


Abstract
Although there are several 99mTc perfusion tracers introduced for clinical use, there are no data available directly comparing these tracers with microsphere-determined flow. The aim of this study was to compare the myocardial retention of sestamibi, tetrofosmin, and Q12 in a porcine model. Methods: We used a pig model with (n = 6) or without (n = 3) coronary occlusion. Each pig received a simultaneous injection of sestamibi and either tetrofosmin (group 1, n = 5) or Q12 (group 2, n = 4) labeled with either 99mTc or 95mTc (physical half-life, 61 d; photon energy, 204 keV) during pharmacologic vasodilation. Absolute myocardial retention of each tracer was calculated from the myocardial tracer activity and arterial input function. Results: The plot of all three tracers versus flow achieved a plateau at a higher flow range. However, sestamibi showed a higher mean retention than either tetrofosmin (group 1, 0.27 ± 0.11 vs. 0.16 ± 0.06 mL/g/min, respectively; P < 0.01) or Q12 (group 2, 0.32 ± 0.13 vs. 0.09 ± 0.03 mL/g/min, respectively; P < 0.01). Furthermore, when a linear regression analysis was performed to assess the relationship between retention and microsphere-determined flow, sestamibi showed a greater increment in retention than did tetrofosmin or Q12. Conclusion: Although all of the tracers showed a nonlinear increase in retention as flow increased, sestamibi may display more favorable characteristics as a flow tracer in the porcine heart.
For two decades, stress 201Tl myocardial perfusion imaging has been widely used for the evaluation of coronary artery disease (CAD). Despite its excellent physiologic characteristics, however, the low photon energy as well as relatively long physical half-life poses limitations. Therefore, efforts have been made to develop new myocardial perfusion tracers that can be labeled with 99mTc. To date, several 99mTc-labeled perfusion agents have been introduced as an alternative to conventional 201Tl (1–3).
99mTc-sestamibi, a lipophilic cationic tracer, is currently the most widely used 99mTc perfusion tracer in the clinical setting. The diagnostic utility of 99mTc-sestamibi for CAD assessment as well as for risk stratification has been well described in the literature (4,5). Recently, two other 99mTc- labeled tracers (i.e., 99mTc-tetrofosmin and 99mTc-Q12) have been proposed for clinical use (2,3). Although both tracers have physiologic characteristics similar to 99mTc-sestamibi (i.e., long myocardial retention and no significant redistribution over time), no investigations have simultaneously compared the characteristics of these 99mTc tracers in assessing myocardial blood flow.
The aim of this study was to directly compare the myocardial retention of sestamibi, tetrofosmin, and Q12 against myocardial blood flow in a porcine model. To resolve the difficulties when comparing technetium tracers in the same animals, we used 95mTc (physical half-life, 61 d; photon energy, 204 keV) (6) as a radionuclide to be compared with conventional 99mTc, which allows for simultaneous administration of the tracers.
MATERIALS AND METHODS
Production of 95mTc
95mTc was produced, along with other technetium isotopes (94mTc, 94Tc, 95Tc, and 96Tc), by the irradiation of natural molybdenum by 20 MeV protons on a cyclotron in a manner similar to one previously described (7–9). After 50 d, allowing for decay of other technetium isotopes, the comparatively long half-life of 95mTc was obtained with a high purity. The activity proved to be >99% 95mTcO4− as shown by high-performance liquid chromatography (HPLC). The sterility and pyrogenicity tests of the 95mTcO4− assured us that we were in the same pharmaceutical position as one would be before introducing generator-derived 99mTcO4−.
Radiopharmaceutical Preparation
Sestamibi was supplied by DuPont Pharma Radiopharmaceuticals (Bad Homburg, Germany) in a commercially available kit. Each vial was reconstituted with 99mTcO4− or 95mTcO4− in 3 mL saline. The vial was then shaken, and complete reaction of the complex was achieved at 100°C for 10 min by incubating the vial in boiling water. The preparation was completed after a 15-min period to allow the vial to cool to room temperature.
Tetrofosmin was supplied by Amersham International (Braunschweig, Germany). Each vial was reconstituted with 99mTcO4− or 95mTcO4− in 4–8 mL saline. The vial was shaken gently and incubated for 15 min at room temperature.
Q12 (furifosmin) was provided by Mallinckrodt Radiopharma Gmbh (Hennef, Germany). Each vial was supplied with 99mTcO4− or 95mTcO4− in 3 mL saline. The vial was then shaken, and complete reaction of the complex was achieved at 100°C for 20 min by incubating the vial in boiling water, followed by a 15-min period to allow the vial to cool to room temperature. The preparation and quality control of Q12 were performed in a manner similar to one previously described (10).
The radiochemical purity of each sample was assessed by HPLC, and only a purity of >90% was considered acceptable quality for use.
Experimental Preparation
Eleven domestic pigs (weight range, 22–29 kg; mean weight, 25 kg) were anesthetized with sodium pentobarbital (30 mg/kg of body weight). The pigs were intubated and ventilated with room air. A peripheral catheter was inserted for the administration of fluids as necessary and for subsequent dipyridamole infusion. Both femoral arteries were catheterized for arterial blood sampling and for arterial blood pressure monitoring. The heart was then exposed by means of a left thoracotomy and suspended in a peripheral cradle. A left atrial catheter was inserted through the left atrial appendage for microsphere and isotope injection. In six pigs, the midportion of the left anterior descending artery was dissected free of the pericardium and a snare placed loosely around it for subsequent occlusion. Two pigs died during the experimental procedure because of sustained ventricular fibrillation; the remaining nine pigs were included in the study. All experiments were performed with the approval of the institutional committee for animal research in compliance with the position of the American Heart Association on use of research animals.
Experimental Protocols
Figure 1 illustrates the experimental procedure. After stabilization, 0.57 mg/kg dipyridamole was infused intravenously for 4 min. In two pigs, low-dose dobutamine (10 μg/kg/min) was also infused to further increase myocardial blood flow. At the end of the infusion, the left anterior descending artery was occluded by the snare. After 6 min, approximately 1 million microspheres, with a mean size of 15 μm in diameter (113Sn), sestamibi and tetrofosmin (group 1) or Q12 (group 2) labeled with either 99mTc (150 μCi) or 95mTc (60 μCi) were simultaneously injected into the left atrium. The blood samples for technetium agents were obtained from the same site for blood pressure monitoring by switching the output at the time of tracer administration. Arterial input function was determined by serial arterial blood sampling for 5 min in a manner similar to that for PET studies (11). For microspheres, a withdrawal pump was used for blood sampling at a constant rate of 12.7 mL/min (12). At the end of blood sampling, the pigs were killed by injection of a saturated solution of potassium chloride. The heart was then excised immediately. Atrial, right ventricular, and connective tissues were trimmed away. The left ventricle was cut along the short axis into slices 1 cm thick, and each sample was weighed. Tissue samples usually weighed between 0.5 and 1.5 g. Activity in myocardial and blood samples was measured using a multichannel well counter. The photo energy peaks were centered for 99mTc (140 keV), 95mTc (204 keV), and 113Sn (392 keV) with a 20% window. Blood and tissue samples were counted immediately after the study. A computer program corrected for spillover of radioactive counts into the counting window of other tracers.
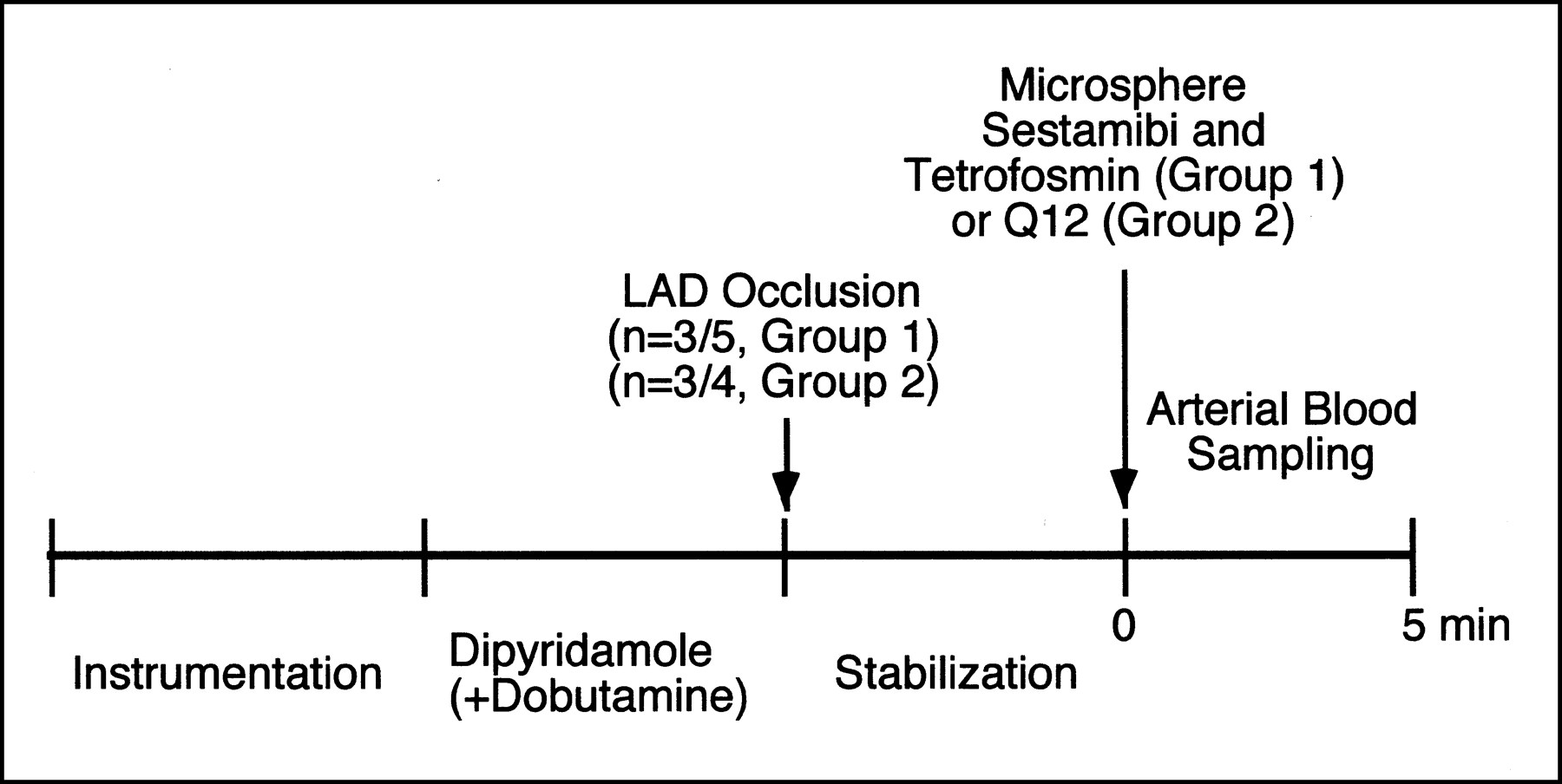
Experimental procedures. LAD = left descending coronary artery.
Data Analysis
Measurement of Myocardial Blood Flow.
Myocardial blood flow (MBF, mL/g/min) was determined using the microsphere technique (13):
 where Ct is the activity in the myocardial tissue sample (cpm/g), Fw is the reference withdrawal rate of the blood flow pump, and Ab is the activity in the entire reference blood sample (cpm).
where Ct is the activity in the myocardial tissue sample (cpm/g), Fw is the reference withdrawal rate of the blood flow pump, and Ab is the activity in the entire reference blood sample (cpm).
Measurement of Absolute Tracer Retention.
Absolute myocardial tracer retention was calculated for each tissue sample in a manner previously described (14) as follows:
 where R is the retention (mL/min/g) of the tracer, Ct is the radioactivity of the tracer in the myocardium (cpm/g), Cb is the arterial radioactivity concentration (cpm/mL), and ∫0tCb(γ)d(γ) is the time-integral of Cb.
where R is the retention (mL/min/g) of the tracer, Ct is the radioactivity of the tracer in the myocardium (cpm/g), Cb is the arterial radioactivity concentration (cpm/mL), and ∫0tCb(γ)d(γ) is the time-integral of Cb.
Statistical Analysis
Data were reported as mean ± 1 SD. Differences between mean values within a group were compared using a paired t test. A linear regression analysis was performed to assess the relationship between the retention and microsphere-determined flow for the low (≤1.0 mL/g/min) and high (>1.0 mL/g/min) flow range. We also tested whether the slopes from sestamibi and either tetrofosmin or Q12 are different by the null hypothesis that the slopes are identical. P < 0.05 was considered significant.
RESULTS
Hemodynamic Recordings
Hemodynamic parameters were obtained at baseline and at the time of tracer and microsphere administration. Complete hemodynamic data were available for seven of nine pigs; in the remaining two pigs, arterial blood pressure after dipyridamole infusion could not be measured because of technical reasons. In the pigs with dipyridamole infusion alone, the mean systolic pressure and heart rate were 110 ± 16 mm Hg and 80 ± 8 bpm at baseline and were 82 ± 24 mm Hg and 97 ± 12 bpm at the time of tracer administration. In the two pigs with dipyridamole and low-dose dobutamine infusion, the mean systolic pressure and heart rate were 110 ± 21 mm Hg and 78 ± 9 bpm at baseline and were 94 ± 43 mm Hg and 165 ± 9 bpm at the time of tracer administration.
Absolute Tracer Retention Versus Myocardial Blood Flow
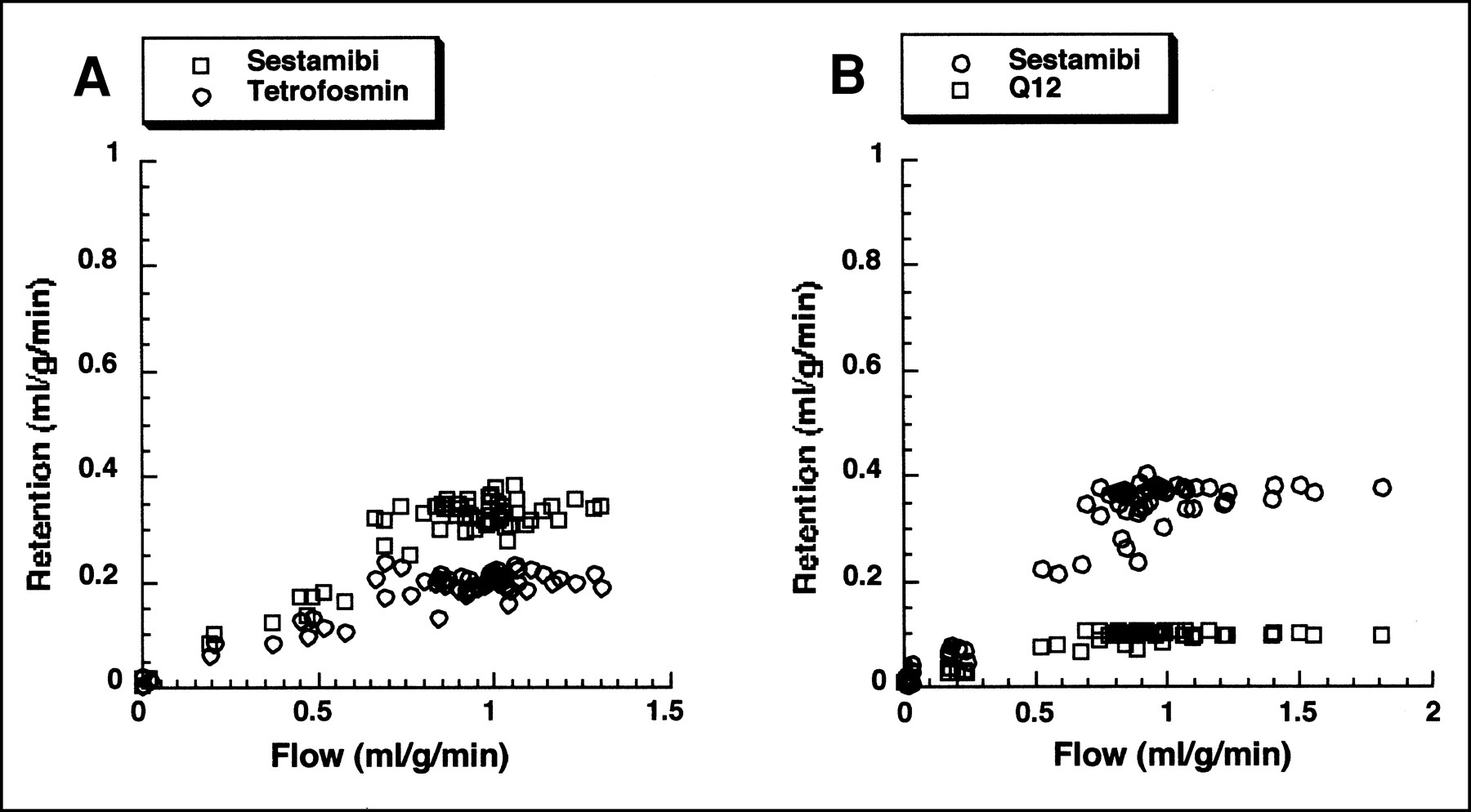
Figure 2 displays examples of representative relationships between absolute tracer retention versus microsphere-determined flow in groups 1 and 2. The plot of all the tracers versus flow achieved a plateau at a higher flow range. However, sestamibi consistently had a higher tracer retention compared with tetrofosmin or Q12.
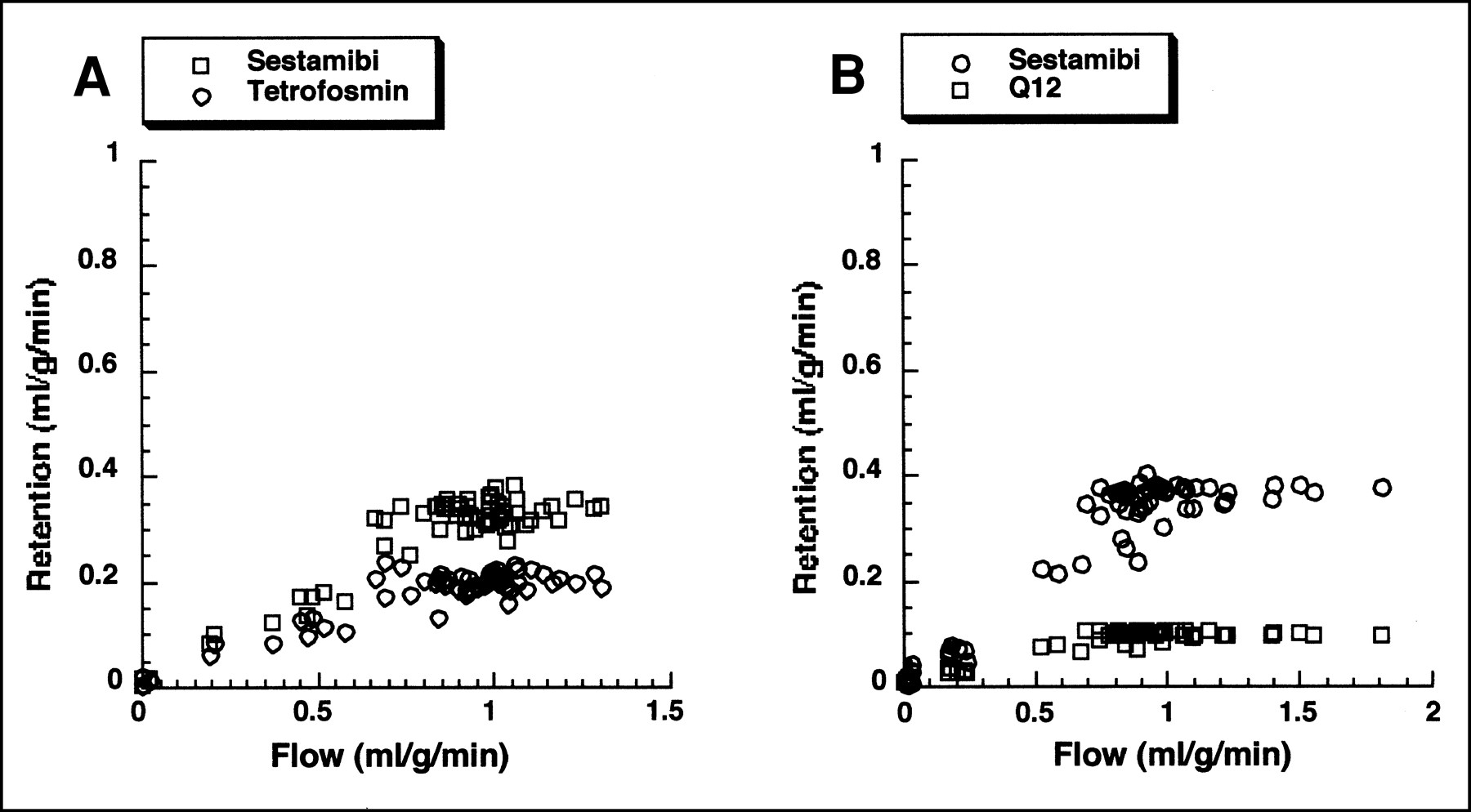
Example of absolute myocardial retention of sestamibi and tetrofosmin plotted against microsphere-determined flow (A), and example of absolute myocardial retention of sestamibi and Q12 plotted against microsphere-determined flow (B).
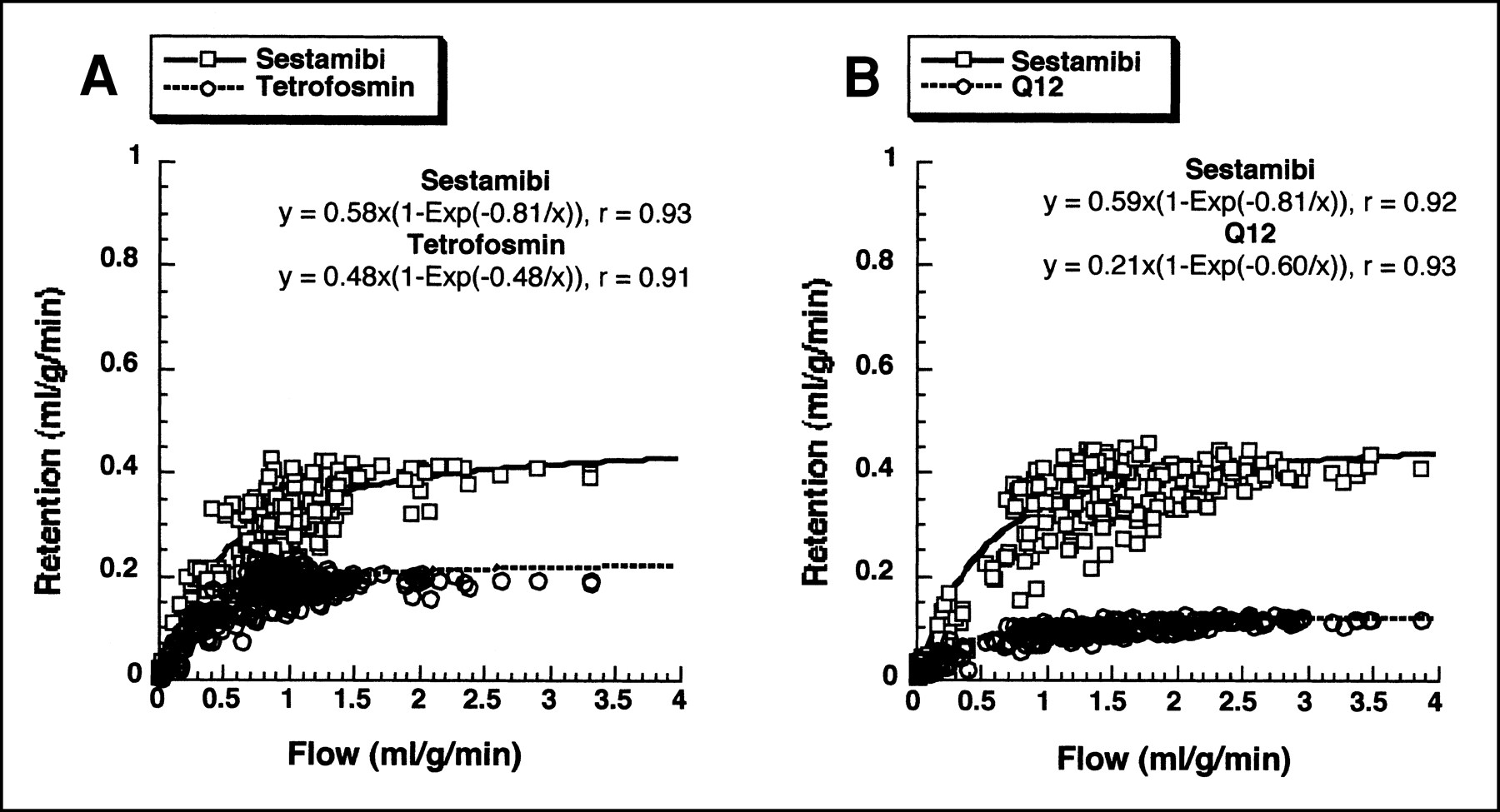
Because the absolute retention is determined by tissue activity concentration and arterial input function and thus intrinsically normalizes the variability in flow ranges achieved in individual pigs, we combined the data obtained from all the pigs in each group. Figure 3 summarizes the relationship between absolute tracer retention versus microsphere-determined flow in each group. In group 1, although neither sestamibi nor tetrofosmin showed an increase in retention in direct proportion to flow, sestamibi had a significantly higher mean absolute retention than did tetrofosmin (0.27 ± 0.11 vs. 0.16 ± 0.06 mL/g/min, respectively; P < 0.001). When the curve for retention versus blood flow for each tracer was fitted to a nonlinear function as previously described (14,15), sestamibi yielded a function of y = 0.58 × (1 − e−0.81/x), r = 0.93, whereas tetrofosmin yielded a function of y = 0.47 × (1 − e−0.48/x), r = 0.91. In a manner similar to the results obtained from the pigs in group 1, the mean sestamibi retention was significantly higher than Q12 retention (0.32 ± 0.13 vs. 0.09 ± 0.03 mL/min/g, respectively; P < 0.001). The nonlinear fitting for sestamibi retention (y = 0.59 × (1 − e−0.81/x), r = 0.92) in group 2 yielded a function nearly identical to that obtained in group 1, whereas Q12 yielded a function of y = 0.21 × (1 − e−0.60/x), r = 0.93.

Absolute myocardial retention of sestamibi and tetrofosmin plotted against microsphere-determined flow for group 1 pigs (A), and that of sestamibi and Q12 for group 2 pigs (B).
When a linear regression analysis of tracer retention versus flow was performed for the low (≤1.0 mL/g/min) and high (>1.0 mL/g/min) flow ranges, the slope for sestamibi was greater than that for tetrofosmin for both low flow and high flow in group 1 (Table 1). In particular, the linear relationship between tracer retention and flow was abolished at the high flow range for tetrofosmin, whereas this was not the case for sestamibi. In group 2, the slope for sestamibi was greater than that for Q12 for the low flow range, and there was a trend for a greater slope for sestamibi compared with Q12 for the high flow range (Table 1). These results indicate a greater increment in retention with sestamibi than with either tetrofosmin or Q12.
Linear Regression Analysis of Retention Vs. Myocardial Blood Flow for Low and High Flow Ranges
DISCUSSION
This study in open-chest anesthetized pigs directly compares for the first time the myocardial retention of sestamibi, tetrofosmin, and Q12 in relation to myocardial blood flow. The major finding of this study was that, although all of the tracers investigated in this study showed a nonlinear increase in retention as flow increased, sestamibi showed a higher mean absolute retention and greater increment in retention against myocardial blood flow than did either tetrofosmin or Q12.
To overcome limitations of 201Tl such as the low photon energy and relatively long physical half-life, several 99mTc perfusion tracers have been developed for clinical use (1–3,16). Among them, 99mTc-teboroxime has gained a limited clinical acceptance because of its rapid washout from the myocardium (17), which precludes high image quality of the heart. Other tracers, such as 99mTc-sestamibi, 99mTc-tetrofosmin, or 99mTc-Q complexes, have much longer myocardial retention characteristics and thus are suitable for SPECT imaging. Unlike 201Tl, these tracers do not show significant redistribution over time.
Although prior experimental studies have shown lower extraction and retention of 99mTc-sestamibi than 201Tl, particularly at high flow ranges (14,18), clinical studies have shown comparable diagnostic performance for the detection of coronary artery disease between 99mTc-sestamibi and 201Tl (1,19), likely because of better image quality with 99mTc-sestamibi. Similar results have been reported for both tetrofosmin and Q12 (2,3). It should be noted, however, that both 99mTc-sestamibi (20) and 99mTc-tetrofosmin (21) have been shown to reveal smaller defects than 201Tl during exercise stress, but not at rest, which suggests that such lower retention between 99mTc and 201Tl, rather than differences in physical characteristics, may account for the differences in myocardial tracer distribution. Because all three tracers investigated in this study can be labeled with the same radionuclide, that is, 99mTc, the image quality of these agents should essentially be similar. In this regard, the relationship between the tracer retention and myocardial blood flow becomes even more important to define which agent has more favorable characteristics as a flow tracer.
Absolute tissue retention of a tracer represents its ability to accumulate in the tissue as a function of delivery to the tissue. An ideal myocardial flow tracer would be one with high myocardial extraction and retention that are maintained throughout the wide range of blood flow, such as that encountered during pharmacologic vasodilation or dynamic exercise stress. Although interpretation of conventional SPECT images mainly relies on heterogeneity of tracer retention achieved between normal and abnormal regions, the knowledge of absolute retention of a tracer allows for more comprehensive understanding of the tracer characteristics than relative parameters and, further, may represent an important issue in future when attempting quantitation of myocardial blood flow using SPECT techniques (22,23).
As is the case for all extractable perfusion tracers, none of the tracers investigated in this study showed an increase in retention in direct proportion to flow, especially at high flow rates. This is consistent with prior experimental studies, all of which have shown a plateau effect of tracer extraction at high flow rates. However, the results showed that sestamibi had a significantly higher absolute retention and greater increments in retention than either tetrofosmin or Q12, indicating the more favorable retention characteristics of sestamibi as a flow tracer.
Although one study showed the retention of sestamibi to be higher than that of Q12 in the isolated perfused rat heart (24), there are few experimental data available comparing technetium-labeled perfusion tracers against myocardial blood flow. Using a coinjection technique that is similar to the one used in this study, Di Rocco et al. (25) found higher retention of teboroxime than sestamibi. Their results, together with the current data, suggest that the retention of tetrofosmin or Q12 would be lower than that of teboroxime or 201Tl. In a study by Meleca et al. (26) that compared seven perfusion tracers (201Tl and six technetium-labeled tracers) in canine hearts, sestamibi did not show the more favorable uptake characteristics as a flow tracer compared with tetrofosmin or Q12, which does not agree with our results. This may, at least partially, stem from technical differences used in this study, in which two tracers (i.e., sestamibi and either tetrofosmin or Q12) were simultaneously injected in the same animals, allowing a head-to-head comparison of the agents.
Although clinical studies using 99mTc perfusion tracers have shown diagnostic accuracy comparable with that of 201Tl, a study by He et al. (27) reported that the sensitivity of dipyridamole stress 99mTc-tetrofosmin SPECT for the detection of individual coronary stenoses was only 53%. This may partially be explained by the relatively low tracer retention especially at the high flow range observed in this study. There are few clinical data available in the literature directly comparing the 99mTc perfusion tracers for the detection of CAD. Studies comparing 99mTc-sestamibi and 99mTc-tetrofosmin distribution during dipyridamole or exercise stress have shown that the tracer distribution is, in general, similar (28,29). However, this is contradicted by a recent study (30) showing more extensive and severe defects detected with sestamibi than with tetrofosmin when the detection of mild to moderate coronary stenosis is of clinical concern. Thus, it still remains unclear which agent provides more favorable results when it is used to assess CAD. To date, no direct comparison has been made for 99mTc-sestamibi versus 99mTc-Q12. Although the direct applicability of the results in the porcine heart to a clinical setting remains uncertain, the results would suggest a theoretic advantage of sestamibi over either tetrofosmin or Q12 as a flow tracer.
We used 95mTc as a radionuclide to be compared with 99mTc in this study. A benefit of this approach is that sestamibi and either tetrofosmin or Q12 were simultaneously injected, permitting direct comparison of the tracer retention characteristics in the same animals.
In this study, data from different animals were combined because retention values are determined by arterial input function and tissue activity concentration, which normalize the variability in flow range achieved in individual animals. Similar approaches have also been used in experimental PET studies (11,31). The combined absolute retention data fitted well a nonlinear function for both group 1 and group 2. Furthermore, the parameters for nonlinear fitting of sestamibi data were nearly identical for both groups, indicating that the model used in this study gives logical and reproducible results.
The study has several noteworthy limitations. First, we used a low-dose dobutamine infusion in addition to dipyridamole to boost myocardial blood flow in two pigs, which may have influenced the results. An animal study by Calnon et al. (32) showed that dobutamine infusion may affect myocardial uptake of sestamibi. Nevertheless, the higher retention of sestamibi compared with tetrofosmin or Q12 was consistently observed regardless of whether dobutamine was infused. Thus, it is not likely that the use of low-dose dobutamine infusion significantly altered our results.
Second, we did not attempt to directly compare 99mTc-tetrofosmin with 99mTc-Q12, although 99mTc-tetrofosmin appeared to have a higher retention than did 99mTc-Q12 (Figs. 2 and 3). This limitation could have been resolved using the triple-isotope technique (e.g., 99mTc, 96Tc, and 95mTc). However, the results of this study showed that 99mTc-sestamibi has more favorable retention characteristics as a flow tracer than either 99mTc-tetrofosmin or 99mTc-Q12.
Third, we did not assess the timing of data acquisition after tracer injection in this study. It has been shown that 99mTc-sestamibi may redistribute to some degree (33). In contrast, to date there are no published data supporting the presence of redistribution with 99mTc-tetrofosmin (34) or 99mTc-Q12 (10). It is uncertain, therefore, whether the superiority of 99mTc-sestamibi, which has a slower hepatic clearance of the tracer than tetrofosmin or Q12, observed in this study remains unchanged if the data acquisition is substantially delayed. This needs to be addressed in further studies.
Finally, a very high blood flow rate (e.g., 5–7 mL/g/min) was not achieved in the current study even with catecholamine in addition to dipyridamole to boost myocardial blood flow. However, it is unlikely that the retention–flow relationship, which already plateaued at the flow range achieved in this study, would show further changes at higher flow rates.
CONCLUSION
The results indicate that, although all of the 99mTc tracers tested in this study showed a nonlinear increase in retention in proportion to flow, sestamibi may display more favorable characteristics as a flow tracer compared with tetrofosmin or Q12 in the porcine model.
Footnotes
Received Sept. 28, 2000; revision accepted Jan. 4, 2001.
For correspondence or reprints contact: Ichiro Matsunari, MD, The Medical and Pharmacological Research Center Foundation, Wo32, Inoyama-town, Hakui-city, Ishikawa, 925-0613, Japan.




{kind=link}
{kind=link}
{kind=link}