


Abstract
This study evaluated the relationship between the location of the most severe myocardial perfusion defects, the most severe coronary artery stenosis, and the site of subsequent acute myocardial infarction (AMI). Methods: Of 3,180 patients who were admitted with a diagnosis of AMI, we identified 44 patients who had undergone previous myocardial perfusion SPECT. Thirty-one of them also had previous coronary angiography. The relationship between the location of the myocardial perfusion defects, the coronary artery stenosis, and the site of subsequent AMI was studied in these patients. Results: The concordance between the location of the most severe reversible defects detected by SPECT and the site of subsequent AMI was 71% (κ = 0.499). The concordance between the most severe stenosis detected by coronary angiography and the site of subsequent AMI was 64% (κ = 0.451). However, κ values for SPECT and coronary angiography were good when the interval between these investigations and subsequent AMI was <3 mo (0.724 and 0.661, respectively), for moderate to severe perfusion defects (0.719), and for 90%–99% coronary stenosis (0.626). Conclusion: The culprit lesion is not always the one that is manifested by the most severe reversible perfusion defect or the most critical coronary artery stenosis. Myocardial SPECT and coronary angiography can predict the location of a future AMI in 71% and 64% of patients, respectively. The percentage is higher when the interval between investigations and subsequent AMI is <3 mo, for moderate to severe perfusion defects, and for 90%–99% coronary stenosis.
Some angiographic studies (1–3) have suggested that the site of acute myocardial infarction (AMI) does not correlate well with the severity of preexisting anatomic coronary artery disease. These studies have concluded that non–flow-limiting stenoses are a common site of subsequent plaque rupture and thrombotic occlusion. Other studies (3–5) with myocardial perfusion SPECT have shown a similar correlation between the location of the perfusion defects and the site of the subsequent AMI. These differences could be attributed to a poor relationship between anatomic descriptors of coronary lesions and the hemodynamic impact on coronary blood flow. However, other factors, such as the time between imaging and infarction, the severity of coronary artery disease, or the presence of previous acute coronary syndromes, can influence the results.
This study evaluated the relationship between the location of the most severe myocardial perfusion defects, the most severe coronary artery stenosis, and the site of subsequent AMI. The study also considered factors that could influence the predictive power of both SPECT and coronary angiography.
MATERIALS AND METHODS
Patients
Between October 1991 and November 1999, 3,180 patients were admitted to our critical care unit with a diagnosis of AMI. Also during this period, myocardial perfusion SPECT with 99mTc compounds was performed in our hospital for 4,876 patients. Of these patients, we identified 59 patients who had undergone myocardial perfusion imaging before an AMI. We excluded from our analysis 8 patients who had either coronary artery bypass surgery or percutaneous coronary angioplasty in the period between myocardial perfusion imaging and AMI as well as a patient with chronic left bundle branch block. We also excluded 4 patients because the area of infarction could not be defined (non-Q-wave AMI) and 2 patients because ischemia was not observed by SPECT. Thus, the study group included 44 patients (18 women; age range, 45–78 y; mean age, 65.0 ± 8.0 y). Thirty-one of these patients underwent coronary angiography before AMI.
Diagnosis and Localization of AMI
AMI was diagnosed when an episode of chest pain (>30 min) was accompanied by either an electrocardiogram (ECG) finding of abnormal Q-wave or laboratory documentation of creatine kinase myocardial band release. According to the localization of the Q-wave, the AMI was classified as anterior (acute changes in leads V1 to V4), inferior (acute changes in leads II, III, and aVF, with or without acute changes in contiguous lateral and posterior leads), and lateral (changes limited to any or all leads I, aVL, V5, and V6). In non-Q-wave AMI, the infarct site was determined by analysis of regional wall motion abnormalities (hypokinesia or akinesia) on contrast ventriculography performed after subsequent AMI.
Each AMI was assigned to a coronary territory based on its location: the left anterior descending (LAD) coronary artery for anterior AMIs, the right coronary artery (RCA) for inferior AMIs, and the left circumflex (LCX) coronary artery for lateral AMIs.
Stress Test
All patients in the study underwent a symptom-limited exercise stress test on a bicycle ergometer with an initial 50-W load and successive 25-W increments every 3 min until exhaustion, development of moderate to severe angina, serious arrhythmia, exertional hypotension, or ST segment depression >2 mm measured at 80 ms from J point. When the peak heart rate was <80% of the predictive value and oxygen consumption was <5 metabolic equivalents without angina or positive ECG changes, dipyridamole was administered intravenously at a rate of 0.14 mg/kg/min for 4 min while the patient continued to exercise at the maximal tolerated load until 2 min after the end of the dipyridamole administration (6). The administration of the drug was interrupted if the patient developed angina or ≥1-mm ST segment depression.
Myocardial Perfusion SPECT
99mTc-methoxyisobutylisonitrile (99mTc-MIBI) was used in the first 24 patients, and 99mTc-tetrofosmin was used in the next 20 patients. Patients studied with 99mTc-MIBI received an intravenous dose of 555 MBq 30–60 s before the end of exercise. The stress study and the study at rest were performed on different days, with a minimal separation of 24 h between both. The same dose was used for the study at rest. Images were acquired 1 h after the administration of the radiopharmaceutical. Patients studied with 99mTc-tetrofosmin received an intravenous dose of 99mTc-tetrofosmin (296 MBq) 30–60 s before the end of exercise. Stress images were acquired 15–30 min after the administration of the radiopharmaceutical. An 888-MBq dose of 99mTc-tetrofosmin was administered immediately after stress images were obtained. Rest images were acquired 15–30 min after the administration of the radiopharmaceutical.
For both radiopharmaceuticals, SPECT was performed on an SP4 single-head tomographic system (Elscint, Haifa, Israel) using a step-and-shoot mode. Sixty projections were obtained over a semicircular 180° arc starting at the 30° right anterior oblique position and with detections every 3°. The camera was equipped with 0.925-cm-thick sodium iodide (Tl) crystals and a high-resolution, low-energy, parallel-hole collimator. A 20% energy window centered on the 140-keV photopeak of 99mTc was used. All projection images were stored on optical disk using a 64 × 64, 8-bit matrix. Reconstruction was performed (Butterworth filter, order 5, section frequency 0.4), and short-axis, horizontal long-axis, and vertical long-axis images were obtained according to current recommendations (7). No attenuation or scatter correction was used. Before reconstruction, all studies were corrected for nonuniformity with a 100-million-count matrix obtained weekly from a 99mTc flood source.
Semiquantitative visual interpretation was performed using short-axis, horizontal long-axis, and vertical long-axis tomograms divided into 13 predefined segments for SPECT (8). In each of these segments, uptake was assessed as normal, equivocal, mild defect, moderate defect, or severe defect (similar to the background uptake). All studies were evaluated by consensus between three experienced observers. The reversible perfusion defects in each study were then assigned a coronary artery territory, analogous to assignment for the site of the AMI. Anterior-basal, midanterior, anterior-apical, septum-basal, midseptum, septum-apical, and apical defects were assigned to the LAD territory; inferior-basal, midinferior, and inferior-apical defects were assigned to the RCA; and lateral-basal, midlateral, and lateral-apical defects were assigned to the LCX. Only the most severe reversible perfusion defects were considered for the analysis of concordance with the site of subsequent AMI.
Catheterization
Coronary angiography was performed using standard Seldinger’s technique. At least four projections were performed (orthogonally 2 × 2) for the left coronary artery, and two projections were performed (orthogonally) for the RCA. Coronary stenoses were evaluated visually by two experienced angiographers and were classified into four categories: <50% = nonsignificant, 50%–69%, 70%–89%, and 90%–99%. Only the most severe stenosis was considered for the analysis of concordance with the subsequent site of AMI.
Statistical Analysis
Continuous variables are described as mean ± SD, and categoric data are expressed as proportions. The χ2 test was used to compare results between groups. A value of P < 0.05 was considered statistically significant. The degree of association between the location of the most severe reversible defects, the most severe stenosis, and the subsequent site of AMI was evaluated by a κ coefficient of agreement. This coefficient was graded as follows: 0–0.2, very poor; 0.21–0.4, poor; 0.41–0.6, moderate; 0.61–0.8, good; 0.81–1.0, very good (9). All analyses were performed using the SPSS v. 7.5 (Chicago, IL) for Windows statistical package (10).
RESULTS
The clinical and myocardial SPECT stress characteristics of the study population are summarized in Table 1. There were 24 patients with moderate or severe reversible perfusion defects in the region where a subsequent AMI developed. Among the 44 patients with prior perfusion defects detected by SPECT, AMIs were classified as anterior in 16 (36%), inferior in 18 (41%), and lateral in 4 (9%). In 6 patients (14%) with non-Q-wave AMI, the localization could be determined by analysis of regional wall motion abnormalities on contrast ventriculography performed after subsequent AMI (4 anterior and 2 inferior). The interval between myocardial perfusion imaging and AMI was 4–1,100 d (mean, 206.5 ± 229 d).
Clinical Characteristics and Results of SPECT Exercise Testing (n = 44)
Coronary angiography was performed on 31 of the 44 patients (70%). In 17 of these patients, catheterization was performed before SPECT. Seven patients had one-vessel disease (4 RCA, 2 LAD, and 1 LCX), 13 had two-vessel disease (5 LAD + RCA, 5 LAD + LCX, and 3 RCA + LCX), and 11 had three-vessel disease. The interval between cardiac catheterization and subsequent AMI was 99.2 ± 118 d (range, 1–426 d). Four patients had 50%–69% stenosis, 10 patients had 70%–89% stenosis, and 17 patients had 90%–99% stenosis of the coronary artery related to the subsequent AMI.
Concordance between SPECT and coronary angiography to identify the most severe defect and the most severe stenosis was good (12/15, 80%; κ = 0.650) when the interval between the two investigations was <3 mo but was only moderate (9/16, 56%; κ = 0.349) when the interval was longer.
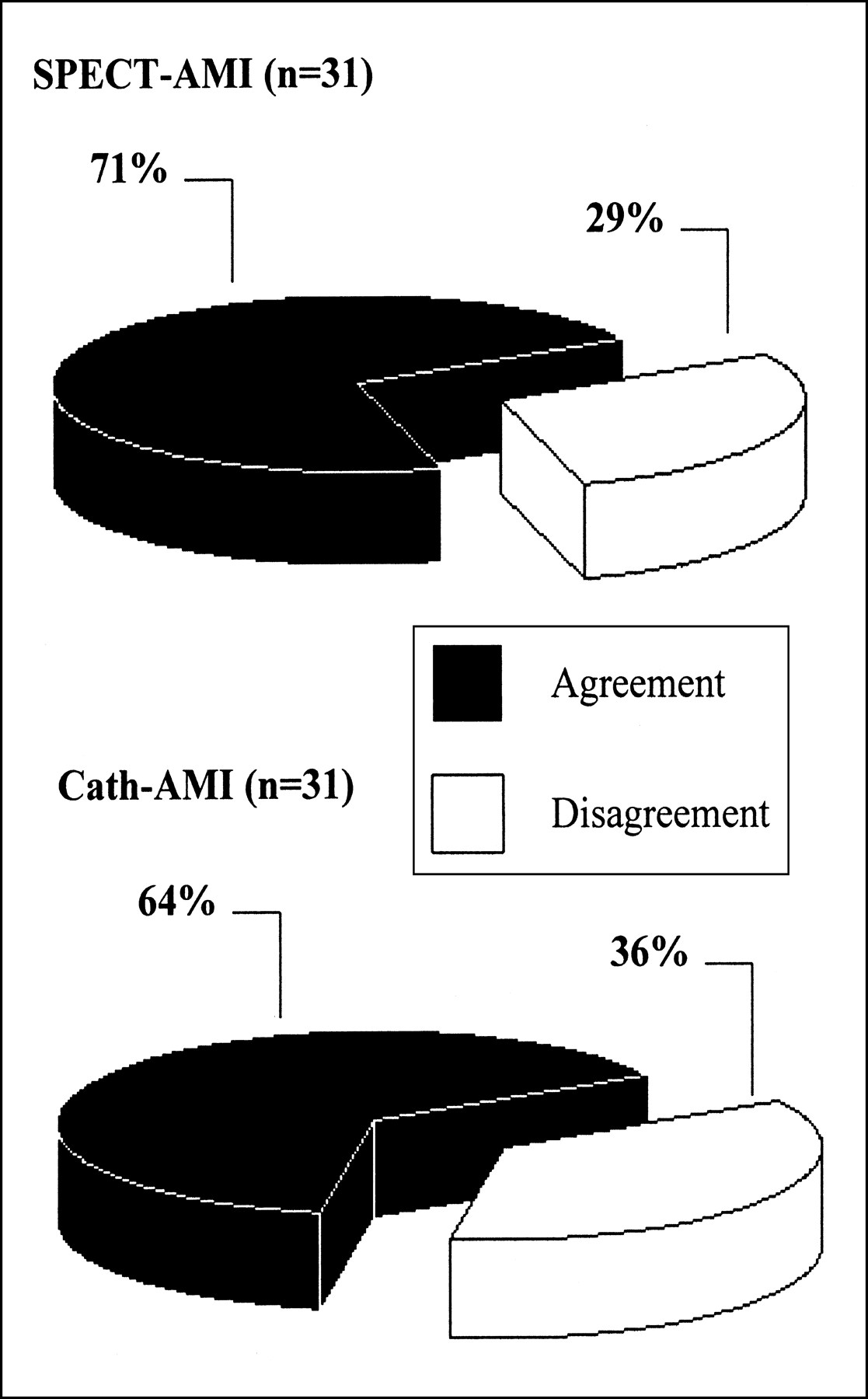
In the 31 patients studied with SPECT and coronary angiography, the concordance between the location of the most severe reversible defects detected by SPECT or the most severe stenosis detected by coronary angiography, and the site of subsequent AMI was 71% (22/31) and 64% (20/31), respectively (Fig. 1). The κ values were 0.499 and 0.451, respectively (Table 2).

Agreement between site of most severe reversible defects detected by SPECT, most severe stenosis detected by coronary angiography, and subsequent AMI location. Cath = catheterization.
Relationship Between Location of Most Severe Reversible Defects, Most Severe Stenosis, and Subsequent AMI Location
A κ value of 0.724 (concordance, 85%; 17/20) was observed in patients with a ≤3-mo interval between SPECT and AMI in contrast with a κ value of 0.503 (concordance, 71%; 17/24) in patients with a >3-mo interval (Table 3). For coronary angiography, κ values of 0.661 (concordance, 80%; 12/15) and 0.273 (concordance, 50%; 8/16) were observed for intervals ≤3 mo or >3 mo, respectively (Table 4).
Analysis of Interval Between SPECT Defect Detection and Subsequent AMI Location (n = 44)
Analysis of Interval Between Detection of Stenosis by Coronary Angiography and Subsequent AMI Location (n = 31)
The κ value between SPECT and subsequent AMI in patients with moderate to severe myocardial defects was 0.719 (concordance, 83%; 20/24), and it was 0.492 (concordance, 70%; 14/20) in patients with mild defects. The κ value between coronary angiography and subsequent AMI in patients with stenosis between 90% and 99% was 0.626 (concordance, 76%; 13/17), and it was 0.263 (concordance, 50%; 7/14) in patients with stenosis ≤90%.
The κ values between SPECT and subsequent AMIs in patients with and without previous AMIs were 0.602 (concordance, 77%; 23/30) and 0.638 (concordance, 78%; 11/14), respectively. The κ values between coronary angiography and subsequent AMIs in patients with and without previous AMIs were 0.448 (concordance, 63%; 14/22) and 0.449 (concordance, 67%; 6/9), respectively.
The κ values between SPECT and subsequent AMI in patients with and without previous unstable angina were 0.531 (concordance, 72%; 13/18) and 0.658 (concordance, 81%; 21/26) respectively. The κ values between coronary angiography and subsequent AMI in patients with and without previous unstable angina were 0.466 (concordance, 64%; 9/14) and 0.407 (concordance, 65%; 11/17), respectively.
In the 31 patients studied with coronary angiography, the concordance between the location of the most severe stenosis and the site of subsequent AMI was 75% (12/16) for LAD, 46% (6/13) for RCA, and 100% (2/2) for LCX. In the 44 patients studied with SPECT, the concordance between the location of the most severe reversible defects and the site of subsequent AMI was 85% (17/20) for the anterior region, 75% (15/20) for the inferior region, and 50% (2/4) for the lateral region (Table 5).
Catheterization and SPECT Findings
DISCUSSION
The correlation between anatomy and function is not strict in coronary artery disease, but knowledge of both factors is increasingly necessary for the management of coronary patients. Myocardial perfusion SPECT and coronary angiography can underestimate the severity and extent of coronary atherosclerosis. Stress myocardial perfusion scintigraphy fails to detect non–flow-limiting mild coronary stenoses, thus precluding accurate prediction of future AMI. In some patients, severe and extensive coronary artery disease does not result in clear defects detected by SPECT because of “homogeneity” of the ischemia (11). Angiographically severe stenoses are more likely to be asociated with collateral circulation than milder stenoses; therefore, an overt acute coronary syndrome is more likely to develop when occlusive thrombosis complicates a mildly obstructive plaque. To establish adequate management of coronary patients, it is important to know the ability of anatomic and functional investigations to predict future events. However, in previuos studies, the limited accuracy of coronary angiography (1–3) and myocardial SPECT (3–5) for predicting the site of subsequent AMI was found.
Previous studies with coronary angiography (Table 5) found only a 22%–55% agreement between the location of the most severe coronary stenosis and the site of subsequent AMI. In our study, we found a higher level (64%) of agreement. A possible explanation for this result is a short mean interval (3.6 ± 3.8 mo) between catheterization and AMI in our study compared with a 2-y interval for the other studies (1–3).
The agreement for previous SPECT studies (3–5) seems to be higher (47%–71%), although the intervals between the scintigraphic test and AMI (7–34 mo) tend to be lower. In the only previous study (3) in which SPECT and catheterization were performed on the same group of patients, no difference (55% vs. 47%) between these investigations in predicting the site of subsequent AMI was observed. We found similar values of agreement for myocardial SPECT (κ = 0.499) and coronary angiography (κ = 0.451).
Intervals between myocardial SPECT and AMI (3.4 ± 3.8 mo) and between coronary angiography and AMI (6.9 ± 7.7 mo) in our study were lower than those reported in all previous studies (1–5) (Table 5). We found the best agreement for SPECT and coronary angiography (κ = 0.724 and 0.661, respectively) when the interval between the investigation and subsequent AMI was <3 mo. Galvin and Brown (3) found a good association (κ = 0.680) between the coronary territory showing transient defects on myocardial perfusion imaging and the site of subsequent AMI when the duration was <2 y.
The correlation between coronary angiography and SPECT in the diagnosis of a culprit lesion is not optimal. Candell-Riera et al. (11) found 84% agreement in a series of 159 patients with coronary artery disease studied with an interval of <3 mo between these investigations. A lack of agreement in identifying the coronary lesion responsible for ischemia corresponds to patients with triple-vessel disease with a similar degree of stenosis in at least two of the three diseased arteries. The lack of agreement is also caused by problems with SPECT for assigning ischemia to the territory of the RCA or the LCX. In our study, concordance between SPECT and coronary angiography was 80% (κ = 0.650) when the interval between the two investigations was <3 mo, but it was only 56% (κ = 0.349) when the interval was longer.
Other factors that can influence the results have not been investigated in previous studies. We found that agreement is higher in the subgroup of patients with 90%–99% coronary stenosis and with moderate to severe perfusion defects. This result seems to confirm the higher correlation between SPECT and coronary angiography to detect the myocardium at risk of the culprit lesion (11). We found that other factors, such as previous acute coronary syndromes (unstable angina or AMI), did not affect the prediction of SPECT and coronary angiography.
Myocardial perfusion scintigraphy and coronary angiography may be very helpful in indicating the need for a revascularization procedure in patients with chronic coronary artery disease (12–14). Such use is particularly relevant when the aim is to identify the coronary lesion responsible for ischemia, the so-called culprit lesion (15,16). However, it is also important to know if these diagnostic tests can predict sites of future coronary events, such as an AMI.
Our study has shown a correlation between the location of a SPECT defect, the most severe coronary stenosis, and the location of a subsequent AMI. However, many AMIs occurred in territories without the most severe reversible defects (23%) or without the most severe coronary stenosis (38%). In these patients, the image findings served as markers of disease, predicting an increased risk of an infarct-producing plaque rupture somewhere in the coronary arterial circulation, which in these patients did not occur at the site of the most severe coronary flow impairment (17,18). Performing a revascularization procedure only for the most severe coronary stenosis or in response to the most severe reversible defect on myocardial perfusion imaging may not necessarily be effective in preventing a future AMI.
Our study, like most previous ones, is limited by its small size and retrospective design. In addition, as in other studies, it is subject to bias, because patients with the most severe and largest transient defects would likely be referred for revascularization, and less abnormal coronary angiography and SPECT results would be selected for study. The difficulty in assigning inferolateral defects to the RCA or to the LCX can decrease the agreement between territories (11). Finally, these studies were also limited by the difficulty in identifying the site of ischemia in medically treated patients who perform an insufficient exercise test (19–21) and in knowing the actual site of subsequent necrosis in some instances of non-Q-wave AMI.
CONCLUSION
The culprit lesion is not always the one that is manifested by the most severe reversible perfusion defect or the most critical coronary artery stenosis. Coronary angiography and myocardial SPECT can predict the location of a future AMI in 71% and 64% of patients, respectively. The percentage is higher when the interval between investigations and subsequent AMI is <3 mo and also for severe coronary stenosis and severe perfusion defects.
Acknowledgments
The authors are grateful to Irene Moral, Aida Ribera, and Gaietà Permanyer-Miralda, MD, for their revision of the manuscript.
Footnotes
Received Aug. 21, 2000; revision accepted Dec. 4, 2000.
For correspondence or reprints contact: Jaume Candell-Riera, MD, PhD, Servei de Cardiologia, Hospital Universitari Vall d’Hebron, P. del Vall d’Hebron 119–129, CP. 08035, Barcelona, Spain.




{kind=link}