


Abstract
The alteration of 99mTc-labeled diethylenetriaminepentaacetic acid (DTPA) transalveolar clearance in an initial phase of radiation lung injury was experimentally investigated. Methods: Fourteen dogs were irradiated to the hemithorax with a single dose of 20 Gy. A DTPA radioaerosol study was performed before irradiation and on day 12 after irradiation. On day 14, the DTPA study was repeated again, with seven animals undergoing the study after inhalation of an aerosolized synthetic surfactant. The penetration index (P.I.) and clearance half-time (T1/2) of DTPA were measured in each lung. To evaluate the changes in lung surfactant after irradiation, alveolar lipids were stained in the resected lungs (n = 14), and the amounts of alveolar surfactant phospholipid and protein were measured by a bronchoalveolar lavage study in another six irradiated dogs. Results: In all of the 14 irradiated animals, DTPA radioaerosol distributed uniformly throughout the lungs without significant changes in P.I. The T1/2 values in irradiated lungs were significantly prolonged compared with the matched baseline values and those in nonirradiated lungs (P < 0.05 and 0.001, respectively). The aerosolized synthetic surfactant retarded the DTPA clearance both in the irradiated and in the nonirradiated lungs (P < 0.001) without significant changes in P.I. The histologic and bronchoalveolar lavage studies revealed an increase of alveolar surfactant materials in the irradiated lungs without substantial histologic changes in the alveolar structures. Conclusion: DTPA transalveolar clearance was retarded soon after irradiation. Increased alveolar surfactant may be partly responsible for this retarded DTPA clearance because the aerosolized synthetic surfactant also prolonged the clearance in nonirradiated lungs. A DTPA clearance test is sensitive for the early detection of radiation lung injury and seems helpful for clarifying the association of epithelial integrity changes and lung surfactant in radiation lung injury.
- 99mTc-DTPA
- lung surfactant
- pulmonary radioaerosol scintigraphy
- alveolar permeability
- radiation lung injury
During radiotherapy, thoracic irradiation is carefully controlled because of potential damage to lung parenchyma. Ultrastructural morphologic damage of alveolar epithelial and endothelial cells is a consistent feature soon after irradiation (1–3), but the development of exudative radiation pneumonitis usually is delayed. During this latent period, alveolar integrity may be altered by morphologic damage to the alveolar–capillary membrane and also by impairment of the alveolar surfactant system caused by damage to type II alveolar epithelial cells (4,5). The study of early changes in alveolar integrity may aid in understanding the pathogenesis of radiation lung injury. Pulmonary clearance rates of aerosolized 99mTc-labeled diethylenetriaminepentaacetic acid (DTPA) provide a sensitive index for evaluation of changes in the alveolar permeability of small solutes (6–9). Accordingly, we used this technique to study the alteration of alveolar integrity after irradiation in an experimental model. Because only a few studies have focused on early changes in alveolar integrity after irradiation, this study was designed to investigate the alteration of DTPA lung clearance in initial phases of radiation injury in canine lungs. Further, to clarify the association between the altered alveolar integrity and lung surfactant soon after irradiation, we also investigated the changes in alveolar surfactant and the effects of inhalation of an aerosolized synthetic surfactant (Exosurf; Burroughs Wellcome Co., Research Triangle Park, NC) on DTPA clearance.
MATERIALS AND METHODS
Animal Models
A total of 26 mongrel dogs (weight range, 12.6–22.2 kg; mean weight ± SD, 15.7 ± 2.8 kg) were anesthetized by intravenous administration of 30 mg/kg phenobarbital sodium. The animals were placed in the supine position, intubated using a cuffed endotracheal tube, and connected to a volume-cycled piston ventilator (Harvard Instrument Co., Cambridge, MA). The respiratory rate was set at 15 breaths per minute, with a tidal volume of 15 mL/kg (volume range, 258–352 mL). Small supplementary doses of phenobarbital sodium (total doses ranged from 2.0 to 6.7 mg/kg) were given intermittently during the course of the experiments as needed to maintain adequate levels of sedation. Approval for this experimental study was received from the institutional animal care committee.
Six of the 26 animals served as controls. These animals each underwent two DTPA radioaerosol clearance studies separated by 48 h to assess the reproducibility of DTPA clearance rates. The same techniques were used in the remainder of the animals. Another 14 animals were irradiated through a right hemithorax field, 15 × 8 cm, with a single dose of 20 Gy using a 10-MeV linear accelerator apparatus. A relatively high dose of 20 Gy was given on the basis of previous electron microscopic studies (1,2) that showed minimal lung injury in the alveolocapillary structures at these levels of exposure. Each of these irradiated animals underwent a baseline DTPA clearance test 2 d before irradiation and on day 12 after irradiation. On day 14, the study was repeated in 7 of these 14 irradiated animals (group A). In the remaining 7 irradiated animals (group B), the study was repeated after inhalation of an aerosolized suspension of a dose of 1.5 mL/kg synthetic surfactant. The selection of these animals was decided before the beginning of the experiment without access to the information from the DTPA clearance tests.
The aerosolized synthetic surfactant is composed of 85% dipalmitylphosphatidylcholine, 9% hexadecanol, and 6% tyloxapol (7,8,10). An ultrasonic nebulizer (NE-U12; Omron, Tokyo, Japan) was used to deliver the surfactant. The nebulizer consists of a 50-mL canister, warmed to a 37°C operating temperature, which continuously generates a heterodisperse aerosol <2 μm in aerodynamic median mass diameter. It took approximately 80 min to complete aerosolization of a total dose of the surfactant (mean, 27.5 ± 1.3 mL for each dog), and the aerosol was administered to the animals through the ventilated circuit. A DTPA clearance study was performed approximately 30 min after inhalation of the surfactant. All 14 irradiated animals underwent chest radiography before irradiation and after the completion of each experiment.
The remaining six animals also received right hemithorax irradiation in the same manner as for the preceding 14 animals. These six animals underwent a bronchoalveolar lavage (BAL) study 12 d after irradiation to measure the amounts of alveolar surfactant phospholipid and protein A (SP-A), which are the major constituents of lung surfactant (11). All these animals underwent chest CT before the lavage study, and the absence of abnormal opacities in the lungs was confirmed. BAL was performed under fluoroscopy, during which a 4-French catheter was wedged to the peripheral bronchi in the symmetric portions of the irradiated and contralateral nonirradiated lungs. A total of 15 mL ice-cold 0.9% NaCl was then injected into the bronchi. Approximately 95% of the injected saline was recovered in all these animals. The concentrations of surfactant phospholipids and SP-A in aliquots of the lavage fluid were measured by the colorimetric ammonium ferrothiocyanate method of Furlong et al. (12) and Stewart (13) and by the anti–SP-A antibody method, respectively (SRL Inc., Tokyo, Japan). After the lavage study, these six animals also underwent chest CT every 3 wk to check the development of radiation pneumonitis up to 4 mo after irradiation.
DTPA Aerosol Study
Intubated animals were positioned supine over a 4/11 gamma camera (Picker, Bedford, OH) with a low-energy, all-purpose collimator. The camera was interfaced to a Gamma-600 data storage and analysis system (Strichman Medical Equipment, Inc., New York, NY) on a Macintosh personal computer (Apple Computer Inc., Cupertino, CA). DTPA radioaerosol was delivered to the animals through the ventilation circuit under the same constant ventilation conditions described earlier. The animals were ventilated by the same ventilator described previously, with the same respiratory rate and tidal volume. DTPA (740 MBq [20 mCi]) was aerosolized with compressed air at a rate of 6 L/min using a commercially available air jet nebulizer (AeroTech I Aerosol Inhalation System, model CA-1312; CIS, Bedford, MA) that generated a submicrometer polydisperse radioaerosol. The radioaerosol was administered until a count rate of more than 280 cps over the lung fields was obtained (usually for 4–5 min). The DTPA aerosol was delivered to the ventilated animals through the ventilation circuit under the same constant ventilation conditions described earlier. Computer-assisted evaluation of the radioaerosol clearance was started immediately after disconnection of the radioaerosol unit. Pulse-height analysis was performed at 140 keV with a 10% window, and sequential posterior views of the lung images were obtained with a 64 × 64 matrix at 15-s intervals for 30 min. To avoid changes in DTPA clearance in response to changes in the ventilation pattern (14,15), the mechanical ventilation conditions described earlier were used throughout all the experiments and the data collection. After the clearance phase was completed, 100,000-count digital 128 × 128 radioaerosol images (posterior, both right and left posterior obliques, and anterior) were acquired.
Additional Control Studies
Four of seven irradiated animals in the aerosolized surfactant group also inhaled an aerosolized DTPA/surfactant mixture to investigate the distribution of aerosolized surfactant in irradiated lungs (6). This study was performed 2 d after the initial surfactant inhalation, that is, 16 d after irradiation. Approximately 10 min before inhalation, 740 MBq (20 mCi) 99mTc-DTPA (volume < 1 mL) was added to 5 mL surfactant in the ultrasonic nebulizer canister. The aerosolized mixture was delivered to the animals in the same way as for the DTPA aerosol study, and digital lung images were similarly acquired.
In addition, a 99mTc macroaggregated albumin (MAA) perfusion scan was performed on six randomly selected animals (three each from groups A and B) to investigate the early postirradiation distribution of pulmonary arterial perfusion. Perfusion scans were performed 2 h after the DTPA study on day 14 after irradiation. After intravenous injection of 74 MBq (2 mCi) 99mTc-MAA, containing 100,000 MAA particles 10–60 μm in size, static 500,000-count images were acquired on a 128 × 128 matrix in the same four views as for the DTPA study described below.
Data Analysis
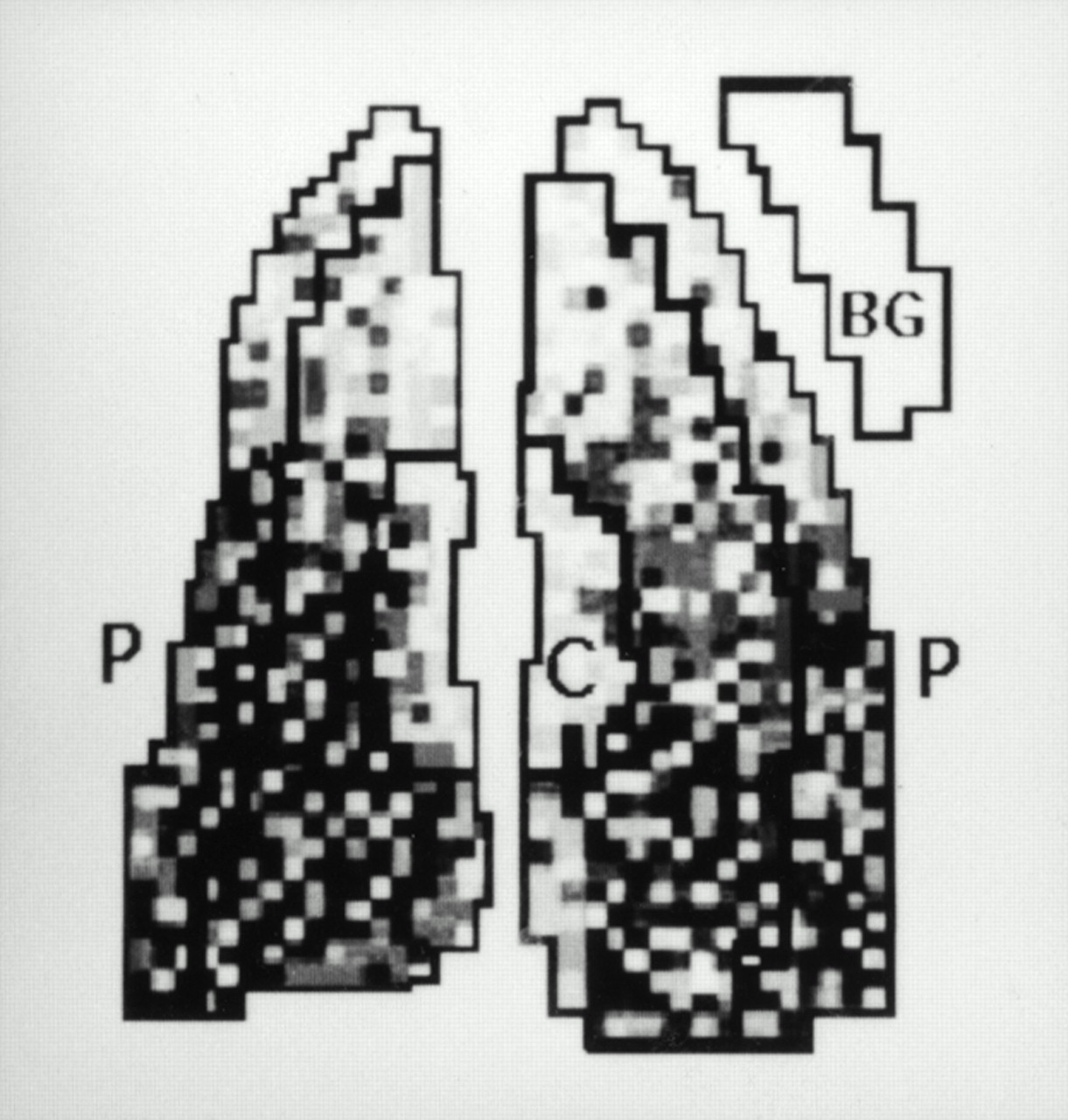
To determine the borders of each lung in the DTPA clearance test, a 20% isocontour line of the maximum count in either lung field was traced by computer on the posterior lung images. Time–activity curves describing DTPA clearance from the lungs were then obtained from regions of interest (ROIs) over the peripheral one third of each lung (Fig. 1). This procedure was done to obtain as pure an alveolar ROI (i.e., alveoli only) as possible. After correction for the physical decay of 99mTc and for background using radioactivity in the upper chest wall (Fig. 1), the logarithmic regression line of the decreased radioactivity as a function of time was fit by the least squares method to the experimental data from 1 to 30 min, and the clearance half-time (T1/2 in minutes) of the slope of the regression line was determined. The correlation coefficient for the best fit in the logarithmic regression line of all clearance curves exceeded 0.900 (average, 0.948 ± 0.025).

ROIs used to quantify DTPA radioaerosol study. BG = background area placed over upper chest wall; C = central ROI corresponding to inner third of lung; P = peripheral ROI of each lung.
To quantify the distribution of DTPA aerosol in the lungs, the penetration index (P.I.)—defined as the ratio of the mean activity per pixel of the peripheral one third of the lung to that of the central one third—was calculated for each initial 15-s image (15,16). A central ROI was inscribed bilaterally in the perihilar region covering approximately the central third of the lung, and counts in this region were compared with counts from the previously described ROIs over the periphery of the lungs.
Fourteen irradiated animals of groups A and B were euthanized on day 14 (n = 10) or day 16 (n = 4) after irradiation, and the remaining six irradiated animals were euthanized at 11–13 wk; histologic analysis of the lungs was then performed. Morphologic changes in the irradiated lungs were microscopically evaluated by an independent pathologist who was unaware of all other experimental information. Hematoxylin–eosin stain was used. In addition, alveolar surfactant lipids were stained by Sudan black B in the freeze-dried lung specimens of group A animals after fixation with 5% paraformaldehyde (16).
Statistical Analysis
99mTc-DTPA T1/2 values, P.I. values, and concentrations of the lavage surfactant phospholipids and SP-A were expressed as mean values ± SD. Paired and unpaired t tests were used to compare values within and between groups, respectively. Significant levels were accepted as being P < 0.05.
RESULTS
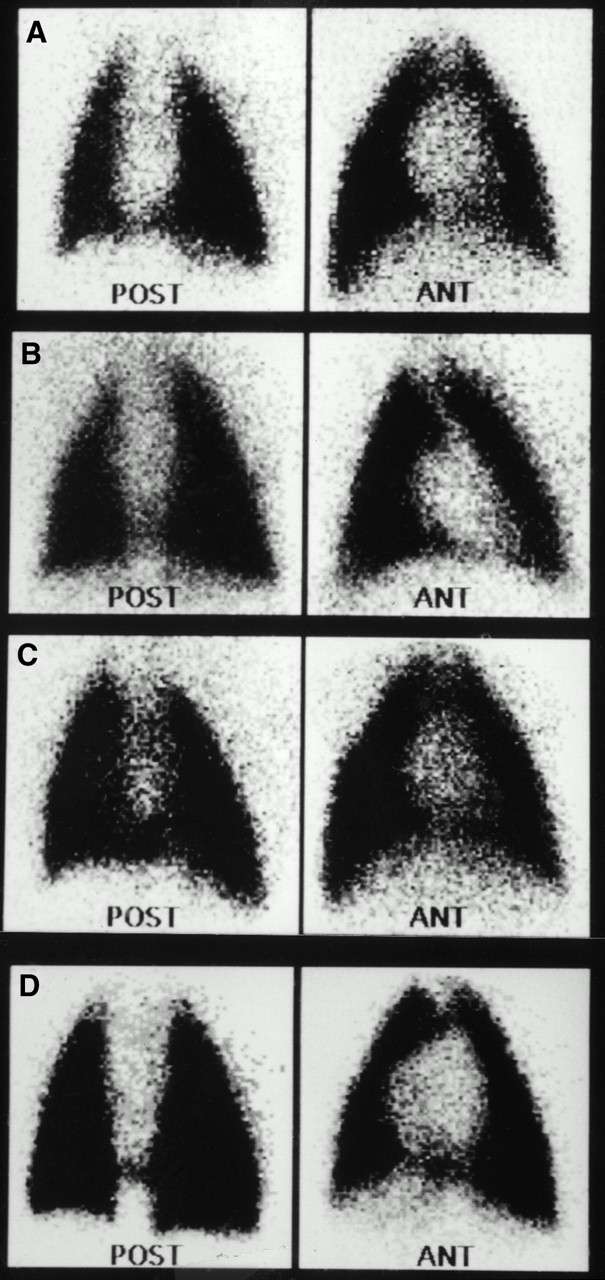
DTPA aerosol distributed uniformly throughout the lungs of all 14 irradiated animals without central hyperdeposition of radioactivity (Fig. 2). P.I. values in the irradiated lungs of these animals were not significantly changed from the matched baseline values in the repeated measurements on days 12 and 14 after irradiation (Table 1). The values in the irradiated lungs were not different from those in the nonirradiated lungs with the exception of day 12 after irradiation in group A. The combined P.I. values of all 14 animals at this time did not show significant differences (113.2% ± 17.1% vs. 120.5% ± 9.5%; not significant [NS]) (Table 1). After inhalation of a mixture of DTPA and surfactant, the radioactivity distributed uniformly in the lungs of four animals (Fig. 2), and no significant difference was found in the P.I. values between nonirradiated and irradiated lungs (112.6% ± 16.5% vs. 108.6% ± 14.2%; NS). P.I. values of the DTPA/surfactant mixture in the irradiated lungs of these animals were not different from those of the DTPA radioaerosol in the irradiated or nonirradiated lungs in group A animals (NS). No significant changes were noted in the chest radiography findings or the distribution of pulmonary perfusion in any irradiated animals.
P.I. Values of DTPA Radioaerosol in 14 Irradiated Animals

DTPA images acquired from group B animal. (A) Before irradiation. (B) Twelve days after irradiation. (C) After surfactant inhalation 14 d after irradiation. (D) After inhalation of mixture of DTPA and surfactant 16 d after irradiation. In all images, DTPA radioaerosol distributed uniformly throughout lungs. ANT = anterior; POST = posterior.
Two measurements of T1/2 at a 2-d interval in the six control animals showed good reproducibility (26.3 ± 6.5 min vs. 23.4 ± 6.1 min; NS). In the 14 irradiated animals before irradiation, no significant difference in T1/2 was seen between the right and the left lungs (23.6 ± 5.6 min vs. 24.9 ± 5.4 min; NS). On day 12 after irradiation, a significant prolongation in T1/2 in the irradiated right lungs compared with preirradiation was noted in both group A and group B animals (Fig. 3; Table 2) (P < 0.05), although no significant change in T1/2 was seen in the nonirradiated lungs (NS). The average T1/2 in all the irradiated lungs in the two groups was also significantly prolonged compared with that in the six control animals (29.1 ± 5.0 min vs. 24.6 ± 5.2 min; P < 0.05). In a repeated clearance test 2 d later, T1/2 was also significantly prolonged compared with baseline values in irradiated lungs of group A animals (P < 0.01), but no significant changes occurred in nonirradiated lungs (NS). In the group B animals that inhaled surfactant at this time, T1/2 in both nonirradiated and irradiated lungs was significantly prolonged compared with that measured on day 12 after irradiation (Fig. 3; Table 2) (both, P < 0.001). The percentage increase in T1/2 in irradiated lungs compared with that measured on day 12 after irradiation, however, was significantly greater in the group B animals than in the group A animals that did not inhale surfactant (25.3% ± 9.5% vs. 10.2% ± 10.4%; P < 0.05). No significant difference was seen in the percentage increase in T1/2 compared with baseline between irradiated lungs of group A animals and nonirradiated lungs of group B animals that inhaled surfactant (48.9% ± 34.4% vs. 46.6% ± 8.8%; NS).
T1/2 of DTPA in 14 Irradiated Animals
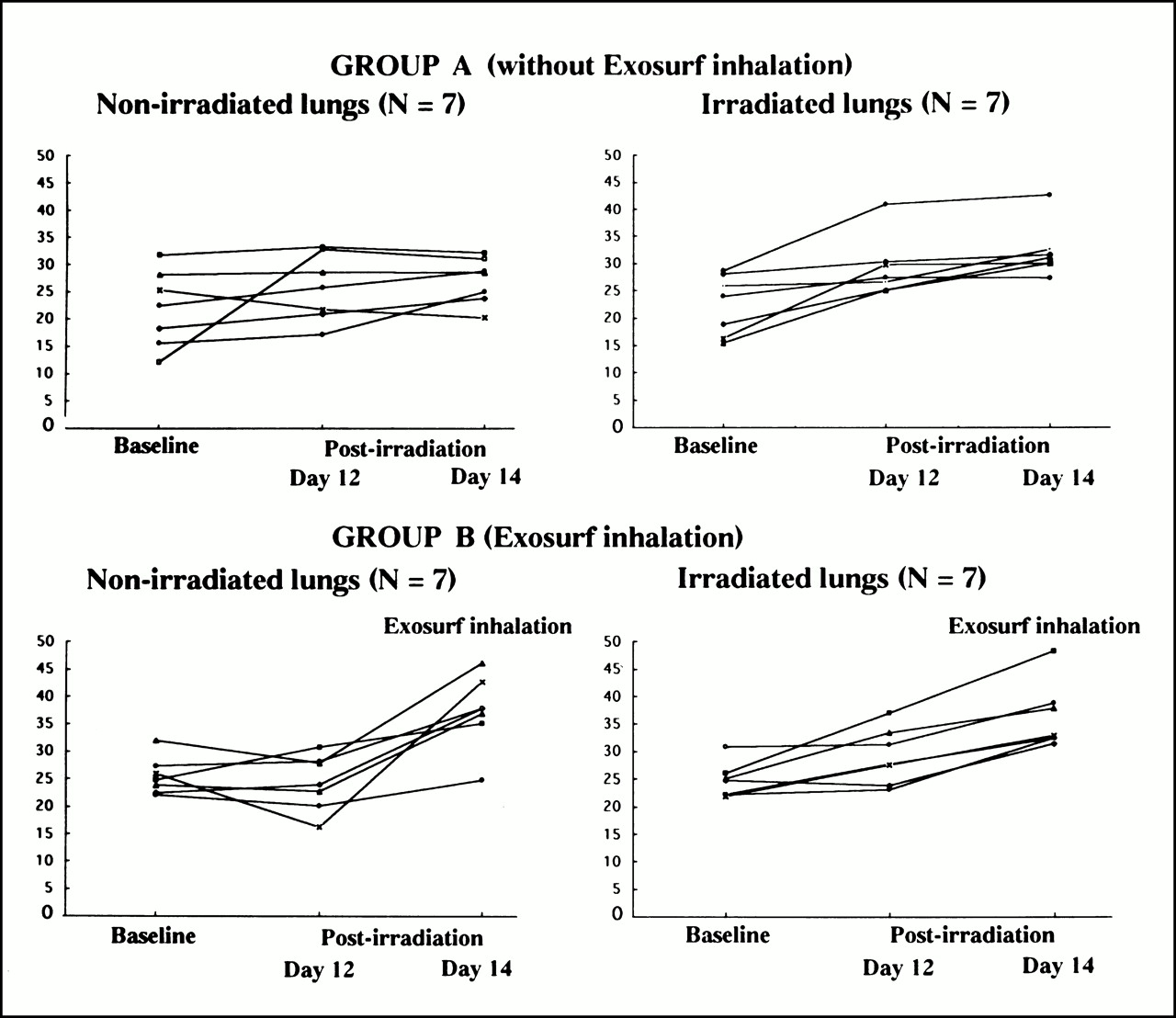
Changes of DTPA clearance time (T1/2) in 14 irradiated animals.
The concentrations of phospholipids and SP-A in lavage fluid from irradiated lungs were significantly increased compared with those from the nonirradiated lungs in the six animals (17.8 ± 3.0 μg/L vs. 9.2 ± 2.3 μg/L; P < 0.01; and 1.23 ± 0.83 ng/mL vs. 0.55 ± 0.65 ng/mL; P < 0.05, respectively). In these animals, follow-up CT scans 11–13 wk later showed infiltrates in the irradiated lung area.
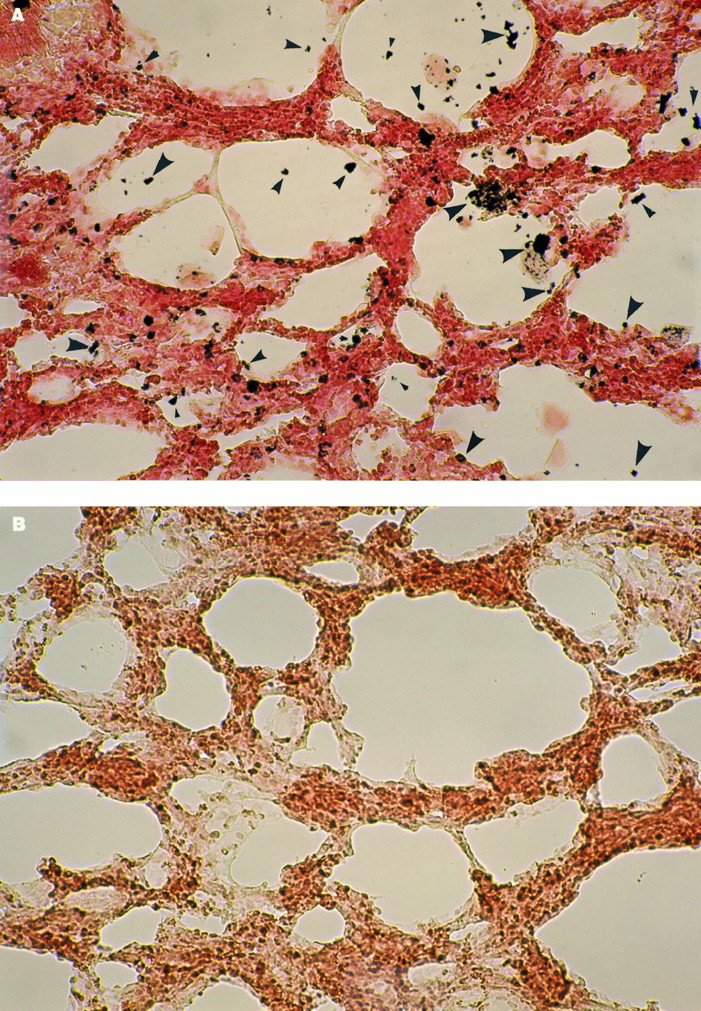
Histologic examination did not show substantial morphologic changes in the alveolar structures in any irradiated lungs of group A and B animals. In a Sudan black B fat stain of the lungs of group A animals, darkly stained granular or aggregated sudanophilic substances were seen scattered in the alveolar spaces throughout the irradiated lungs, although these substances were absent from nonirradiated lungs (Fig. 4). The development of exudative radiation pneumonitis was histologically confirmed in the six animals that manifested infiltrates in the irradiated lung area on follow-up CT scans.
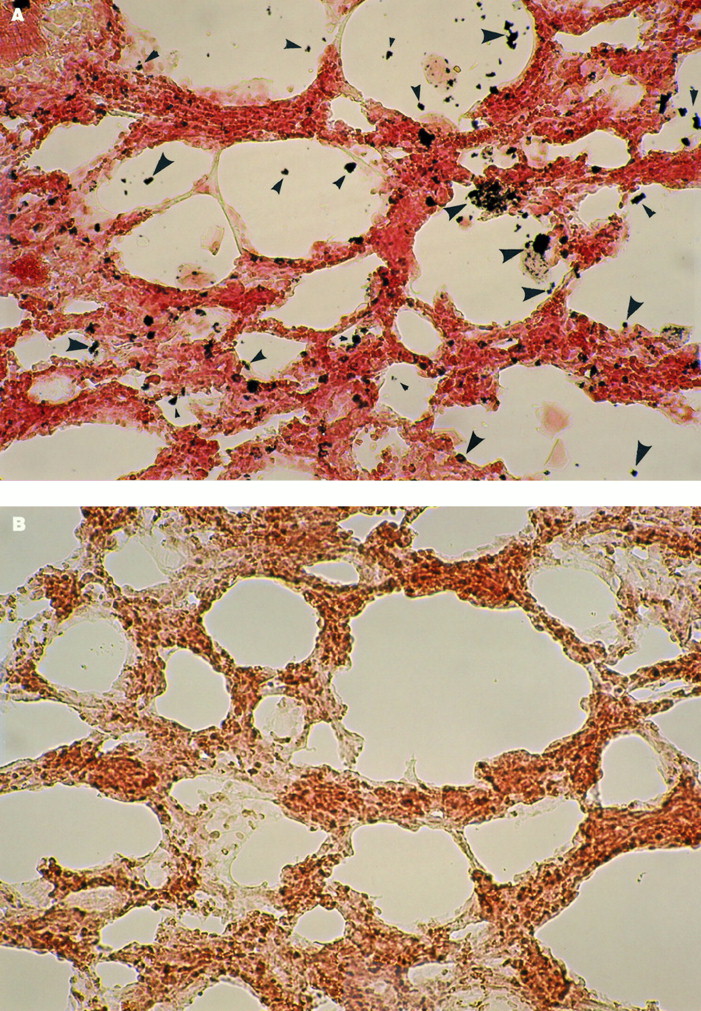
Photomicrographs of Sudan black B fat staining of lungs in group A animal. Alveolar darkly stained, granular or aggregated sudanophilic substances are scattered in irradiated lung (A, arrowheads) but are absent in nonirradiated lung (B).
DISCUSSION
This study showed significant and early prolongation of DTPA lung clearance in irradiated canine lungs. This result indicates that alveolar permeability to DTPA solute may be retarded in the initial phase of radiation lung injury before infiltrates are visible on CT and before substantial histologic signs of tissue damage. Several factors other than altered alveolar permeability, such as changes in the deposition pattern of DTPA aerosol or changes in pulmonary perfusion, might have influenced the results (17). However, when compared with normal or nonirradiated lungs, no significant changes were noted in these other factors in this study. The presence of alveolar sudanophilic substances and elevated lavage phospholipids and SP-A levels in the irradiated lungs suggests an early increase of alveolar surfactant after irradiation. The fact that surfactant inhalation similarly retarded DTPA clearance in nonirradiated lungs suggests that increased alveolar surfactant materials may be related to the retarded permeability of DTPA solute associated with the early phase of radiation lung injury.
Irradiation has an early effect on the lung surfactant system, as observed in our histologic and BAL studies. Previous animal BAL studies have also shown oversecretion of surfactant into the alveolar space soon after irradiation, and one of these studies reported that peak levels of alveolar surfactant phospholipids were reached 3–4 wk after irradiation (18–20). The increase of alveolar surfactant is considered to be related to early damage to type II alveolar epithelial cells with a rapid loss of lamellar bodies after irradiation. The damage to these cells leads to the early release of surfactant from the lamellar bodies into alveolar spaces and reduces the turnover of alveolar surfactant, thereby increasing the amount of alveolar surfactant (1,21–23). This study suggests that DTPA clearance studies may be an effective way to monitor these changes.
In the literature, only a few studies have focused on early alterations in DTPA lung clearance after irradiation. Similar to our result, Ahmed et al. (24) showed a trend toward a prolongation of DTPA clearance in irradiated canine lungs for several weeks after irradiation with single-fraction doses of 10–20 Gy, although they could not with confidence show a difference compared with preirradiation values. Small (molecular weight of 492) and water-soluble molecules of DTPA solute, after deposition on the alveolar surface, move across the alveolar epithelium through paracellular pathways by passive diffusion. The overall change in alveolar clearance of the solute is determined by an interplay of the surface area for transfer, the concentration gradient across the alveolar–capillary membrane, and the distance of the diffusion pathway of the solute (24,25). The mechanisms for the early retardation of alveolar DTPA clearance in irradiated lungs are not well known. However, in the absence of marked reductions in pulmonary blood flow, which can be the most important determinant of the transmembrane concentration gradient of the solute (26), it is plausible that increased alveolar surfactant may be partly responsible for the retarded clearance. Increased surfactant over the alveolar epithelium lengthens the distance of the diffusion pathway of the DTPA solute (8). The hydrophobic alveolar surfactant layer should strictly inhibit the diffusion of the water-soluble molecules of DTPA solute (8). The endoalveolar oxidation status after irradiation may also significantly influence the clearance of DTPA by modifying the affinity of clearance of DTPA. In the current study, the suppression effect of excess alveolar surfactant on DTPA clearance was observed in nonirradiated lungs after surfactant administration. This suppression effect was also shown in normal lungs of animals that underwent tracheal instillation of natural surfactant or inhalation of aerosolized surfactant (8,26). Clinically, a similar situation, with increased alveolar surfactant and retarded alveolar DTPA clearance, can be seen in patients with alveolar proteinosis (24).
Degeneration of the alveolar–capillary membrane is a consistent ultrastructural morphologic feature in the early phase of radiation lung injury (1,2,24). As part of this damage, swelling of the alveolar structures also may retard alveolar DTPA clearance by increasing the diffusion distance for the solute (1,2,24). Conversely, intercellular junctional loosening and cellular denudations increase the surface area for transfer of the solute, thereby accelerating DTPA clearance (6). From our results, it can be speculated that the increase in the surface area for transfer of DTPA caused by alveolar–capillary membrane damage is not sufficient to overcome possible surfactant-induced retardation of DTPA clearance in the early phase of radiation lung injury.
In contrast to our results, studies at a later time after irradiation showed accelerated DTPA clearance (a prepneumonic or pneumonic phase of radiation lung injury) (27–29). This result was also frequently observed in a variety of acute or chronic lung injuries (5–7,24,29,30). In these relatively late phases of radiation lung injury, the alveolar epithelium is more severely damaged, and excess lamellar bodies in alveolar type II cells are observed. This situation is associated with a reduction of alveolar surfactant (1,2,18–21,31,32). These morphologic changes and the reduction in alveolar surfactant should facilitate the alveolar transfer of DTPA solute (26,33).
Early oversecretion of endogeneous surfactant after irradiation may be a protective response to inhibit the increase in the surface area for the transfer of small solutes caused by the alveolar structural damage and may contribute to the preservation of alveolar liquid homeostasis. Inhalation of an adequate dose of a synthetic surfactant agent may have similar effects on DTPA clearance to increased levels of endogeneous lung surfactant soon after irradiation, as indicated by the current study. Exogenous surfactant therapy might augment the in vivo protective response of endogeneous surfactant and might be effective in partial protection from the later development of critical radiation pneumonitis (10,33–36). This result might especially occur in patients with significant acceleration of DTPA clearance soon after the initiation of external-beam pulmonary radiotherapy. To better clarify the interaction between alveolar permeability and surfactant after irradiation and to ascertain the most beneficial timing of exogenous surfactant therapy, further long-term studies, including patient studies, seem warranted.
CONCLUSION
This study revealed the retardation of DTPA transalveolar clearance soon after irradiation. It also showed that detectable changes of DTPA clearance preceded radiologic findings and alveolar structural changes as assessed by light microscopy. Alveolar lipid staining and lavage studies indicated the increase of alveolar surfactant in irradiated lungs. Just as the synthetic surfactant prolonged DTPA clearance in nonirradiated lungs, excess alveolar endogeneous surfactant may partly cause the slowing of DTPA clearance. Quantitative analysis of DTPA clearance is a sensitive way to evaluate the early response of the lung to radiation lung injury and may be helpful in clarifying the association between the changes in epithelial integrity and the alveolar surfactant system in the development of radiation pneumonitis.
Acknowledgments
The authors thank P. Esser, PhD, and T. Pozniakoff for their technical help, and Dr. T.S.T. Wang for his advice concerning radiopharmaceuticals. The authors also thank Dr. Warrett and Dr. Scittschell of Burroughs Wellcome Co. for Exosurf preparation.
Footnotes
Received Mar. 27, 2000; revision accepted Aug. 14, 2000.
For correspondence or reprints contact: Kazuyoshi Suga, MD, Department of Radiology, Yamaguchi University School of Medicine, 1-1-1 Minamikogushi, Ube, Yamaguchi, 755-8505, Japan.




{kind=link}
{kind=link}
{kind=link}
{kind=link}