


Abstract
The combination of myocardial perfusion and poststress ejection fraction (EF) provides incremental prognostic information. This study assessed predictors of nonfatal myocardial infarction (MI) versus cardiac death (CD) by gated myocardial SPECT and examined the value of integrating the amount of ischemia and poststress EF data in risk stratification. Methods: We identified 2,686 patients who underwent resting 201Tl/stress 99mTc-sestamibi gated SPECT and were monitored for >1 y. Patients who underwent revascularization ≤60 d after the nuclear test were censored from the prognostic analysis. Visual scoring of perfusion images used 20 segments and a scale of 0–4. Poststress EF was automatically generated. Results: Cox regression analysis showed that after adjusting for prescan data, the most powerful predictor of CD was poststress EF, whereas the best predictor of MI was the amount of ischemia (summed difference score [SDS]). Integration of the EF and SDS yielded effective stratification of patients into low-, intermediate-, and high-risk subgroups. Patients with EF >50% and a large amount of ischemia were at intermediate risk (2%–3%), whereas those with mild or moderate ischemia were at low risk of CD (<1%/y). Patients with EF between 30% and 50% were at intermediate risk even in the presence of only mild or moderate ischemia. In patients with EF <30%, the CD rate was high (>4%/y) irrespective of the amount of ischemia. Conclusion: Poststress EF is the best predictor of CD, whereas the amount of ischemia is the best predictor of nonfatal MI. Integration of perfusion and function data improves stratification of patients into low, intermediate, and high risk of CD.
Stratification of patients into low, intermediate, and high risk of cardiac death (CD) is valuable in deciding on the appropriate treatment modality in patient subsets. Whereas patients at intermediate to high risk of CD benefit from revascularization (1), patients at low risk of CD but at a substantial risk of ischemic events might be better suited for medical therapy (2). Perfusion imaging has been shown to provide incremental prognostic value over clinical data and improves stratification of patients into different levels of CD risk (3–5). We have recently shown that poststress left ventricular ejection fraction (EF) and end-systolic volume, measured by gated myocardial perfusion SPECT, provide incremental information over perfusion and clinical data in the prediction of CD as well as the combined endpoint of CD or myocardial infarction (MI) (6). Harris et al. (7) showed that in patients with normal left ventricular function, nonfatal infarction accounted for at least 50% of initial events, whereas in patients with severe ventricular dysfunction death was the predominant event. However, to our knowledge, the relative importance of perfusion and function in predicting CD and nonfatal MI as separate endpoints has not been determined. Moreover, the interaction between the amount of stress-induced ischemia and poststress EF in stratifying patients into risk levels of CD has not been evaluated.
The aim of this study was to determine the value of gated myocardial perfusion SPECT in the assessment of outcome-specific (nonfatal MI vs. CD) independent predictors and to examine the value of integrating perfusion and function data in stratifying patients into subsets with low, intermediate, and high risk of CD.
MATERIALS AND METHODS
Study Population
We identified 3,191 consecutive patients who underwent separate acquisition, dual-isotope myocardial perfusion gated SPECT (resting 201Tl/stress 99mTc-sestamibi gated SPECT) between July 1, 1992, and January 31, 1997, at Cedars-Sinai Medical Center and were monitored for >1 y for CD and nonfatal MI. Of these patients, 79 (2.5%) were lost to follow-up and therefore were excluded from the study. Patients with nonischemic cardiomyopathy or significant valvular disease were excluded (n = 86), and patients who underwent revascularization within 60 d after the nuclear testing (n = 340) were censored from the prognostic portion of the analysis (8), leaving 2,686 patients (1,678 underwent treadmill exercise and 1,008 underwent adenosine stress testing). Patient follow-up consisted of scripted and blinded telephone interviews. Events were defined as either CD, as noted and confirmed by review of death certificates and hospital charts or physicians’ records, or nonfatal MI, as evidenced by hospital records, indicating the appropriate combination of symptoms, electrocardiography (ECG), and creatine phosphokinase myocardial band (CPK-MB) levels.
Acquisition Protocol
All patients underwent separate acquisition, dual-isotope myocardial perfusion SPECT as described (9). 201T1 111–166 MBq (3–4.5 mCi) was injected intravenously at rest, and SPECT imaging was initiated 10 min later. 99mTc-sestamibi 925–1,480 MBq (25–40 mCi) was then injected during stress, and 8-frame gated SPECT imaging (100% acceptance window) was initiated 15–30 min after exercise or 30–60 min after adenosine stress. Acquisitions were obtained using a 2-detector (Vertex; ADAC Laboratories, Milpitas, CA), 3-detector (Prism; Picker International, Cleveland Heights, OH), or single detector (Orbiter; Siemens Medical Systems, Hoffmann Estates, IL) camera, 60–64 projections over 180° for 35 s (201Tl) or 25 s (99mTc-sestamibi) per projection. The 8 projection sets were summed to generate an ungated set. Projection images were filtered using a 2-dimensional Butterworth filter, order 5 (201Tl) or order 2.5 (99mTc-sestamibi), and a cutoff frequency of 0.25 cycle/pixel (201Tl) or 0.3 cycle/pixel (99mTc) (pixel size = 0.53, 0.64, and 0.61 cm for the Prism, Vertex, and Orbiter, respectively), and reconstructed into transaxial images using filtered backprojection with a ramp filter. No scatter or attenuation correction was applied.
Exercise and Adenosine Protocols
Patients were instructed to discontinue β-blockers and calcium antagonists 48 h before testing and nitrates 6 h before testing, whenever possible. A symptom-limited treadmill exercise test was performed, using the Bruce protocol. Patients received an injection of 99mTc-sestamibi at peak stress and exercised at the same level for an additional 60 s and 2 min more at 1 level lower. Horizontal or downsloping ST segment depression ≥1 mm or upsloping ≥1.5 mm at 80 ms after the J point was considered positive. Failure to achieve 85% of the maximal predicted heart rate or an ischemic ECG response during exercise was followed by conversion to an adenosine stress test.
For adenosine stress, patients were instructed to avoid caffeine-containing products for 24 h before the test. Adenosine (140 μg/kg/min) was infused over 6 min, and 99mTc-sestamibi was injected at the end of the third minute. Whenever possible, patients performed a low-level treadmill exercise during the adenosine infusion. The ECG response was evaluated by the same criteria as those used for exercise testing.
Analysis of Perfusion and Function
Stress and rest perfusion images were scored semiquantitatively using a 20-segment model of the left ventricle and a 5-point scale (0, normal uptake; 1, mildly reduced uptake; 2, moderately reduced uptake; 3, severely reduced uptake; 4, no uptake) (10). The global summed stress score (SSS) and summed rest score (SRS) were calculated by adding the scores of the 20 segments in the stress and resting images, respectively. The summed difference score (SDS), assessing defect reversibility, was derived as the difference between the SSS and the SRS (4).
After automatic reorientation (10), gated short-axis images were processed using quantitative gated SPECT software, and the EF was automatically calculated (11).
Statistical Analysis
Comparisons between patient groups were performed using 1-way ANOVA for continuous variables and the χ2 test for categoric variables. Continuous variables were described as mean ± SD. P < 0.05 was considered statistically significant.
Cox proportional hazards regression analysis was applied to determine the independent predictors of CD and nonfatal MI as separate endpoints. Patients were censored at the first event. Variables were divided into 3 groups: (a) prescan (age, sex, history of MI and revascularization, hypertension, diabetes mellitus, current smoking, angina, and type of stress used); (b) perfusion variables (SSS, SRS, and SDS); and (c) function (poststress EF). Multivariate analysis was performed in a stepwise fashion, evaluating prescan, perfusion, and function data in hierarchic fashion. At each step, variables were entered using the forward Wald method. Of all prescan variables, only the prescan likelihood of coronary artery disease (CAD) was entered to the multivariable analysis to avoid overfitting the model. The prescan likelihood of CAD was calculated using the microcomputer program CADENZA (Advanced Heuristics, Inc., Bainbridge Island, WA) (12), which is based on Bayesian analysis of prescan patient data. For patients undergoing exercise, the prescan likelihood of CAD included clinical, historic, and exercise information; for patients undergoing pharmacologic stress, the prescan likelihood was based on clinical and historic data only. The prescan likelihood of CAD was set to 1 (maximal value) in patients with a history of MI or revascularization.
A value of P < 0.05 in univariate analysis was required for entry into the multivariate analysis. The final model included only significantly independent variables (P < 0.05). Kaplan–Meier survival analysis with stratification by EF and SDS was performed. Survival curves were compared by the log rank test. Correlations between the CD rate and EF and between the MI rate and SDS were evaluated using ANOVA. The statistical analysis was performed using Graduate Pack 9.0 (SPSS, Chicago, IL).
RESULTS
Patient Characteristics
Table 1 summarizes clinical, scintigraphic, and follow-up data on the 2,686 patients who were included in the prognostic evaluation. The mean prescan likelihood of coronary disease was 0.38 ± 0.31, with 1,027 patients (38.2%) <0.20, 1,317 patients (49.1%) between 0.20 and 0.80, and 342 patients (12.7%) >0.80. In patients with previous MI, the median time between the MI and the nuclear test was 3.9 y. Of these 698 patients (26%) (Table 1), only 73 (2.7%) were studied within 3 mo of the MI.
Patient Characteristics
The perfusion scan showed that 1,261 patients (47%) had reversible perfusion defects; 680 patients (25.3%) had a mild or moderate amount of ischemia (SDS, 2–7), and 581 (21.6%) had a large amount of ischemia (SDS, >7). The mean EF was 58 ± 5; 1,956 patients (72.8%) had normal left ventricular function (EF, >50%), 574 (21.4%) had mild or moderate dysfunction (EF, 30%–50%), and 156 (5.8%) had severe ventricular dysfunction (EF, <30%).
During the follow-up (20.9 ± 4.6 mo), 57 CDs (2.12%) and 30 nonfatal MIs (1.12%) occurred. One hundred eighty-nine patients underwent late (>60 d after the nuclear test) revascularization (bypass surgery, 77 [2.9%]; coronary angioplasty, 112 [4.2%]).
Prediction of CD and MI
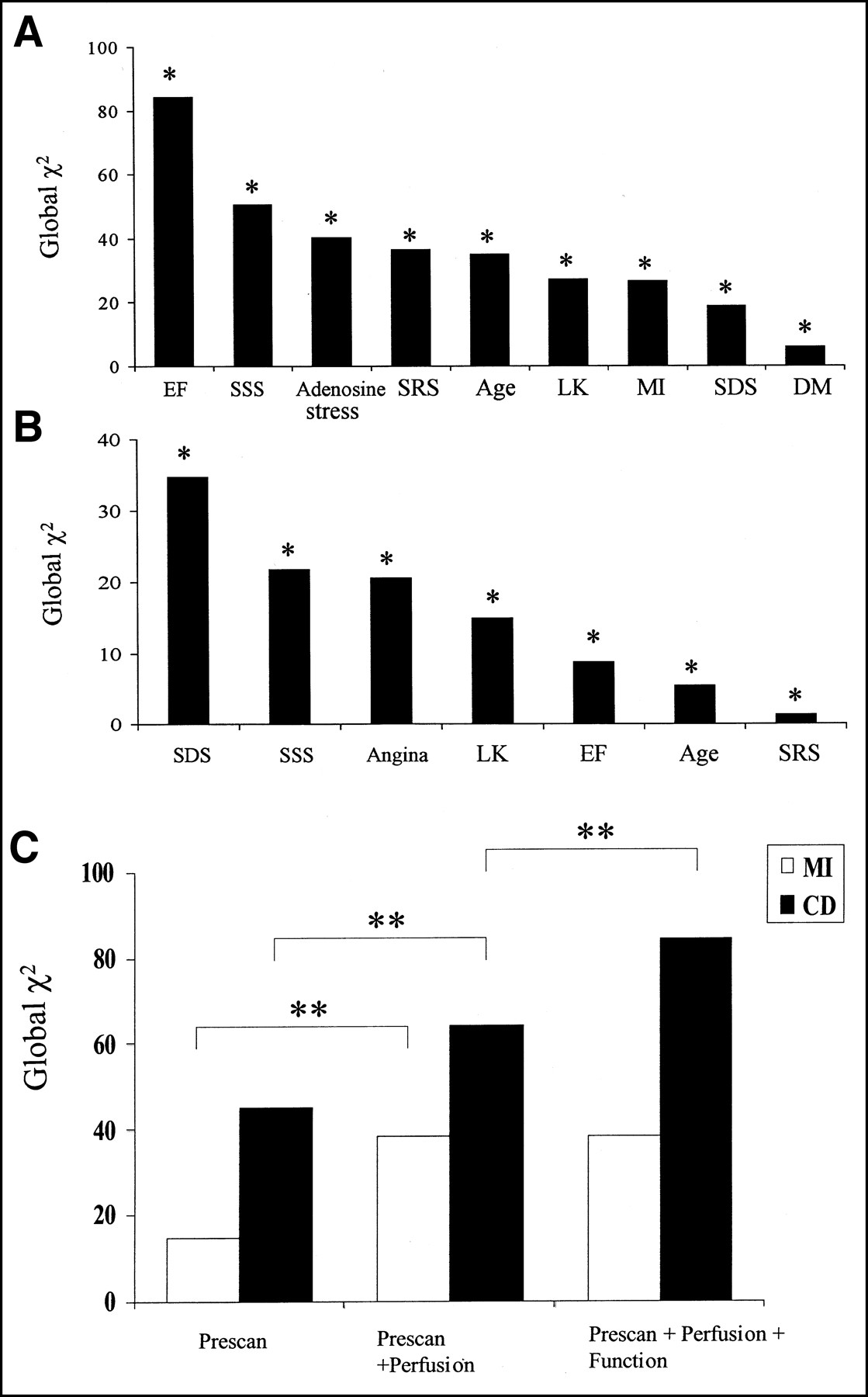
Univariate Cox proportional hazards regression analysis of prescan, perfusion, and function data showed that the best predictor of CD was the EF (χ2, 84.3; P < 0.0001) (Fig. 1A), followed by the SSS (χ2, 50.5; P < 0.0001). The amount of ischemia (SDS) was a significant but weaker predictor of CD (χ2, 18.8; P = 0.0002). The best predictor of MI was the SDS (χ2, 34.7; P < 0.0001) (Fig. 1B). Prediction of MI by EF, although significant (Fig. 1B), was substantially weaker (χ2, 8.7; P = 0.003) than by SDS. The type of stress used (adenosine vs. exercise), history of MI, and diabetes mellitus were significant predictors of CD but not of MI, whereas typical angina was a predictor of MI but not CD.

Univariate (A and B) and multivariate (C) Cox regression analysis for prediction of CD and nonfatal MI. LK = prescan likelihood of coronary disease; DM = diabetes mellitus. *P < 0.02. **P < 0.001.
Multivariate analysis showed that addition of perfusion variables to prescan variables resulted in a significant increase in the global χ2 in the prediction of both MI and CD (Fig. 1C). However, addition of the EF data to the combined model of prescan and perfusion data yielded a significant increase in the global χ2 only in the prediction of CD, whereas no prognostic information was added in the prediction of MI. The statistical results of the final multivariate models for the prediction of MI and CD are summarized in Table 2. The independent variables for the prediction of MI were the amount of ischemia (SDS) and the prescan likelihood of CAD. The independent variables for predicting CD were the EF, adenosine stress, and the prescan likelihood of CAD.
Multivariate Cox Proportional Hazards Analysis: Best Models for Prediction of MI and CD
Risk Stratification
Univariate.
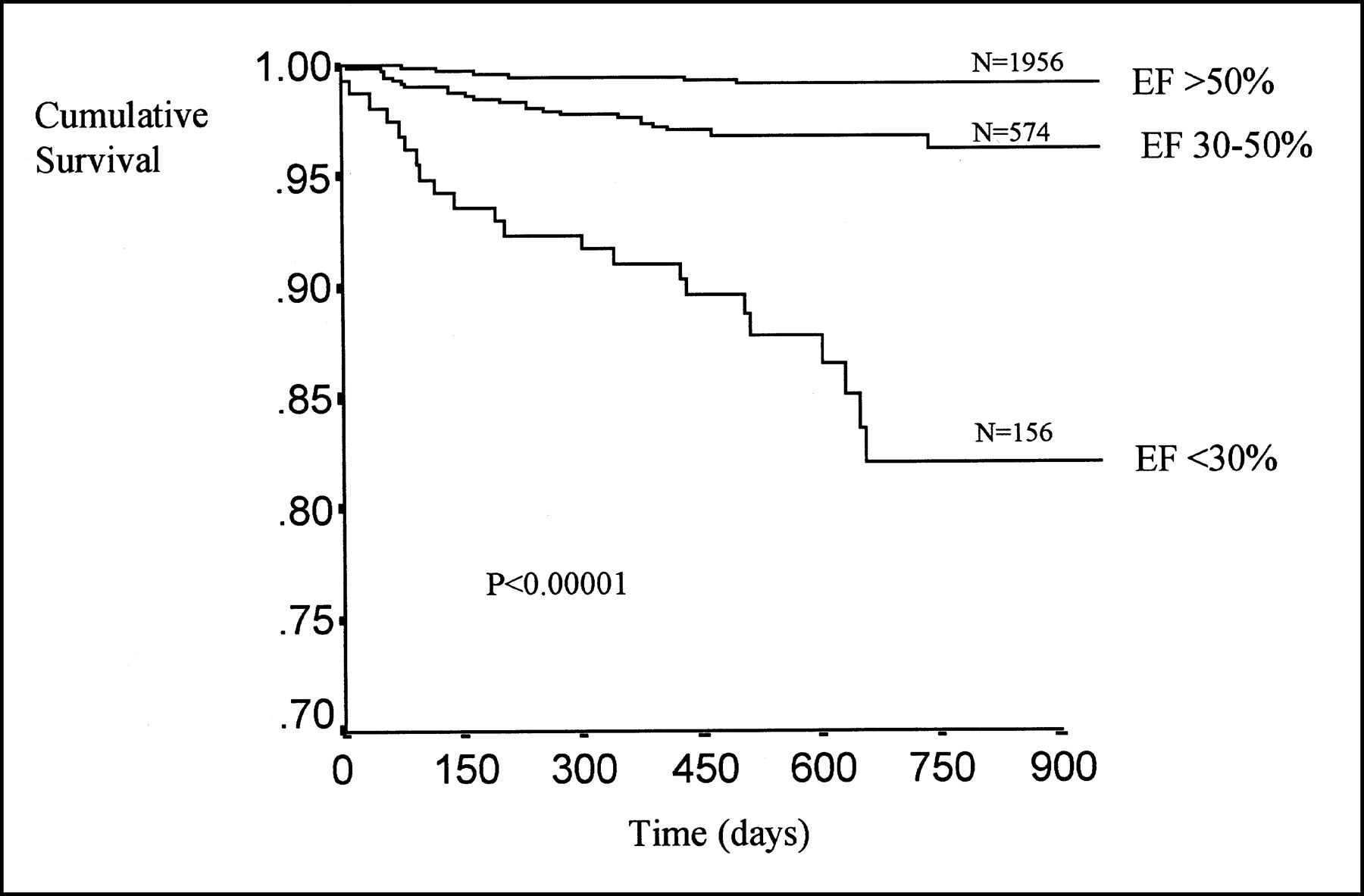
Figure 2 shows an inverse relationship between the average CD rate (%/y) and the EF. Values of the EF were obtained by averaging over 10% intervals. This relationship was best fitted by an exponential curve, yielding a high correlation coefficient (y = 28.5 × e−0.063x; r = −0.99, P < 0.005). According to this curve estimate, the CD rate exceeded 1%/y for EF ≤50% and 4%/y for EF <30%. On the basis of this equation, the study group was stratified into 3 risk categories of CD: (a) EF >50%, low risk (CD rate, <1%/y); (b) EF 30%–50%, intermediate risk (CD rate, 1%–4%/y); and (c) EF <30%, high risk (CD rate >4%/y). Kaplan–Meier survival analysis showed a decrease in survival with decreasing EF (P < 0.000001) (Fig. 3). The large gap between survival curves of patients with an EF between 30% and 50% and patients with an EF <30% is attributed to the exponential relationship between cardiac mortality and the EF.
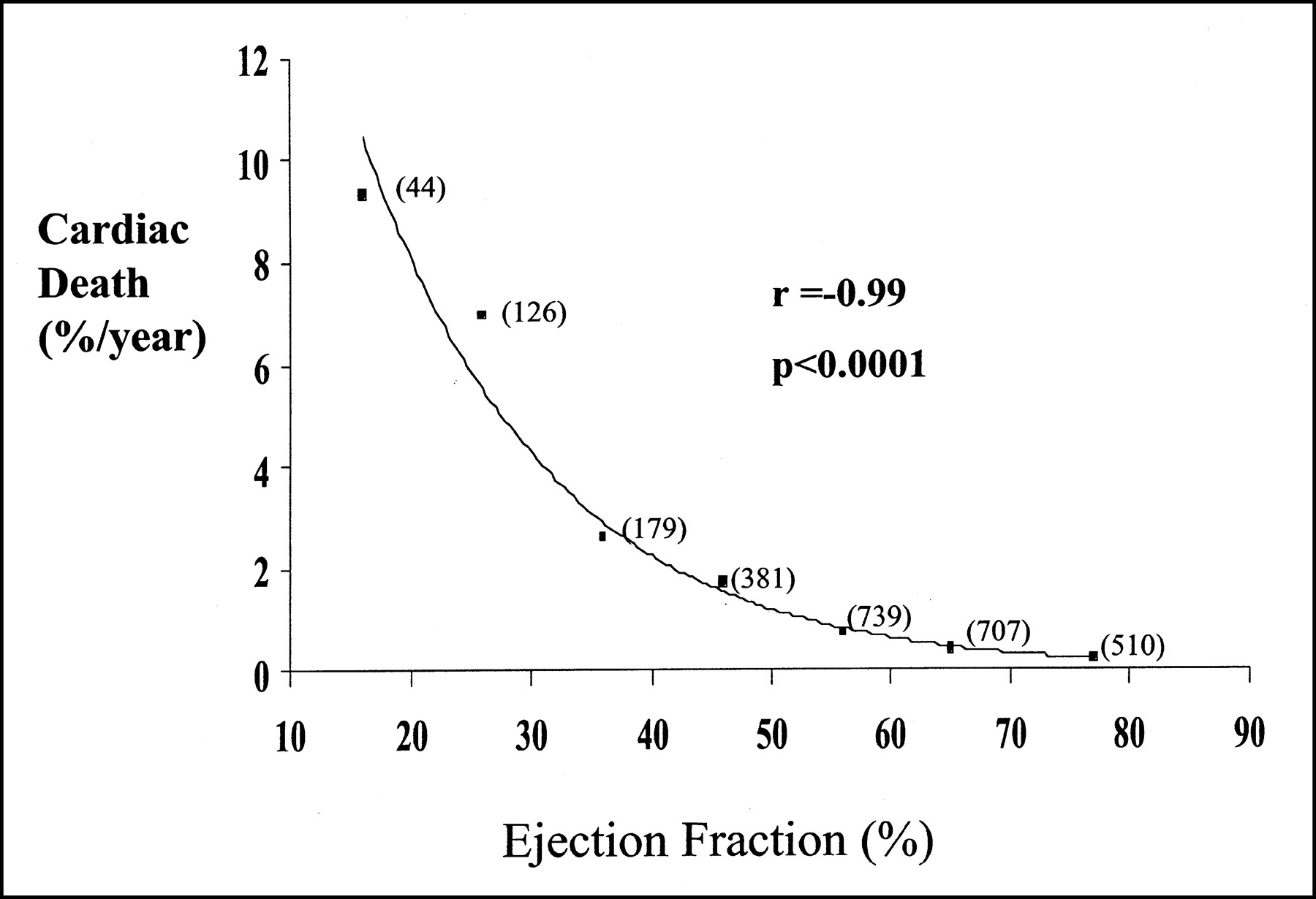
Annual CD rate as function of EF. Number of patients at each 10% interval is indicated in parentheses.

Cumulative survival with stratification by EF. Number of patients in each subgroup is indicated.
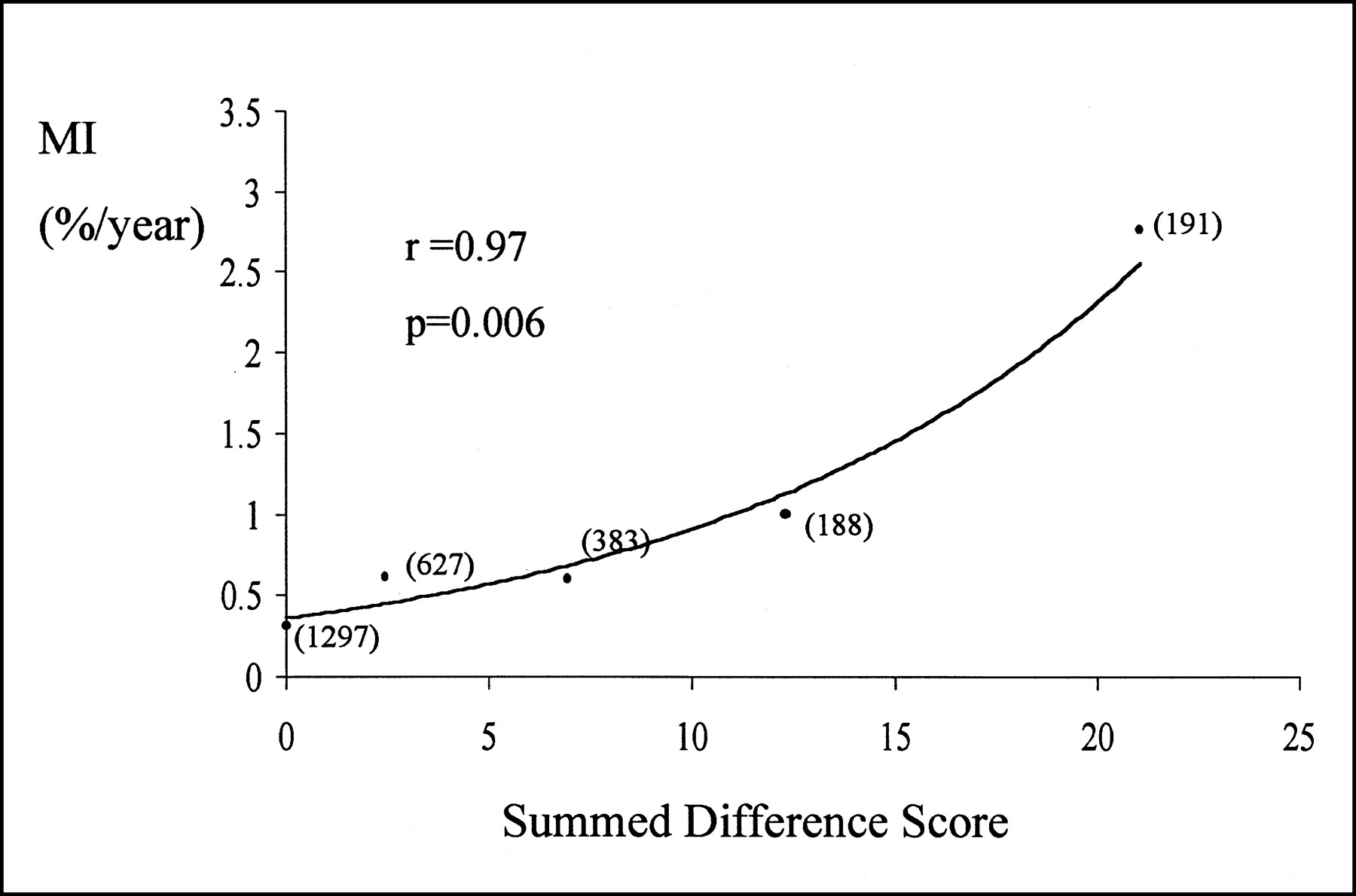
The relationship between the MI rate (%/year) and the SDS (averaged over 5-unit intervals) was also best fit by an exponential curve (y = 0.36 × e0.09x; r = 0.97, P = 0.02) (Fig. 4). Kaplan–Meier analysis showed a significantly higher cumulative hazard for MI in patients with ischemia (SDS, ≥2) compared with patients without ischemia (SDS, <2) (Fig. 5).

Nonfatal MI rate as function of SDS. Number of patients at each 5-unit interval is indicated.

Cumulative hazard of nonfatal MI with stratification by presence or absence of ischemia. Number of patients in each subgroup is indicated.
Perfusion and Function.
Figure 6A illustrates the relationship between the CD rate and the amount of ischemia in patients with normal left ventricular function (EF, ≥50%) and in patients with mild or moderate ventricular dysfunction (EF, 30%–50%). The CD rate increased as a function of the amount of ischemia (P to trend < 0.00001). In the group with no ischemia (SDS, 0–1), the CD rate was <1%/y in patients with normal function as well as in patients with mild or moderate left ventricular dysfunction. Among patients with a large amount of ischemia (SDS, >7), the CD rate was >1%/y in patients with an EF >50% and in patients with an EF between 30% and 50%. Although mortality was higher in patients with an EF of 30%–50% (2.5%/y vs. 1.3%/y), the difference was statistically insignificant. In the group with a mild to moderate amount of ischemia (SDS, 2–7), patients with normal left ventricular function had a very low risk of CD (0.7%/y), whereas patients with mild or moderate dysfunction had a significantly higher CD rate, placing them at the intermediate risk level (2.2%/y; P < 0.05 vs. patients with normal function). Among patients with severe left ventricular dysfunction (EF, <30%), the CD rate was high (>4%/y) regardless of the amount of ischemia (Fig. 6B).
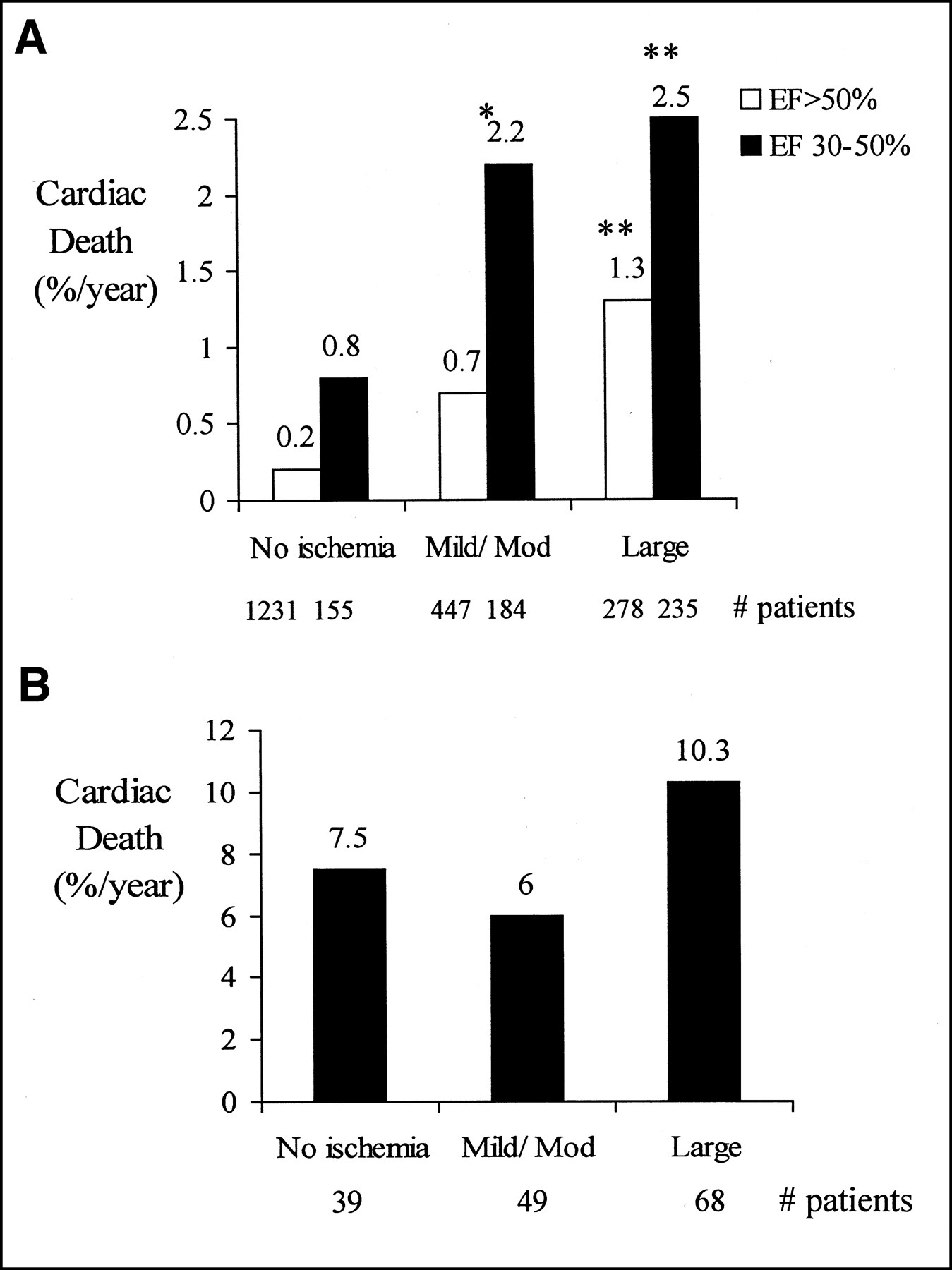
CD rate as function of amount of ischemia in patients with EF >50% and EF between 30% and 50% (A) and in patients with EF <30% (B). Mod = moderate. *P < 0.05 vs. EF >50% in same perfusion category. **P < 0.005 compared with no ischemia and same EF category.
DISCUSSION
This study evaluated the prognostic value of the combined assessment of myocardial perfusion and function in the prediction of ischemia, as measured by the SDS, nonfatal MI, and CD as separate endpoints. We found that after adjustment for prescan information, the best independent predictor of MI was the amount of perfusion defect reversibility, and the best predictor of CD was the poststress EF. The integration of the amount of ischemia and the poststress EF data provided incremental values in risk stratification of patients with an EF ≥30%.
Hachamovitch et al. (5) have shown that the amount of perfusion abnormality at stress is a powerful predictor of both nonfatal MI and CD. Moreover, the specific risk of each of these endpoints can be estimated by the amount of perfusion abnormality. Whereas moderate and severe perfusion abnormality identifies patients at intermediate to high risk of both nonfatal MI and CD, mild perfusion abnormality is related to an intermediate risk of nonfatal MI but very low risk (<1%/y) of CD. We have recently shown that poststress EF by gated perfusion SPECT provides incremental values over the amount of stress perfusion abnormality (6). However, the contribution of perfusion and function data in predicting nonfatal MI and CD as separate endpoints was not assessed in that study because of the relatively small number of MIs during the follow-up period. In this study, the larger patient population and the larger number of hard events allowed for separate evaluation of CD and nonfatal MI. Univariate analysis identified the poststress EF as the most powerful predictor of CD among all prescan, perfusion, and function variables studied. Multivariate analysis showed that after adjusting for prescan data (prescan likelihood of CAD and adenosine stress) the best and independent predictor of CD was the EF. As shown in post-MI patients (13), the relationship between the CD rate and poststress EF was exponential, with a progressive increase in mortality as the EF fell below 50%.
The best predictor of nonfatal MI by univariate and multivariate analysis was the amount of ischemia (SDS). This variable reflects the extent and severity of hemodynamically significant coronary stenoses and the amount of jeopardized myocardium. Although several serial angiographic studies have shown that 60%–70% of all acute coronary syndromes evolve from mildly to moderately obstructive lesions (14,15), significant stenotic lesions progress to total occlusion more frequently than do mild to moderate obstructions, and, at autopsy, coronary thrombosis is more prevalent in severely stenotic plaques (16). In our data the amount of ischemia was an independent predictor of MI after adjustment for the prescan likelihood of CAD, indicating the value of the extent and severity of obstructive coronary disease in predicting MI. The relationship between the MI rate and the SDS was exponential, with an excellent correlation coefficient.
Although the amount of ischemia was a weak and nonindependent predictor of CD in the overall patient population, the SDS improved risk stratification in patients with an EF ≥30%. We found that in these patients cardiac mortality increases as a function of the amount of ischemia, and the integration of perfusion and function improves risk stratification. Patients with no ischemia were at very low risk of CD (<1%/y), and patients with a large amount of ischemia (SDS, >7) had a death rate of >1%/y regardless of their cardiac function. However, patients with a mild or moderate amount of ischemia (SDS, 2–7) could be stratified further to very low risk if they had normal ventricular function and intermediate risk if they had mild to moderate ventricular dysfunction (EF, 30%–50%). Knowledge of the amount of ischemia did not improve risk stratification in patients with severe left ventricular dysfunction (EF, <30%) because these patients had a high mortality rate regardless of the perfusion findings.
Coronary artery bypass surgery has been shown to prolong survival (17–19). In a meta-analysis of randomized trials of coronary artery bypass surgery versus medical management, Yusuf et al. (1) examined the value of a strategy of early bypass surgery versus initial medical therapy with delayed surgery for advanced symptoms. These investigators showed a beneficial effect on survival for early bypass surgery at 5 y, which extended over 10 y. Subgroup analysis showed that the benefit was most pronounced in patients with more extensive coronary disease or ischemia and in patients at intermediate risk (cardiac mortality = 2%–3%/y with medical therapy) or high risk (>4%/y) on the basis of clinical and angiographic data. Left ventricular dysfunction (EF, <50%) was also associated with a beneficial effect for the early bypass surgery strategy. In low-risk patients (cardiac mortality, <1%/y), a nonsignificant trend toward greater mortality with bypass surgery was evident. The beneficial effect of bypass surgery on survival was not associated with increased relative benefits of the procedure itself but, rather, with an increased absolute benefit in patients at higher baseline risk of CD. Therefore, stratification of patients into risk levels and improving the identification of those at intermediate and high risk of CD might be valuable in applying the results of these large-scale studies to individual patient management.
Medical therapy has been shown to reduce the rate of ischemic events and CD in selected patient groups (20–23). Trials that compared initial coronary angioplasty strategy with medical therapy in non–high-risk patients with angiographically documented CAD failed to show a beneficial effect for an initial invasive strategy with respect to long-term survival and prevention of nonfatal MI (2,24,25). The Coronary Angioplasty Versus Medical Therapy for Angina (RITA-2) trial (25) showed a significant excess in mortality and nonfatal MI for an initial coronary angioplasty strategy compared with conventional medical therapy. Aggressive lipid lowering has been shown recently to be associated with a significantly lower ischemic event rate and a significant delay in the time to first ischemic event compared with catheter-based revascularization (2). Thus, it would appear that patients at low risk of CD might benefit more from initial medical therapy and delayed revascularization (if necessary) than from an early revascularization strategy.
In this study, we showed that the relationship between perfusion and function data, derived from gated myocardial perfusion SPECT, can be useful in stratifying patients into low, intermediate, and high risk of CD (Fig. 7). According to this risk stratification, patients are initially categorized into 2 groups: those with an EF ≥30% and those with an EF <30%. Patients with an EF ≥30% are further classified into 3 subgroups: (a) patients with a large amount of ischemia (SDS, >7), who are at intermediate or higher risk of CD and, therefore, might benefit from an early revascularization strategy; (b) patients with no evidence of ischemia on perfusion imaging, who have very low risk of CD and, therefore, might benefit more from initial medical therapy; and (c) patients with a moderate amount of ischemia (SDS, 2–7), in whom risk assessment might be improved by further stratification into those with normal ventricular function (EF, >50%), who are at low risk of CD, and those with mild or moderate ventricular dysfunction (EF, 30%–50%), who are at intermediate risk. Aggressive medical therapy might be preferred in the former subgroup, whereas early invasive strategy, in conjunction with medical therapy, should be considered in the latter subgroup. Because cardiac mortality in patients with an EF <30% is high even in the absence of ischemia, these patients should be considered for evaluation of stress-induced ischemia and myocardial viability as well as early revascularization when inducible ischemia or a large amount of viable myocardium is identified (26).
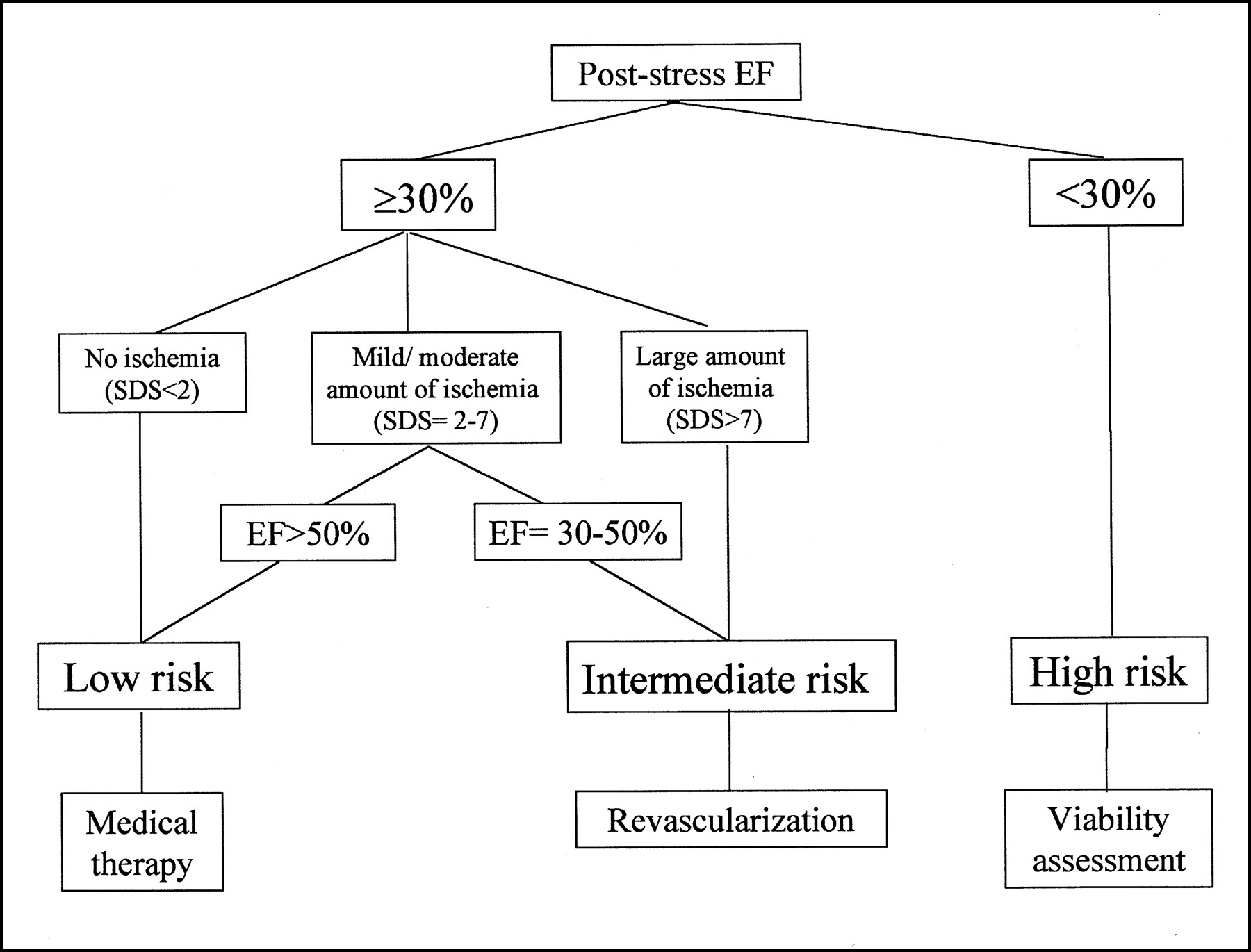
Risk stratification by poststress EF and amount of stress-induced ischemia.
The risk stratification provided in this study is based on integrating the amount of stress-induced ischemia and the poststress EF, acquired from gated myocardial perfusion SPECT. Ventricular function assessed during the first hour after stress incorporates information on baseline as well as poststress cardiac function. Johnson et al. (27) showed that patients with reversible stress perfusion defects frequently had poststress (exercise or adenosine) stunning. We have shown that poststress stunning is a marker of severe angiographic coronary disease (28). Therefore, the prognostic value of poststress EF may not be attributed solely to baseline ventricular dysfunction but may also be attributed to transient worsening of ventricular function in patients with stress-induced ischemia and extensive coronary disease. Resting EF, obtained using a 1- or 2-d 99mTc-sestamibi nongated stress gated rest protocol, is not likely to be influenced by stress-induced ischemia and does not reflect poststress stunning. Therefore, the resting EF may not be as strong a predictor of CD or MI.
CONCLUSION
This study showed that, after adjustment for prescan information, the amount of ischemia was the best predictor of nonfatal MI, and the poststress EF was the best predictor of CD. The amount of ischemia and the left ventricular functional status ought to be integrated to improve stratification of patients into low, intermediate, and high risk of CD and can assist in determining the appropriate treatment strategy for the individual patient.
Acknowledgments
Various nuclear medicine hardware and software manufacturers have an agreement with Cedars-Sinai Medical Center, through which the Medical Center receives royalties based on the distribution of the quantitative gated SPECT software. A portion of these royalties is shared by the algorithm developers.
Footnotes
Received Oct. 5, 2000; revision accepted Jan. 24, 2001.
For correspondence or reprints contact: Daniel S. Berman, MD, Department of Imaging, Cedars-Sinai Medical Center, 8700 Beverly Blvd., Rm. A041, Los Angeles, CA 90048-1865.
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Appropriate Use Criteria for PET Myocardial Perfusion Imaging
- Prognostic Value of Combined Clinical and Myocardial Perfusion Imaging Data Using Machine Learning
- Diagnostic Performance of 3D Bulls Eye Display of SPECT and Coronary CTA Fusion
- Risk stratification using gated stress myocardial perfusion imaging: comparison between patients with and without sexual dysfunction
- Transient Ischemic Dilation in Patients With Diabetes Mellitus: Prognostic Value and Effect on Clinical Outcome After Coronary Revascularization
- Impact of Appropriate Use on the Prognostic Value of Single-Photon Emission Computed Tomography Myocardial Perfusion Imaging
- SNMMI/ASNC/SCCT Guideline for Cardiac SPECT/CT and PET/CT 1.0
- Association Between Aortic Valve Calcification and Myocardial Ischemia, Especially in Asymptomatic Patients
- Coronary Calcium Score as an Adjunct to Nuclear Myocardial Perfusion Imaging for Risk Stratification Before Noncardiac Surgery
- Semiconductor Detectors Allow Low-Dose-Low-Dose 1-Day SPECT Myocardial Perfusion Imaging
- Improved Near-Term Coronary Artery Disease Risk Classification With Gated Stress Myocardial Perfusion SPECT
- Predictive Value of Multislice Computed Tomography Variables of Atherosclerosis for Ischemia on Stress-Rest Single-Photon Emission Computed Tomography
- The Present State of Coronary Computed Tomography Angiography: A Process in Evolution
- Prediction of New-Onset Refractory Congestive Heart Failure Using Gated Myocardial Perfusion SPECT Imaging in Patients With Known or Suspected Coronary Artery Disease: Subanalysis of the J-ACCESS Database
- Prognostic Value of Myocardial Infarct Size and Contractile Reserve Using Magnetic Resonance Imaging
- Are Shades of Gray Prognostically Useful in Reporting Myocardial Perfusion Single-Photon Emission Computed Tomography?
- Stress/Rest Myocardial Perfusion Abnormalities by Gated SPECT: Still the Best Predictor of Cardiac Events in Stable Ischemic Heart Disease
- Single-Photon Emission Computed Tomography Myocardial Perfusion Defects Are Associated With an Increased Risk of All-Cause Death, Cardiovascular Death, and Sudden Cardiac Death
- Gated Myocardial Perfusion SPECT: Algorithm-Specific Influence of Reorientation on Calculation of Left Ventricular Volumes and Ejection Fraction
- Assessment of the Influence of Atrial Fibrillation on Gated SPECT Perfusion Data by Comparison with Simultaneously Acquired Nongated SPECT Data
- Role of non-invasive imaging in the management of coronary artery disease: an assessment of likely change over the next 10 years. A report from the British Cardiovascular Society Working Group
- Roles of Nuclear Cardiology, Cardiac Computed Tomography, and Cardiac Magnetic Resonance: Noninvasive Risk Stratification and a Conceptual Framework for the Selection of Noninvasive Imaging Tests in Patients with Known or Suspected Coronary Artery Disease
- Risk Stratification With Electrocardiographic-Gated Dobutamine Stress Technetium-99m Sestamibi Single-Photon Emission Tomographic Imaging: Value of Heart Rate Response and Assessment of Left Ventricular Function
- Prognostic Value of Lung Sestamibi Uptake in Myocardial Perfusion Imaging of Patients With Known or Suspected Coronary Artery Disease
- Radionuclide-Based Insights into the Pathophysiology of Ischemic Heart Disease: Beyond Diagnosis
- Prognostic Value of Automated Quantification of 99mTc-Sestamibi Myocardial Perfusion Imaging
- Prediction of Death and Nonfatal Myocardial Infarction in High-Risk Patients: A Comparison Between the Duke Treadmill Score, Peak Exercise Radionuclide Angiography, and SPECT Perfusion Imaging
- Gated Myocardial Perfusion SPECT: Basic Principles, Technical Aspects, and Clinical Applications
- The Additive Value of Combined Assessment of Myocardial Perfusion and Ventricular Function Studies
- Prognostic implications of atrial fibrillation in patients undergoing myocardial perfusion single-photon emission computed tomography
- Assessment of prognosis in chronic coronary artery disease
- The Diagnostic and Prognostic Value of ECG-Gated SPECT Myocardial Perfusion Imaging
- Risk stratification using stress myocardial perfusion imaging: don't neglect the value of clinical variables
- Technetium99msestamibi myocardial perfusion imaging predicts clinical outcome in the community outpatient setting: The Nuclear Utility in the Community (NUC) Study
- Transient ischemic dilation ratio of the left ventricle is a significant predictor of future cardiac events in patients with otherwise normal myocardial perfusion SPECT
- Is there a referral bias againstcatheterization of patients withreduced left ventricular ejection fraction?: Influence of ejection fraction and inducible ischemia onpost-single-photon emission computed tomographymanagement of patients without a history of coronary artery disease
- ACC/AHA/ASNC Guidelines for the Clinical Use of Cardiac Radionuclide Imaging--Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (ACC/AHA/ASNC Committee to Revise the 1995 Guidelines for the Clinical Use of Cardiac Radionuclide Imaging)
- ACC/AHA/ASNC Guidelines for the Clinical Use of Cardiac Radionuclide Imaging--Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (ACC/AHA/ASNC Committee to Revise the 1995 Guidelines for the Clinical Use of Cardiac Radionuclide Imaging)
- Prognostic Value of Combined Assessment of Regional Left Ventricular Function and Myocardial Perfusion by Dobutamine and Rest Gated SPECT in Patients with Uncomplicated Acute Myocardial Infarction
- Prognostic Impact of Hemodynamic Response to Adenosine in Patients Older Than Age 55 Years Undergoing Vasodilator Stress Myocardial Perfusion Study
- Adenosine myocardial perfusion single-photon emission computed tomography in women compared with men: Impact of diabetes mellitus on incremental prognostic value and effect on patient management
- Preoperative Risk Stratification Using Stress Myocardial Perfusion Scintigraphy with Electrocardiographic Gating