor of the death/MI composite endpoint. Rest ejection fraction was the strongest predictor of this endpoint, with a χ2 value of 21.8. Only myocardial perfusion and RNA ejection fractions were significant predictors of the death endpoint; ejection fraction had the greatest predictive power, with a χ2 value of 16.0. Additionally, when patients undergoing dobutamine infusion were analyzed separately, both rest and stress RNA ejection fractions were significant predictors of the death endpoint or the death/MI composite endpoint (Table 3). Furthermore, the rest and stress measures of ejection fraction were comparable in the strength of their association with either endpoint.
Univariate Models
Dobutamine Patients with Stress and Rest Ejection Fraction Univariate Models
Kaplan-Meier curves for unadjusted survival and unadjusted cardiac event-free survival stratified by rest ejection fraction are presented in Figures 1A and 1B. For both endpoints, significant differences in survival were observed for the strata (P < 0.001 for both outcomes).

Unadjusted Kaplan-Meier survival (A) and event-free survival (B) curves stratified by ejection fraction (EF) > 45% or ≤ 45%.
Multivariate Models
The results of Cox multivariate analysis are presented in Table 4. After an adjustment for clinical information, perfusion imaging (SSS) added significant prognostic information to the model for predicting death or the death/MI composite endpoint. The addition of ejection fraction after adjusting for clinical risk and perfusion information improved the model to a statistically significant degree. This observation was valid for predicting the death endpoint and the event-free survival composite endpoint. Survival curves, stratified by ejection fraction and adjusted for clinical index and myocardial perfusion information, are presented in Figures 2A and 2B. For both the death endpoint and the event-free survival endpoint, patients with lower ejection fractions had significantly higher event rates compared with patients with higher ejection fractions. The probability values for the contribution of the continuous ejection fraction measurement appear on the adjusted graphs.

Adjusted (for clinical and perfusion results) Kaplan-Meier survival (A) and event-free survival (B) curves stratified by ejection fraction (EF) > 45% or ≤ 45%.
Multivariate Models
Prognostic Value of Ejection Fraction
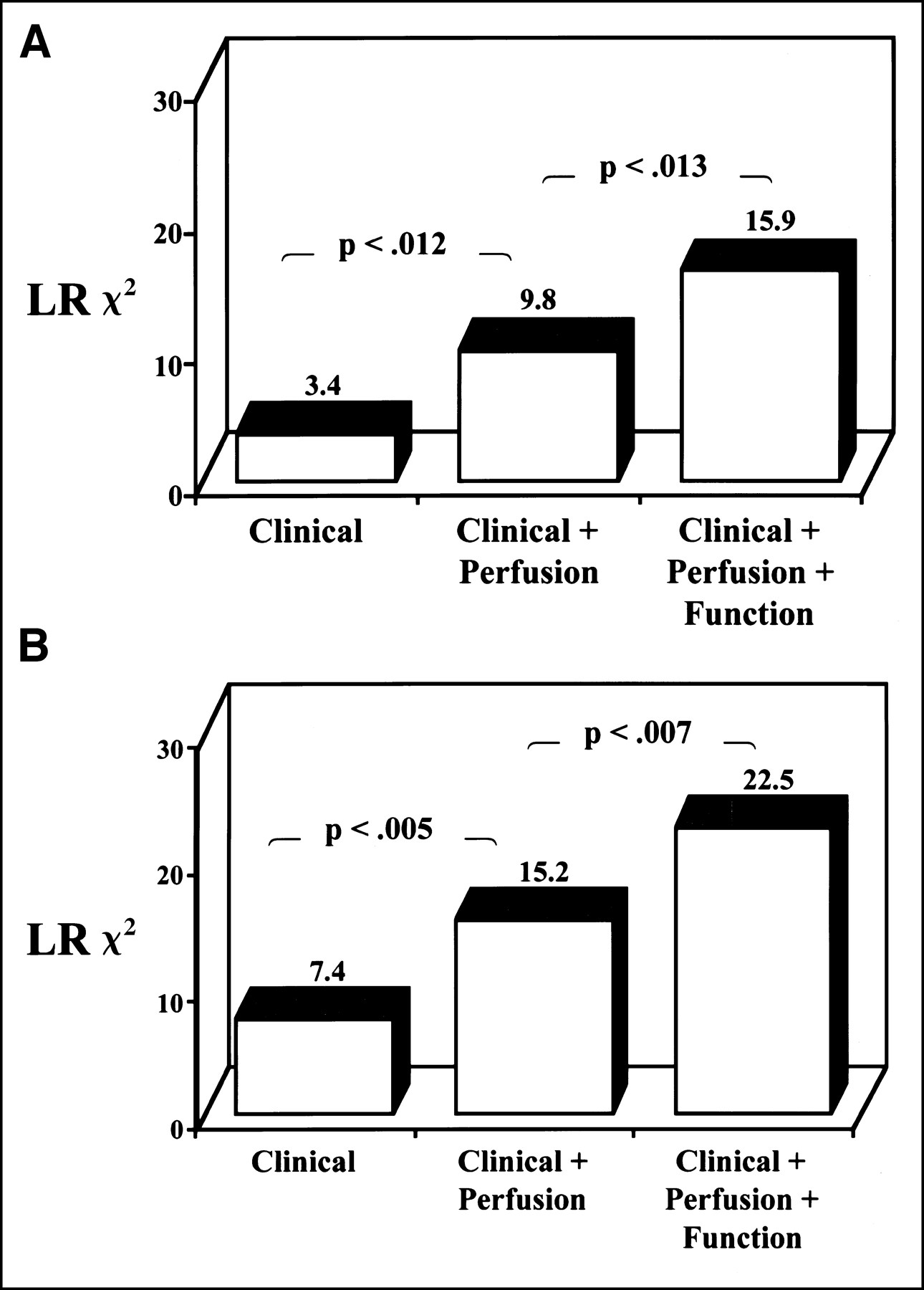
The value of RNA ejection fraction, when added to clinical and perfusion information, for predicting death is summarized in Figure 3A. The clinical index in combination with perfusion imaging provided 61% of information provided by the total model for predicting death. The ejection fraction contributed 39% of the total prognostic information provided by the combination of clinical information, perfusion information, and RNA (P = 0.013). When the event-free survival composite endpoint was considered, clinical and perfusion data together contained 68% of the prognostic information, with ejection fraction adding 32% to the total prognostic information (P = 0.07) (Fig. 3B). When RNA ejection fraction was added to the clinical index before perfusion information was added, the combination of ejection fraction and clinical index contained 99% of the total prognostic information for both endpoints (P < 0.001 for death and P < 0.001 for the composite endpoint) (Figs. 4A and 4B). Once clinical and ejection fraction data were known, no significant incremental prognostic information was obtained by adding perfusion information (P = 0.638 for death and P = 0.586 for the composite endpoint).

Incremental prognostic value of clinical information (clinical index), perfusion imaging (SSS), and RNA (ejection fraction) considered in hierarchical order for prediction of death (A) and death/MI composite endpoint (B). LR = likelihood ratio.

Independent and relative prognostic power of RNA ejection fraction over clinical (clinical index) and perfusion information (SSS) for death (A) and death/MI composite endpoint (B). Once clinical and ejection fraction information was known, no further improvement in χ2 statistics was obtained with addition of perfusion information. LR = likelihood ratio.
DISCUSSION
This study evaluated the prognostic value of pharmacologic stress testing with 99mTc-sestamibi myocardial perfusion imaging combined with first-pass RNA in the evaluation of patients with a moderate-to-high likelihood of coronary artery disease. In this population with a high prevalence of coronary artery disease (81% of the patients), multivariate Cox proportional hazards analysis showed the incremental prognostic value of myocardial perfusion over clinical variables in the prediction of death or the death/MI composite endpoint. Furthermore, when added to the multivariate model, rest ejection fraction as measured by first-pass RNA provided prognostic information beyond that provided by the clinical and perfusion variables combined. This study documents the prognostic power of ejection fraction in patients undergoing pharmacologic stress testing with combined myocardial perfusion and functional imaging studies.
Multiple studies have documented the prognostic value of rest and exercise RNA variables in patients with known or suspected coronary artery disease (12,18). Of these RNA variables, exercise left ventricular ejection fraction has been found to be the single best predictor of cardiovascular events. However, in a recent study that included 863 patients with known coronary artery disease, Shaw et al. (19) found similar prognostic power for rest and stress gated RNA ejection fraction in the prediction of cardiac events. In our study, the addition of rest RNA ejection fraction to the clinical index provided 99% of the prognostic information for the death endpoint and the death/MI composite endpoint. Further addition of perfusion variables provided prognostic information that was then statistically insignificant.
Like rest and exercise RNA ejection fractions, exercise and pharmacologic stress myocardial perfusion imaging has been shown to have an excellent ability to predict cardiovascular events (2–10). Particularly, the extent and severity of reversible perfusion defects, as well as the presence of significant fixed defects, exhibit robust prognostic ability for MI or death. In our study, the prognostic strength of perfusion imaging was confirmed, because both univariate and multivariate models showed that perfusion imaging can independently predict death or the death/MI composite endpoint. Clinical and perfusion data provided 61% of the total predictive ability of the multivariate model for the death endpoint, and the same variables accounted for 68% of the prognostic information for the death/MI composite endpoint.
Little information is available on the usefulness of combined myocardial perfusion imaging and first-pass RNA in the risk stratification of patients with known or suspected coronary artery disease. Furthermore, the few available studies have provided somewhat mixed results. In a study evaluating 412 patients undergoing exercise myocardial perfusion imaging, Nallamouthu et al. (20) found no additional prognostic information from stress first-pass RNA ejection fraction compared with exercise myocardial perfusion imaging alone. The study was limited, however, by a low event rate (14 events) over a relatively short follow-up period. In a report by Marie et al. (21) describing 217 patients undergoing exercise myocardial perfusion imaging and rest RNA, ejection fraction at rest did show significant prognostic power that added to the information provided by perfusion imaging alone. Similarly, Heiba et al. (22) showed independent and predictive power for RNA-derived ejection fraction in patients undergoing dipyridamole stress testing before vascular surgery. In a large study of 1,680 patients undergoing exercise or adenosine-gated myocardial perfusion imaging, poststress gated ejection fraction and end systolic volume provided incremental information for prediction of cardiac events besides that provided by myocardial perfusion imaging (23). In that study, by investigators from Cedars-Sinai Medical Center (Los Angeles, CA), once gated SPECT ejection fraction measurements were obtained, no incremental prognostic value was found by perfusion information, including the SSS, the summed rest score, and the summed reversibility score. In fact, the only variable that actually had independent value for predicting hard events was pharmacologic stress with adenosine. The findings further support our conclusion that patients undergoing pharmacologic stress testing and perfusion studies for diagnostic purposes should undergo an evaluation of left ventricular ejection fraction to further improve, prognostically, the value of nuclear imaging.
Our study further supports the ability of ejection fraction during myocardial perfusion imaging to provide independent and incremental prognostic information. The study is also unique in that most of the patients underwent dobutamine stress testing, with RNA performed both at rest and at peak stress.
The major clinical implication of our study is that measurement of ejection fraction improves risk stratification in patients undergoing pharmacologic stress perfusion imaging studies. On the basis of our study results, in this high-risk patient population unable to exercise, ejection fraction measurement should be included when noninvasive testing is contemplated.
Many nuclear cardiology laboratories now routinely perform multigated acquisition to determine myocardial function during standard myocardial perfusion imaging. The ejection fraction calculated in this manner represents a poststress measurement rather than a true rest or peak stress ejection fraction (24,25). In comparison with first-pass RNA, this technique has several advantages in that it is readily available on many imaging systems, does not require a separate camera, and obviates external jugular venous access for reliable imaging. Because both rest and stress ejection fraction by first-pass RNA appeared to offer comparably robust predictive power in our study, and because excellent correlation between rest first-pass RNA and rest gated myocardial perfusion imaging ejection fraction has been documented (26), our results can likely be extrapolated to the use of gated myocardial perfusion imaging, which is more easily performed. Indeed, our results agree with the recent findings of Sharir and Germano (23), who performed gated SPECT during myocardial perfusion imaging in conjunction with exercise or vasodilator stress testing. Further studies are required, especially among patients undergoing dobutamine stress testing, to more definitively evaluate and compare with RNA ejection fraction the predictive power of gated ejection fraction derived from myocardial perfusion imaging studies.
Although a limitation of our study is use of data from a single site, and validation at other sites would improve the generalizability of these results, data from other institutions has supported similar conclusions in patients at less risk for coronary artery disease using gated SPECT (23). Despite a cardiac event rate of nearly 20% in this study, the relatively small sample size precluded optimal assessment of multiple nuclear imaging variables. The study population contained a heterogeneous mixture of patients undergoing dobutamine and vasodilator stress testing rather than a pure study population. Thus, the number of events occurring among patients undergoing different types of stress testing is relatively small. Furthermore, the significance of peak stress RNA ejection fraction during dobutamine stress testing, which may represent a more physiologic stress ejection fraction compared with measurements obtained after vasodilator testing, is unclear. Studies involving larger patient populations are needed to further clarify these issues.
CONCLUSION
In this study, a clinical risk index, myocardial perfusion imaging, and first-pass RNA ejection fraction were independent predictors of the death/MI composite endpoint. Additionally, myocardial perfusion imaging and first-pass RNA showed a significant ability to predict the death endpoint. By multivariate analysis, the addition of both myocardial perfusion imaging and first-pass RNA ejection fraction provided independent and incremental prognostic information besides that provided by the clinical index alone. Furthermore, once RNA ejection fraction was added to the clinical index, the further addition of myocardial perfusion information made only an insignificant contribution to the model. This study showed that noninvasive risk assessment for patients undergoing pharmacologic stress testing and perfusion imaging is enhanced by simultaneous measurement of first-pass RNA-derived ejection fraction.
Footnotes
Received Oct. 23, 2000; revision accepted Feb. 15, 2001.
For correspondence or reprints contact: Salvador Borges-Neto, MD, Nuclear Cardiology, Duke University Medical Center, P.O. Box 3949, Durham, NC 27710.





{kind=link}
{kind=link}
{kind=link}
{kind=link}