


Abstract
To determine whether hemodynamic parameters are changed by upright posture in healthy middle-aged humans, absolute values of regional cerebral blood flow (rCBF) were investigated for three different orthostatic conditions. Methods: PET with [15O]H2O and arterial blood sampling were performed on eight middle-aged healthy volunteers while they were sitting passively or standing actively. Absolute rCBF values estimated by the autoradiographic method in regions of interest were compared using ANOVA, and relative changes in rCBF were also analyzed voxel by voxel using statistical parametric mapping (SPM). Results: Physiologic data remained unchanged for different conditions. ANOVA and SPM showed that absolute and relative rCBF levels were significantly elevated in the cerebellar vermis in the standing position compared with those in the supine and sitting positions. In contrast, ANOVA showed that rCBF in the frontal and parietal cortices tended to be lower in the sitting and standing positions than in the supine position. Regression analysis showed that the frontal rCBF measured during standing tended to be inversely correlated with age. Conclusion: The results showed that cerebellar vermis activation was more marked in the standing position than in the sitting or supine positions, indicating that the vermis is a neural substrate for controlling voluntary upright posture. Brain perfusion in the distal internal carotid artery region may be subject to orthostatic postural changes in healthy middle-aged humans.
Cerebral perfusion in humans is maintained chiefly by cerebrovascular autoregulation (1), which is considered to function effectively within a wide range of perfusion pressures. In some diseases, long-lasting arterial hypertension shifts the upper and lower thresholds for autoregulation upward on the pressure scale (2,3). In contrast, patients with autonomic failure show a reduction in the lower limit of autoregulation (4). In the normal state, however, autoregulation in the human brain is sustained regionally (5,6) and postural changes are assumed to alter regional cerebral blood flow (rCBF). Previous imaging studies of cerebral perfusion under orthostatic stress conditions in humans showed a significant or mild reduction in relative rCBF in the frontal lobe of healthy humans using SPECT with 133Xe gas (7,8) or with a lipophilic perfusion tracer, 99m-labeled hexamethylpropyleneamine oxime (9,10). Therefore, whether orthostatic challenge or upright posture can reduce or raise rCBF substantially in specific brain regions in healthy humans remains unclear.
Alterations in cerebral hemodynamics during orthostatic stress by a head-up maneuver have been studied using a transcranial Doppler method measuring velocity in the large cerebral artery (11–13). In healthy volunteers with their head up, a mild reduction in mean velocity in the middle cerebral artery has been shown, along with a mild or negligible change in mean arterial blood pressure. Although the change in flow velocity does not necessarily imply a change in rCBF in brain tissue, the reduction in flow velocity in the specific cerebral artery was consistent with the SPECT finding of a reduction in rCBF in the frontal region. The regional differences in this relative rCBF change under orthostatic conditions was confirmed by our previous mapping study using PET with [15O]H2O (14). That study showed, in the anterior cerebellum and the visual cortex, a significant increase in rCBF relative to the global cerebral blood flow change during bipedal standing, along with no evidence of rCBF elevation in the frontal lobe.
Quantitative measurement of cerebral blood flow in upright positions (sitting and standing) allowed us to examine the neural substrate for postural control as well as regional susceptibility (specifically in the distal internal carotid artery region, i.e., frontal and parietal areas) to head-up conditions. This study was performed to clarify these issues using PET with [15O]H2O.
MATERIALS AND METHODS
Subjects
Eight healthy volunteers (6 men, 2 women; mean age ± SD, 56.4 ± 10.8 y) participated. None was receiving medication, and none had neurologic or cardiac problems such as hypertension, diabetes, or peripheral vascular disease, as assessed through a questionnaire on individual clinical history and through analyses of peripheral blood obtained before the PET examination. This study was approved by the ethics committee of the Hamamatsu Medical Center, and written informed consent was obtained from all participants after the nature and possible risks of the experiment had been explained.
Postural Conditions and Physiology
Three conditions were used in this study. A volunteer lay supine on a scanner bed with eyes open and looking forward (condition A). Subsequently, the volunteer sat passively on the scanner bed, which was tilted at an angle of 75°, with the body bent at the waist and with eyes open and looking forward (condition B). Then, the volunteer stood with feet together and eyes open and looking forward (condition C). In all conditions, the left arm, with a catheter inserted into the brachial artery, was supported by an arm rest positioned at the height of the heart. As physiologic parameters, arterial blood pressure, heart rate, partial pressure of arterial carbon dioxide (Paco2), and pH were monitored during each PET measurement.
Arterial Blood Sampling Procedure
Arterial blood was extracted automatically using a coincidence counter system (BACC-2; Hamamatsu Photonics K.K., Hamamatsu, Japan) to continuously measure arterial blood radioactivity. The system consisted of a coincidence counter, a signal processor (CNT-24-4(98)E; Contec, Tokyo, Japan), a personal computer (PC9821 Xc200; NEC, Tokyo, Japan), and a peristaltic pump (Perista Biominipump, model AC-2120; Atto Corp., Tokyo, Japan). The coincidence counter has a detector unit with a pair of bismuth germanate scintillation crystals and a position-sensitive photomultiplier tube. The detector electronics showed that the coincidence time window was 100 ns, the energy window was set >300 keV, and the dwell time per sample (minimum, 1 s) and the number of samples (maximum, 5,000 samples) were entered through the computer, allowing us to measure arterial blood radioactivity at 1-s intervals for >80 min.
PET and MRI Procedure
PET was performed using a high-resolution scanner (SHR2400; Hamamatsu Photonics, Hamakita, Japan) with a spatial resolution of 2.7 mm (full width at half maximum) transaxially and 5.5 mm axially and with an 80-mm axial field of view (15). This PET system had a mobile gantry that enabled vertical movement (up to 165 cm from the bottom) and tilting (−20° to +90°). This small axial field of view obliged us to predetermine the scanning area required for each PET study using a midsagittal MR image acquired with a 0.3-T static-magnet MRI system (MRP-7000AD; Hitachi Medical Corp., Tokyo, Japan) and three-dimensional mode (14,16). Through tilting of the PET gantry parallel to the intercommissural line determined on the MR image, the axial field of view could cover the area from the lower part of the superior frontal gyrus to the upper half of the cerebellum. After backprojection and filtering (Hanning filter; cutoff frequency, 0.2 cycles per pixel), image resolution was 6.0 × 6.0 × 6.5 mm full width at half maximum. The voxel of each reconstructed image measured 1.45 × 1.45 × 8 mm.
After fixation of the subject’s head to the urethane head holder using a specially made thermoplastic face mask, a 20-min transmission scan was obtained with the subject supine. With three-directional laser beams marking face sites three-dimensionally, and with the tilt system of the PET gantry, we could fixate the subject’s head in the same position as for the transmission scan during sitting or standing. For 120-s dynamic emission scans (10 s × 12 frames), individuals received a 600-MBq bolus of [15O]H2O through the right cubital vein using an automated injector. After injection, arterial blood was continuously withdrawn through the left brachial artery using the automated arterial blood γ-ray coincidence counter described above, yielding arterial input data per second. After completion of two emission scans with the subject supine (condition A), the head holder was temporarily removed from the receiver attached to the gantry and the subject sat on the scanner bed, which was tilted at an angle of 75° (condition B). Two consecutive sitting-position scans coupled with arterial sampling using the automated γ-ray coincidence counter were followed by the next two quantitative scans, in which the position of the gantry was lifted and tilted optimally for each volunteer’s head height during standing (condition C). The order of conditions was counterbalanced except for condition A: A-A-B-B-C-C or A-A-C-C-B-B. Because the head position was marked three-dimensionally with lasers attached to the gantry in these three conditions, the head position was satisfactorily realigned to that during the first scan (14). During the intervals between standing-position scans, the subjects were released temporarily from head fixation to the gantry and allowed to rest on a chair. During PET scans, each subject continued to assume sitting or standing postures for approximately 5 min in total. If reconstructed images created just after each emission scan were distorted, indicating a location error, the rCBF image was discarded and imaging was performed again after a recheck of head position.
Region-of-Interest Methods and Statistics
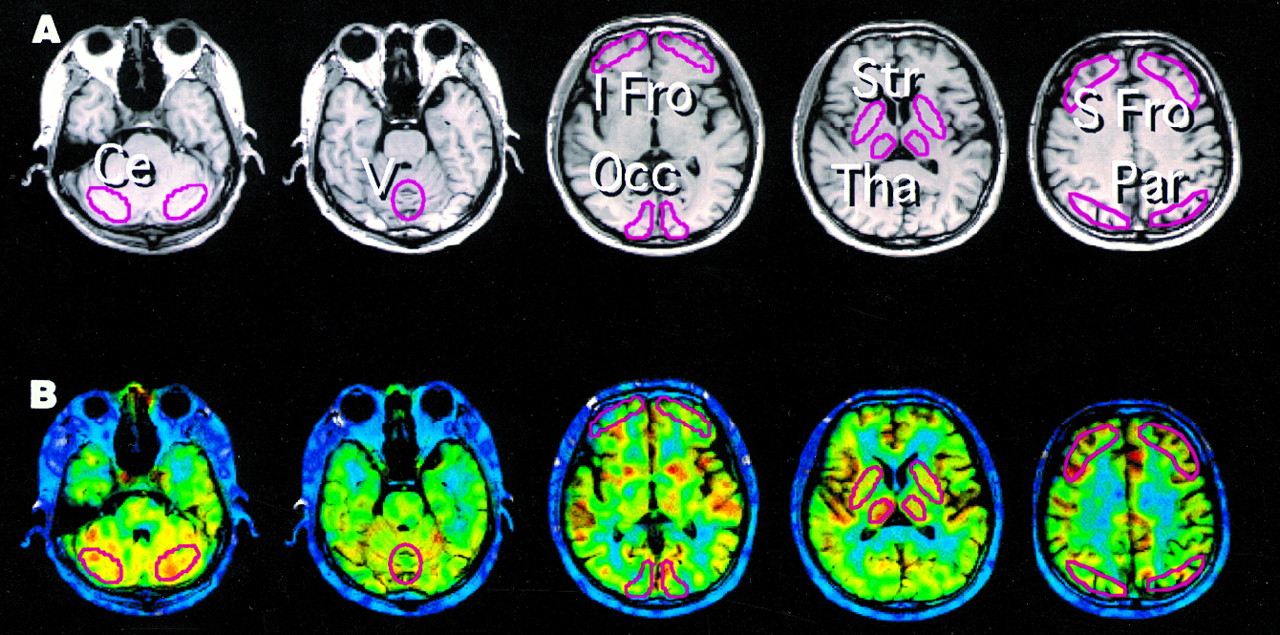
Irregular regions of interest (ROIs) were drawn bilaterally over the lateral hemispheres of the posterior cerebellar cortex; cerebellar vermis; lower frontal (orbitofrontal) cortex (Brodmann’s area, or BA: 10, 11); upper frontal (prefrontal) cortex (BA: 6, 8); temporal (BA: 21, 22), parietal (BA: 7), and occipital (BA: 17, 18) cortices; striatum; and thalamus on the MR images according to the Atlas of the Human Brain (17) (Fig. 1). After ROIs were drawn parallel to the intercommissural plane on the MR images, PET images were displayed side by side together with the MR images using an image processing system (Dr View; Asahi Kasei Co., Tokyo, Japan) (16) on a HyperSPARC ss-20 workstation (Sun Microsystems, Palo Alto, CA), which enabled us to place the ROIs automatically on the same area on both the MR image and the corresponding PET image (18). By adjusting the time axes of the arterial and PET time–activity curves, we could base the estimation of quantitative rCBF on the autoradiographic method (19). To investigate differences in arterial input functions under each condition, we compared dose-corrected integral areas calculated as percentage dose per liter from the time of [15O]H2O injection to the end of scanning among the three conditions using an unpaired Student t test. Statistical analysis for rCBF was first performed using two-way ANOVA with a posthoc Scheffé F test with respect to brain region and study condition (supine, sitting, or standing). Because no cross-interactions were observed in the two-way ANOVA between the two factors (P = 0.8671), one-way ANOVA was performed to compare rCBF effects in each brain area separately. Because posthoc multiple comparisons were performed in both analyses, P < 0.05 was taken to indicate statistical significance.

ROI setting. Irregular ROIs, drawn on concerned regions of MR images (A), were placed on corresponding PET images (B) superimposed on MR images. Ce = cerebellum; I Fro = inferior frontal; Occ = occipital cortex; Par = parietal; S Fro = superior frontal; Str = striatum; Tha = thalamus; V = vermis.
Voxel-Based Mapping Method
To investigate relative changes in rCBF among the three conditions voxel by voxel in the whole brain, we used statistical parametric mapping (SPM) software (SPM96; Wellcome Department of Cognitive Neurology, London, U.K.) implemented in MATLAB (The MathWorks, Inc., Natick, MA) on a HyperSPARC ss-20 workstation. The effect of variance caused by global cerebral blood flow was removed using analysis of covariance with the global flow normalized to 50 mL/100 g/min. This process generated normalized mean rCBF values on a voxel-by-voxel basis for each condition. Adjusted mean rCBF in a specific condition was compared with that in the supine position on a voxel-by-voxel basis with t statistics. The resultant set of voxel values for each contrast constituted a t statistic (SPMt), which was then transformed to a unit normal distribution (SPMz) map (20). We report here significant activation areas consisting of clusters of voxels that had the peak height P < 0.05, with a correction for multiple comparison.
RESULTS
Physiologic Parameters and Arterial Input Functions
No significant differences were seen in arterial BP, Paco2, or arterial pH measured just before PET scanning in the first study in each condition (P > 0.05, unpaired t test) (Table 1). These stable physiologic parameters were further supported by the calculated areas integrated under the arterial input curves showing no differences among the three conditions (Table 1). No clinical symptoms such as hyperventilation or reduced consciousness were observed during orthostatic conditions in any of the participants.
Physiologic Data and Integrals of Arterial Input Functions in Three Conditions
Absolute rCBF Changes in Upright Positions (ROI Analysis)
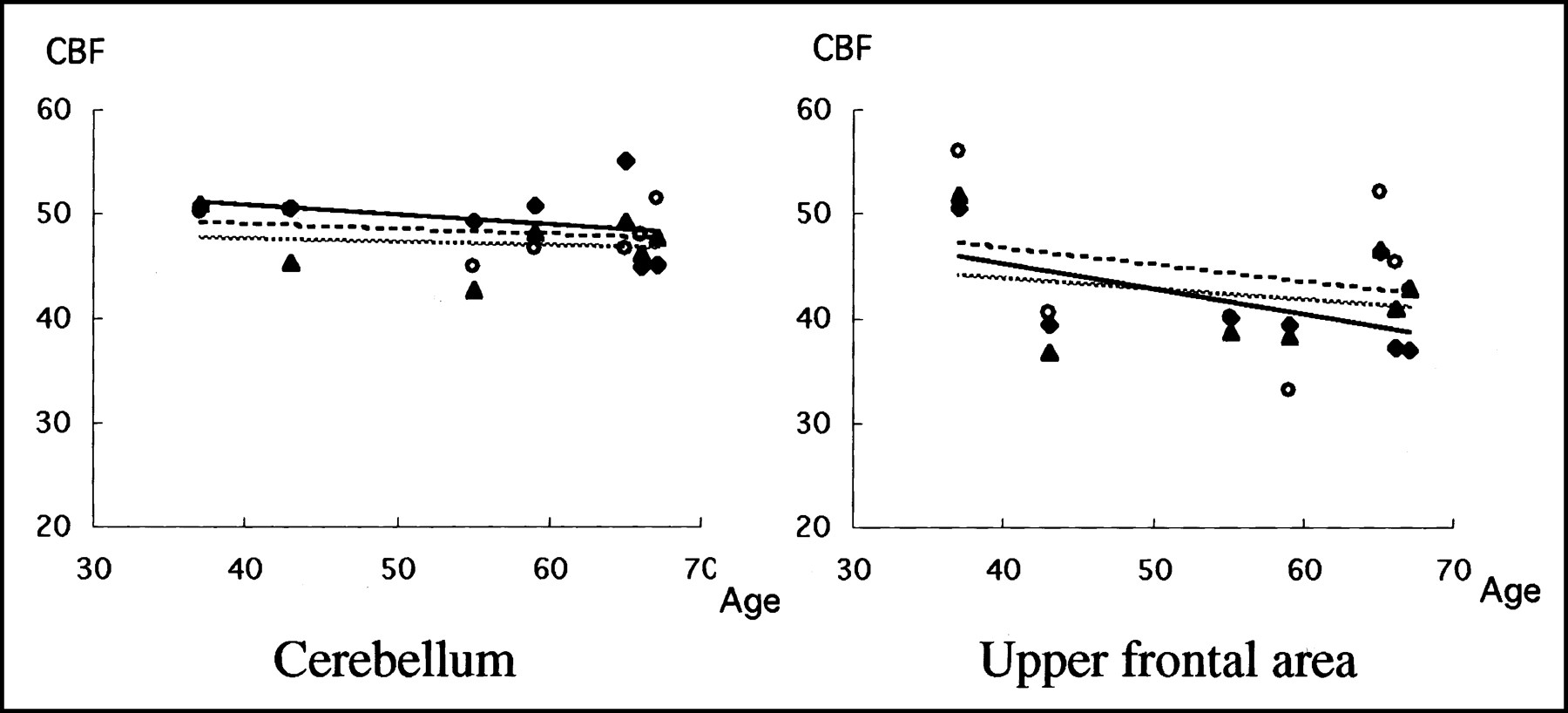
The absolute rCBF value in the cerebellar vermis was significantly higher in the standing position than in the supine or sitting positions (P < 0.05, ANOVA) (Table 2). No significant elevation in rCBF was found in the basal ganglia or thalamus. In the sitting position, rCBF levels tended to be low globally compared with rCBF in the supine position, except in the cerebellar vermis. Slight reductions in rCBF were observed in the frontal and parietal cortices in the upright positions. Regression analysis showed that rCBF during standing tended to be inversely correlated with age in the upper frontal cortex (Fig. 2). No other brain regions disclosed a larger value for the regression coefficient than the value in the upper frontal cortex, possibly because the study participants were few and had a relatively narrow age range.

Correlations between age and rCBF in different postures in cerebellum (supine, r = 0.13; sitting, r = 0.26; standing, r = 0.43) and upper frontal area (supine, r = 0.25; sitting, r = 0.23; standing, r = 0.55). Absolute levels of upper frontal rCBF in standing position tended to decrease with age. CBF = cerebral blood flow; ○ with dashed line = supine; ▴ with dotted line = sitting; ♦ with solid line = standing.
Changes in rCBF (mL/100 g/min) Under Different Postural Conditions
Relative rCBF Increase in Upright Positions (SPM Analysis)
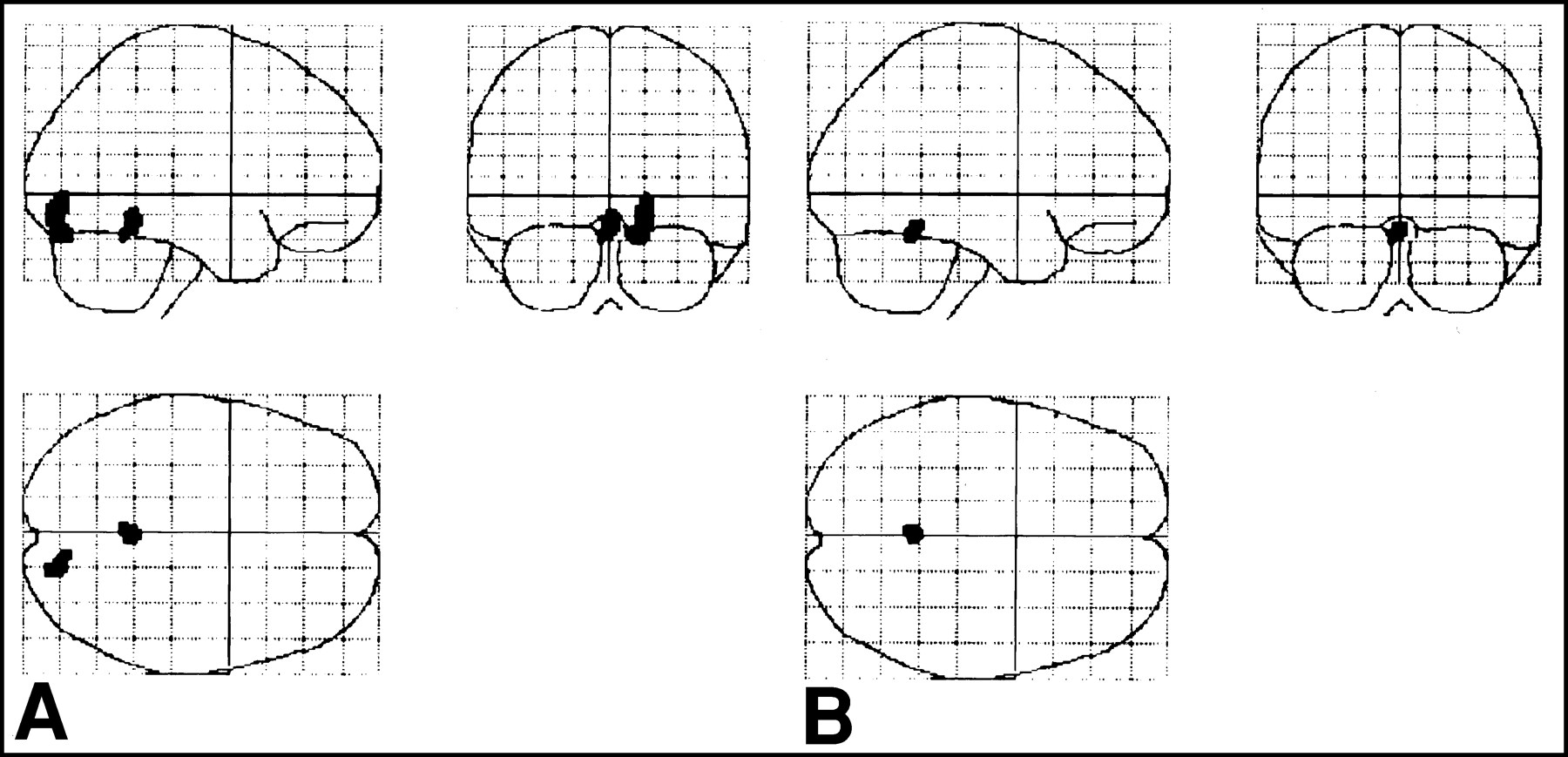
Comparison of standing with supine positions showed significant rCBF increases in the cerebellar anterior vermis and in the right lingual and inferior occipital gyri (BA: 17, 18) (Table 3; Fig. 3A). Compared with the sitting position, the standing position increased rCBF significantly in the cerebellar anterior vermis (Table 3; Fig. 3B). No significant differences were found in rCBF between the supine and the sitting positions.
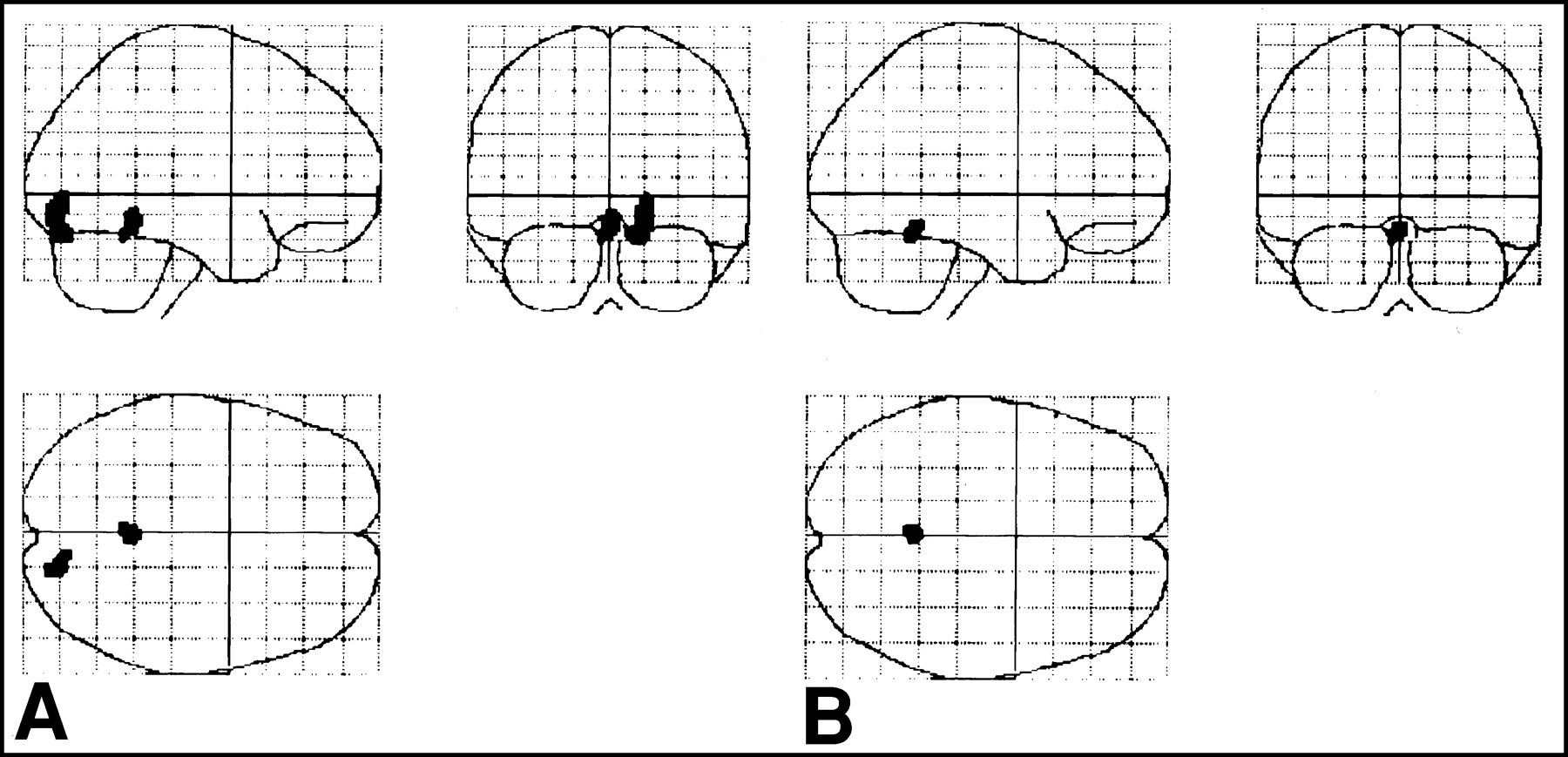
(A) Standing position versus supine position. Significant increase in relative rCBF is detected in anterior vermis and visual cortex. (B) Standing position versus sitting position. Significant increase in rCBF is still detected in anterior vermis. Details of coordinates and z values are given in Table 3.
Coordinates and z Scores for Significant Activation in Standing Position Compared with Supine and Sitting Positions
DISCUSSION
To our knowledge, this study was the first to investigate absolute values of brain perfusion in specific areas with the assuming of orthostatic postures in humans. Before interpreting the results, we carefully considered the methodologic limitations of this study. First, as discussed in our previous study (14), it was difficult to predict to what extent participants depended on fixation of the head during upright postures. Head fixation might contribute to emotional activation, resulting in alterations of physiologic parameters or cerebral blood flow levels. However, the physiologic data in this study showed that the basic tone of physiology was almost the same among the different postural conditions. The stability of physiologic data during PET measurement was confirmed by the similarities in the patterns of arterial input functions in each condition. Second, the short axial field of view of our PET scanner was insufficient to cover the whole brain, forcing us to exclude the region of the brain that covers the primary somatosensory foot area. The primary somatosensory foot area may be involved in postural control, because a cat was reported to be able to walk even after resection of its cerebellum (21) and because, anatomically, the efferent fibers from the cerebellar nuclei project to the contralateral primary motor area (22). This possibility was also supported by our previous human SPECT study showing significant activation in the foot area during walking (23). Third, the current PET study, unlike transcranial Doppler studies, could not measure rapid hemodynamic changes on a real-time basis in response to an orthostatic behavioral shift. This finding indicated that rCBF estimated in this study was a value for a hemodynamically equilibrated condition of the adopted posture. A recent orthostatic stress study using transcranial Doppler combined with near-infrared spectroscopy showed that the levels of physiologic parameters, including heart rate, systemic blood pressure, and oxyhemoglobin and deoxyhemoglobin concentration, plateaued 3 min after an orthostatic postural change from the supine to the standing position (24). Because emission scans after head fixation in orthostatic conditions were performed >5 min after postural change in this study, the results were considered to reflect stable hemodynamics in orthostatic conditions.
This study showed a significant increase in the absolute value of rCBF in the cerebellar anterior vermis during standing but not during passive sitting. In addition, the absolute rCBF level in the occipital cortex covering primary and secondary visual areas tended to be higher when subjects were standing than when they were supine or passively sitting. Pathophysiologic studies showed that medial cerebellar lesions caused deterioration of balance and gait, whereas lateral cerebellar lesions impaired motor coordination in the distal extremities in humans (25,26). As postulated in the previous standing-posture PET study (14), the vermis activation observed only during standing in the current study indicated that the cerebellar anterior vermis plays a crucial role in maintaining a voluntary upright posture in humans. We had also speculated that visual activation without macroscopic eye saccade movement during standing in that study might have been partially caused by stereopsis, because stereoscopic processing requires activation of BA 18 in the right hemisphere (27). Further significant vermis activation in standing versus sitting illustrated by SPM (Fig. 3B) was in line with the results of a previous study indicating that sitting required less attention and less integration of sensory inputs than standing (28). Because rCBF did not significantly differ between the supine and the sitting positions in this study, reclining on the 75° tilted bed might have been insufficient to induce neuronal activation in the postural control system in healthy subjects.
In contrast, quantitative rCBF levels appeared to be globally lower in the sitting position. This finding agreed with the results of a previous orthostatic stress study showing a mild reduction in the mean velocity of the middle cerebral artery along with a slight elevation in the deoxyhemoglobin level during the 80° head-up condition in healthy subjects (24). Because spatial memory performance was reported to be affected by postural condition (standing or sitting voluntarily) (29), the basal brain function and brain physiology during standing may differ from those in the supine position or in involuntary orthostatic conditions such as reclining.
Upright postures may affect regional hemodynamics in the frontal and parietal areas, because a small but consistent reduction in absolute rCBF value was found during sitting and standing in this study. This finding was supported by previous 133Xe SPECT studies showing a significant reduction in relative rCBF in the frontal area during a 70° head-up tilt under normocapnic conditions (7,8). Because our physiologic data showed no significant changes in respiratory or blood pressure parameters in the upright positions, this rCBF reduction was unlikely to be caused exclusively by metabolic or cardiovascular effects on autoregulation, which may be impaired in several diseases with orthostatic hypotension (30–32). The mechanism of this frontal and parietal rCBF reduction during standing remains to be established. However, the result of correlation analysis in this study, showing a tendency toward an age-related reduction in frontal rCBF during standing, suggested that vascular resistance, possibly caused by age-related arteriosclerotic changes, may affect the range of autoregulation in the distal internal carotid artery region. This hypothesis is supported by a previous report that the autoregulatory responses of arterioles, albeit not cerebral arterioles, were reduced in an axial gradient–dependent manner (33).
CONCLUSION
We identified absolute increases in rCBF in the cerebellar vermis and a tendency toward persistent reduction in absolute rCBF in the distal internal carotid artery region during standing in healthy middle-aged humans. The latter finding may be hemodynamically important for understanding brain physiology during standing in elderly individuals, because stroke is one reason for deterioration of the standing posture in the aged population (34,35).
Acknowledgments
The authors thank Dr. Tatsuo Torizuka and Toshihiko Kanno for their cooperation.
Footnotes
Received Jul. 31, 2000; revision accepted Dec. 20, 2000.
For correspondence or reprints contact: Yasuomi Ouchi, MD, PhD, Positron Medical Center, Hamamatsu Medical Center, 5000 Hirakuchi, Hamakita 434-0041, Japan.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Health and productivity at work: which active workstation for which benefits: a systematic review
- Patients With Heart Failure With Reduced Ejection Fraction Have Exaggerated Reductions in Cerebral Blood Flow During Upright Posture
- Overview of potential procedural and participant-related confounds for neuroimaging of the resting state
- Brain Activity during Ankle Proprioceptive Stimulation Predicts Balance Performance in Young and Older Adults
- Effects of Brain Amyloid Deposition and Reduced Glucose Metabolism on the Default Mode of Brain Function in Normal Aging
- Regional cerebral glucose metabolism in akinetic catatonia and after remission