


Abstract
99mTc-labeled ciprofloxacin (infecton) has been developed for detecting infectious foci, which localize in high concentrations in living bacteria. Other studies performed with various infections in animals and humans have found that infecton is a promising agent with better specificity for bacterial infections than white blood cell (WBC) scans. In this study, we evaluated the efficacy of infecton scintigraphy for detecting chronic bone and joint infections. Methods: Fifty-six sites with suspected bone or joint infection were examined with 99mTc-WBC and infecton scans in 51 patients. Of these patients, 21 had prosthetic implant materials. Biochemical, radiologic, and microbiologic data and clinical outcomes also contributed, along with the results from scintigraphic techniques, in determining the presence or absence of infection. Scintigraphic images were produced at 1 and 4 h after injection of 370–400 MBq infecton or 185–200 MBq 99mTc-hexamethylpropyleneamine oxime (HMPAO)-WBCs. For each patient, there were at least 2 d and at most 7 d between scintigraphic studies. Results: There were 30 true-positive, 4 false-positive, 20 true-negative, and 2 false-negative results with infecton. With 99mTc-HMPAO-WBCs, the results were 20, 1, 23, and 12, respectively. Values for sensitivity, specificity, and accuracy were 94%, 83%, and 89%, respectively, with the infecton scan and 63%, 96%, and 77%, respectively, with WBC scanning. Differences between the two agents were statistically significant (P < 0.001). Infecton and WBC scan results were in general concordance for 43 of 56 sites (77%). Infecton results for vertebral infections were the most notable findings in this study, despite the limited number of patients with this condition. Infecton scans were positive for hot spots in five of six patients with vertebral osteomyelitis. WBC scans showed photon-deficient areas in four of these same patients and normal distribution in the remaining two patients. Conclusion: Infecton is a useful agent for detecting infectious foci in bones and joints. Moreover, the infecton scan seems to be a more powerful tool in diagnosing vertebral infections than WBC scintigraphy.
Radiolabeled white blood cell (WBC) scintigraphy, which has an established role in detecting infectious processes, including osteomyelitis, enables detection of areas of general inflammation but cannot be used to distinguish between bacterial and nonbacterial inflammatory processes (1,2). Some other current infection-localizing radiopharmaceuticals, including polyclonal and monoclonal antibodies, also localize in inflammatory areas but do not have a significant advantage over WBC scanning in terms of specificity for bacterial infection (3,4). Moreover, these agents are not reliable in diagnosing osteomyelitis in the axial skeleton, which frequently is seen as nonspecific photopenic areas (5–9).
Recently a new radiopharmaceutical, 99mTc-ciprofloxacin (infecton), has been developed for improved specificity in diagnosis of inflammation (10). Infecton consists of the synthetic broad-spectrum antibiotic ciprofloxacin linked to the radiochemical 99mTc. This agent combines the advantages of a 99mTc label and the broad-spectrum bacteria-localizing capability of ciprofloxacin. Initial in vitro studies and animal experiments have shown that infecton localizes in high concentrations in abscesses caused by both gram-positive and gram-negative bacteria, but it does not localize to areas of sterile inflammation or abscesses with dead bacteria (10). Infecton scanning was further compared with WBC scanning in humans with various types of infections and showed improved specificity over WBC scans (11–13).
Taking this improved specificity into consideration, our goal was to determine the efficacy of infecton imaging in the detection of chronic orthopedic infections. We also compared the results of infecton imaging with 99mTc-hexamethylpropyleneamine oxime (HMPAO)-labeled WBC imaging.
MATERIALS AND METHODS
Patients
We prospectively studied 51 patients with clinically suspected chronic skeletal infection (29 females, 22 males; age range, 6–85 y; mean age, 50 y) over a period of 3 y. The study was approved by the hospital ethics committee, and informed consent was obtained from all patients. On the basis of localization and the presence of an endoprosthesis, the patients were classified into three groups, described below.
Group I consisted of 18 patients with suspected infection in different parts of the skeleton (Table 1). Of these patients, 15 had an underlying preexisting condition such as trauma or orthopedic surgery. Three patients still have orthopedic devices (two intramedullary nails in the femur and one hip screw).
Group I Patient Data
Group II included 18 patients with a single endoprosthesis or double endoprostheses in the hip or knee joints, giving a total of 23 sites of suspected infection (11 hips, 11 knees, and 1 femoral fixation nail).
Group III contained 15 patients with suspected spinal infections. Of these, 4 had a previous history of infection (2 with pulmonary tuberculosis and 2 with bacterial sepsis).
A history was obtained from all patients, and all received a physical examination and routine biochemical analysis as well as appropriate radiologic examinations. In 24 patients, materials for microbiologic or histopathologic investigations were obtained as follows; swab cultures from draining wounds in 3 patients, joint aspiration material from 12 patients, needle aspiration material from 4 patients, and bone biopsy material from 5 patients. Specimens were sent for culture (aerobic, anaerobic, mycobacterial, and fungal cultures) and histopathologic analyses. In 6 patients, the results of microbiologic and histopathologic studies were inadequate or undiagnosable. Eleven of 51 patients were receiving antibiotic treatment when they were referred to our department.
Confirmation of osteomyelitis by microbiologic or histopathologic investigations was possible in 18 patients. In the remaining patients, at least 3 mo of clinical follow-up results were correlated with radiologic findings, and surgical reports were evaluated to decide whether bacterial infection was actually present.
Radiopharmaceuticals
Infecton was prepared by reconstitution of a two-phase labeling kit, by mixing 2 mg ciprofloxacin, 500 μg stannous tartrate, and 400 MBq freshly eluted sodium pertechnetate (St. Bartholomew’s Hospital, London, U.K.). The mixture was left standing at room temperature for 15 min. Radiochemical purity was determined with a simple thin-layer chromatography technique, using 1-mm paper (Whatman, Ann Arbor, MI) running in methylethylketone. Infecton was at the base, and free pertechnetate moved with the solvent front. Labeling efficiency was consistently >92%.
99mTc-HMPAO-WBCs were prepared from a 50-mL anticoagulated blood sample according to standard protocol (2). Labeling efficiency ranged from 40% to 60%.
Scintigraphic Imaging and Data Analysis
Patients underwent both 99mTc-HMPAO-WBC scanning and infecton imaging. There were at least 2 d and at most 7 d between scintigraphic procedures for each patient. Scintigraphic images from the areas of interest were obtained at 1 and 4 h after injection of 370–400 MBq infecton or 185–200 MBq 99mTc-HMPAO-WBCs, in at least two projections. In suspicious patient cases, 24-h images were also acquired. For areas of interest, the counting rate was varied from 300,000 to 750,000 counts per image for WBC scanning and from 500,000 to 1,000,000 counts per image for infecton scanning at 1- and 4-h imaging. For the 24-h late scans, we performed a 15-min acquisition per image for both agents. In eight patients, whole-body images with infecton were obtained to inspect biodistribution of the agent. Images were recorded using a large-field-of-view (LFOV) camera fitted with a low-energy, all-purpose collimator. Forty-six patients also had a three-phase 99mTc-methylene diphosphonate (MDP) bone scan. The possible site of osteomyelitis was determined from clinical history and plain-radiograph findings as well as findings from the bone scan.
The scintigrams were visually evaluated by two experienced nuclear medicine physicians. In both WBC and infecton scans, any area of abnormally increased uptake in the suspected sites compared with surrounding healthy tissue or the contralateral side was considered positive for infection. Photon-deficient lesions seen in spines at WBC scanning were classified as negative results. The infecton results were compared with those of WBC scans. Sequential 1- and 4-h images from WBC and infecton studies were required for interpretation and inclusion in this study. The scans were read independently, and if there was disagreement in interpretation, the readers discussed their findings and reached a consensus. At the time of interpretation, the readers were unaware of the final diagnosis, as well as the results of other imaging modalities, except for delayed MDP bone scans.
Safety Considerations
All patients were monitored before, during, and after the study. Blood pressure, heart and respiratory rates, and body temperature were examined before and 4 h after injection of infecton. In addition, patients were told to report anything unusual during the subsequent few days.
Statistical Analysis
The outcomes from the two imaging techniques were analyzed using the χ2 test. The degree of agreement between the two procedures was measured by κ statistics calculating the index κ (where κ is 0.0 when there is just a chance agreement and 1.0 when there is perfect agreement).
RESULTS
Group I Patients
Of the 18 patients in group I, 14 presented with osteomyelitis, 1 (patient 7) had soft-tissue infection, and no infection was proven in the remaining 3 (Table 1).
Infecton scans gave positive results in all patients (14/14) with active osteomyelitis in this group (Fig. 1), whereas the results of WBC imaging were positive in 13 of these 14 patients. WBC scanning missed low-grade septic arthritis in the knee of patient 16. In the patient with soft-tissue infection without osteomyelitis in the hip (patient 7), the infecton result was positive despite a negative result for the WBC scan (Fig. 2). In the patient with avascular necrosis in her left hip (patient 12), both infecton and WBC scanning gave false-positive results. In the patient with fibrous dysplasia in her right ulna (patient 9), infecton imaging results were positive despite negative results from the WBC scan.
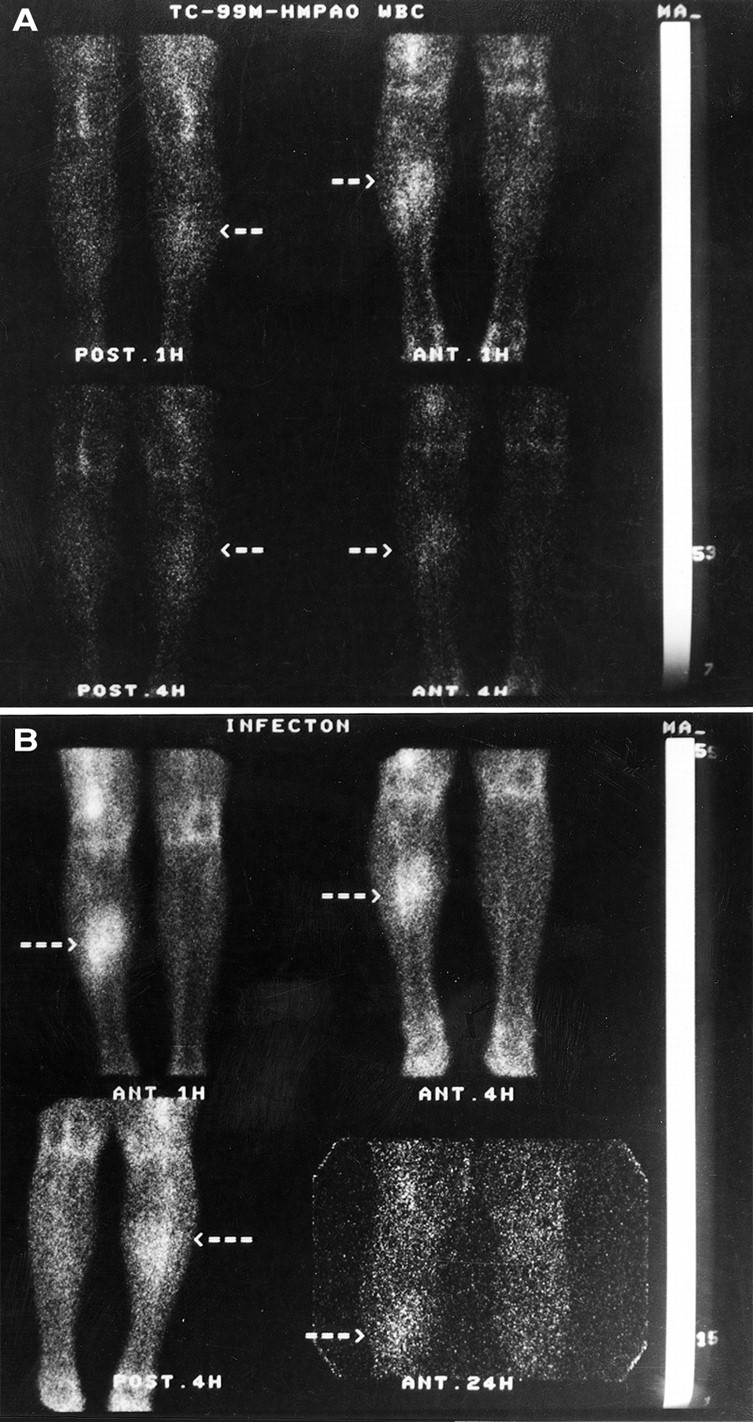
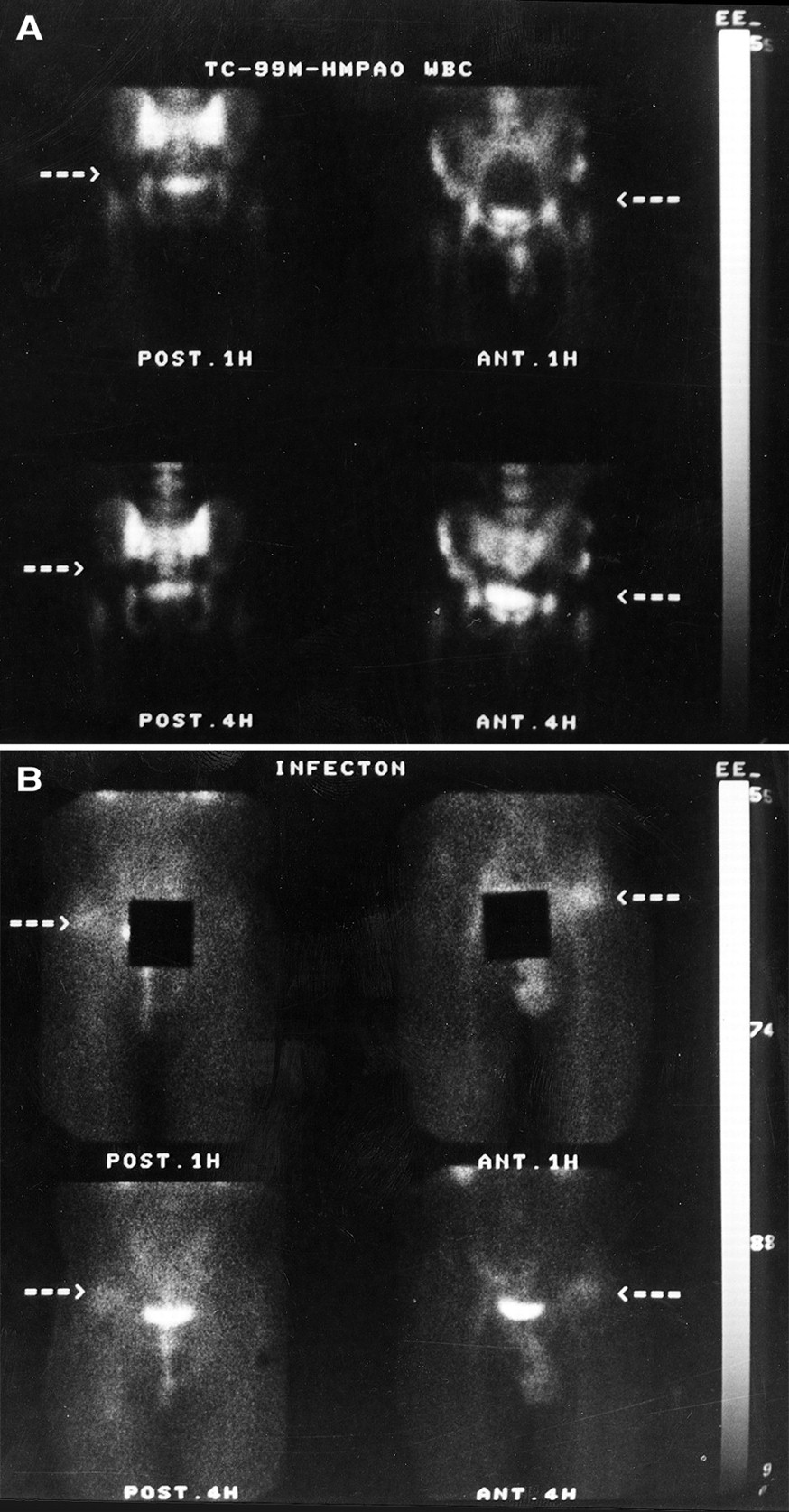
99mTc-HMPAO-WBC (A) and infecton (B) diagnostic images of 42-y-old man with chronic osteomyelitis in right leg after traumatic fracture, produced at 1 and 4 h after injection and at 1, 4, and 24 h after injection, respectively. Images show concordant results. Note increased synovial activity in knees even on contralateral healthy side in infecton images.
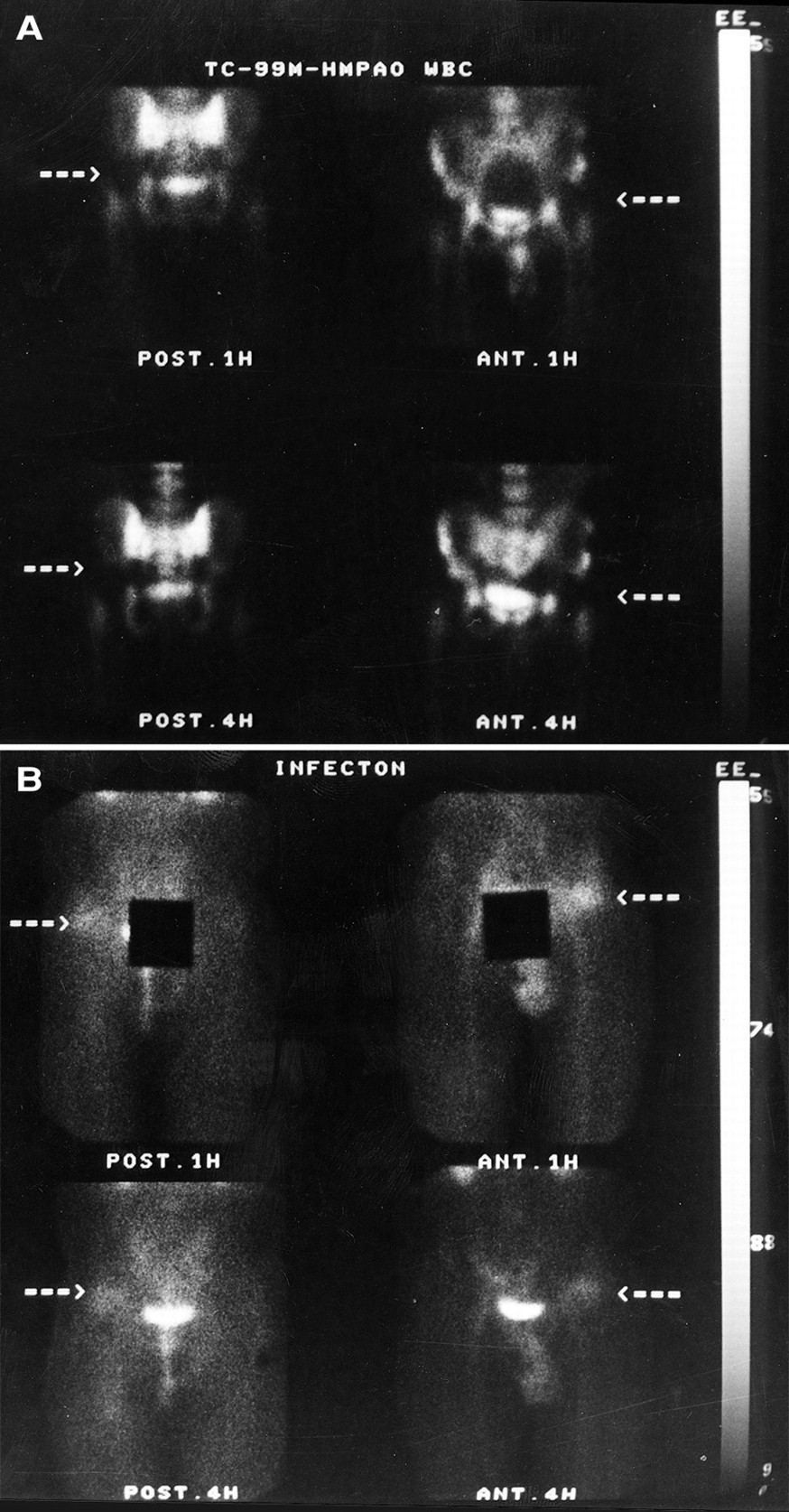
99mTc-HMPAO-WBC (A) and infecton (B) images at 1 and 4 h after injection of 31-y-old man with pain in left hip 2 y after hip orthopedic surgery. Hip injury was sustained in traffic accident. Infecton images show marked abnormality of left hip, which was reported as soft-tissue abscess without osteomyelitis.
Group II Patients
In group II patients, 12 of 23 sites of suspected infection were finally considered positive for osteomyelitis (Table 2). One patient (patient 14) had only periprosthetic soft-tissue infection without osteomyelitis in his left hip. In the remaining 10 sites, there was no proven evidence of infection. Infecton scans gave positive results for 11 of 12 sites with osteomyelitis. Infecton was also positive in the patients with periprosthetic soft-tissue infection without active osteomyelitis. WBC imaging gave positive results in only 7 of 12 sites with osteomyelitis. Figure 3 shows discordance between infecton and WBC images in a patient with a fixation nail in the right femora and proven osteomyelitis.
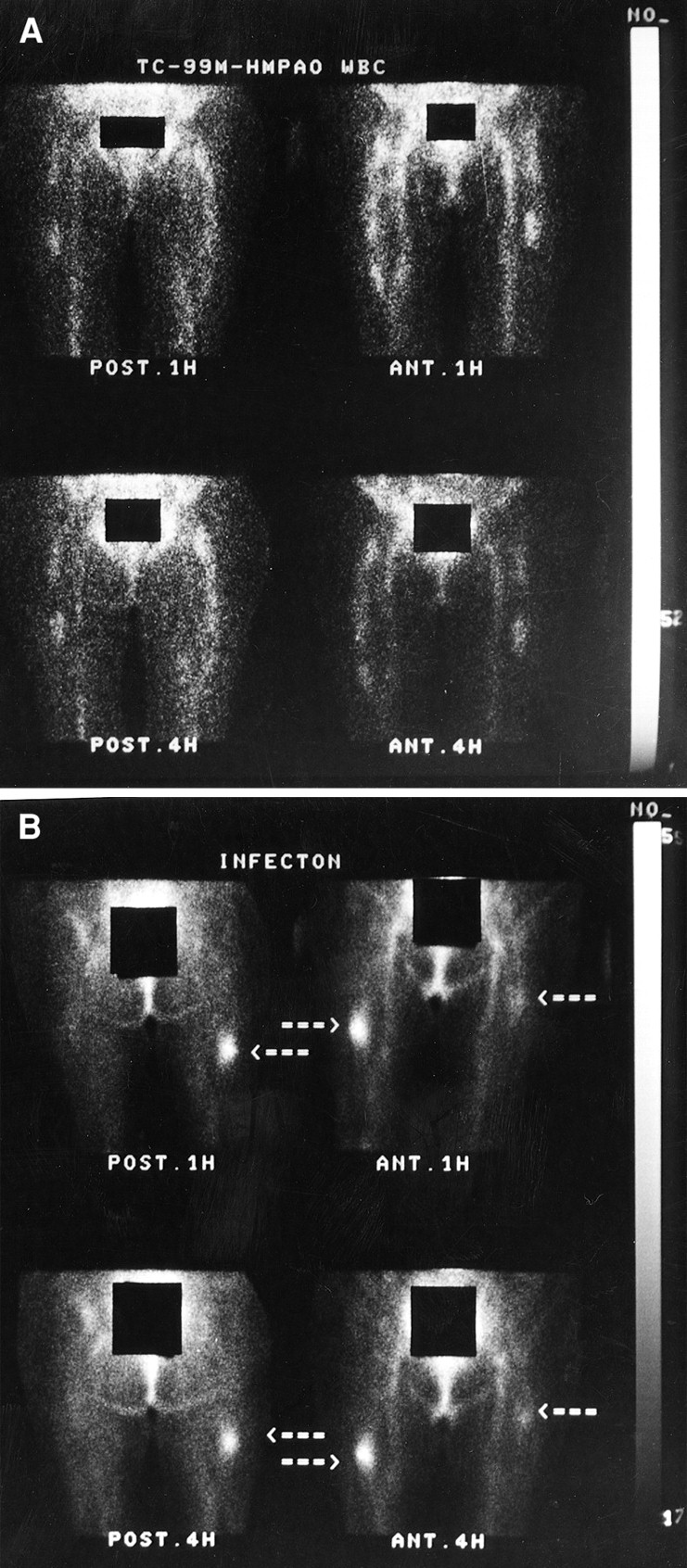
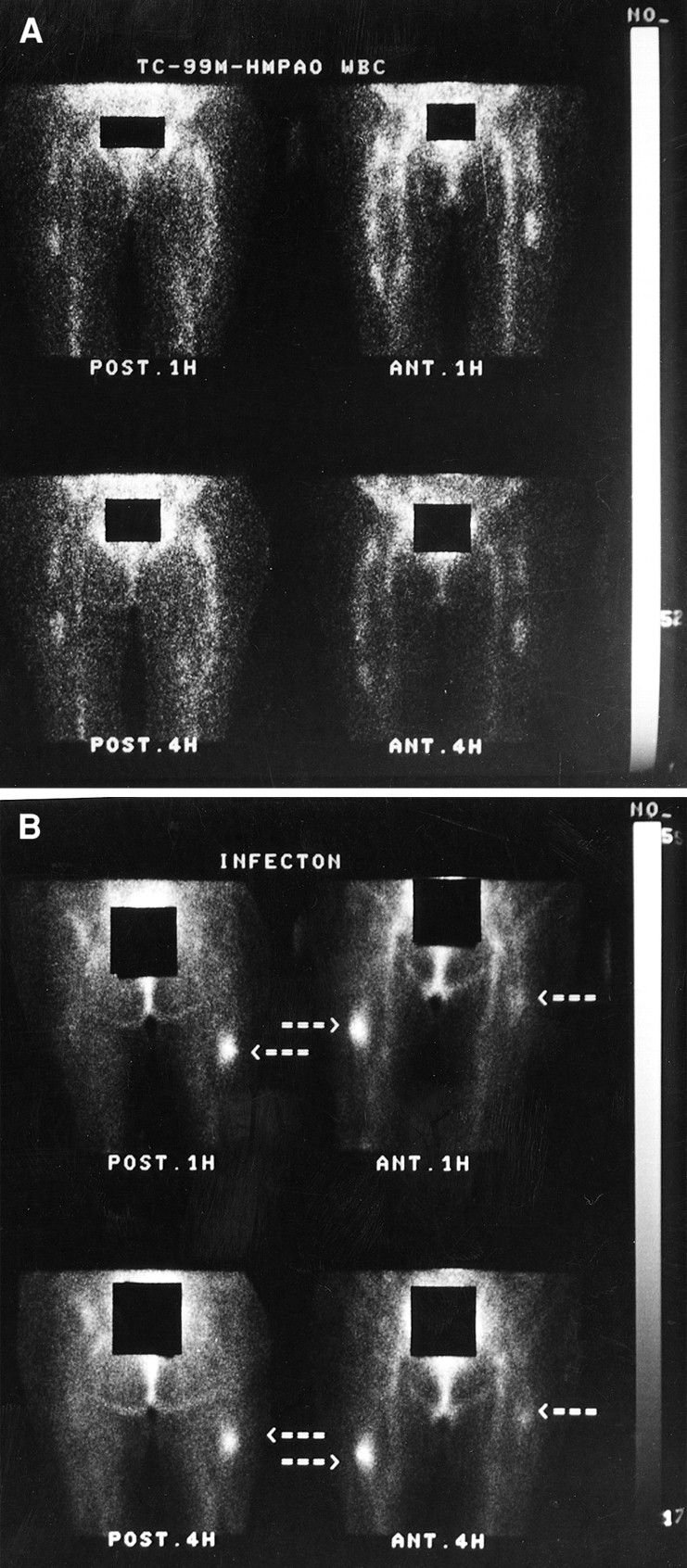
(A) 99mTc-HMPAO-WBC images show focal tracer accumulation in distal tip of left hip endoprosthesis but no abnormal findings in right femora, where fixation nail is present, in 77-y-old man who underwent orthopedic surgery 1 y previously. (B) Infecton scans confirm abnormality in distal end of left hip prosthesis and also show pronounced focal accumulation of tracer in area of right femoral fixation nail. Biopsy results confirmed osteomyelitis on both sides.
Patients with Joint Replacement
Group III Patients
The results in group III deserve particular attention. The results of infecton scans were positive for a hot spot in five of six patients with proven vertebral infection and were negative in nine patients with disproven spinal infections, including one with bone metastasis and one with bone lymphoma (Table 3). WBC scans showed photon-deficient areas in four infected vertebrae and normal distribution in the other two infected vertebrae. One patient (patient 6) with spondylodiskitis in lumbar vertebrae 4 and 5 who had false-negative results in both infecton and WBC scans was under intense antibiotic and corticosteroid therapy for 3 wk. The results of 67Ga scanning were also negative in this patient. Figure 4 shows an example of vertebral infection with a hot spot in infecton images and a photopenic lesion in a WBC scan. In Figure 5, another patient with spinal infection and an increased uptake of infecton on initial scans shows a relatively decreased uptake on follow-up scans 1 mo later.
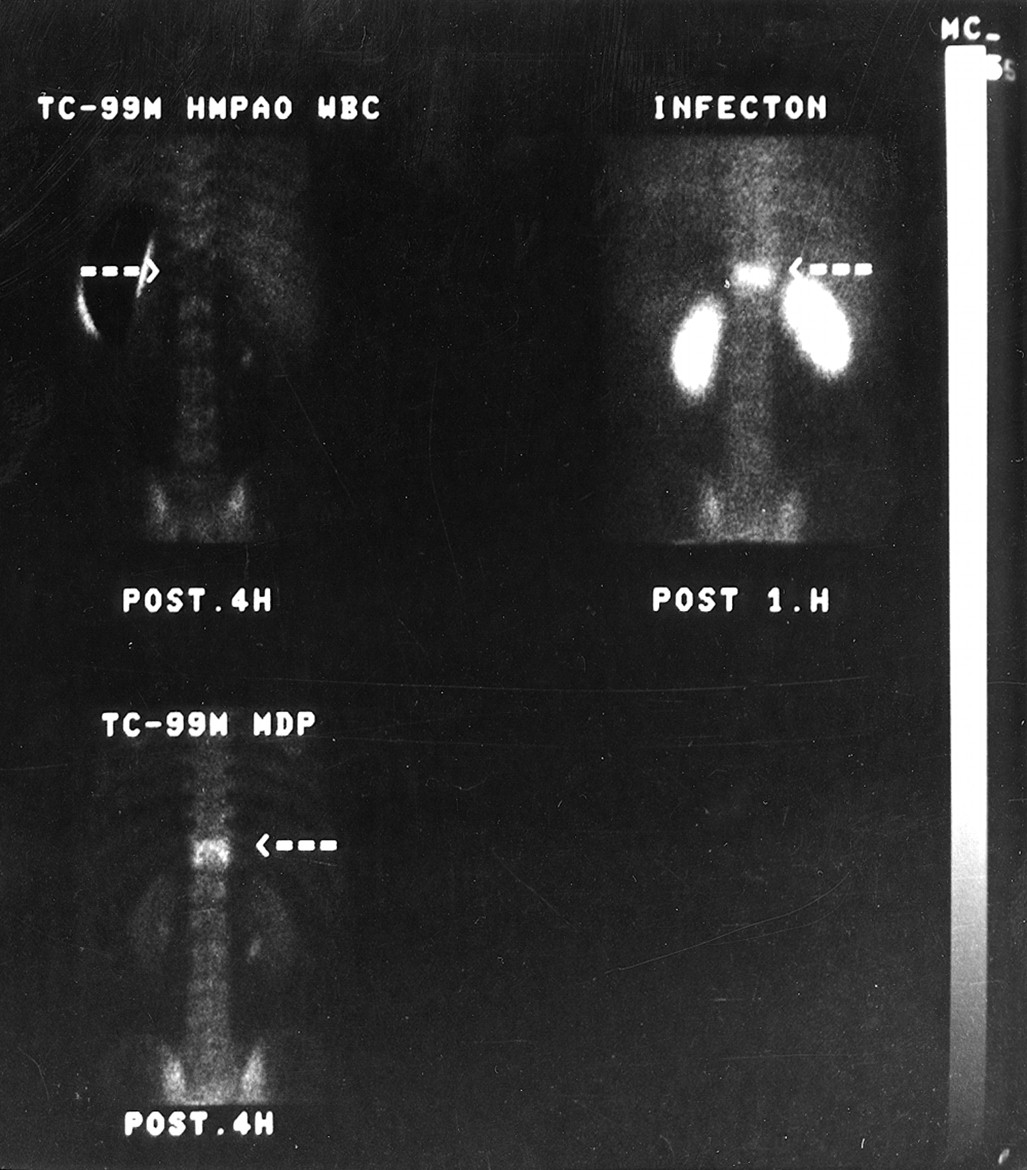
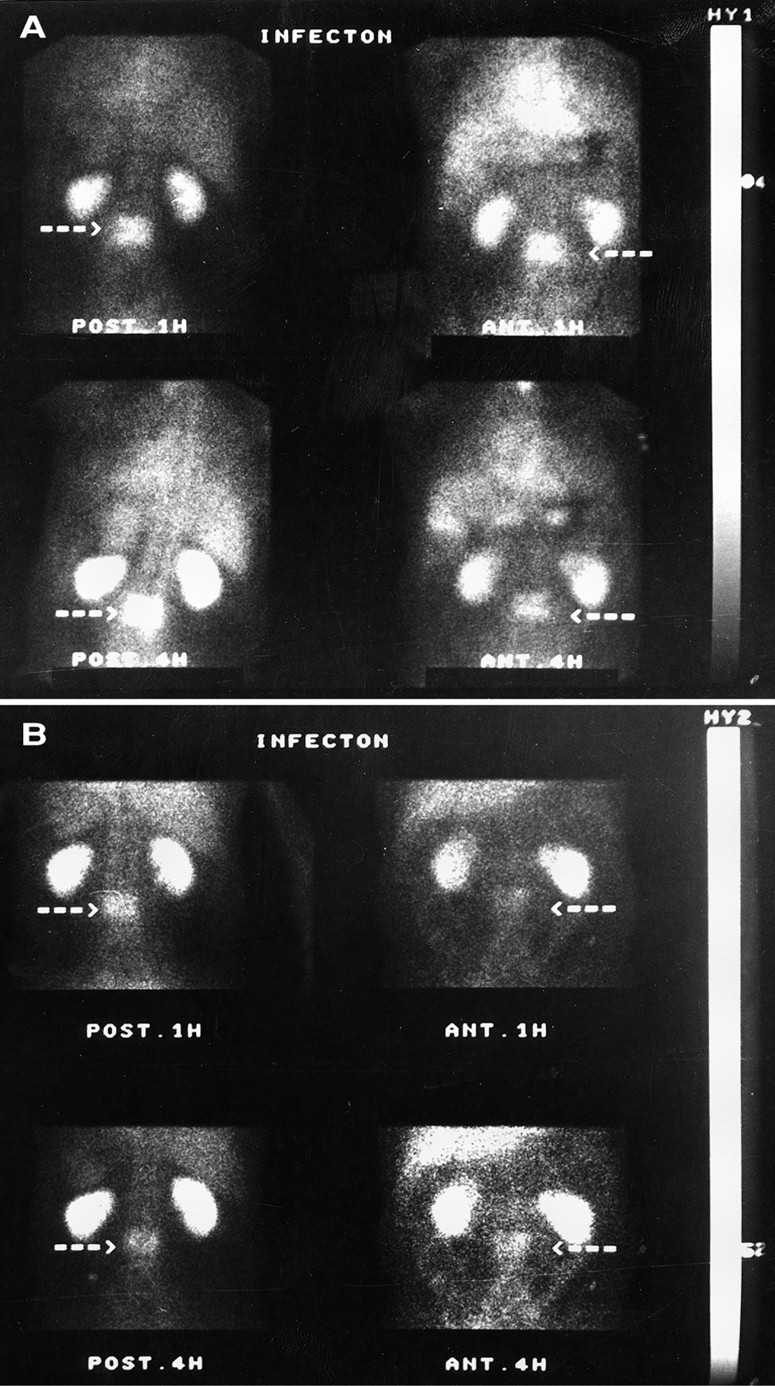
Infecton image (upper right) shows increased focal activity concordant with results of MDP scans (lower left), whereas 99mTc-HMPAO-WBC scan revealed cold lesion on same area (upper left) in 60-y-old man with history of suspected spondylodiscitis and pain on dorsal vertebra 12.
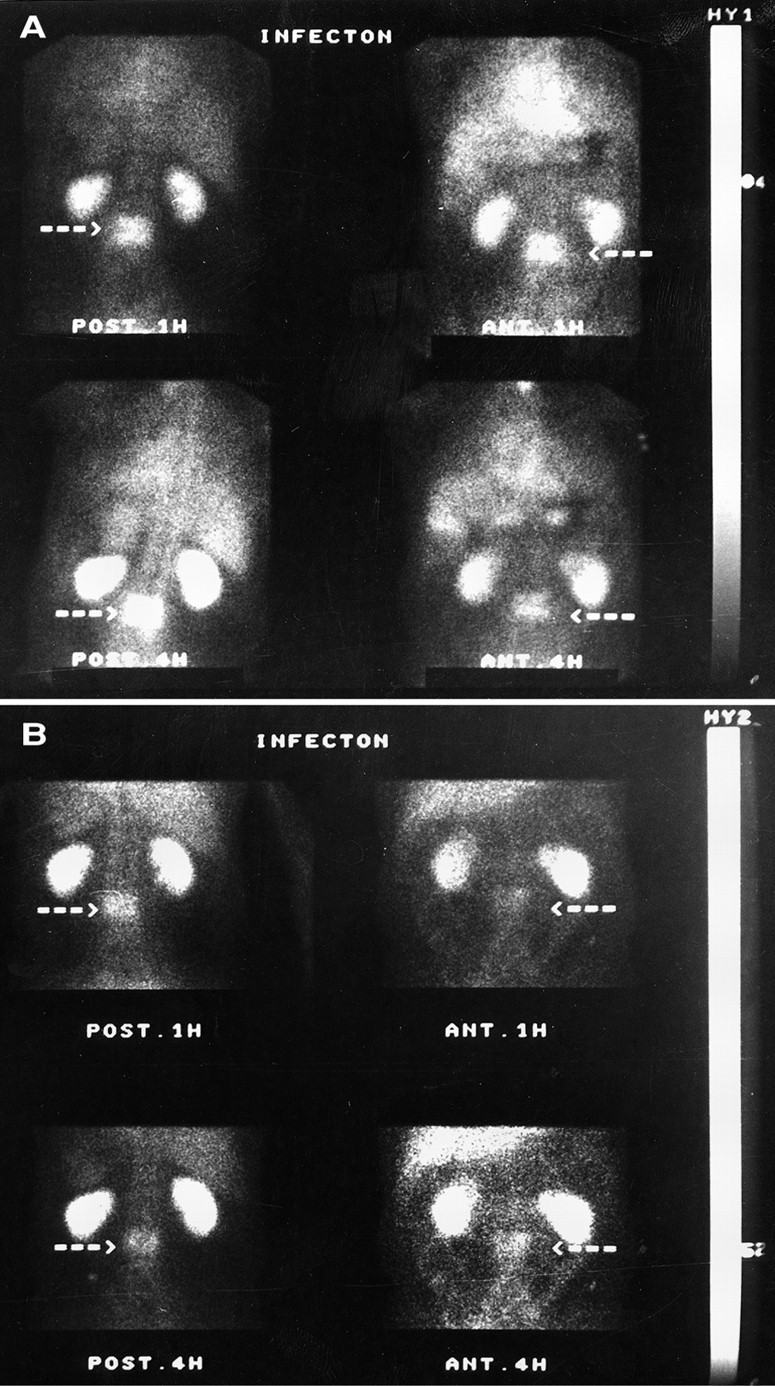
Series of infecton images of 62-y-old man with severe lower back pain caused by spondylodiskitis on lumbar vertebrae 2 and 3. Initial image (A) revealed marked increase in activity in that area, with lesion-to-background ratio of 1:66. One month after intense antibiotic therapy, dramatic improvement was observed; however, infecton images (B) still showed increased activity in same area but relatively decreased density of lesion (lesion-to-background ratio, 1:24).
Patients with Suspected Vertebral Osteomyelitis
Total Evaluation
Of the 56 sites suspected of infection, 32 had osteomyelitis and 24 did not; 2 of these 24 negative sites had soft- tissue infections. Infecton imaging correctly detected 30 of 32 sites (94%) with active osteomyelitis and 20 of 24 sites (83%) without osteomyelitis. When photopenic lesions in the spine were considered negative, the results of WBC scans were positive in 20 foci (63%) with osteomyelitis and negative in 23 of 24 sites (96%) without osteomyelitis. In two patients who had only soft-tissue infection, infecton gave positive results, whereas WBC scans were negative. There were four and one false-positive results with infecton and WBC scans, respectively. The general concordance rate of the infecton and WBC scans was 43 of 56 (77%, κ = 0.55).
Overall, there were 30 true-positive, 4 false-positive, 20 true-negative, and 2 false-negative results with infecton scanning. When the photopenic lesions in the spine were considered negative, the figures were 20, 1, 23, and 12, respectively, with 99mTc-HMPAO-WBC scanning. The values for sensitivity, specificity, and accuracy were 94%, 83%, and 89%, respectively, for infecton scintigraphy and 63%, 96%, and 77%, respectively, for 99mTc-HMPAO-WBC scintigraphy. The differences between the two methods are significant (χ2 = 7.14; P < 0.001).
Sixteen of 24 knee joints imaged with infecton showed typical synovial accumulation even in healthy knees with no previous surgery and no proven infection (Fig. 1). Of the knee joints with infecton accumulation in synovial cavities, three had septic arthritis, one had rheumatoid arthritis, six had prostheses with disproven infection, and the remaining six had possible degenerative changes.
We observed a biodistribution pattern of infecton identical to patterns described in previous studies: high uptake in the kidneys with excretion to the urinary bladder, moderate uptake in the liver and spleen, and no bone marrow or lung uptake. Early images show blood-pool activity, which is reduced in delayed images (12).
The most common microorganism grown on bacteriologic cultures was Staphylococcus aureus (n = 7) followed by coagulase-negative Staphylococcus species (n = 5), Pseudomonas species (n = 3), and Escherichia coli (n = 1).
No changes in vital signs were observed after the administration of infecton, and none of the patients reported any adverse reactions after the study.
DISCUSSION
Detection of chronic osteomyelitis remains a diagnostic challenge, particularly when the disease is localized to the axial skeleton. Clinical symptoms are often vague, and laboratory data are not very helpful. In spite of the established role of nuclear medicine in infection imaging, neither conventional agents, including 67Ga-citrate and 111In- or 99mTc-labeled WBCs, nor new radiopharmaceuticals such as radiolabeled polyclonal and monoclonal antibodies completely meet the requirements for an ideal infection imaging agent. In particular, the inability to discriminate infection from noninfectious inflammation with these agents is a major limitation in their current use for the diagnosis of infection. In this respect, infecton seems to have some important advantages over other infection-localizing radiopharmaceuticals. Furthermore, infecton meets many of the criteria described for an ideal infection imaging agent (14). It does not require handling of blood during preparation; it is packaged as a kit and is technically easier and less labor intensive than radiolabeling WBCs. The complex within the kit is stable over 8 h (10). Infecton is independent of the WBC status of the patients and thus has a valuable advantage for the detection of infection in leukopenic patients. Finally, this agent can be used to easily detect infection in the spine and proximal parts of the limbs because it is not taken up by bone marrow, in contrast to most of the other agents in current clinical use.
The overall sensitivity, specificity, and accuracy of infecton in musculoskeletal infection were 94%, 83%, and 89%, respectively. These results compare well with the reported figures in the literature for other infection-localizing agents used in routine practice (15–20). WBC scanning was found to be less sensitive than expected in this study population; this low sensitivity was thought to be mainly because of the spinal patients, all of whom had negative WBC scans. In addition, infections in almost all of the patients in our study were chronic and likely to have low granulocyte migration and turnover in infected areas (21,22). Furthermore, the study population was not randomly selected. We have generally done WBC scans first and then infecton scans, particularly when there is a high likelihood for infection. Nevertheless, it is clear that infecton is better in spinal infections in which WBC scanning and radioimmunoscintigraphy have proved unreliable (7,19,23). In our series, five of six patients with proven vertebral infection had a hot spot at the site of infection, although WBC scans showed either a cold defect (in four patients) or normal distribution (in two patients). Amaral et al. (24) also observed a hot spot with infecton in three patients with vertebral infections.
In four patients who had bacterial strains resistant to ciprofloxacin, infecton imaging was also positive. Britton et al. (12) have found similar results, and this finding implies that the infecton scan is also effective in some antibiotic-resistant-bacterial infections.
There were two false-negative results with the infecton scan. One of these was from a patient who had spondylodiskitis in lumbar vertebrae 4 and 5 and was receiving intensive antibiotic and corticosteroid therapy. WBC and 67Ga scans were also negative in this patient. The other patient with false-negative infecton scan results and positive WBC scan results had a total-knee prosthesis. WBC scans revealed increased activity in the tibial component of the knee. In the infecton images, there was intense synovial accumulation which may have masked the foci seen in the WBC scan. Vinjamuri et al. (11) reported that antibiotic therapy might cause false-negative results with an infecton study. However, we observed this effect for only one of seven patients with proven infection who were receiving antibiotic treatment at the time of their infecton scan.
Four patients with disproven osteomyelitis had positive infecton scans. Two of them had a soft-tissue abscess in the hip without osteomyelitis, which was confirmed by surgical exploration. One patient was histopathologically proven to have fibrous dysplasia. The last patient had severe pain of recent onset in her left hip. The bone, WBC, and infecton scans revealed increased tracer accumulation in that area together with positive clinical and laboratory findings for infection. However, postoperative histologic examination revealed a diagnosis of avascular necrosis with no microbial growth.
There might be some controversies regarding two patients with solely soft-tissue infection and positive infecton scans. Even though there was no diagnostic entity of osteomyelitis, the positive results of infecton scans correlated well with the clinical status of the patients and revealed the cause of the pain in these two patients. Because the presence of a soft-tissue infection is quite important in the identification of chronic orthopedic infections, maybe these two patients do not clearly fall under the false-negative category for the infecton scan. This approach makes the infecton stronger in diagnosis of chronic musculoskeletal infections.
Regarding a localization mechanism, infecton most probably binds to living bacteria at foci of infection in the same way that ciprofloxacin itself binds to bacteria, as confirmed in previous in vitro studies (10). However, our false-positive studies in the patients with histologically confirmed fibrous dysplasia and avascular necrosis suggest that there might be additional localization mechanisms for infecton.
CONCLUSION
infecton appears to be an effective and sensitive agent to detect chronic skeletal infections. Its specificity is slightly decreased by a relatively small percentage of false-positive results. It can be used as an alternative to conventional agents for diagnosis of bone infections. Moreover, the lack of bone marrow uptake makes it a powerful and promising agent to detect vertebral infections.
Acknowledgments
The authors thank Dr. Mustafa Senocak and Dr. Levent Kabasakal for statistical assistance and Cavit Nisli and Nedim Erdogan for technical assistance. This study was supported by the research fund of the University of Istanbul (project B-273/110899).
Footnotes
Received Aug. 24, 2000; revision accepted Nov. 17, 2000.
For correspondence or reprints contact: Kerim Sonmezoglu, MD, Cerrahpasa Medical Faculty, Nuclear Medicine Department, Istanbul University, P.O. Box 23, Cerrahpasa 34303, Istanbul, Turkey.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Role of Modern Imaging Techniques for Diagnosis of Infection in the Era of 18F-Fluorodeoxyglucose Positron Emission Tomography
- Synthesis and Comparison of 99mTc-Enrofloxacin and 99mTc-Ciprofloxacin
- Nuclear Medicine, the Painful Prosthetic Joint, and Orthopedic Infection
- Inability of 99mTc-Ciprofloxacin Scintigraphy to Discriminate Between Septic and Sterile Osteoarticular Diseases
- 99mTc-Labeled Antimicrobial Peptides for Detection of Bacterial and Candida albicans Infections