


Abstract
This study was designed to evaluate the age dependency of 18F-FDG uptake in the thymus and the frequency of PET confirmation of thymus hyperplasia after chemotherapy in cancer patients. Methods: Whole-body FDG PET recordings of 168 patients were retrospectively examined for a retrosternal lesion in the anterior mediastinum that was attributable to the thymus. The patients were assigned to the following four groups: children with malignant lesions before the first therapy (group Ia; n = 15; mean age ± SD, 11.9 ± 3.7 y), children with malignant disease after chemotherapy (group Ib; n = 12; mean age, 10.3 ± 5.0 y), adults with histologically confirmed malignant lymphoma before the first therapy (group IIa; n = 37; mean age, 43.9 ± 16.7 y), and adult lymphoma patients 3 wk to 4 mo after chemotherapy (group IIb; n = 104; mean age, 40.9 ± 14.6 y). Results: Increased FDG accumulation in the thymus was seen in 11 patients (73%) of group Ia and 9 patients (75%) of group Ib. Thymus hyperplasia was found in 5 patients (5%) of group IIb. The eldest of these 5 patients was 25 y old. No increased FDG accumulation in the thymus was observed in any of the group IIa patients. In cases of visible FDG uptake in the thymus, standardized uptake values did not exceed 4. Conclusion: FDG accumulation in the thymus is a common finding in children and can occasionally be observed in young adults after chemotherapy. Knowledge of the characteristics of a typical retrosternal lesion in conjunction with the clinical history allows avoidance of diagnostic uncertainty and unnecessary procedures.
The occurrence of thymus hyperplasia after successful chemotherapy of malignant diseases is a known phenomenon that is observed particularly among younger patients with testicular carcinoma (1–4) or malignant lymphoma (5–11). With expanding use of CT (2,6–8,12) and scintigraphy with 67Ga (13,14), more of these cases of posttherapeutic thymus hyperplasia are being detected.
In recent years, 18F-FDG PET has grown in importance in the primary diagnosis and course control of malignancies, especially malignant lymphomas. A preliminary report shows visually discernible FDG accumulation in two cases of thymus hyperplasia in adults (15). Usually, physiologic FDG uptake in the thymus disappears in adolescence in accordance with the involution of the thymus (16). This article examines the frequency of PET confirmation of thymus hyperplasia after chemotherapy in cancer patients and the age dependency of thymic FDG uptake.
MATERIALS AND METHODS
Preparation of Patients
All PET scans were routinely obtained for oncologic reasons. Whole-body FDG PET recordings of 168 patients were retrospectively examined for a triangular retrosternal accumulation of moderate intensity in the anterior mediastinum that was attributable to the thymus. The patients were assigned to the following four groups: children with malignant lesions before the first therapy (group Ia; n = 15; mean age ± SD, 11.9 ± 3.7 y) (Table 1), children with malignant disease after chemotherapy (group Ib; n = 12; mean age, 10.3 ± 5.0 y) (Table 2), adults with histologically confirmed malignant Hodgkin’s disease or non-Hodgkin’s lymphoma before the first therapy (group IIa; n = 37; mean age, 43.9 ± 16.7 y), and adult patients with malignant lymphoma 3 wk to 4 mo after chemotherapy (group IIb; n = 104; mean age, 40.9 ± 14.6 y). In addition, one 63-y-old man with known thymus carcinoma was examined under the same PET protocol. For all patients, the diagnoses were confirmed histopathologically.
Thymic FDG Uptake in Children with Malignant Lesions Before First Therapy (Group Ia)
Thymic FDG Uptake in Children with Malignant Disease After Chemotherapy (Group Ib)
Radiopharmaceutical
The isotope and the radiopharmaceutical were produced and synthesized as previously reported (17). After the patients had fasted for 12 h, 5 MBq FDG per kilogram of body weight were injected into a peripheral vein. The administered radioactive dose was calculated for the children according to the recommendations of the European Association of Nuclear Medicine (18). Patients rested during the 90-min uptake period. All patients presented with normal blood sugar values at the time of FDG application. No patient had known diabetes mellitus.
PET Protocol
Static whole-body PET was performed with an ECAT EXACT 921/31 tomograph (Siemens Medical Systems, Hoffman Estates, IL/CTI, Knoxville, TN). This device simultaneously records 31 planes, which encompass a 10.6-cm field of view. The spatial resolution is 6.0 mm full width at half maximum. The scanner is calibrated for activity concentration (kBq/mL). Patients were positioned with the aid of a laser beam and a vacuum support mattress. Beginning 90 min after tracer injection, an emission image and a transmission image (for subsequent photon attenuation correction using an external germanium source) were recorded at each bed position for 9 and 3 min, respectively. Data were corrected for the dead time of the scanner, decay, and photon attenuation. Coronal, sagittal, and transaxial images were produced on the basis of an iterative reconstruction algorithm using ordered-subset expectation maximization and segmented attenuation correction after injection (19,20).
Image Analysis
The images were reviewed on hard copy and on a computer workstation (SunSPARC 20; SUN Microsystems, Palo Alto, CA) linked to the data archiving and processing system commercially supplied by Siemens Medical Systems. The latter enabled the use of multiple operator-defined planes. The PET images were interpreted blindly and independently by two experienced investigators. They did not disagree about the nature of any FDG accumulation in the thymus. For semiquantitative evaluation of thymic FDG uptake, observer-defined regions of interest were outlined around the entire area of suggestive thymic FDG accumulations in transaxial slices. The maximum activity in a selected region of interest was chosen for calculation of standardized uptake value (SUV) (21).
A retrosternal soft-tissue lesion was classified as potentially benign thymic FDG accumulation if there was focally increased radiotracer uptake in a typical triangular shape and if there was an SUV < 4. This cutoff criterion was based on the 90-min uptake period of the radiopharmaceutical (22). Malignancy was suspected if there was focally increased radiotracer uptake retrosternal in any shape except triangular, if there was an SUV > 4, or if both findings were present. The PET findings were compared with the sum of findings of the other staging procedures. CT and MRI were performed according to standard protocols (23). If required, thin-section techniques were applied.
RESULTS
The frequency of a visually discernible FDG accumulation in the thymus has been summarized for the individual patient groups in Table 3. Increased FDG accumulation in the thymus was seen in 11 patients (73%) of group Ia and 9 patients (75%) of group Ib.
Thymic FDG Uptake in Patient Groups
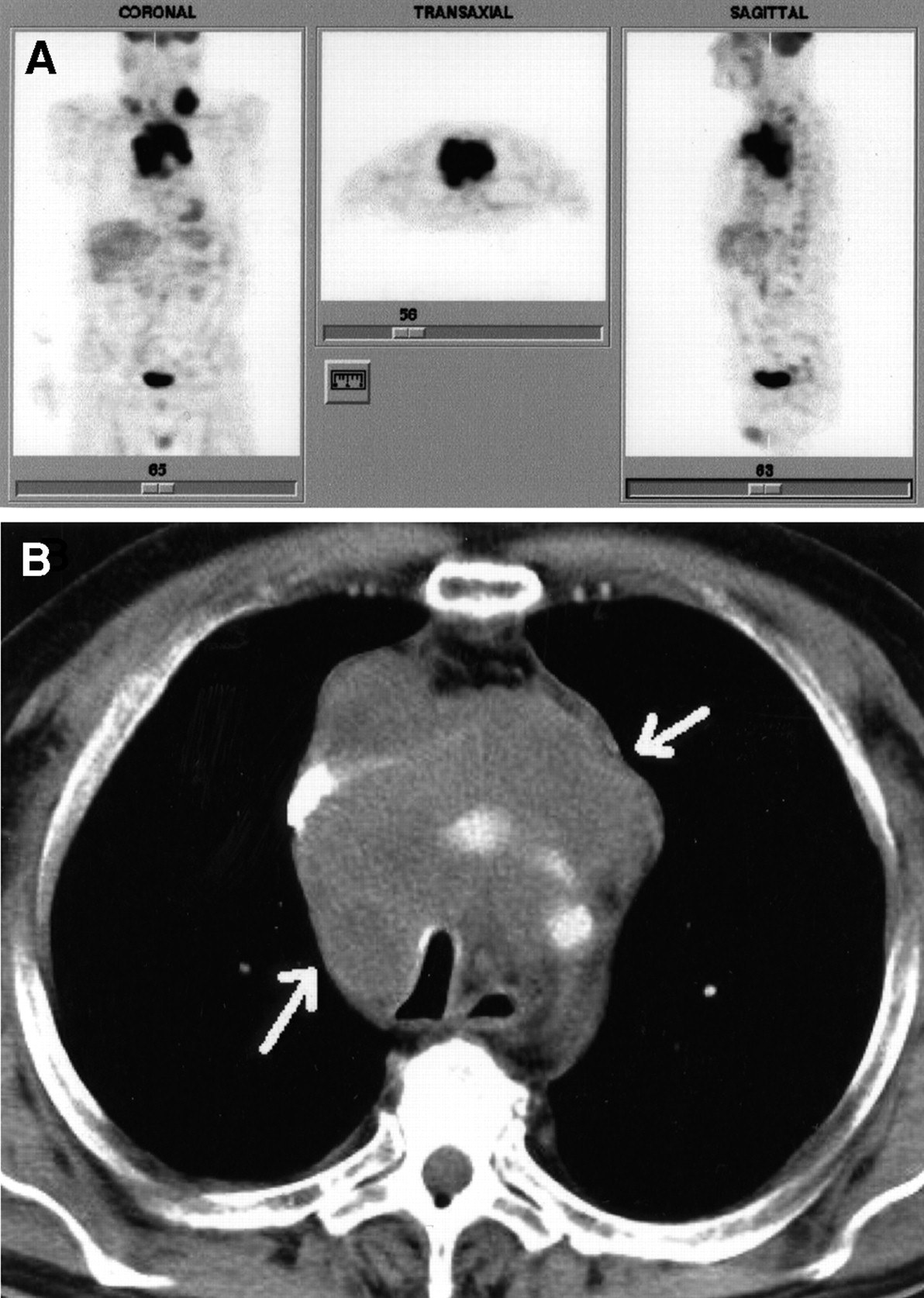
No increased FDG accumulation was observed in the thymus of any group IIa patient. By contrast, the typical triangular FDG accumulation was observed in the thymus of 5 group IIb patients (5%). Figure 1 shows the PET recording of 1 of these 5 patients, of whom the eldest was 25 y old. All 5 patients had been treated under various chemotherapy protocols. The SUV of the visually discernible thymus accumulations was between 0.98 and 3.83 in all groups (Tables 1 and 2). A mean SUV of 1.84 ± 0.68 (n = 11) was calculated for the FDG-positive cases in group Ia, 2.22 ± 0.93 for group Ib (n = 9), and 2.74 ± 0.66 for group IIb (n = 5). No semiquantitative analysis was performed for any patient in group IIa, because FDG accumulation was not evident in the thymus. At the time of PET, additional CT or MRI scans were obtained for 7 of the 21 patients with positive findings (3 in group Ia, 1 in group Ib, and 3 in group IIb). Thymus hyperplasia was confirmed in the 3 adult patients of group IIa, whereas the thymus gland was morphologically normal in all examined children. Clinical follow-up during at least 6 mo did not show any thymic malignancy in the 21 FDG-positive cases.

Thymus hyperplasia images with FDG PET (A) and MRI (B) from 22-y-old woman with Hodgkin’s disease 3 mo after chemotherapy.
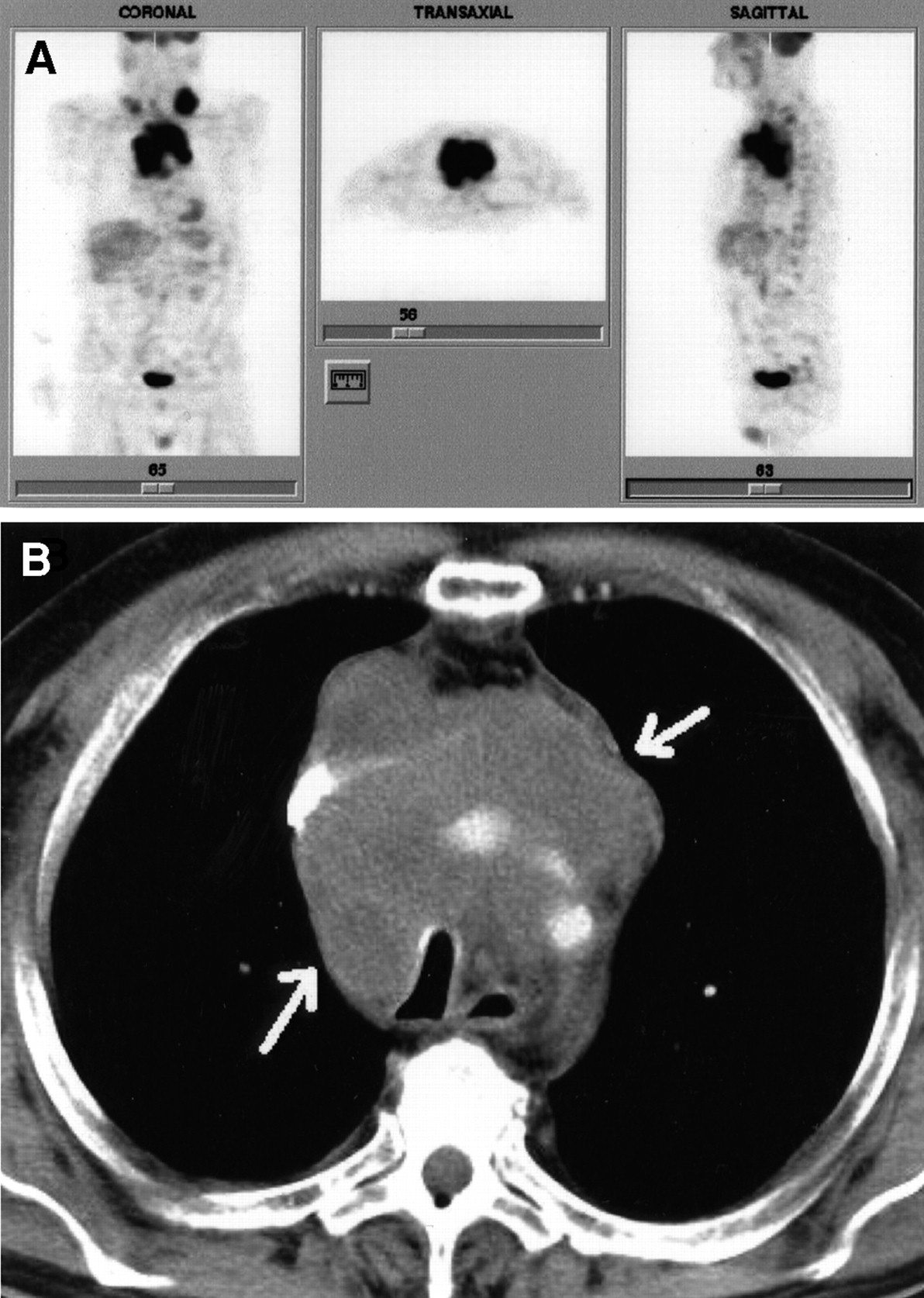
Figure 2 shows the FDG PET image of the 63-y-old man with thymus carcinoma. The extended mediastinal lesion shows a high FDG uptake (SUV, 9.6). The normal shape of the thymus gland has vanished. In addition, a supraclavicular lymph node metastasis on the left side was detected.
A 63-y-old man with thymus carcinoma. (A) FDG PET scan shows mediastinal tumor and supraclavicular lymph node metastasis on left side (physiologic FDG uptake is also seen in urinary bladder). (B) Representative axial CT scan shows that this large retrosternal mass (arrows) surrounds supra-aortic branches.
DISCUSSION
The thymus accumulations examined in this retrospective study were entirely accidental findings. Considering the age of the patients, the case histories, and the typical triangular shape of the retrosternal accumulation, which corresponds to the anatomic bilobed figure of the thymus, the findings could easily be interpreted without further clarification as physiologic accumulation in childhood or as reactive thymus hyperplasia in adults after chemotherapy. Both the higher metabolic activity of the thymus in the first years of life to puberty and the known phenomenon of the occurrence of thymus hyperplasia after chemotherapy were considered.
Information on the frequency of thymus hyperplasia is usually obtained from analysis of small patient groups with varying mean ages using morphologically based radiologic procedures such as CT or MRI. Some individual case reports on malignant lymphoma have been published, but no systematic study on its prevalence. Only Peylan-Ramu et al. (13) have reported on an increased 67Ga uptake after chemotherapy in 10 of 62 patients (16.1%) with malignant non-Hodgkin’s lymphoma. A study by Kissin et al. (24) showed thymus hyperplasia in 14 of 120 patients (11.7%) after chemotherapy of malignant testicular teratomas. This study found increased FDG accumulation in the thymus in only 5% of the lymphoma patients who had received chemotherapy.
Although islands of functional residual tissue can be found in the thymus in histologic studies of patients up to 60 y old (25), reactive thymus hyperplasia is a phenomenon that occurs primarily among younger patients and apparently is independent of tumor entities and chemotherapeutics (7,8,13). The five FDG-positive cases in this study occurred in patients treated according to various therapeutic regimens. The only report of increased FDG accumulation in the thymus of an older person was by Alibazoglu et al. (26), who observed elevated metabolic activity of the thymus in a 54-y-old woman after ablative 131I therapy of follicular thyroid carcinoma. Of interest is that only normal thymus tissue, with no signs of hyperplasia, was found at histologic examination. The pathophysiology of reactive thymus hyperplasia has not yet been completely elucidated. By unanimous agreement, aplasia of the thymus is the initial step, elicited by a steroid-related apoptosis and inhibition of lymphocyte proliferation, such as may be observed not only after chemotherapy but also, for example, after acute infection, stress, intoxication, cortisone, or radiation. In the sense of an immunologic rebound phenomenon, lymph follicles with large nuclear centers and infiltration with plasma cells subsequently develop. In light of the improved immunologic parameters, thymus hyperplasia is generally considered a prognostically favorable phenomenon (24,27).
No significant differences were seen in FDG accumulation in the thymus of children in the groups before or after chemotherapy. The mentioned decrease in FDG accumulation on reaching puberty agrees in both groups. Interestingly, the thymus cannot be visualized in PET recordings in all children younger than 10 y old. The cause of this variability in pediatric thymal FDG accumulation, which was also observed by Patel et al. (16), is unclear. However, both in this study and in the study by Patel et al., children with known malignant disease were examined, not healthy children. The physical and emotional stress attendant on the disease can lead to corticoid release in the adrenal cortex through the mechanisms described above and influence thymus metabolism. The available data indicate that metabolic activity as FDG accumulation can be shown in childhood until the onset of puberty; this finding would correlate with the known immunologic activity of the thymus gland. After chemotherapy, this FDG accumulation cannot be differentiated in childhood from thymus hyperplasia. However, in view of the small number of pediatric cases and the wide variety of malignant tumors, the influence of tumor-specific factors cannot be distinguished from that of age-associated factors.
FDG accumulation in the thymus is suggestive of malignancy if the activity reaches the concentration in the bladder or cerebellum or if the typical triangular shape of the thymus is abolished. Liu et al. (15) were able to differentiate between thymus carcinoma and hyperplasia using semiquantitative analysis. However, the number of patients in that study (n = 12) was low, so that additional studies must be performed for a final evaluation of FDG PET in differentiation of thymus tumors. In addition to biopsy, scintigraphy with somatostatin analogs may be helpful for further clarification, because they have been shown to accumulate in many thymus carcinomas but not in thymus hyperplasias (28).
Thymus carcinomas are only one type of thymus malignancy. Corresponding to the embryonic development of the thymus, in which it is formed from an epithelial structure into which lymphocytic cells migrate at the end of the second fetal month, the thymus tumors that occur are primarily epithelial, lymphocytic, and mixed-cell tumors, in addition to very rare lipomas and sarcomas. Pure lymphocytic thymus tumors are classified as primary or secondary lymphomas. Interestingly, Keller and Castleman (29) reported that thymus involvement can be histologically shown in 48% of mediastinal lymphoma invasion. Because increased FDG accumulation in the thymus could not be shown in any of the 14 untreated lymphoma patients with known mediastinal involvement, the method appears unsuitable for proving the presence of lymphoma. However, this thesis requires further clarification because of the lack of histologic data. Approximately 30%–40% of benign and malignant thymomas are associated with autoimmune diseases, especially with myasthenia gravis. Increased homogeneous uptake of FDG in myasthenia gravis–related thymomas has been described (15). Therefore, patients with myasthenia gravis and thymic FDG accumulation require special attention.
CONCLUSION
FDG accumulation in the thymus is a common finding in children and can occasionally be observed in young adults after chemotherapy. Knowledge of the characteristics of a typical retrosternal lesion in conjunction with the clinical history makes possible the avoidance of diagnostic uncertainty and unnecessary procedures. FDG PET does not appear to be suitable for proving that the thymus has been invaded by lymphoma.
Acknowledgments
The authors thank Michael Mix for iterative image reconstruction; Ursula Sahm, Kenneth Stålmo, and Bernd Morasch for producing the radioisotope and radiopharmaceutical; and Claudia Santini-Böttcher and Åsa Stålmo for technical assistance.
Footnotes
Received Aug. 7, 2000; revision accepted Dec. 11, 2000.
For correspondence or reprints contact: Ingo Brink, MD, PET Center, Division of Nuclear Medicine, University of Freiburg, Hugstetterstrasse 55, 79106 Freiburg, Germany.
REFERENCES
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Physiologic Thymic Uptake of 18F-FDG in Children and Young Adults: A PET/CT Evaluation of Incidence, Patterns, and Relationship to Treatment
- The role of FDG-PET scans in patients with lymphoma
- PET Evaluation of Lung Cancer
- Hodgkin's Lymphoma: Evolving Concepts with Implications for Practice
- Effect of Respiratory Gating on Quantifying PET Images of Lung Cancer
- FDG uptake in the morphologically normal thymus: comparison of FDG positron emission tomography andCT